
Effects of Whole-Body Stretching Exercise during Lunch Break for Reducing Musculoskeletal Pain and Physical Exertion among Healthcare Professionals

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
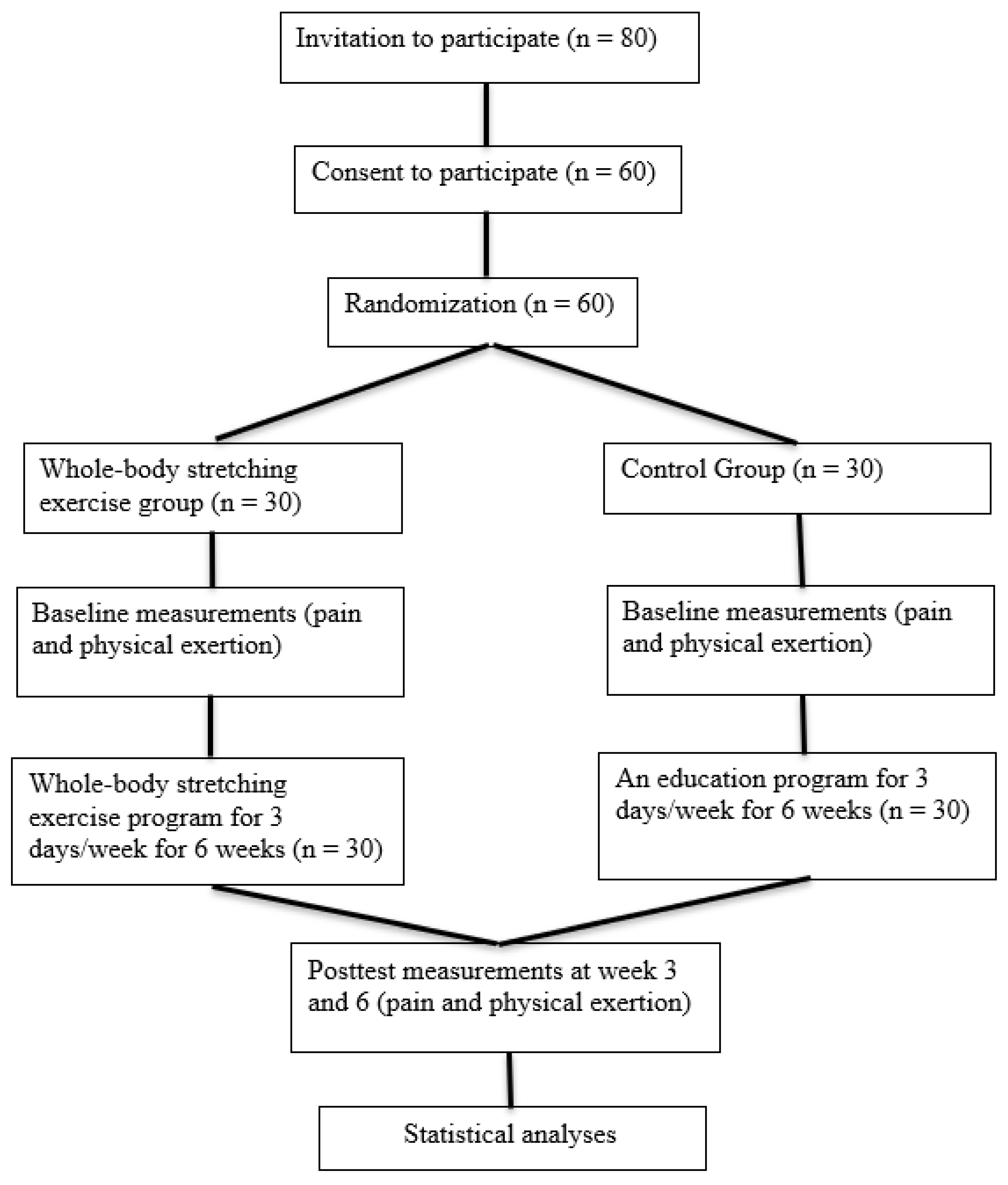
2.1. Study Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hosseini, E.; Sharifian, R.; Bashiri, A.; Daneshmandi, H. Effect of a Developed Nursing Stretch Break Application on Work-Related Musculoskeletal Complications and Fatigue among Nurses: An Interventional Study. Pain Res. Manag. 2022, 2022, 7870177. [Google Scholar] [CrossRef]
- Iqbal, M.U.; Ahmad, N.; Khan, Z.S.U.; Awan, M.; Zafar, I.; Safdar, G.; Altaf, S.; Sajjad, A.G.; Kiyani, M.M. Prevalence of musculoskeletal disorders among chefs working in restaurants of twins cities of Pakistan. Work 2023, 74, 1507–1513. [Google Scholar] [CrossRef]
- Atia, D.T.; Elsayed, N.I.; Abdelmonem, A.F.; Mahmoud, S.M.S.; Mahmoud, M.M.M.; Mohamed, K.E.S.; Turky, K.T.Y.; Rashad, U.M.; Abdel Karim, A.E. Prevalence of Musculoskeletal Disorders among General and Technical Secondary School Students in Egypt. Int. J. Environ. Res. Public Health 2023, 20, 1465. [Google Scholar] [CrossRef] [PubMed]
- Piranveyseh, P.; Motamedzade, M.; Osatuke, K.; Mohammadfam, I.; Moghimbeigi, A.; Soltanzadeh, A.; Mohammadi, H. Association between psychosocial, organizational and personal factors and prevalence of musculoskeletal disorders in office workers. Int. J. Occup. Saf. Ergon. 2016, 22, 267–273. [Google Scholar] [CrossRef]
- Yasobant, S.; Rajkumar, P. Health of the healthcare professionals: A risk assessment study on work-related musculoskeletal disorders in a tertiary hospital, Chennai, India. Int. J. Med. Public Health 2015, 5, 189–195. [Google Scholar] [CrossRef]
- Almhdawi, K.A.; Mathiowetz, V.; Al-Hourani, Z.; Khader, Y.; Kanaan, S.F.; Alhasan, M. Musculoskeletal pain symptoms among allied health professions’ students: Prevalence rates and associated factors. J. Back Musculoskelet. Rehabil. 2017, 30, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Çınar-Medeni, Ö.; Elbasan, B.; Duzgun, I. Low back pain prevalence in healthcare professionals and identification of factors affecting low back pain. J. Back Musculoskelet. Rehabil. 2017, 30, 451–459. [Google Scholar] [CrossRef]
- Nuernberg Back, C.G.; Liebano, R.E.; Avila, M.A. Perspectives of implementing the biopsychosocial model to treat chronic musculoskeletal pain in primary health care. Pain Manag. 2021, 11, 217–225. [Google Scholar] [CrossRef]
- Roffey, D.M.; Wai, E.K.; Bishop, P.; Kwon, B.K.; Dagenais, S. Causal assessment of workplace manual handling or assisting patients and low back pain: Results of a systematic review. Spine J. 2010, 10, 639–651. [Google Scholar] [CrossRef]
- Asghari, E.; Dianat, I.; Abdollahzadeh, F.; Mohammadi, F.; Asghari, P.; Jafarabadi, M.A.; Castellucci, H.I. Musculoskeletal pain in operating room nurses: Associations with quality of work life, working posture, socio-demographic and job characteristics. Int. J. Ind. Ergon. 2019, 72, 330–337. [Google Scholar] [CrossRef]
- Suganthirababu, P.; Parveen, A.; Mohan Krishna, P.; Sivaram, B.; Kumaresan, A.; Srinivasan, V.; Vishnuram, S.; Alagesan, J.; Prathap, L. Prevalence of work-related musculoskeletal disorders among health care professionals: A systematic review. Work 2023, 74, 455–467. [Google Scholar] [CrossRef]
