The Effect of Olive Leaf Extract on Upper Respiratory Illness in High School Athletes: A Randomised Control Trial


Abstract
:
1. Introduction
2. Materials and Methods
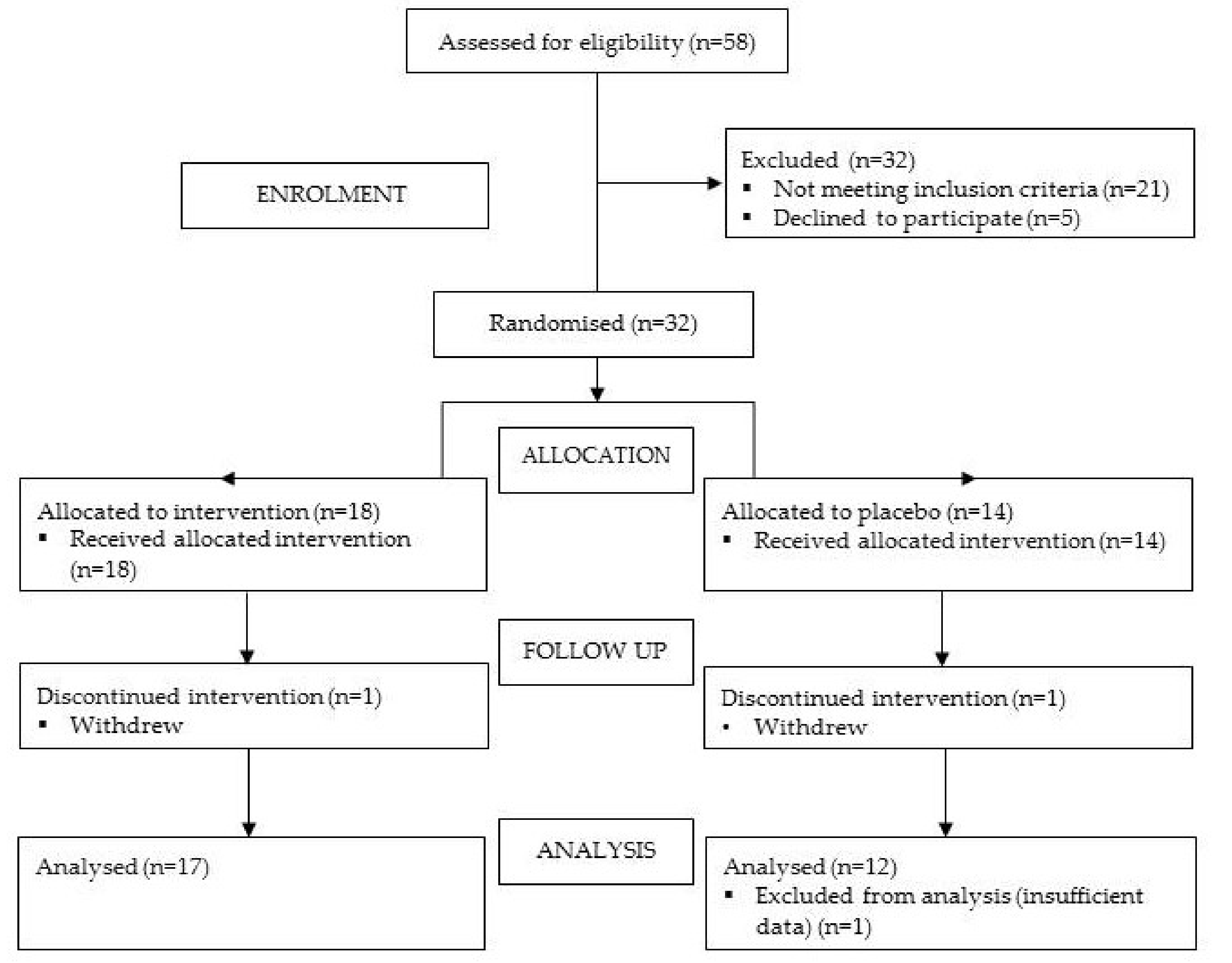
2.1. Design
2.2. Participants
2.3. Questionnaires
- How sore are you today?
