Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients

 ,
,  ,
, 
Abstract
1. Introduction
1.1. Scientific Background
1.2. Explanation of Rationale
1.3. Objective or Hypotheses
- -
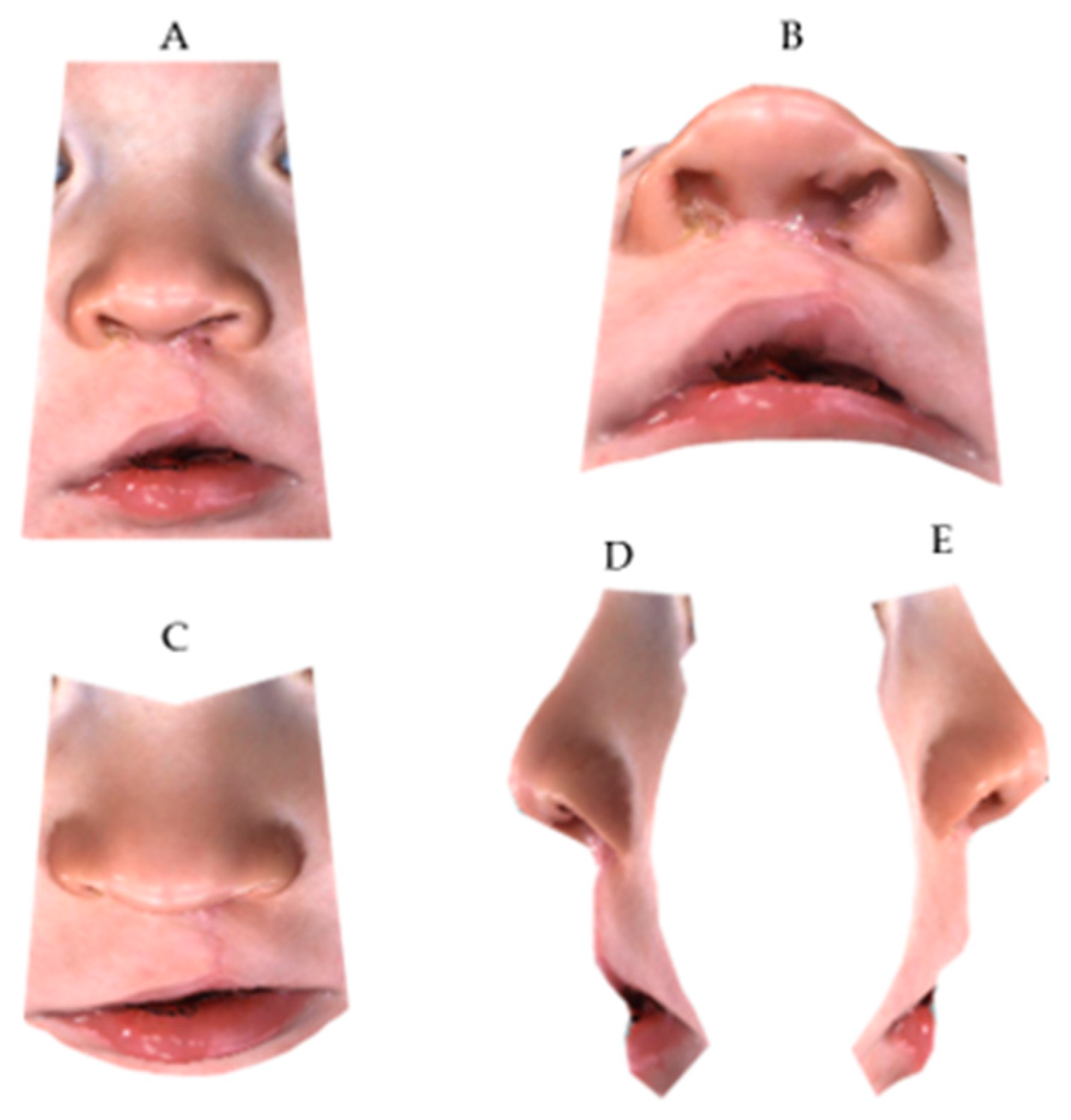
- Primary outcome: How much the aesthetic judgment can be influenced by the complete view of the child’s face as compared to a cropped one, specifically related to the nose and lips (“cropped assessment bias”);
- -
- Secondary outcome: How much the gender of the observer might affect the expression of laypeople judgment (“gender assessment bias”).
