Effect of Supplementation of a Whey Peptide Rich in Tryptophan-Tyrosine-Related Peptides on Cognitive Performance in Healthy Adults: A Randomized, Double-Blind, Placebo-Controlled Study


Abstract
1. Introduction
2. Materials and Methods
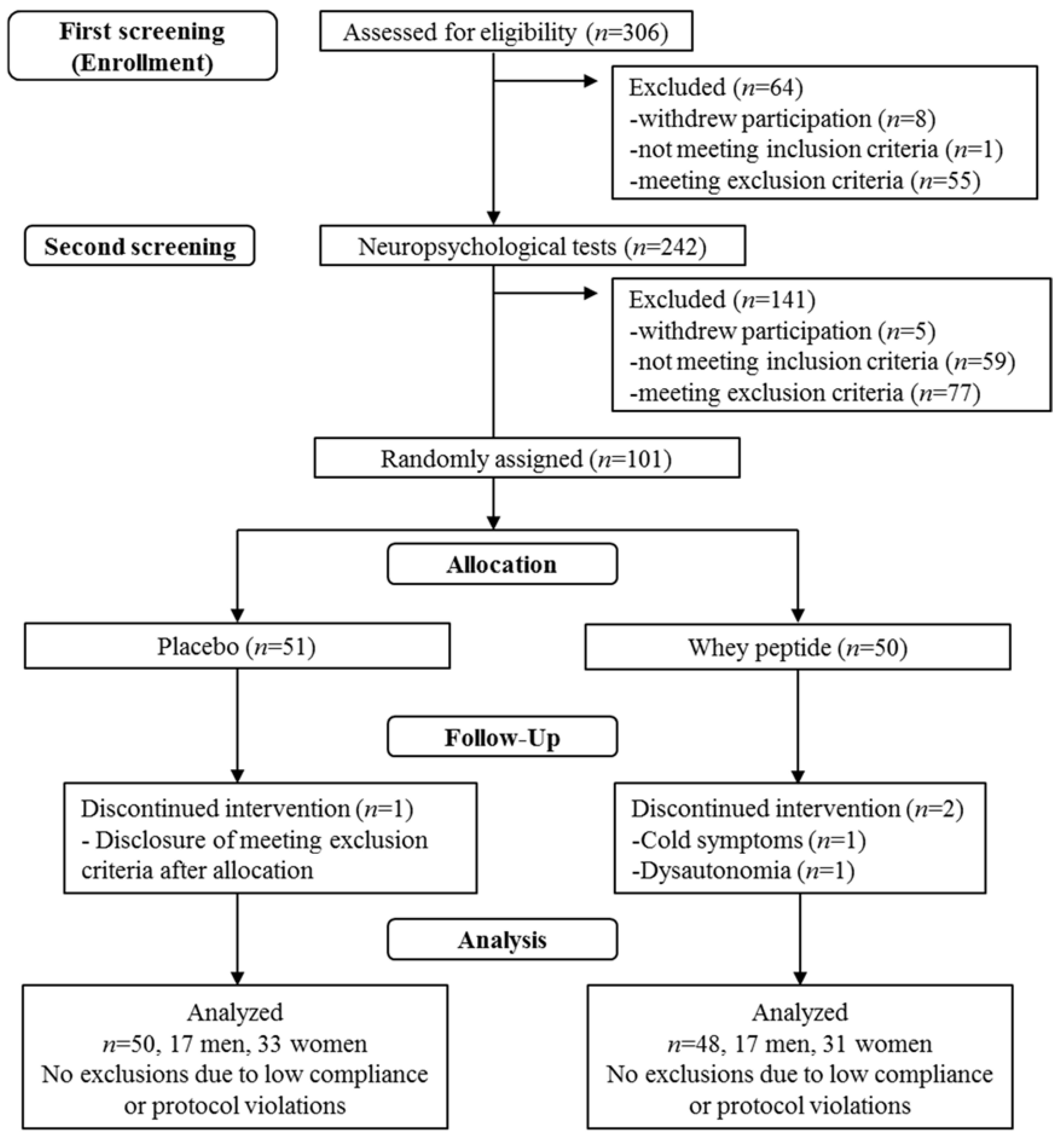
2.1. Subjects
2.2. Experimental Supplements
2.3. Procedures
2.4. Neuropsychological Tests
2.5. Subjective Psychological Assessment
2.6. Safety Assessment
2.7. Statistical Analysis
2.8. Ethics and Registration
3. Results
3.1. Baseline Characteristics of the Study Groups
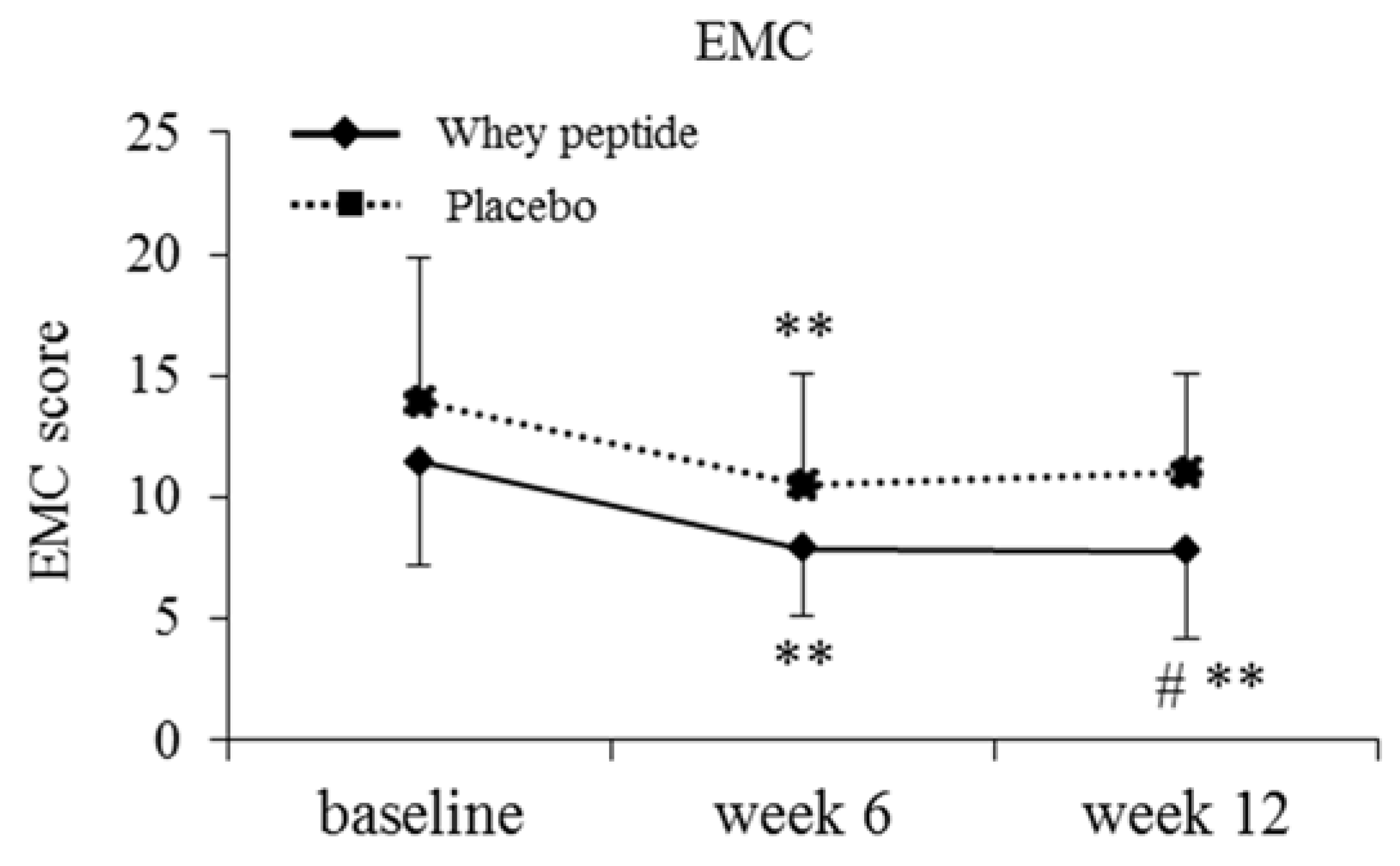
3.2. Subjective Psychological Assessment
3.3. Neuropsychological Tests (Full Analysis Set (FAS))
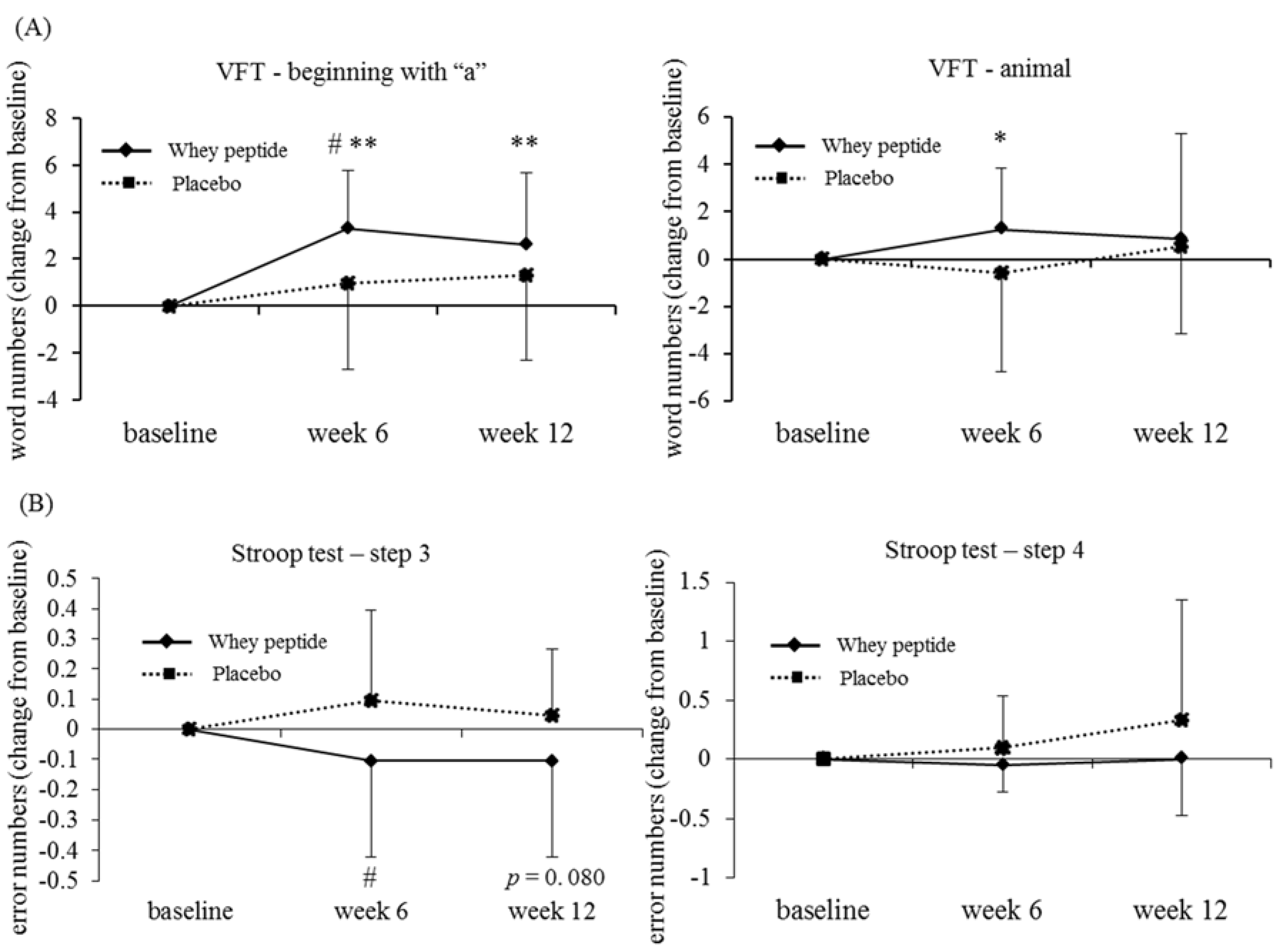
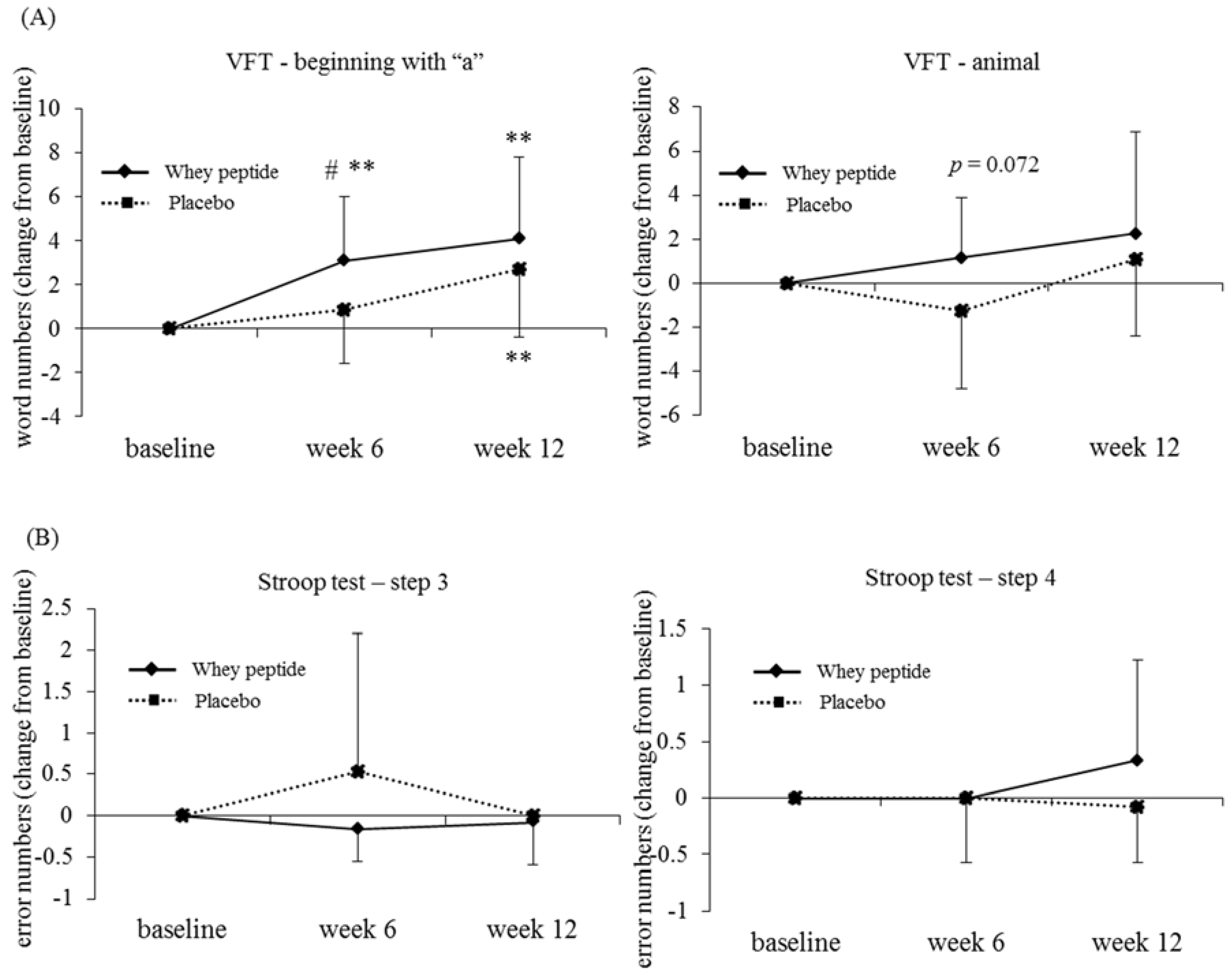
3.4. Subgroup Analysis by the Degree of Fatigue
3.5. Safety Assessment and Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Department of Economic and Social Affairs United Nations. World Population Prospects: Key Findings and Advance Tables—The 2015 Revision; United Nations Publications: New York, NY, USA, 2015. [Google Scholar]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015 The Global Impact of Dementia. An Analysis of Prevalence, Incidence, Cost and Trends. Alzheimer’s Disease International publications. Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf. (accessed on 25 January 2018).
- Ano, Y.; Nakayama, H. Preventive effects of dairy products on dementia and the underlying mechanisms. Int. J. Mol. Sci. 2018, 19, 1927. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, M.; Ninomiya, T.; Ohara, T.; Doi, Y.; Uchida, K.; Shirota, T.; Yonemoto, K.; Kitazono, T.; Kiyohara, Y. Dietary patterns and risk of dementia in an elderly Japanese population: The Hisayama Study. AJCN 2013, 97, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Murphy, K.J.; Bryan, J. Dairy intake and cognitive health in middle-aged South Australians. Asia Pac. J. Clin. Nutr. 2010, 19, 161–171. [Google Scholar] [PubMed]