- Seaton, J.; Jones, A.; Johnston, C.; Francis, K. Allied health professionals’ perceptions of interprofessional collaboration in primary health care: An integrative review. J. Interprof. Care 2021, 35, 217–228. [Google Scholar] [CrossRef]
- Dawson, A.P.; McLennan, S.N.; Schiller, S.D.; Jull, G.A.; Hodges, P.W.; Stewart, S. Interventions to prevent back pain and back injury in nurses: A systematic review. Occup. Environ. Med. 2007, 64, 642–650. [Google Scholar] [CrossRef]
- Gropelli, T.M.; Corle, K. Nur’es’ and therapi’ts’ experiences with occupational musculoskeletal injuries. AAOHN J. 2010, 58, 159–166. [Google Scholar]
- Hignett, S. Intervention strategies to reduce musculoskeletal injuries associated with handling patients: A systematic review. Occup. Environ. Med. 2003, 60, e6. [Google Scholar] [CrossRef]
- Macdonald, W.; Evans, O.; Armstrong, R. Research on the prevention of musculoskeletal disorders-stage 2. A study of a small smale of workpaces in high risk industries. Dep. Employ. Workplace Relat. Proj. No. CIR 2008, 1001439, 072007. [Google Scholar]
- MacDonald, W. Workload, stress and pychosocial factors as hazards for musculoskeletal disorders: Special issue: OHS Practitioners: Adapting to a Changing World of Work and Risk. J. Occup. Health Saf. 2004, 20, 37–47. [Google Scholar]
- Kumar, S. A conceptual model of oxerexertion, safety, and risk of injury in occupational settings. Hum. Factors 1994, 36, 197–209. [Google Scholar] [CrossRef]
- Jang, Y.; Chi, C.F.; Tsauo, J.Y.; Wang, J.D. Prevalence and risk factors of work-related musculoskeletal disorders in massage practitioners. J. Occup. Rehabil. 2006, 16, 416–429. [Google Scholar] [CrossRef]
- Kallistratos, E.; Kallistratou, A.; Toliopoulos, J. Attitudes to work and work environment management in lifetime practice: A questionnaire-based study for physiotherapists working in the private sector in Greece. Int. J. Health Sci. 2009, 2, 184–190. [Google Scholar]
- Rozenfeld, V.; Ribak, J.; Danziger, J.; Tsamir, J.; Carmeli, E. Prevalence, risk factors and preventive strategies in work-related musculoskeletal disorders among Israeli physical therapists. Physiother. Res. Int. 2010, 15, 176–184. [Google Scholar] [CrossRef]
- Mikołajewska, E. Work-related musculoskeletal injuries in physiotherapists. Med. Pr. 2014, 64, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.; Burdorf, A.; Stynes, S.M.; de Vet, H.C.; Koes, B.W. Conservative interventions for treating work-related complaints of the arm, neck or shoulder in adults. Cochrane Database Syst. Rev. 2013, 2013, CD008742. [Google Scholar] [CrossRef]
- Montano, D.; Hoven, H.; Siegrist, J. A meta-analysis of health effects of randomized controlled worksite interventions: Does social stratification matter? Scand. J. Work. Environ. Health 2014, 40, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Nastasia, I.; Coutu, M.F.; Tcaciuc, R. Topics and trends in research on non-clinical interventions aimed at preventing prolonged work disability in workers compensated for work-related musculoskeletal disorders (WRMSDs): A systematic, comprehensive literature review. Disabil. Rehabil. 2014, 36, 1841–1856. [Google Scholar] [CrossRef]
- Choi, S.D.; Woletz, T. Do stretching programs prevent work-related musculoskeletal disorders? J. Saf. Health Environ. Res. 2010, 6, 1–19. [Google Scholar]