- No difference exists between FF or CF 3D images;
- Esthetic evaluation is not dependent on observers’ gender.
2. Materials and Methods
2.1. Trial Design
2.2. Baseline Data
2.3. Data Collection
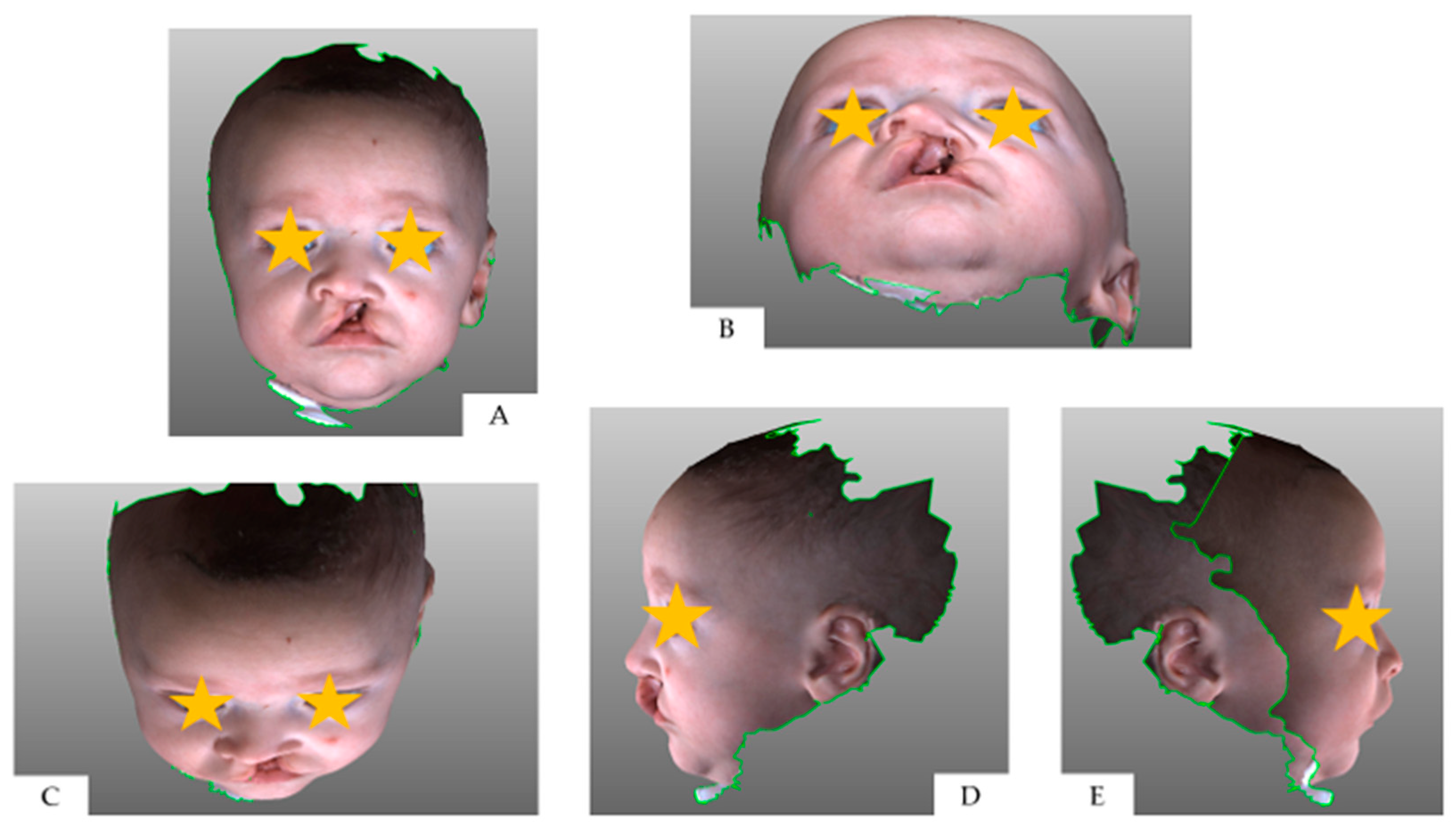
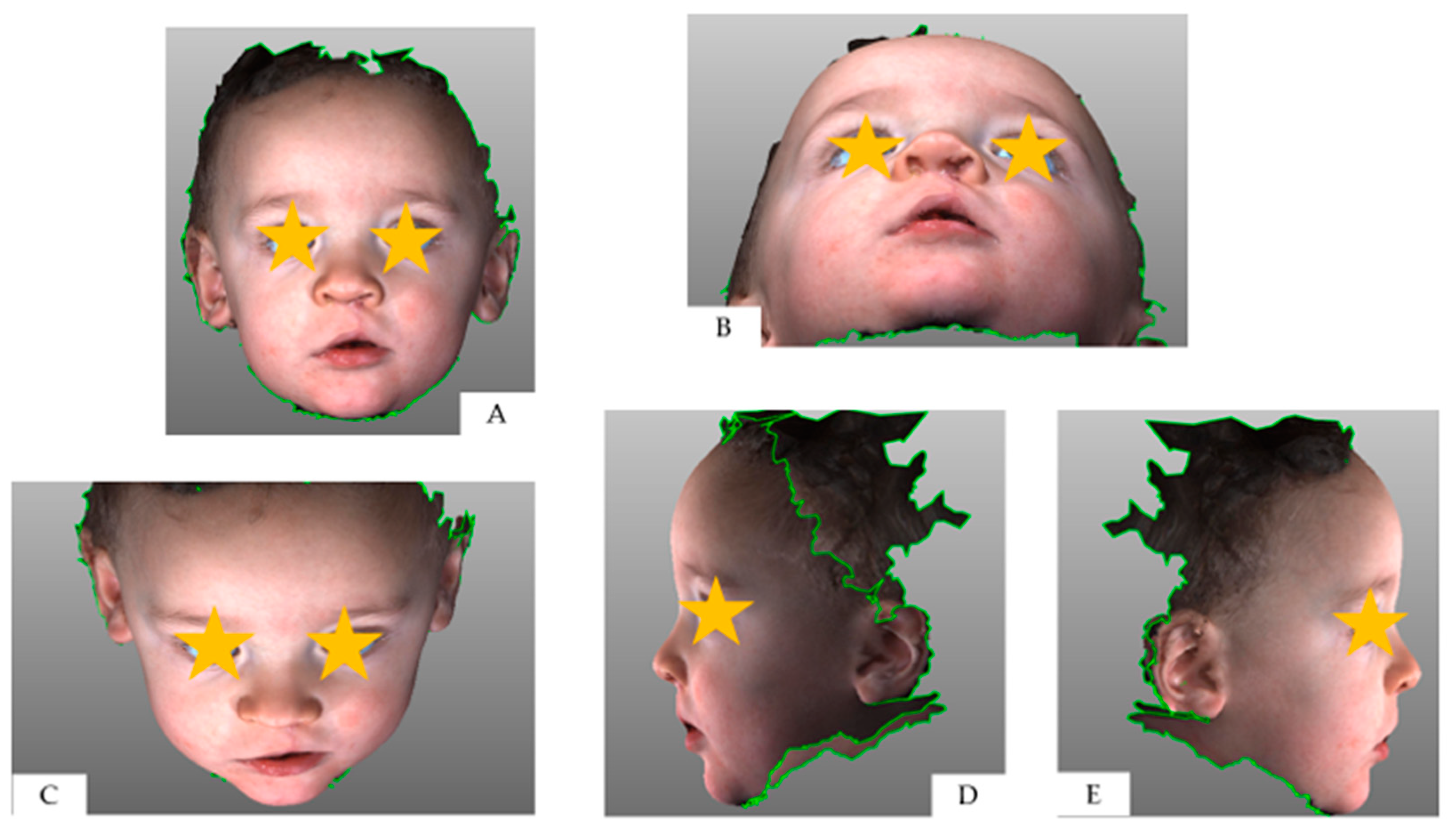
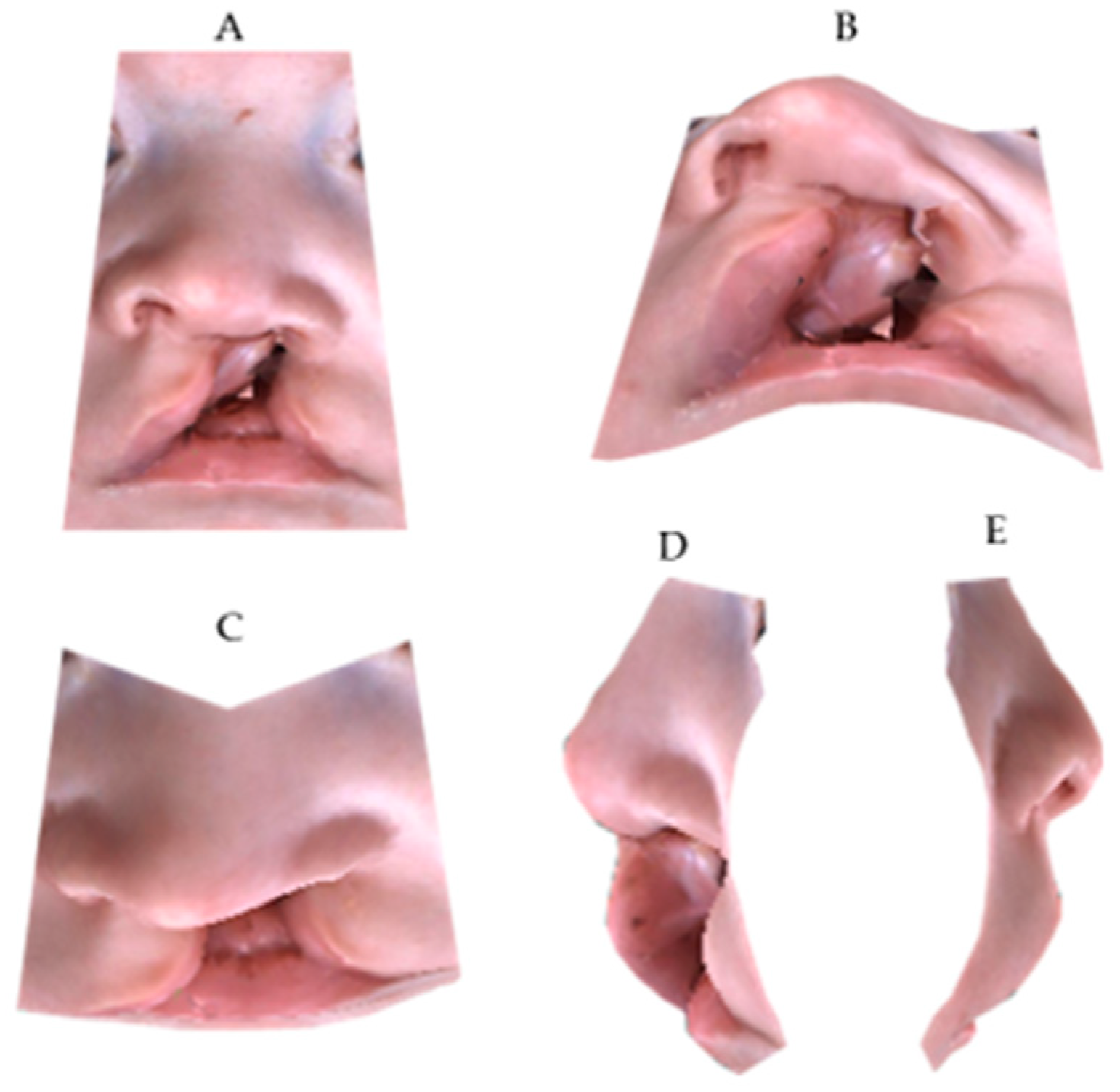
2.4. Data Preparation
2.5. Rating form Design
2.6. Participants—Panel Sample Size and Composition
2.7. Participants—Recruitment
2.8. Blinding
2.9. Outcomes and Estimation—Selection of Assessment Scale
2.10. Evaluation Procedure
2.11. Numbers Analysed
2.12. Statistical Methods
2.12.1. Intra-Examiner Reliability—Primary Outcome
2.12.2. Intra-Examiner Reliability—Secondary Outcome
2.12.3. Inter-Examiner Reliability
3. Results
3.1. Intra-Examiner Reliability—Primary Outcome
3.2. Intra-Examiner Reliability—Secondary Outcome
3.3. Inter-Examiner Reliability
4. Discussion
4.1. Interpretation in the Context of the Available Literature
4.2. Limitations and Strengths
- Answer consecutively, without any leaving blank answer, and successively, filling the rating form in the order proposed in the survey;
- Decide spontaneously; each examiner should ask himself/herself if patients who have unequal esthetics are differently rated in the rating form;
- Check each answer by visualizing the CF and FF 3D model.
- Avoid that judges would discover that CF and FF images were derived from the same patients;
- Eliminate the tendency to avoid extreme response categories (central tendency bias);
- Avoid outguessing.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Zaleckas, L.; Linkeviciene, L.; Olekas, J.; Kutra, N. The comparison of different surgical techniques used for repair of complete unilateral cleft lip. Medicina 2011, 47, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Papamanou, D.A.; Christou, P.; Topouzelis, N. Aesthetic outcome of cleft lip and palate treatment. Perceptions of patients, families, and health professionals compared to the general public. J. Cranio Maxillofac Surg. 2013, 41, e105–e110. [Google Scholar] [CrossRef] [PubMed]