- Ogata, S.; Tanaka, H.; Omura, K.; Honda, C.; Hayakawa, K. Association between intake of dairy products and short-term memory with and without adjustment for genetic and family environmental factors: A twin study. Clin. Nutr. 2016, 35, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Ano, Y.; Ozawa, M.; Kutsukake, T.; Sugiyama, S.; Uchida, K.; Yoshida, A.; Nakayama, H. Preventive effects of a fermented dairy product against Alzheimer's disease and identification of a novel oleamide with enhanced microglial phagocytosis and anti-inflammatory activity. PLoS ONE 2015, 10, e0118512. [Google Scholar] [CrossRef] [PubMed]
- Camfield, D.A.; Owen, L.; Scholey, A.B.; Pipingas, A.; Stough, C. Dairy constituents and neurocognitive health in ageing. Br. J. Nutr. 2011, 106, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Kiyosawa, I. Progress in Recent Reesearches on the Whey Protein Concentrates and their Functional Properties (Japanese). Milk Sci. 2002, 51, 13–26. [Google Scholar]
- Markus, C.R.; Olivier, B.; de Haan, E.H. Whey protein rich in alpha-lactalbumin increases the ratio of plasma tryptophan to the sum of the other large neutral amino acids and improves cognitive performance in stress-vulnerable subjects. AJCN 2002, 75, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Markus, C.R.; Olivier, B.; Panhuysen, G.E.; Van Der Gugten, J.; Alles, M.S.; Tuiten, A.; Westenberg, H.G.; Fekkes, D.; Koppeschaar, H.F.; de Haan, E.E. The bovine protein alpha-lactalbumin increases the plasma ratio of tryptophan to the other large neutral amino acids, and in vulnerable subjects raises brain serotonin activity, reduces cortisol concentration, and improves mood under stress. AJCN 2000, 71, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.J.; Greenwood, C.E.; Winocur, G.; Wolever, T.M. Dietary protein, carbohydrate, and fat enhance