- Sirisawasd, S.; Taptagaporn, S.; Boonshuyar, C.; Earde, P. Interventions commonly used to prevent work-related musculoskeletal disorders among healthcare workers. J. Health Res. 2018, 32, 371–383. [Google Scholar] [CrossRef]
- McDonald, M.; Salisbury, H. Physical activity, exercise, and musculoskeletal disorders in sonographers. J. Diagn. Med. Sonogr. 2019, 35, 305–315. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Healy, G.N.; Eakin, E.G.; Lamontagne, A.D.; Owen, N.; Winkler, W.A.; Wiesner, G.; Gunning, L.; Neuhaus, M.; Lawler, S.; Fjeldsoe, B.S.; et al. Reducing sitting time in office workers: Short-term efficacy of a multicomponent intervention. Prev. Med. 2013, 27, 43–48. [Google Scholar] [CrossRef]
- Shrestha, N.; Ijaz, S.; Kukkonen-Harjula, K.T.; Kumar, S.; Nwankwo, C.P. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2015, 6, 26. [Google Scholar] [CrossRef]
- Commissaris, D.A.; Huysmans, M.A.; Mathiassen, S.E.; Srinivasan, D.; Koppes, L.; Hendriksen, I.J. Interventions to reduce sedentary behavior and increase physical activity during productive work: A systematic review. Scand. J. Work. Environ. Health 2016, 42, 181–191. [Google Scholar] [CrossRef]
- Demou, E.; MacLean, A.; Cheripelli, L.J.; Hunt, K.; Gray, C.M. Group-based healthy lifestyle workplace interventions for shift workers: A systematic review. Scand. J. Work. Environ. Health 2018, 44, 568. [Google Scholar] [CrossRef] [PubMed]
- Sundstrup, E.; Seeberg, K.G.V.; Bengtsen, E.; Andersen, L.L. A systematic review of workplace interventions to rehabilitate musculoskeletal disorders among employees with physical demanding work. J. Occup. Rehabil. 2020, 30, 588–612. [Google Scholar] [CrossRef]
- Worley, V.; Fraser, P.; Allender, S.; Bolton, K.A. Describing workplace interventions aimed to improve health of staff in hospital settings—A systematic review. BMC Health Serv. Res. 2022, 22, 459. [Google Scholar] [CrossRef]
- Sa’adah, H.D. Andomingaruh landomifleksi william (stretching) terhadap tingkat nyeri punggung bawah pada lansia di Posyandu Lansia RW 2 Desa Kedungkandang Malang. J. Sain Med. 2018, 5, 56–61. [Google Scholar]
- Kusuma, H.; Setiowati, A. Pengaruh William Flexion Exercise Terhadap Peningkatan Lingkup Gerak Sendi Penderita Low Back Pain. J. Sport Sci. Fit. 2015, 4, 16–21. [Google Scholar] [CrossRef]
- Ratu, J.M. Ergo-Physiology Decreases Work Postur Risk and LBP in Red Land Workers in Bosen Village, North Mollo Sub-District, South Central Timor District. Log. J. Ranc. Bangun Dan Teknol. 2018, 18, 92–97. [Google Scholar]
- Matsuo, S.; Suzuki, S.; Iwata, M.; Hatano, G.; Nosaka, K. Changes in force and stiffness after static stretching of eccentrically-damaged hamstrings. Eur. J. Appl. Physiol. 2015, 115, 981–991. [Google Scholar] [CrossRef]
- Knudson, D.V. Warm-Up and Flexibility. In Conditioning for Strength and Human Performance; Routledge: England, UK, 2018; pp. 212–231. [Google Scholar]
- Behm, D.G.; Chaouachi, A. A review of the acute effects of static and dynamic stretching on performance. Eur. J. Appl. Physiol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef]
- Bingul, B.M.; Son, M.; Aydin, M.; Gelen, E.; Cinel, Y.; Bulgan, C. The effects of static and dynamic stretching on agility performance. Nigde Univ. J. Phys. Educ. Sport Sci. 2014, 8, 43–48. [Google Scholar]