- How stressed are you currently?
- Rate last night’s quality of sleep.
- How physically fatigued are you today?
- How hungry have you been recently?
2.3.2. Training Load
2.3.3. Upper Respiratory Illness
2.3.4. 24-Hour Food Recalls
2.4 Statistical Analysis
2.4.1. URI Incidence
2.4.2. URI Duration
2.4.3. Secondary Outcomes
2.4.4. 24-Hour Food Recalls
3. Results
3.1. Population Characteristics
3.2. URI Incidence and Duration
3.3. Secondary Outcomes
3.4. Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nieman, D.; Pedersen, B. Exercise and Immune Function. Sports Med. 1999, 27, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Steffen, K.; Alonso, J.M.; Aubry, M.; Dvorak, J.; Junge, A.; Meeuwisse, W.; Mountjoy, M.; Renstrom, P.; Wilkinson, M. Sports Injuries and Illnesses during the Winter Olympic Games 2010. Br. J. Sports Med. 2010, 44, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M.; et al. Sports Injuries and Illnesses during the London Summer Olympic Games 2012. Br. J. Sports Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.J.; Gleeson, M.; Pyne, D.B.; Callister, R.; Hopkins, W.G.; Fricker, P.A. Clinical and Laboratory Evaluation of Upper Respiratory Symptoms in Elite Athletes. Clin. J. Sport Med. 2008, 18, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Brink, M.S.; Visscher, C.; Arends, S.; Zwerver, J.; Post, W.J.; Lemmink, K.A. Monitoring Stress and Recovery: New Insights for the Prevention of Injuries and Illnesses in Elite Youth Soccer Players. Br. J. Sports Med. 2010, 44, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Ruedl, G.; Schobersberger, W.; Pocecco, E.; Blank, C.; Engebretsen, L.; Soligard, T.; Steffen, K.; Kopp, M.; Burtscher, M. Sport Injuries and Illnesses during the First Winter Youth Olympic Games 2012 in Innsbruck, Austria. Br. J. Sports Med. 2012, 46, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Somerville, V.; Gill, N.D.; Ross, A.; Braakhuis, A. Upper Respiratory Illness in Different Tiers of Rugby Union. Sport Sci. for Health 2018, 1–9. [Google Scholar] [CrossRef]
- Common Cold. Best Practice. Available online: http://bestpractice.bmj.com.ezproxy.auckland.ac.nz/best-practice/monograph/252/highlights.html (accessed on 27 November 2018).
- Somerville, V.S.; Braakhuis, A.J.; Hopkins, W.G. Effect of Flavonoids on Upper Respiratory Tract Infections and Immune Function: A Systematic Review and Meta-Analysis. Adv. Nutr. 2016, 7, 488–497. [Google Scholar] [CrossRef]
- Haywood, B.A.; Black, K.E.; Baker, D.; McGarvey, J.; Healey, P.; Brown, R.C. Probiotic Supplementation Reduces the Duration and Incidence of Infections but Not Severity in Elite Rugby Union Players. J. Sci. Med. Sport 2013, 17, 356–360. [Google Scholar] [CrossRef]
- Douglas, R.M.; Hemilä, H. Vitamin C for Preventing and Treating the Common Cold. PLoS Med. 2005, 2, e168. [Google Scholar] [CrossRef]
- Strasser, B.; Geiger, D.; Schauer, M.; Gostner, J.M.; Gatterer, H.; Burtscher, M.; Fuchs, D. Probiotic Supplements Beneficially Affect Tryptophan–kynurenine Metabolism and Reduce the Incidence of Upper Respiratory Tract Infections in Trained Athletes: A. Randomized, Double-Blinded, Placebo-Controlled Trial. Nutrients 2016, 8, 752. [Google Scholar] [CrossRef] [PubMed]
