Effects of Topical Prostaglandin Analog on Macular Thickness Following Cataract Surgery with Postoperative Topical Bromfenac Treatment

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
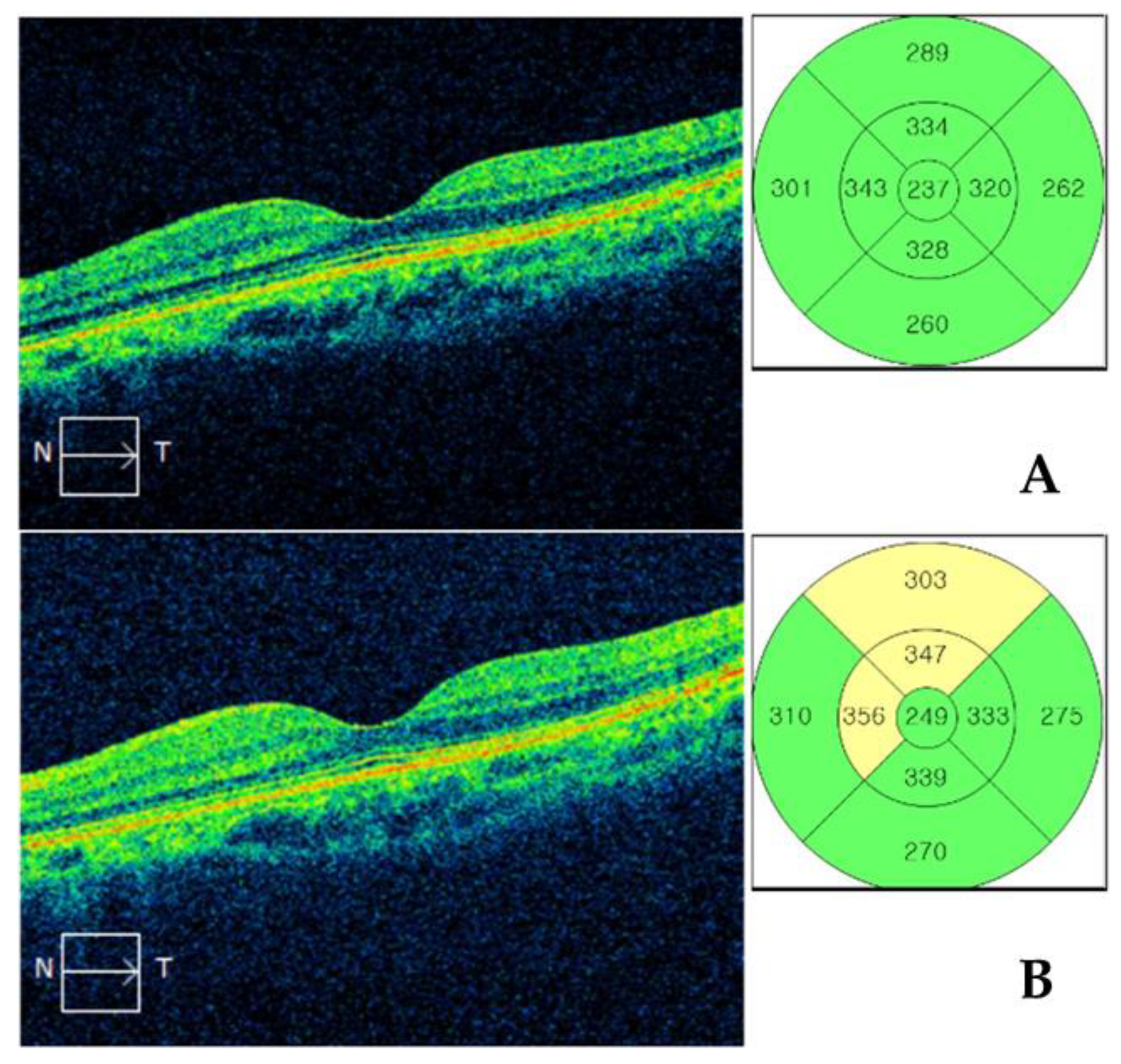
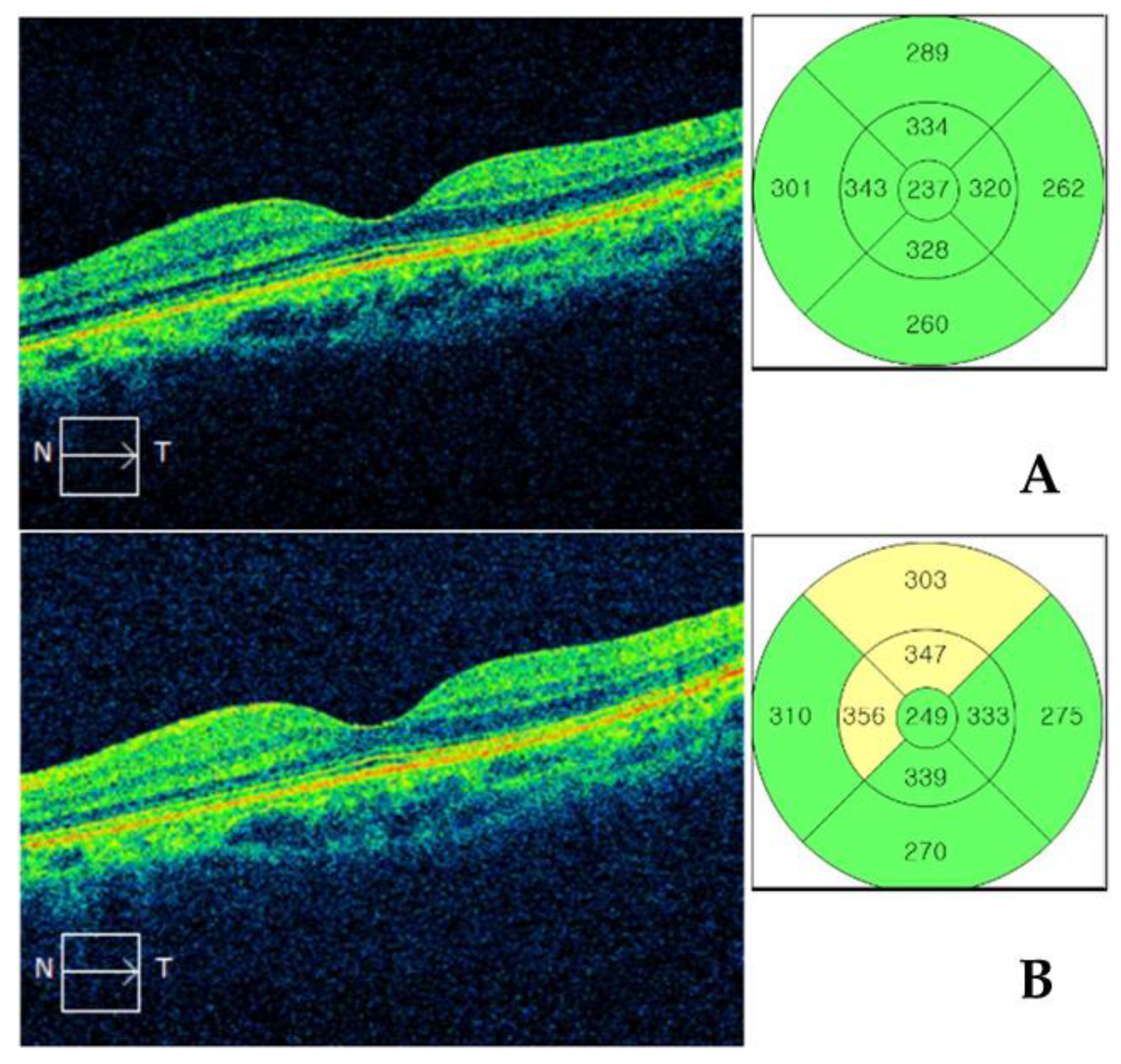
2.2. Macular Thickness Measurement by SD-OCT
2.3. Statistical Analysis
3. Results
3.1. Demographics
3.2. Comparisons of Macular Thickness Measured by SD-OCT
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Henderson, B.A.; Kim, J.Y.; Ament, C.S.; Ferrufino-Ponce, Z.K.; Grabowska, A.; Cremers, S.L. Clinical pseudophakic cystoid macular edema: Risk factors for development and duration after treatment. J. Cataract Refract. Surg. 2007, 33, 1550–1558. [Google Scholar] [CrossRef] [PubMed]
- Flach, A.J. The incidence, pathogenesis and treatment of cystoid macular edema following cataract surgery. Trans. Am. Ophthalmol. Soc. 1998, 96, 557. [Google Scholar] [PubMed]
- Kessel, L.; Tendal, B.; Jørgensen, K.J.; Erngaard, D.; Flesner, P.; Andresen, J.L.; Hjortdal, J. Post-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: A systematic review. Ophthalmology 2014, 121, 1915–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Schoenberger, S.D.; Thorne, J.E.; Ehlers, J.P.; Yeh, S.; Bakri, S.J. Topical nonsteroidal anti-inflammatory drugs and cataract surgery: A report by the American Academy of Ophthalmology. Ophthalmology 2015, 122, 2159–2168. [Google Scholar] [CrossRef] [Green Version]
- Wright, P.L.; Wilkinson, C.; Balyeat, H.D.; Popham, J.; Reinke, M. Angiographic cystoid macular edema after posterior chamber lens implantation. Arch. Ophthalmol. 1988, 106, 740–744. [Google Scholar] [CrossRef]
- Biro, Z.; Balla, Z.; Kovacs, B. Change of foveal and perifoveal thickness measured by OCT after phacoemulsification and IOL implantation. Eye 2008, 22, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Perente, I.; Utine, C.A.; Ozturker, C.; Cakir, M.; Kaya, V.; Eren, H.; Kapran, Z.; Yilmaz, O.F. Evaluation of macular changes after uncomplicated phacoemulsification surgery by optical coherence tomography. Curr. Eye Res. 2007, 32, 241–247. [Google Scholar] [CrossRef]
- Kim, S.J.; Belair, M.-L.; Bressler, N.M.; Dunn, J.P.; Thorne, J.E.; Kedhar, S.R.; Jabs, D.A. A method of reporting macular edema after cataract surgery using optical coherence tomography. Retina 2008, 28, 870–876. [Google Scholar] [CrossRef]