- Susanto, B. Perbedaan Antara Aquatic Exercise Dengan Mckenzie Exercise Dalam Menurunkan Disabilitas Pada Penderita Discogenic Low Back Pain. J. Syntax Transform. 2020, 1, 20–31. [Google Scholar] [CrossRef]
- Taylor, W.C. Transforming work breaks to promote health. Am. J. Prev. Med. 2005, 29, 461–465. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for offandomizeds—A randomised controlled trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef]
- Kett, A.R.; Sichting, F. Sedentary behaviour at work increases muscle stiffness of the back: Why roller massage has potential as an active break intervention. Appl. Ergon. 2020, 82, 102947. [Google Scholar] [CrossRef]
- Henning, R.A.; Jacques, P.; Kissel, G.V.; Sullivan, A.B.; Alteras-Webb, S.M. Frequent short rest breaks from computer work: Effects on productivity and well-being at two field sites. Ergonomics 1997, 40, 78–91. [Google Scholar] [CrossRef]
- Andersen, L.L.; Christensen, K.B.; Holtermann, A.; Poulsen, O.M.; Sjøgaard, G.; Pedersen, M.T.; Hansen, E.A. Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: A one-year randomized controlled trial. Man. Ther. 2010, 15, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Lidegaard, M.; Jensen, R.B.; Andersen, C.H.; Zebis, M.K.; Colado, J.C.; Wang, Y.; Heilskov-Hansen, T.; Andersen, L.L. Effect of brief daily resistance training on occupational neck/shoulder muscle activity in office workers with chronic pain: Randomized controlled trial. Biomed Res. Int. 2013, 2013, 262386. [Google Scholar] [CrossRef] [PubMed]
- Waongenngarm, P.; Areerak, K.; Janwantanakul, P. The effects of breaks on low back pain, discomfort, and work productivity in office workers: A systematic review of randomized and non-randomized controlled trials. Appl. Ergon. 2018, 68, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Marangoni, A.H. Effects of intermittent stretching exercises at work on musculoskeletal pain associated with the use of a personal computer and the influence of media on outcomes. Work 2010, 36, 27–37. [Google Scholar] [CrossRef]
- Macedo, A.C.; Trindade, C.S.; Brito, A.P.; Socorro Dantas, M. On the effects of a workplace fitness program upon pain perception: A case study encompassing office workers in a Portuguese context. J. Occup. Rehabil. 2011, 21, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Freitas-Swerts, F.C.T.D.; Robazzi, M.L.D.C.C. The effects of compensatory workplace exercises to reduce work-related stress and musculoskeletal pain. Rev. Lat.-Am. De Enferm. 2014, 22, 629–636. [Google Scholar] [CrossRef]
- Gasibat, Q.; Simbak, N.B.; Aziz, A.A.; Petridis, L.; Tróznai, Z. Stretching exercises to prevent work-related musculoskeletal disorders: A review article. AJSSM 2017, 5, 27–37. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting pandomizedoup randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Sil, A.; Kumar, P.; Kumar, R.; Das, N.K. Selection of control, randomization, blinding, and allocation concealment. Indian Dermatol. Online J. 2019, 10, 601. [Google Scholar]
- Franco, B.L.; Signorelli, G.R.; Trajano, G.S.; de Oliveira, C.G. Acute effects of different stretching exercises on muscular endurance. J. Strength Cond. Res. 2008, 22, 1832–1837. [Google Scholar] [CrossRef] [PubMed]