- Molsted, K.; Humerinta, K.; Kuseler, A.; Skaare, P.; Bellardie, H.; Shaw, W.; Karsten, A.; Kare Saele, P.; Rizell, S.; Marcusson, A.; et al. Scandcleft randomised trials of primary surgery for unilateral cleft lip and palate: 8. Assessing naso-labial appearance in 5-year-olds—A preliminary study. J. Plast. Surg. Hand Surg. 2017, 51, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Papamanou, D.A.; Gkantidis, N.; Topouzelis, N.; Christou, P. Appreciation of cleft lip and palate treatment outcome by professionals and laypeople. Eur. J. Orthod. 2012, 34, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Paiva, T.S.; Andre, M.; Paiva, W.S.; Mattos, B.S. Aesthetic evaluation of the nasolabial region in children with unilateral cleft lip and palate comparing expert versus nonexperience health professionals. BioMed Res. Int. 2014, 2014, 460106. [Google Scholar] [CrossRef] [PubMed]
- Schwirtz, R.M.F.; Mulder, F.J.; Mosmuller, D.G.M.; Tan, R.A.; Maal, T.J.; Prahl, C.; de Vet, H.C.W.; Don Griot, J.P.W. Rating nasolabial aesthetics in unilateral cleft lip and palate patients: Cropped versus full-face images. Cleft Palate Craniofac. J. 2018, 55, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, M.; Staudt, C.B.; Pandis, N.; Gnoinski, W.; Eliades, T. Facial attractiveness of patients with unilateral cleft lip and palate and of controls assessed by laypersons and professionals. Eur. J. Orthod. 2014, 36, 284–289. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Three-dimensional assessment of morphological changes following nasoalveolar molding therapy in cleft lip and palate patients: A case report. Dent. J. 2019, 7, 27. [Google Scholar] [CrossRef]