memory performance in the healthy elderly. AJCN 2001, 74, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Ano, Y.; Ayabe, T.; Kutsukake, T.; Ohya, R.; Uchida, S.; Yamada, K.; Takashima, A.; Nakayama, H. Novel lacto-peptides in fermented dairy products improve memory function and cognitive decline. Neurobiol. Aging 2018. under review. [Google Scholar]
- Imamura, Y.; Uemura, K. Functional localization in prefrontal area by hamamatsu higher brain function scale (Japanese). Japan. J. Neuropsychol. 1996, 12, 99–105. [Google Scholar]
- Kazui, H.; Watamori, T.; Honda, R.; Tokimasa, A.; Hirono, N.; Mori, E. Nihonban Rivermead Behavioural Memory Test (RBMT) no yuuyousei no kentou (Japanese). Adv. Neurol. Sci. 2002, 46, 307–318. [Google Scholar]
- Borkowski, J.G.; Benton, A.L.; Spreen, O. Word fluency and brain damage. Neuropsychologia 1967, 5, 135–140. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Kato, M. The development and standardization of Clinical Assessment for Attention (CAT) and Clinical Assessment for Spontaneity (CAS) (Japanese). Higher Brain Function Res. 2006, 26, 310–319. [Google Scholar] [CrossRef]
- Japanese Society of Fatigue Science. Available online: http://www.hirougakkai.com (accessed on 27 February 2017).
- Verhoeven, E.W.; Kraaimaat, F.W.; van de Kerkhof, P.C.; van Weel, C.; Duller, P.; van der Valk, P.G.; van den Hoogen, H.J.; Bor, J.H.; Schers, H.J.; Evers, A.W. Prevalence of physical symptoms of itch, pain and fatigue in patients with skin diseases in general practice. Br. J. Dermatol. 2007, 156, 1346–1349. [Google Scholar] [CrossRef] [PubMed]
- Rat, A.C.; Pouchot, J.; Fautrel, B.; Boumier, P.; Goupille, P.; Guillemin, F. Factors associated with fatigue in early arthritis: Results from a multicenter national French cohort study. Arthrit. Care Res. 2012, 64, 1061–1069. [Google Scholar]
- Heuchert, J.P.; McNair, D.M. Profiles of Mood States, 2nd ed.; Kaneko syobo: Tokyo, Japan, 2015. [Google Scholar]