- Chu, C.J.; Johnston, R.L.; Buscombe, C.; Sallam, A.B.; Mohamed, Q.; Yang, Y.C.; United Kingdom Pseudophakic Macular Edema Study Group. Risk factors and incidence of macular edema after cataract surgery: A database study of 81984 eyes. Ophthalmology 2016, 123, 316–323. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.M.; Lee, E.J.; Kim, T.-W.; Kim, H. Pseudophakic macular edema in primary open-angle glaucoma: A prospective study using spectral-domain optical coherence tomography. Am. J. Ophthalmol. 2017, 179, 97–109. [Google Scholar] [CrossRef]
- Packer, M.; Lowe, J.; Fine, H. Incidence of acute postoperative cystoid macular edema in clinical practice. J. Cataract Refract. Surg. 2012, 38, 2108–2111. [Google Scholar] [CrossRef] [PubMed]
- Wand, M.; Gaudio, A.R.; Shields, M.B. Latanoprost and cystoid macular edema in high-risk aphakic or pseudophakic eyes. J. Cataract Refract. Surg. 2001, 27, 1397–1401. [Google Scholar] [CrossRef]
- Cagini, C.; Fiore, T.; Iaccheri, B.; Piccinelli, F.; Ricci, M.A.; Fruttini, D. Macular thickness measured by optical coherence tomography in a healthy population before and after uncomplicated cataract phacoemulsification surgery. Curr. Eye Res. 2009, 34, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Leiba, H.; Bukelman, A.; Oliver, M. Cystoid macular oedema following cataract extraction in patients with diabetes. Br. J. Ophthalmol. 1992, 76, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotsos, T.G.; Moschos, M.M. Cystoid macular edema. Clin. Ophthalmol. (Auckl. NZ) 2008, 2, 919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendel, C.; Zakrzewski, H.; Carleton, B.; Etminan, M.; Mikelberg, F.S. Association of postoperative topical prostaglandin analog or beta-blocker use and incidence of pseudophakic cystoid macular edema. J. Glaucoma 2018, 27, 402–406. [Google Scholar] [CrossRef]
- Wielders, L.H.; Lambermont, V.A.; Schouten, J.S.; Van den Biggelaar, F.J.; Worthy, G.; Simons, R.W.; Winkens, B.; Nuijts, R.M. Prevention of cystoid macular edema after cataract surgery in nondiabetic and diabetic patients: A systematic review and meta-analysis. Am. J. Ophthalmol. 2015, 160, 968–981. [Google Scholar] [CrossRef]
- Schehlein, E.M.; Novack, G.D.; Robin, A.L. New classes of glaucoma medications. Curr. Opin. Ophthalmol. 2017, 28, 161–168. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Razeghinejad, M.R. The effect of latanaprost on intraocular inflammation and macular edema. Ocul. Immunol. Inflamm. 2019, 27, 181–188. [Google Scholar] [CrossRef]