- Shaw, W.C.; Rees, G.; Dawe, M.; Charles, C.R. The influence of dentofacial appearance on the social attractiveness of young adults. Am. J. Orthod. 1985, 87, 21–26. [Google Scholar] [CrossRef]
- Kuijpers, M.A.; Chiu, Y.T.; Nada, R.M.; Carels, C.E.; Fudalej, P.S. Three-dimensional imaging methods for quantitative analysis of facial soft tissues and skeletal morphology in patients with orofacial clefts: A systematic review. PLoS ONE 2014, 9, e93442. [Google Scholar] [CrossRef]
- Moher, D. CONSORT: An evolving tool to help improve the quality of reports of randomized controlled trials. Consolidated Standards of Reporting Trials. JAMA 1998, 279, 1489–1491. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, G.; Doneddu, P.; Gasparini, G.; Staderini, E.; Boniello, R.; Todaro, M.; D’Amato, G.; Pelo, S.; Moro, A. Custom made onlay implants in peek in maxillofacial surgery: A volumetric study. Childs Nerv. Syst. 2019. [Google Scholar] [CrossRef] [PubMed]
- Staderini, E.; Patini, R.; De Luca, M.; Gallenzi, P. Three-dimensional stereophotogrammetric analysis of nasolabial soft tissue effects of rapid maxillary expansion: A systematic review of clinical trials. Acta Otorhinolaryngol. Ital. 2018, 38, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Heike, C.L.; Upson, K.; Stuhaug, E.; Weinberg, S.M. 3D digital stereophotogrammetry: A practical guide to facial image acquisition. Head Face Med. 2010, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Isidor, S.; Di Carlo, G.; Cornelis, M.A.; Isidor, F.; Cattaneo, P.M. Three-dimensional evaluation of changes in upper airway volume in growing skeletal Class II patients following mandibular advancement treatment with functional orthopedic appliances. Angle Orthod. 2018, 88, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Desmedt, D.J.; Maal, T.J.; Kuijpers, M.A.; Bronkhorst, E.M.; Kuijpers-Jagtman, A.M.; Fudalej, P.S. Nasolabial symmetry and esthetics in cleft lip and palate: Analysis of 3D facial images. Clin. Oral. Investig. 2015, 19, 1833–1842. [Google Scholar] [CrossRef] [PubMed]