- Kazui, H.; Watamori, T.S.; Honda, R.; Mori, E. The validation of a Japanese version of the Everyday Memory Checklist (Japanese). Brain Nerve 2003, 55, 317–325. [Google Scholar] [PubMed]
- Cottingham, M.E.; Hawkins, K.A. Verbal fluency deficits co-occur with memory deficits in geriatric patients at risk for dementia: Implications for the concept of mild cognitive impairment. Behav. Neurol. 2010, 22, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef] [PubMed]
- Troyer, A.K.; Moscovitch, M.; Winocur, G.; Alexander, M.P.; Stuss, D. Clustering and switching on verbal fluency: The effects of focal frontal- and temporal-lobe lesions. Neuropsychologia 1998, 36, 499–504. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.W.; Cohen, J.D.; Stenger, V.A.; Carter, C.S. Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science 2000, 288, 1835–1838. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Roiland, R.; Heffner, K.; Johnson, M.; Chen, D.G.; Mapstone, M. Evaluation of objective and perceived mental fatigability in older adults with vascular risk. J. Psychosom. Res. 2014, 76, 458–464. [Google Scholar] [CrossRef] [PubMed]
- DeLuca, J.; Genova, H.M.; Capili, E.J.; Wylie, G.R. Functional neuroimaging of fatigue. Phys. Med. Rehabil. Clin. N. Am. 2009, 20, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Wylie, G.R.; Genova, H.M.; DeLuca, J.; Dobryakova, E. The relationship between outcome prediction and cognitive fatigue: A convergence of paradigms. Cogn. Affect. Behav. Neurosci. 2017, 17, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, A.F.; Li, B.M. Neurobiology of executive functions: Catecholamine influences on prefrontal cortical functions. Biol. Psychiatry 2005, 57, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Puig, M.V.; Rose, J.; Schmidt, R.; Freund, N. Dopamine modulation of learning and memory in the prefrontal cortex: Insights from studies in primates, rodents, and birds. Front. Neural Circ. 2014, 8, 93. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, K.; Takahashi, H.; Kashiwagura, T.; Yamada, K.; Yanagida, S.; Homma, M.; Dairiki, K.; Sasaki, H.; Kawagoshi, A.; Satake, M.; et al. Effect of anti-inflammatory supplementation with whey peptide and exercise therapy in patients with COPD. Respir. Med. 2012, 106, 1526–1534. [Google Scholar] [CrossRef] [PubMed]
- Madadlou, A.; Abbaspourrad, A. Bioactive whey peptide particles: An emerging class of nutraceutical carriers. Clin. Rev. Food Sci. Nutr. 2018, 58, 1468–1477. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Placebo (n = 50) | Whey Peptide (n = 48) | p-Value |
|---|---|---|---|
| Age | 51.8 ± 5.2 | 52.3 ± 4.3 | 0.568 |
| Male/female | 17/33 | 17/31 | 1.000 |
| Body mass index (kg/m2) | 21.35 ± 2.04 | 21.11 ± 2.10 | 0.564 |
| Education years | 14.1 ± 1.8 | 14.5 ± 2.0 | 0.406 |
| HDS-R score | 28.4 ± 1.5 | 28.5 ± 1.8 | 0.678 |
| Psychological Status | Placebo (n = 50) | Whey Peptide (n = 48) | p-Value |
|---|---|---|---|
| POMS2 | |||
| AH | 45.9 ± 9.1 | 45.5 ± 8.7 | 0.842 |
| CB | 48.8 ± 7.6 | 48.2 ± 8.4 | 0.707 |
| DD | 46.9 ± 6.0 | 46.3 ± 7.3 | 0.663 |
| FI | 45.2 ± 7.9 | 44.2 ± 8.9 | 0.547 |
| TA | 47.8 ± 7.4 | 46.4 ± 7.9 | 0.360 |
| VA | 47.2 ± 8.3 | 53.0 ± 10.2 | 0.002 |
| F | 48.8 ± 8.9 | 53.3 ± 9.5 | 0.019 |
| TMD | 47.2 ± 6.9 | 45.0 ± 8.6 | 0.159 |
| VAS (after-before) | 19.1 ± 16.1 | 20.6 ± 18.1 | 0.661 |
| EMC | 13.0 ± 4.8 | 12.8 ± 4.6 | 0.826 |
| Test | Group | Week 0 (Baseline) | Week 6 | Week 12 | |
|---|---|---|---|---|---|
| Word recall | |||||
| Immediate recall | Score | P | 4.2 ± 0.9 | 4.8 ± 0.9 ** | 5.1 ± 1.1 ** |
| W | 4.4 ± 1.0 | 5.1 ± 0.9 ** | 5.2 ± 1.0 ** | ||
| Changes from baseline | P | 0.7 ± 1.3 | 0.9 ± 1.1 | ||
| W | 0.8 ± 1.2 | 0.8 ± 1.3 | |||
| 5-min delayed recall | Score | P | 3.6 ± 1.1 | 4.9 ± 1.3 ** | 5.3 ± 1.2 ** |