- Makri, O.E.; Tsapardoni, F.N.; Plotas, P.; Ifantis, N.; Xanthopoulou, P.T.; Georgakopoulos, C.D. Cystoid macular edema associated with preservative-free latanoprost after uncomplicated cataract surgery: Case report and review of the literature. BMC Res. Notes 2017, 10, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moroi, S.E.; Gottfredsdottir, M.S.; Schteingart, M.T.; Elner, S.G.; Lee, C.M.; Schertzer, R.M.; Abrams, G.W.; Johnson, M.W. Cystoid macular edema associated with latanoprost therapy in a case series of patients with glaucoma and ocular hypertension. Ophthalmology 1999, 106, 1024–1029. [Google Scholar] [CrossRef]
- Fakhraie, G.; Mirghorbani, M.; Katz, L.J.; Mollazadeh, A.; Vahedian, Z.; Zarei, R.; Eslami, Y.; Mohammadi, M.; Hamzeh, N.; Masoomi, A. Cystoid macular edema with prostaglandin analogue use after uneventful cataract surgery in glaucoma patients. J. Cataract Refract. Surg. 2019, 45, 1436–1445. [Google Scholar] [CrossRef] [PubMed]
- Sigler, E.J.; Randolph, J.C.; Kiernan, D.F. Longitudinal analysis of the structural pattern of pseudophakic cystoid macular edema using multimodal imaging. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.C.; Ramanathan, S. Latanoprost and clinically significant cystoid macular edema after uneventful phacoemulsification with intraocular lens implantation. J. Cataract Refract. Surg. 2002, 28, 1814–1818. [Google Scholar] [CrossRef]
- Lima, M.C.; Paranhos, J.A.; Salim, S.; Honkanen, R.; Devgan, L.; Wand, M.; Gaudio, A.R.; Shields, M.B. Visually significant cystoid macular edema in pseudophakic and aphakic patients with glaucoma receiving latanoprost. J. Glaucoma 2000, 9, 317–321. [Google Scholar] [CrossRef]
- Warmar, R. Cystoid macular edema and anterior uveitis associated with latanoprost use. Ophthalmology 1998, 105, 263–268. [Google Scholar] [CrossRef]
- Miyake, K.; Ota, I.; Maekubo, K.; Ichihashi, S.; Miyake, S. Latanoprost accelerates disruption of the blood-aqueous barrier and the incidence of angiographic cystoid macular edema in early postoperative pseudophakias. Arch. Ophthalmol. 1999, 117, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Lim, K.S.; Nau, C.B.; O’Byrne, M.M.; Hodge, D.O.; Toris, C.B.; McLaren, J.W.; Johnson, D.H. Mechanism of action of bimatoprost, latanoprost, and travoprost in healthy subjects: A crossover study. Ophthalmology 2008, 115, 790–795.e4. [Google Scholar] [CrossRef] [Green Version]