- Visioli, F.; Galli, C.; Galli, G.; Caruso, D. Biological Activities and Metabolic Fate of Olive Oil Phenols. Eur. J. Lipid Sci. Technol. 2002, 104, 677–684. [Google Scholar] [CrossRef]
- Visioli, F.; Bellosta, S.; Galli, C. Oleuropein, the Bitter Principle of Olives, Enhances Nitric Oxide Production by Mouse Macrophages. Life Sci. 1998, 62, 541–546. [Google Scholar] [CrossRef]
- Aziz, N.H.; Farag, S.E.; Mousa, L.A.; Abo-Zaid, M.A. Comparative Antibacterial and Antifungal Effects of some Phenolic Compounds. Microbios 1998, 93, 43–54. [Google Scholar] [PubMed]
- Bisignano, G.; Tomaino, A.; Cascio, R.L.; Crisafi, G.; Uccella, N.; Saija, A. On the In-vitro Antimicrobial Activity of Oleuropein and Hydroxytyrosol. J. Pharm. Pharmacol. 1999, 51, 971–974. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Deng, X.; But, P.P.; Ooi, V.E.; Xu, H.; Lee, S.H.; Lee, S. In Vitro Evaluation of Secoiridoid Glucosides from the Fruits of Ligustrum Lucidum as Antiviral Agents. Chem. Pharm. Bull. 2001, 49, 1471–1473. [Google Scholar] [CrossRef]
- New Zealand’s Exchange. Comvita Announces Records Earning. Available online: https://www.nzx.com/announcements/264680 (accessed on 27 November 2018).
- Gleeson, M.; Bishop, N.; Oliveira, M.; Tauler, P. Daily Probiotic’s (Lactobacillus Casei Shirota) Reduction of Infection Incidence in Athletes. Int. J. Sport Nutr. Exerc Metab. 2011, 21, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Somerville, V.; Moore, R.; Braakhuis, A. Creation and Validation of a Sporting Upper Respiratory Illness (SUPPRESS) Questionnaire to Determine Upper Respiratory Illness Incidence and Duration in New Zealand Athletes. (manuscript in preparation).
- Huang, T.T.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of Screening Out Implausible Energy Intake Reports on Relationships between Diet and BMI. Obes. Res. 2005, 13, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Otis, C.L.; Drinkwater, B.; Johnson, M.; Loucks, A.; Wilmore, J. American College of Sports Medicine Position Stand. the Female Athlete Triad. Med. Sci. Sports Exerc. 1997, 29, i–ix. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. The IOC Consensus Statement: Beyond the Female Athlete Triad-Relative Energy Deficiency in Sport (RED-S.). Br. J. Sports Med. 2014, 48, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H. IOC Consensus Statement: Dietary Supplements and the High-Performance Athlete. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 104–125. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Bishop, N.; Handzlik, M.K.; Muhamad, A.S.; Gleeson, M. Sex Differences in Upper Respiratory Symptoms Prevalence and Oral-Respiratory Mucosal Immunity in Endurance Athletes. Exerc. Immunol. Rev. 2014, 20, 8–22. [Google Scholar] [PubMed]