| W | 3.7 ± 1.1 | 4.7 ± 1.5 ** | 5.1 ± 1.4 ** | ||
| Changes from baseline | P | 1.3 ± 1.4 | 1.7 ± 1.3 | ||
| W | 1.0 ± 1.9 | 1.4 ± 1.7 | |||
| 20-min delayed recall | Score | P | 4.3 ± 1.2 | 5.3 ± 1.3 ** | 5.6 ± 1.4 ** |
| W | 4.2 ± 1.2 | 5.1 ± 1.6 ** | 5.4 ± 1.4 ** | ||
| Changes from baseline | P | 1.0 ± 1.8 | 1.3 ± 1.6 | ||
| W | 0.9 ± 1.8 | 1.2 ± 1.7 | |||
| Story recall | |||||
| Immediate recall | Score | P | 15.93 ± 2.53 | 17.65 ± 3.03 ** | 17.56 ± 2.77 ** |
| W | 15.51 ± 2.55 | 16.58 ± 2.64 * | 16.92 ± 2.52 ** | ||
| Changes from baseline | P | 1.72 ± 3.71 | 1.63 ± 3.63 | ||
| W | 1.07 ± 3.08 | 1.41 ± 3.38 | |||
| 20-min delayed recall | Score | P | 14.39 ± 3.05 | 16.59 ± 3.45 ** | 16.63 ± 2.81 ** |
| W | 14.44 ± 2.50 | 15.88 ± 3.00 ** | 16.83 ± 2.53 ** | ||
| Changes from baseline | P | 2.20 ± 3.83 | 2.24 ± 3.65 | ||
| W | 1.44 ± 3.51 | 2.40 ± 3.66 | |||
| VFT (verbal fluency test) | |||||
| Beginning with “a” | Score | P | 12.1 ± 3.3 | 13.1 ± 3.6 * | 13.7 ± 3.8 ** |
| W | 11.4 ± 4.1 | 13.2 ± 3.9 ** | 14.1 ± 4.1 ** | ||
| Changes from baseline | P | 1.0 ± 2.8 | 1.7 ± 3.1 | ||
| W | 1.9 ± 3.3 | 2.8 ± 3.1 | |||
| Animal | Score | P | 19.5 ± 4.4 | 19.6 ± 4.7 | 20.9 ± 3.9 * |
| W | 18.3 ± 4.1 | 19.4 ± 4.0 * | 20.1 ± 4.6 ** | ||
| Changes from baseline | P | 0.2 ± 3.7 | 1.4 ± 3.9 | ||
| W | 1.2 ± 3.2 | 1.9 ± 3.9 | |||
| Test | Group | Week 0 (Baseline) | Week 6 | Week 12 | |
|---|---|---|---|---|---|
| Stroop test | |||||
| Step 3 error numbers | Score | P | 0.0 ± 0.1 | 0.2 ± 0.9 | 0.1 ± 0.3 |
| W | 0.1 ± 0.3 | 0.0 ± 0.2 | 0.1 ± 0.3 | ||
| Changes from baseline | P | 0.1 ± 0.9 | 0.1 ± 0.3 | ||
| W | 0.0 ± 0.4 | 0.0 ± 0.5 | |||
| Step 3 reading time (second) | Score | P | 45.6 ± 7.1 | 42.9 ± 8.1 ** | 41.0 ± 7.5 ** |
| W | 44.8 ± 10.7 | 42.4 ± 9.6 ** | 40.9 ± 7.8 ** | ||
| Changes from baseline | P | −2.7 ± 6.0 | −4.6 ± 6.9 | ||
| W | −2.4 ± 5.8 | −3.9 ± 8.2 | |||
| Step 4 error numbers | Score | P | 0.1 ± 0.3 | 0.1 ± 0.4 | 0.2 ± 0.7 |