- Bertens, L.C.; Broekhuizen, B.D.; Naaktgeboren, C.A.; Rutten, F.H.; Hoes, A.W.; van Mourik, Y.; Moons, K.G.; Reitsma, J.B. Use of expert panels to define the reference standard in diagnostic research: A systematic review of published methods and reporting. PLoS Med. 2013, 10, e1001531. [Google Scholar] [CrossRef] [PubMed]
- Asher-McDade, C.; Roberts, C.; Shaw, W.C.; Gallager, C. Development of a method for rating nasolabial appearance in patients with clefts of the lip and palate. Cleft Palate Craniofac. J. 1991, 28, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Tobiasen, J.M.; Hiebert, J.M. Combined effects of severity of cleft impairment and facial attractiveness on social perception: An experimental study. Cleft Palate Craniofac. J. 1993, 30, 82–86. [Google Scholar] [CrossRef]
- Ritter, K.; Trotman, C.A.; Phillips, C. Validity of subjective evaluations for the assessment of lip scarring and impairment. Cleft Palate Craniofac. J. 2002, 39, 587–596. [Google Scholar] [CrossRef]
- Kocher, K.; Kowalski, P.; Kolokitha, O.E.; Katsaros, C.; Fudalej, P.S. Judgment of nasolabial esthetics in cleft lip and palate is not influenced by overall facial attractiveness. Cleft Palate Craniofac. J. 2016, 53, e45–e52. [Google Scholar] [CrossRef] [PubMed]
- Tobiasen, J.M.; Hiebert, J.M.; Boraz, R.A. Development of scales of severity of facial cleft impairment. Cleft Palate Craniofac. J. 1991, 28, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Sinko, K.; Cede, J.; Jagsch, R.; Strohmayr, A.L.; McKay, A.; Mosgoeller, W.; Klug, C. Facial aesthetics in young adults after cleft lip and palate treatment over five decades. Sci. Rep. 2017, 7, 15864. [Google Scholar] [CrossRef] [PubMed]