- Pehlivanoglu, B.; Balkanci, Z.; Ridvanagaoglu, A.; Durmazlar, N.; Öztürk, G.; Erbas, D.; Okur, H. Impact of Stress, Gender and Menstrual Cycle on Immune System: Possible Role of Nitric Oxide. Arch. Physiol. Biochem. 2001, 109, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Brinkworth, G.D.; Buckley, J.D. Concentrated Bovine Colostrum Protein Supplementation Reduces the Incidence of Self-Reported Symptoms of Upper Respiratory Tract Infection in Adult Males. Eur. J. Nutr. 2003, 42, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Henson, D.A.; McMahon, M.; Wrieden, J.L.; Davis, J.M.; Murphy, E.A.; Gross, S.J.; McAnulty, L.S.; Dumke, C.L. Beta-Glucan, Immune Function, and Upper Respiratory Tract Infections in Athletes. Med. Sci. Sports Exerc. 2008, 40, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Constantini, N.W.; Dubnov-Raz, G.; Eyal, B.; Berry, E.M.; Cohen, A.H.; Hemilä, H. The Effect of Vitamin C on Upper Respiratory Infections in Adolescent Swimmers: A. Randomized Trial. Eur. J. Pediatr. 2011, 170, 59–63. [Google Scholar] [CrossRef]
- Dubnov-Raz, G.; Livne, N.; Raz, R.; Cohen, A.H.; Constantini, N.W. Vitamin D Supplementation and Physical Performance in Adolescent Swimmers. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 317–325. [Google Scholar] [CrossRef]
- Hemila, H.; Chalker, E. Vitamin C for Preventing and Treating the Common Cold. Cochrane Database Syst. Rev. 2013, 18. [Google Scholar] [CrossRef]
- Wheeler, A. Hypersensitivity to the Allergens of the Pollen from the Olive Tree (Olea Europaea). Clin. Exp. Allergy 1992, 22, 1052–1057. [Google Scholar] [CrossRef]
- Petkov, V.; Manolov, P. Pharmacological Analysis of the Iridoid Oleuropein. Arzneimittelforschung 1972, 22, 1476–1486. [Google Scholar]
- D’Angelo, S.; Manna, C.; Migliardi, V.; Mazzoni, O.; Morrica, P.; Capasso, G.; Pontoni, G.; Galletti, P.; Zappia, V. Pharmacokinetics and Metabolism of Hydroxytyrosol, a Natural Antioxidant from Olive Oil. Drug Metab. Dispos. 2001, 29, 1492–1498. [Google Scholar] [PubMed]
- Lockyer, S.; Rowland, I.; Spencer, J.P.E.; Yaqoob, P.; Stonehouse, W. Impact of Phenolic-Rich Olive Leaf Extract on Blood Pressure, Plasma Lipids and Inflammatory Markers: A Randomised Controlled Trial. Eur. J. Nutr. 2017, 56, 1421–1432. [Google Scholar] [CrossRef] [PubMed]
- Filip, R.; Possemiers, S.; Heyerick, A.; Pinheiro, I.; Raszewski, G.; Davicco, M.; Coxam, V. Twelve-Month Consumption of a Polyphenol Extract from Olive (Olea Europaea) in a Double Blind, Randomized Trial Increases Serum Total Osteocalcin Levels and Improves Serum Lipid Profiles in Postmenopausal Women with Osteopenia. J. Nutr. Health Aging 2015, 19, 77–86. [Google Scholar] [CrossRef] [PubMed]
- De Bock, M.; Derraik, J.G.; Brennan, C.M.; Biggs, J.B.; Morgan, P.E.; Hodgkinson, S.C.; Hofman, P.L.; Cutfield, W.S. Olive (Olea Europaea, L.) Leaf Polyphenols Improve Insulin Sensitivity in Middle-Aged Overweight Men: A. Randomized, Placebo-Controlled, Crossover Trial. PLoS ONE 2013, 8, e57622. [Google Scholar] [CrossRef] [PubMed]
- Perrinjaquet-Moccetti, T.; Busjahn, A.; Schmidlin, C.; Schmidt, A.; Bradl, B.; Aydogan, C. Food Supplementation with an Olive (Olea Europaea, L.) Leaf Extract Reduces Blood Pressure in Borderline Hypertensive Monozygotic Twins. Phytother. Res. 2008, 22, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- De Bock, M.; Thorstensen, E.B.; Derraik, J.G.; Henderson, H.V.; Hofman, P.L.; Cutfield, W.S. Human Absorption and Metabolism of Oleuropein and Hydroxytyrosol Ingested as Olive (Olea Europaea, L.) Leaf Extract. Mol. Nutr. Food Res. 2013, 57, 2079–2085. [Google Scholar] [CrossRef]