| W | 0.2 ± 0.5 | 0.2 ± 0.4 | 0.2 ± 0.6 | ||
| Changes from baseline | P | 0.0 ± 0.4 | 0.1 ± 0.7 | ||
| W | 0.0 ± 0.6 | 0.0 ± 0.6 | |||
| Step 4 reading time (second) | Score | P | 59.5 ± 15.4 | 53.5 ± 9.9 ** | 50.8 ± 12.0 ** |
| W | 57.2 ± 11.4 | 52.0 ± 10.1 ** | 49.7 ± 8.5 ** | ||
| Changes from baseline | P | −6.1 ± 10.8 | −8.7 ± 12.4 | ||
| W | −5.2 ± 6.8 | −7.5 ± 7.1 | |||
| Digit Span | |||||
| Spans | Score | P | 6.1 ± 1.1 | 6.4 ± 1.2 * | 6.6 ± 1.4 ** |
| W | 6.2 ± 1.2 | 6.3 ± 1.1 | 6.6 ± 1.1* | ||
| Changes from baseline | P | 0.3 ± 1.0 | 0.5 ± 1.1 | ||
| W | 0.1 ± 1.1 | 0.4 ± 1.1 | |||
| PASAT (paced auditory serial addition test) | |||||
| Accuracy (%) | Score | P | 68.8 ± 16.0 | 77.4 ± 16.6 ** | 83.1 ± 11.7 ** |
| W | 70.0 ± 16.0 | 76.4 ± 14.8 ** | 78.4 ± 19.6 ** | ||
| Changes from baseline | P | 8.6 ± 12.3 | 14.2 ± 11.8 | ||
| W | 6.4 ± 12.7 | 8.4 ± 18.1 | |||
| Test | Group | Week 6 | Week 12 | Week 6 | Week 12 | |
|---|---|---|---|---|---|---|
| VFT | High fatigue | Low fatigue | ||||
| Beginning with “a” | Changes from baseline | P | 1.0 ± 3.7 | 1.3 ± 3.6 | 1.1 ± 2.2 * | 2.0 ± 2.8 ** |
| W | 3.3 ± 2.5 **,# | 2.6 ± 3.0 ** | 0.9 ± 3.5 | 2.8 ± 3.2 ** | ||
| Animal | Changes from baseline | P | −0.6 ± 4.2 | 0.5 ± 3.7 | 0.7 ± 3.3 | 2.0 ± 3.9 ** |
| W | 1.3 ± 2.6 * | 0.8 ± 4.5 | 1.1 ± 3.6 | 2.5 ± 3.4 ** | ||
| Stroop test | High fatigue | Low fatigue | ||||
| Step 3 error numbers | Changes from baseline | P | 0.1 ± 0.3 | 0.0 ± 0.2 | 0.2 ± 1.1 | 0.1 ± 0.4 |
| W | −0.1 ± 0.3 # | −0.1 ± 0.3 | 0.0 ± 0.4 | 0.1 ± 0.5 | ||
| Step 4 error numbers | Changes from baseline | P | 0.1 ± 0.4 | 0.3 ± 1.0 | 0.0 ± 0.4 | 0.0 ± 0.4 |
| W | −0.1 ± 0.2 | 0.0 ± 0.5 | 0.0 ± 0.7 | 0.0 ± 0.7 |
| Test | Group | Week 6 | Week 12 | Week 6 | Week 12 | |
|---|---|---|---|---|---|---|
| VFT | High fatigue | Low fatigue | ||||
| Beginning with “a” | Changes from baseline | P | 0.8 ± 2.4 | 2.7 ± 3.1 ** | 1.1 ± 3.0 * | 1.3 ± 3.1 * |