- Kiekens, R.M.; van ‘t Hof, M.A.; Straatman, H.; Kuijpers-Jagtman, A.M.; Maltha, J.C. Influence of panel composition on aesthetic evaluation of adolescent faces. Eur. J. Orthod. 2007, 29, 95–99. [Google Scholar] [CrossRef]
- Tobiasen, J.M.; Hiebert, J.M. Reliability of esthetic ratings of cleft impairment. Cleft Palate J. 1988, 25, 313–317. [Google Scholar] [PubMed]
- Mercado, A.; Russell, K.; Hathaway, R.; Daskalogiannakis, J.; Sadek, H.; Long, R.E., Jr.; Cohen, M.; Semb, G.; Shaw, W. The Americleft study: An inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 4. Nasolabial aesthetics. Cleft Palate Craniofac. J. 2011, 48, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Brattstrom, V.; Molsted, K.; Prahl-Andersen, B.; Semb, G.; Shaw, W.C. The Eurocleft study: Intercenter study of treatment outcome in patients with complete cleft lip and palate. Part 2: Craniofacial form and nasolabial appearance. Cleft Palate Craniofac. J. 2005, 42, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Mosmuller, D.G.; Griot, J.P.; Bijnen, C.L.; Niessen, F.B. Scoring systems of cleft-related facial deformities: A review of literature. Cleft Palate Craniofac. J. 2013, 50, 286–296. [Google Scholar] [CrossRef]
- McLaughlin, K.; Ainslie, M.; Coderre, S.; Wright, B.; Violato, C. The effect of differential rater function over time (DRIFT) on objective structured clinical examination ratings. Med. Educ. 2009, 43, 989–992. [Google Scholar] [CrossRef]
- Al-Omari, I.; Millett, D.T.; Ayoub, A.F. Methods of assessment of cleft-related facial deformity: A review. Cleft Palate Craniofac. J. 2005, 42, 145–156. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Description |
|---|---|
| Age | Two-three months |
| Surgical technique | Millard’s repair |
| Surgeon | M.Z. 1 |
| Treatment timing | Lip and nasal soft tissue repair at about 10 weeks of life |
| Health status | Absence of syndromic or severely compromised medical conditions for children |
| Medical history | Absence of previous orthopedic or surgical treatments on the oral district |