- Bolbol, S.A.; El-Shafei, D.A.; Abdelsalam, A.E.; Abdelsalam, N.M.; Alian, S.M. Work-related musculoskeletal disorders: An ergonomic intervention program among Al-Ahrar Hospital intensive care units nurses. Egypt. J. Occup. Med. 2017, 41, 429–446. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Shadbolt, N.; Burton, A.M.; Wilson, J.; Corlett, N. Evaluation of Human Work: A Practical Ergonomics Methodology, 1st ed.; Taylor and Francis: London, UK, 1990; pp. 563–568. [Google Scholar]
- Crawford, J.O. The Nordic musculoskeletal questionnaire. Occup. Med. 2007, 57, 300–301. [Google Scholar] [CrossRef]
- Borg, G. Ratings of perceived exertion and heart rates during short-term cycle exercise and their use in a new cycling strength test. Int. J. Sport. Med. 1982, 3, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.; Jung, J.W. Validity of Borg’s category ratio 10 scale during maximal-graded exercise testing. Exerc. Sci. 2016, 25, 92–99. [Google Scholar] [CrossRef]
- Williams, N. The Borg rating of perceived exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- Cabral, L.L.; Lopes, P.B.; Wolf, R.; Stefanello, J.M.F.; Pereira, G. A systematic review of cross-cultural adaptation and validation of Borg’s rating of perceived exertion scale. J. Phys. Educ. 2018, 28, 10422. [Google Scholar] [CrossRef]
- Chang, S.F.; Lin, P.C.; Yang, R.S.; Yang, R.J. The preliminary effect of whole-body vibration intervention on improving the skeletal muscle mass index, physical fitness, and quality of life among older people with sarcopenia. BMC Geriatr. 2018, 18, 17. [Google Scholar] [CrossRef]
- Lindegård, A.; Wahlström, J.; Hagberg, M.; Vilhelmsson, R.; Toomingas, A.; Wigaeus Tornqvist, E. Perceived exertion, comfort and working technique in professional computer users and associations with the incidence of neck and upper extremity symptoms. BMC Musculoskelet. Disord. 2012, 13, 38. [Google Scholar] [CrossRef]
- Akodu, A.K.; Akinbo, S.R.; Young, Q.O. Correlation among smartphone addiction, craniovertebral angle, scapular dyskinesis, and selected anthropometric variables in physiotherapy undergraduates. J. Taibah Univ. Med. Sci. 2018, 13, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Cruder, C.; Falla, D.; Mangili, F.; Azzimonti, L.; Araújo, L.S.; Williamon, A.; Barbero, M. Profiling the location and extent of musicians’ pain using digital pain drawings. Pain Pract. 2018, 18, 53–66. [Google Scholar] [CrossRef]
- Moreira-Silva, I.; Queirós, R.; Seixas, A.; Cardoso, R.; Ventura, N.; Azevedo, J. Prevalence of Musculoskeletal Symptoms among Portuguese Call Center Operators: Associations with Gender 2014, Body Mass Index and Hours of Work. In Occupational and Environmental Safety and Health III; Springer International Publishing: Cham, Switzerland, 2021; pp. 207–214. [Google Scholar]
- Vieira, E.R.; Kumar, S.; Coury, H.J.; Narayan, Y. Low back problems and possible improvements in nursing jobs. J. Adv. Nurs. 2006, 55, 79–89. [Google Scholar] [CrossRef]