| W | 3.1 ± 2.9 **,# | 4.1 ± 3.7 ** | 1.4 ± 3.4 * | 2.3 ± 2.8 ** | ||
| Animal | Changes from baseline | P | −1.2 ± 3.5 | 1.1 ± 3.5 | 0.7 ± 3.7 | 1.5 ± 4.0 * |
| W | 1.2 ± 2.7 | 2.3 ± 4.6 | 1.2 ± 3.3 * | 1.7 ± 3.7 ** | ||
| Stroop test | High fatigue | Low fatigue | ||||
| Step 3 error numbers | Changes from baseline | P | 0.5 ± 1.7 | 0.0 ± 0.0 | 0.0 ± 0.2 | 0.1 ± 0.4 |
| W | −0.2 ± 0.4 | −0.1 ± 0.5 | 0.0 ± 0.3 | 0.0 ± 0.4 | ||
| Step 4 error numbers | Changes from baseline | P | 0.0 ± 0.6 | −0.1 ± 0.5 | 0.0 ± 0.4 | 0.2 ± 0.8 |
| W | 0.0 ± 0.0 | 0.3 ± 0.9 | −0.1 ± 0.7 | −0.1 ± 0.5 # |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kita, M.; Obara, K.; Kondo, S.; Umeda, S.; Ano, Y. Effect of Supplementation of a Whey Peptide Rich in Tryptophan-Tyrosine-Related Peptides on Cognitive Performance in Healthy Adults: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2018, 10, 899. https://doi.org/10.3390/nu10070899
Kita M, Obara K, Kondo S, Umeda S, Ano Y. Effect of Supplementation of a Whey Peptide Rich in Tryptophan-Tyrosine-Related Peptides on Cognitive Performance in Healthy Adults: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients. 2018; 10(7):899. https://doi.org/10.3390/nu10070899
Chicago/Turabian StyleKita, Masahiro, Kuniaki Obara, Sumio Kondo, Satoshi Umeda, and Yasuhisa Ano. 2018. "Effect of Supplementation of a Whey Peptide Rich in Tryptophan-Tyrosine-Related Peptides on Cognitive Performance in Healthy Adults: A Randomized, Double-Blind, Placebo-Controlled Study" Nutrients 10, no. 7: 899. https://doi.org/10.3390/nu10070899
APA StyleKita, M., Obara, K., Kondo, S., Umeda, S., & Ano, Y. (2018). Effect of Supplementation of a Whey Peptide Rich in Tryptophan-Tyrosine-Related Peptides on Cognitive Performance in Healthy Adults: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients, 10(7), 899. https://doi.org/10.3390/nu10070899