- García-Villalba, R.; Larrosa, M.; Possemiers, S.; Tomás-Barberán, F.; Espín, J. Bioavailability of Phenolics from an Oleuropein-Rich Olive (Olea Europaea) Leaf Extract and its Acute Effect on Plasma Antioxidant Status: Comparison between Pre-and Postmenopausal Women. Eur. J. Nutr. 2014, 53, 1015–1027. [Google Scholar] [CrossRef]
- Lockyer, S.; Corona, G.; Yaqoob, P.; Spencer, J.P.; Rowland, I. Secoiridoids Delivered as Olive Leaf Extract Induce Acute Improvements in Human Vascular Function and Reduction of an Inflammatory Cytokine: A. Randomised, Double-Blind, Placebo-Controlled, Cross-Over Trial. Br. J. Nutr. 2015, 114, 75–83. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Olive Leaf Extract (OLE) (n = 17) | Control (n = 12) | |
|---|---|---|
| Age (±SD) | 16.5 years (±0.5) | 16.5 years (±0.5) |
| Weight (±SD) | 69.2 kg (±13.0) | 64.3 kg (±7.9) |
| Height (±SD) | 1.73 m (±0.07) | 1.73 m (±0.10) |
| Male | 35% | 33% |
| Wellbeing (±SD) | 65.6% (±12.7) | 64.8% (±12.5) |
| Game Time (±SD) | 137 min·week−1 (±117) | 112 min·week−1 (±114) |
| Cardio (±SD) | 182 min·week−1 (±372) | 99 min·week−1 (±72) |
| Weight (±SD) | 19 min·week−1 (±35) | 37 min·week−1 (±72) |
| Compliance (%) | 74.7 | 83.8 |
| OLE (n = 17) | Control (n = 12) | |||
|---|---|---|---|---|
| N | Proportion | N | Proportion | |
| Incidence | 10 | 0.59 | 7 | 0.58 |
| Sick Days | 145.5 | 0.16 | 135.5 | 0.20 |
| N | N | |||
| Episodes | 15 | 11 | ||
| OLE (n = 16) | Control (n = 11) | ||
|---|---|---|---|
| Total Energy (±SD) | 8209.9 (±3351.3) kJ·day−1 | 7826.9 (±2684.9) kJ·day−1 | |
| Macronutrient | |||
| Carbohydrate (±SD) | 3.67 (±2.00) g·kgBW−1·day−1 | 3.58 (±1.41) g·kgBW−1·day−1 | |
| Protein (±SD) | 1.28 (±0.61) g·kgBW−1·day−1 | 1.34 (±0.39) g·kgBW−1·day−1 | |
| Fat (±SD) | 0.91 (±0.46) g·kgBW−1·day−1 | 1.04 (±0.47) g·kgBW−1·day−1 | |
| Micronutrient | |||
| Vitamin C (±SD) | 94.50 (±69.02) mg·day−1 | 82.40 (±69.85) mg·day−1 | |
| Vitamin D (±SD) | 1.66 (±1.21) µg·day−1 | 2.06 (±1.50) µg·day−1 | |
| Selenium (±SD) | 54.40 (±19.96) µg·day−1 | 59.43 (±21.51) µg·day−1 | |
| Iron (±SD) | 15.17 (±9.60) mg·day−1 | 11.41 (±3.58) mg·day−1 | |
| Zinc (±SD) | 11.54 (±5.74) mg·day−1 | 10.21 (±3.82) mg·day−1 | |
| Polyphenol (±SD) | 115.60 (±176.76) mg·day−1 | 69.75 (±55.63) mg·day−1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somerville, V.; Moore, R.; Braakhuis, A. The Effect of Olive Leaf Extract on Upper Respiratory Illness in High School Athletes: A Randomised Control Trial. Nutrients 2019, 11, 358. https://doi.org/10.3390/nu11020358
Somerville V, Moore R, Braakhuis A. The Effect of Olive Leaf Extract on Upper Respiratory Illness in High School Athletes: A Randomised Control Trial. Nutrients. 2019; 11(2):358. https://doi.org/10.3390/nu11020358
Chicago/Turabian StyleSomerville, Vaughan, Rachel Moore, and Andrea Braakhuis. 2019. "The Effect of Olive Leaf Extract on Upper Respiratory Illness in High School Athletes: A Randomised Control Trial" Nutrients 11, no. 2: 358. https://doi.org/10.3390/nu11020358
APA StyleSomerville, V., Moore, R., & Braakhuis, A. (2019). The Effect of Olive Leaf Extract on Upper Respiratory Illness in High School Athletes: A Randomised Control Trial. Nutrients, 11(2), 358. https://doi.org/10.3390/nu11020358