- Thieme, H.; Stumpff, F.; Ottlecz, A.; Percicot, C.L.; Lambrou, G.N.; Wiederholt, M. Mechanisms of action of unoprostone on trabecular meshwork contractility. Investig. Ophthalmol. Vis. Sci. 2001, 42, 3193–3201. [Google Scholar]
- Poyer, J.F.; Millar, C.; Kaufman, P.L. Prostaglandin F2 alpha effects on isolated rhesus monkey ciliary muscle. Investig. Ophthalmol. Vis. Sci. 1995, 36, 2461–2465. [Google Scholar]
- Lindsey, J.D.; Kashiwagi, K.; Kashiwagi, F.; Weinreb, R.N. Prostaglandins alter extracellular matrix adjacent to human ciliary muscle cells in vitro. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2214–2223. [Google Scholar]
- Lindsey, J.D.; Kashiwagi, K.; Kashiwagi, F.; Weinreb, R.N. Prostaglandin action on ciliary smooth muscle extracellular matrix metabolism: Implications for uveoscleral outflow. Surv. Ophthalmol. 1997, 41, S53–S59. [Google Scholar] [CrossRef]
- Kashiwagi, K.; Jin, M.; Suzuki, M.; Tanaka, Y.; Iizuka, Y.; Tsukahara, S. Isopropyl unoprostone increases the activities of matrix metalloproteinases in cultured monkey ciliary muscle cells. J. Glaucoma 2001, 10, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Digiuni, M.; Fogagnolo, P.; Rossetti, L. A review of the use of latanoprost for glaucoma since its launch. Expert Opin. Pharmacother. 2012, 13, 723–745. [Google Scholar] [CrossRef]
- Stewart, W.C.; Kolker, A.E.; Stewart, J.A.; Leech, J.; Jackson, A.L. Conjunctival hyperemia in healthy subjects after short-term dosing with latanoprost, bimatoprost, and travoprost. Am. J. Ophthalmol. 2003, 135, 314–320. [Google Scholar] [CrossRef]
- Camras, C.B.; Toris, C.B.; Tamesis, R.R. Efficacy and adverse effects of medications used in the treatment of glaucoma. Drugs Aging 1999, 15, 377–388. [Google Scholar] [CrossRef]
- Parrish, R.K.; Palmberg, P.; Sheu, W.-P.; Group, X.S. A comparison of latanoprost, bimatoprost, and travoprost in patients with elevated intraocular pressure: A 12-week, randomized, masked-evaluator multicenter study. Am. J. Ophthalmol. 2003, 135, 688–703. [Google Scholar] [CrossRef]
- Ayyala, R.S.; Cruz, D.A.; Margo, C.E.; Harman, L.E.; Pautler, S.E.; Misch, D.M.; Mines, J.A.; Richards, D.W. Cystoid macular edema associated with latanoprost in aphakic and pseudophakic eyes. Am. J. Ophthalmol. 1998, 126, 602–604. [Google Scholar] [CrossRef]