- Wilhelmus Johannes Andreas, G.; Wernstedt, P.; Campo, M. Work-related musculoskeletal disorders in female Swedish physical therapists with more than 15 years of job experience: Prevalence and associations with work exposures. Physiother. Theory Pract. 2011, 27, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Salik, Y.; Özcan, A. Work-related musculoskeletal disorders: A survey of physical therapists in Izmir-Turkey. BMC Musculoskelet. Disord. 2004, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.R.; Svoboda, S.; Belniak, A.; Brunt, D.; Rose-St Prix, C.; Roberts, L.; da Costa, B.R. Work-related musculoskeletal disorders among physical therapists: An online survey. Disabil. Rehabil. 2016, 38, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Chowdhury, A.; Zaman, M.S.; Sultana, N.; Amin, M.B.; Hossain, M.M. Work-related musculoskeletal disorders among health care professionals. Update Dent. Coll. J. 2017, 7, 4–9. [Google Scholar] [CrossRef]
- Karahan, A.; Kav, S.; Abbasoglu, A.; Dogan, N. Low back pain: Prevalence and associated risk factors among hospital staff. J. Adv. Nurs. 2009, 65, 516–524. [Google Scholar] [CrossRef]
- Yasobant, S.; Rajkumar, P. Work-related musculoskeletal disorders among health care professionals: A cross-sectional assessment of risk factors in a tertiary hospital, India. Indian J. Occup. Environ. Med. 2014, 18, 75. [Google Scholar] [CrossRef]
- Lacaze, D.H.D.C.; Sacco, I.D.C.; Rocha, L.E.; Pereira, C.A.D.B.; Casarotto, R.A. Stretching and joint mobilization exercises reduce call-cente’ operat’rs’ musculoskeletal discomfort and fatigue. Clinics 2010, 65, 657–662. [Google Scholar] [CrossRef]
- McHugh, M.P.; Cosgrave, C.H. To stretch or not to stretch: The role of stretching in injury prevention and performance. Scand. J. Med. Sci. Sport. 2010, 20, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.H.; Kim, H.; Jung, G.P.; Ko, J.Y.; Ryu, J.S. The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine 2019, 98, e16173. [Google Scholar] [CrossRef] [PubMed]
- Boonchum, H.; Bovonsunthonchai, S.; Sinsurin, K.; Kunanusornchai, W. Effect of a home-based stretching exercise on multi-segmental foot motion and clinical outcomes in patients with plantar fasciitis. J. Musculoskelet. Neuronal Interact. 2020, 20, 411. [Google Scholar] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, CD011279. [Google Scholar] [PubMed]
- Rasotto, C.; Bergamin, M.; Simonetti, A.; Maso, S.; Bartolucci, G.B.; Ermolao, A.; Zaccaria, M. Tailored exercise program reduces symptoms of upper limb work-related musculoskeletal disorders in a group of metalworkers: A randomized controlled trial. Man. Ther. 2015, 20, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Machado-Matos, M.; Arezes, P.M. Impact of a workplace exercise program on neck and shoulder segments in office workers. Dyna 2016, 83, 63–68. [Google Scholar] [CrossRef]
- Robertson, M.M.; Huang, Y.H.; Larson, N. The relationship among computer work, environmental design, and musculoskeletal and visual discomfort: Examining the moderating role of supervisory relations and co-worker support. Int. Arch. Occup. Environ. Health 2016, 89, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Sihawong, R.; Janwantanakul, P.; Sitthipornvorakul, E.; Pensri, P. Exercise therapy for office workers with nonspecific neck pain: A systematic review. J. Manip. Physiol. Ther. 2011, 34, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Van Eerd, D.; Munhall, C.; Irvin, E.; Rempel, D.; Brewer, S.; van der Beek, A.J.; Dennerlein, J.T.; Tullar, J.; Skivington, K.; Pinion, C.; et al. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: An update of the evidence. Occup. Environ. Med. 2016, 73, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Michishita, R.; Jiang, Y.; Ariyoshi, D.; Yoshida, M.; Moriyama, H.; Yamato, H. The practice of active rest by workplace units improves personal relationships, mental health, and physical activity among workers. J. Occup. Health 2017, 59, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Johnston, V.; O’Leary, S.; Comans, T.; Straker, L.; Melloh, M.; Khan, A.; Sjøgaard, G. A workplace exercise versus health promotion intervention to prevent and reduce the economic and personal burden of non-specific neck pain in office personnel: A cluster randomized controlled trial. J. Physiother. 2014, 60, 233. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Stretching Exercise Performed | Description |
|---|---|---|
| 1 | Neck stretch | Flexion, extension, and lateral flexion motions. |
| 2 | Shoulder stretch | Shoulder retraction, protraction, and elevation motions. |
| 3 | Arm curl | Biceps and Triceps stretch |
| 4 | Wrist bend | Wrist Flexor and extensor Stretch |
| 5 | Abdominal bend | Lying back extension |
| 6 | Trunk twist | Lumbar rotation |
| 7 | Hamstring stretch | Standing Hamstring stretch |
| 8 | Quad stretch | Standing Quadriceps stretch |
| 9 | Knee to chest | Back stretching |
| 10 | Side bends | Side stretching |
| 11 | Ankle circles | Ankle movement in circular manner |
| 12 | Ankle pumps | Plantar and dorsiflexor stretch |
| Variables | Frequency (%) |
|---|---|
| Age, mean (SD) | 37.15 (3.9) |
| Gender, | |
| Male | 34 (56.7) |
| Female | 26 (43.3) |
| Height (m), mean (SD) | 1.61 (0.04) |
| Body mass (kg), mean (SD) | 67.8 (6.3) |
| Body mass index (kg/m2) | 26.5 (2.1) |
| Occupation/Job | |
| PT | 12 (20) |
| DT | 8 (13.3) |
| Nurse | 15 (25) |
| LT | 6 (10) |
| OT | 8 (13.3) |
| PSN | 4 (6.7) |
| SN | 4 (6.7) |
| PST | 3 (5) |
| Working experience (months), mean (SD) | 101.5 (39.3) |
| Working hours (per week), mean (SD) | 57.4 (9.1) |
| VAS, mean (SD) | |
| Baseline | 5.7 (1.05) |
| Week 3 | 4.1 (1.03) |
| Week 6 | 2.63 (1.06) |
| Borg RPE, mean (SD) | |
| Baseline | 15.8 (1.6) |
| Week 3 | 13.5 (1.6) |
| Week 6 | 10.9 (1.7) |
| 12-Month Prevalence | 1-Week Prevalence | |
|---|---|---|
| Neck pain in last 12 months | ||
| Yes | 26 (43.3) | 11 (18.3) |
| No | 34 (56.7) | 49 (81.7) |
| Shoulder pain in last 12 months | ||
| Yes | 15 (25) | 7 (11.7) |
| No | 45 (75) | 53 (88.3) |
| Elbows pain in last 12 months | ||
| Yes | 10 (16.7) | 4 (6.7) |
| No | 50 (83.3) | 56 (93.3) |
| Wrist/Hand pain in last 12 months | ||
| Yes | 14 (23.3) | 6 (10) |
| No | 46 (76.7) | 54 (90) |
| Upper back pain in last 12 months | ||
| Yes | 16 (26.7) | 5 (8.3) |
| No | 44 (73.3) | 55 (91.7) |
| Lower back pain in last 12 months | ||
| Yes | 28 (46.7) | 8 (13.3) |
| No | 32 (53.3) | 52 (86.7) |
| One or both Hips/Thighs pain in last 12 months | ||
| Yes | 15 (25) | 4 (6.7) |
| No | 45 (75) | 56 (93.3) |
| One or both Knees pain in last 12 months | ||
| Yes | 17 (28.3) | 7 (11.7) |
| No | 43 (71.7) | 53 (88.3) |
| One or both Ankles/Feet pain in last 12 months | ||
| Yes | 13 (21.7) | 3 (5) |
| No | 47 (78.3) | 57 (95) |
| Frequency (%) | |
|---|---|
| Neck pain prevented work in last 12 months | |
| Yes | 13 (21.7) |
| No | 47 (78.3) |
| Shoulder pain prevented work in last 12 months | |
| Yes | 4 (6.7) |
| No | 56 (93.3) |