| Caregivers’ consensus | Decision to participate to the study, to submit the patient at surgical intervention and to follow multiple check-ups from birth onwards |
| Criteria | Description |
|---|---|
| Age | 20–25 years |
| Gender | 25 males and 25 females |
| Educational background | Undergraduate students without extensive professional knowledge on cleft lip and palate patients |
| Health status | Normal visual abilities without contact lenses, not using any medication that could affect vision or attentional control, absence of past or present neurological diseases. |
| Participation to similar studies | Absence of authorship or participation to similar research studies |
| Familiarity | Absence of familiarity or close friendship with UCLP 1 patients |
| Blindness | Blindness about aim of the research, study design and patient’s information. |
| T0 | T1 | T2 | |
|---|---|---|---|
| Question 1 | 0.786 * | 0.690 | 0.659 |
| Question 2 | 0.798 * | 0.728 * | 0.756 * |
| Question 3 | 0.760 * | 0.719 * | 0.789 * |
| Question 4 | 0.781 * | 0.686 | 0.817 * |
| Question 5 | 0.759 * | 0.687 | 0.769 * |
| Question 6 | 0.776 * | 0.732 * | 0.812 * |
| Question 7 | 0.823 * | 0.736 * | 0.737 * |
| Question 8 | - | 0.706 * | 0.791 * |
| Question 9 | - | 0.654 | 0.726 * |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Question 1 | 0.813 * | 0.722 * | 0.710 * | 0.749 * | 0.638 | 0.563 |
| Question 2 | 0.820 * | 0.757 * | 0.800 * | 0.772 * | 0.678 | 0.652 |
| Question 3 | 0.832 * | 0.788 * | 0.824 * | 0.662 | 0.606 | 0.738 * |
| Question 4 | 0.836 * | 0.762 * | 0.845 * | 0.721 * | 0.552 | 0.773 * |
| Question 5 | 0.814 * | 0.734 * | 0.783 * | 0.695 | 0.618 | 0.752 * |
| Question 6 | 0.823 * | 0.788 * | 0.826 * | 0.720 * | 0.646 | 0.792 * |
| Question 7 | 0.854 * | 0.772 * | 0.753 * | 0.789 * | 0.686 | 0.715 * |
| Question 8 | - | 0.731 * | 0.794 * | - | 0.670 | 0.786 * |