- Callanan, D.; Fellman, R.L.; Savage, J.A. Latanoprost-associated cystoid macular edema. Am. J. Ophthalmol. 1998, 126, 134–135. [Google Scholar] [CrossRef]
- Heier, J.S.; Steinert, R.F.; Frederick, A.R. Cystoid macular edema associated with latanoprost use. Arch. Ophthalmol. 1998, 116, 680–682. [Google Scholar] [PubMed]
- Halpern, D.L.; Pasquale, L.R. Cystoid macular edema in aphakia and pseudophakia after use of prostaglandin analogs. In Seminars in Ophthalmology; Taylor & Francis: Abingdon, UK, 2002; pp. 181–186. [Google Scholar]
- Ahad, M.A.; McKee, H.D. Stopping prostaglandin analogues in uneventful cataract surgery. J. Cataract Refract. Surg. 2004, 30, 2644–2645. [Google Scholar] [CrossRef] [PubMed]
- Holló, G.; Aung, T.; Cantor, L.B.; Aihara, M. Cystoid macula edema related to cataract surgery and topical prostaglandin analogs: Mechanism, diagnosis, and management. Surv. Ophthalmol. 2020, 65, 496–512. [Google Scholar] [CrossRef] [PubMed]
- Mataftsi, A.; Tsaousis, K.T.; Tsinopoulos, I.T.; Dimitrakos, S.A. Survey of perioperative prostaglandin analogue administration during cataract surgery in Greece. Int. Ophthalmol. 2012, 32, 97–98. [Google Scholar] [CrossRef]
- Kim, S.J.; Flach, A.J.; Jampol, L.M. Nonsteroidal anti-inflammatory drugs in ophthalmology. Surv. Ophthalmol. 2010, 55, 108–133. [Google Scholar] [CrossRef]
- Lindstrom, R. The pharmacologic and pathophysiologic rationale for using NSAIDs in ocular inflammatory disease and ocular surgery. Int. Ophthalmol. Clin. 2006, 46, 7–11. [Google Scholar] [CrossRef]
- Group, M.S. Cystoid macular edema in aphakic and pseudophakic eyes. Am. J. Ophthalmol. 1979, 88, 45–48. [Google Scholar]
- Stark, W.J.; Worthen, D.M.; Holladay, J.T.; Bath, P.E.; Jacobs, M.E.; Murray, G.C.; McGhee, E.T.; Talbott, M.W.; Shipp, M.D.; Thomas, N.E. The FDA report on intraocular lenses. Ophthalmology 1983, 90, 311–317. [Google Scholar] [CrossRef]
- Miyake, K.; Ibaraki, N. Prostaglandins and cystoid macular edema. Surv. Ophthalmol. 2002, 47, S203–S218. [Google Scholar] [CrossRef]
- Schechter, B.A. Use of topical bromfenac for treating ocular pain and inflammation beyond cataract surgery: A review of published studies. Clin. Ophthalmol. (Auckl. NZ) 2019, 13, 1439. [Google Scholar] [CrossRef] [Green Version]