| Elbows pain prevented work in last 12 months | |
| Yes | 3 (5) |
| No | 57 (95) |
| Wrist/Hand pain prevented work in last 12 months | |
| Yes | 5 (8.3) |
| No | 55 (91.7) |
| Upper back pain prevented work in last 12 months | |
| Yes | 9 (15) |
| No | 51 (85) |
| Lower back pain prevented work in last 12 months | |
| Yes | 11 (18.3) |
| No | 49 (81.7) |
| Hip/Thigh pain prevented work in last 12 months | |
| Yes | 7 (11.7) |
| No | 53 (88.3) |
| Knee pain prevented work in last 12 months | |
| Yes | 5 (8.3) |
| No | 55 (91.7) |
| Ankle/Feet pain prevented work in last 12 months | |
| Yes | 2 (3.3) |
| No | 58 (96.7) |
| Groups | Baseline (A) Mean (SD) | Week 3 (B) Mean (SD) | Week 6 (C) Mean (SD) | ANOVA | Post hoc Analysis (Bonferroni) | |||
|---|---|---|---|---|---|---|---|---|
| F | * p | A vs. B | A vs. C | B vs. C | ||||
| WBS | 5.97 (1.21) | 3.83 (1.15) | 2.40 (1.16) | 216.213 | 0.001 * | p < 0.05 | p < 0.01 * | p < 0.05 * |
| Control | 5.33 (0.76) | 4.37 (0.76) | 2.87 (0.90) | 174.220 | 0.001 * | p > 0.05 | p < 0.05 * | p < 0.05 * |
| Groups | Baseline (A) Mean (SD) | Week 3 (B) Mean (SD) | Week 6 (C) Mean (SD) | ANOVA | Post hoc Analysis (Bonferroni) | |||
|---|---|---|---|---|---|---|---|---|
| F | * p | A vs. B | A vs. C | B vs. C | ||||
| WBS | 16.13 (1.83) | 13.17 (1.91) | 10.50 (2.33) | 161.140 | 0.001 * | p > 0.05 | p < 0.01 * | p < 0.01 * |
| Control | 15.40 (1.31) | 13.80 (1.89) | 11.40 (1.40) | 286.488 | 0.001 * | p > 0.05 | p < 0.05 * | p < 0.05 * |
| Variables | Type III Sum of Squares | Mean Square | F | p | |
|---|---|---|---|---|---|
| VAS | Time | 232.63 | 116.32 | 352.96 | 0.001 * |
| Time * Group | 1.84 | 0.92 | 3.79 | 0.047 * | |
| Time * Gender | 0.44 | 0.22 | 0.67 | 0.513 | |
| Time * Occupation | 9.13 | 0.65 | 1.98 | 0.029 * | |
| Time * Gender * Occupation | 2.88 | 0.29 | 0.87 | 0.560 | |
| Borg RPE | Time | 586.62 | 293.31 | 406.12 | 0.001 * |
| Time * Group | 6.52 | 3.26 | 4.51 | 0.014 * | |
| Time * Gender | 0.77 | 0.38 | 0.530 | 0.590 | |
| Time * Occupation | 21.62 | 1.54 | 2.14 | 0.017 * | |
| Time * Gender * Occupation | 5.64 | 0.56 | 0.780 | 0.647 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqhtani, R.S.; Ahmed, H.; Alshahrani, A.; Khan, A.R.; Khan, A. Effects of Whole-Body Stretching Exercise during Lunch Break for Reducing Musculoskeletal Pain and Physical Exertion among Healthcare Professionals. Medicina 2023, 59, 910. https://doi.org/10.3390/medicina59050910
Alqhtani RS, Ahmed H, Alshahrani A, Khan AR, Khan A. Effects of Whole-Body Stretching Exercise during Lunch Break for Reducing Musculoskeletal Pain and Physical Exertion among Healthcare Professionals. Medicina. 2023; 59(5):910. https://doi.org/10.3390/medicina59050910
Chicago/Turabian StyleAlqhtani, Raee Saeed, Hashim Ahmed, Adel Alshahrani, Abdur Raheem Khan, and Ashfaque Khan. 2023. "Effects of Whole-Body Stretching Exercise during Lunch Break for Reducing Musculoskeletal Pain and Physical Exertion among Healthcare Professionals" Medicina 59, no. 5: 910. https://doi.org/10.3390/medicina59050910
APA StyleAlqhtani, R. S., Ahmed, H., Alshahrani, A., Khan, A. R., & Khan, A. (2023). Effects of Whole-Body Stretching Exercise during Lunch Break for Reducing Musculoskeletal Pain and Physical Exertion among Healthcare Professionals. Medicina, 59(5), 910. https://doi.org/10.3390/medicina59050910