| Question 9 | - | 0.726 * | 0.786 * | - | 0.438 | 0.595 |
| Full-Face | Cropped-Face | |||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Question 1 | 0.824 * | 0.849 * | 0.855 * | 0.831 * | 0.872 * | 0.885 * |
| Question 2 | 0.448 | 0.851 * | 0.891 * | 0.553 | 0.868 * | 0.917 * |
| Question 3 | 0.632 | 0.789 * | 0.884 * | 0.502 | 0.853 * | 0.880 * |
| Question 4 | 0.644 | 0.855 * | 0.917 * | 0.491 | 0.864 * | 0.894 * |
| Question 5 | 0.461 | 0.829 * | 0.833 * | 0.476 | 0.812 * | 0.827 * |
| Question 6 | 0.484 | 0.777 * | 0.829 * | 0.395 | 0.818 * | 0.863 * |
| Question 7 | 0.639 | 0.803 * | 0.833 * | 0.598 | 0.813 * | 0.864 * |
| Question 8 | - | 0.817 * | 0.875 * | - | 0.853 * | 0.873 * |
| Question 9 | - | 0.892 * | 0.890 * | - | 0.907 * | 0.891 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staderini, E.; De Luca, M.; Candida, E.; Rizzo, M.I.; Rajabtork Zadeh, O.; Bucci, D.; Zama, M.; Lajolo, C.; Cordaro, M.; Gallenzi, P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina 2019, 55, 576. https://doi.org/10.3390/medicina55090576
Staderini E, De Luca M, Candida E, Rizzo MI, Rajabtork Zadeh O, Bucci D, Zama M, Lajolo C, Cordaro M, Gallenzi P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina. 2019; 55(9):576. https://doi.org/10.3390/medicina55090576
Chicago/Turabian StyleStaderini, Edoardo, Marilisa De Luca, Ettore Candida, Maria Ida Rizzo, Oriana Rajabtork Zadeh, Daria Bucci, Mario Zama, Carlo Lajolo, Massimo Cordaro, and Patrizia Gallenzi. 2019. "Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients" Medicina 55, no. 9: 576. https://doi.org/10.3390/medicina55090576
APA StyleStaderini, E., De Luca, M., Candida, E., Rizzo, M. I., Rajabtork Zadeh, O., Bucci, D., Zama, M., Lajolo, C., Cordaro, M., & Gallenzi, P. (2019). Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina, 55(9), 576. https://doi.org/10.3390/medicina55090576