- Olson, R.J.; Braga-Mele, R.; Chen, S.H.; Miller, K.M.; Pineda, R.; Tweeten, J.P.; Musch, D.C. Cataract in the adult eye preferred practice pattern®. Ophthalmology 2017, 124, 1–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, B.X.; Lim, C.H.; Lim, D.K.; Evans, J.R.; Bunce, C.; Wormald, R. Prophylactic non-steroidal anti-inflammatory drugs for the prevention of macular oedema after cataract surgery. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Miyake, K.; Masuda, K.; Shirato, S.; Oshika, T.; Eguchi, K.; Hoshi, H.; Majima, Y.; Kimura, W.; Hayashi, F. Comparison of diclofenac and fluorometholone in preventing cystoid macular edema after small incision cataract surgery: A multicentered prospective trial. Jpn. J. Ophthalmol. 2000, 44, 58–67. [Google Scholar] [CrossRef]
- Miyake, K. Nonsteroidal anti-inflammatory agents in cataract intraocular lens surgery. Curr. Opin. Ophthalmol. 1995, 6, 62–65. [Google Scholar]
- Rossetti, L.; Chaudhuri, J.; Dickersin, K. Medical prophylaxis and treatment of cystoid macular edema after cataract surgery: The results of a meta-analysis. Ophthalmology 1998, 105, 397–405. [Google Scholar] [CrossRef]
- Modjtahedi, B.S.; Paschal, J.F.; Batech, M.; Luong, T.Q.; Fong, D.S. Perioperative topical nonsteroidal anti-inflammatory drugs for macular edema prophylaxis following cataract surgery. Am. J. Ophthalmol. 2017, 176, 174–182. [Google Scholar] [CrossRef]
- Koh, C.H.; Chung, S.K. Effect of non-steroidal anti-inflammatory drugs on cystoid macular edema in diabetic patients after cataract surgery. J. Korean Ophthalmol. Soc. 2013, 54, 427–431. [Google Scholar] [CrossRef]
- Song, S.H.; Baek, S.K.; Lee, M.W.; Lee, Y.H. Effect of 0.1% Bromfenac for Preventing Macular Edema after Cataract Surgery in Patients with Diabetes. Korean J. Ophthalmol. 2020, 34, 46–55. [Google Scholar] [CrossRef]
- Van Buren, J.M. The Retinal Ganglion Cell Layer: A Physiological-Anatomical Correlation in Man and Primates of the Normal Topographical Anatomy of the Retinal Ganglion Cell Layer and its Alterations with Lesions of the Visual Pathways; Charles C. Thomas: Springfield, IL, USA, 1963. [Google Scholar]
- Greenfield, D.S.; Bagga, H.; Knighton, R.W. Macular thickness changes in glaucomatous optic neuropathy detected using optical coherence tomography. Arch. Ophthalmol. 2003, 121, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Fitzgibbon, T.; Taylor, S. Retinotopy of the human retinal nerve fibre layer and optic nerve head. J. Comp. Neurol. 1996, 375, 238–251. [Google Scholar] [CrossRef]
- Leung, C.K.; Chan, W.-M.; Yung, W.-H.; Ng, A.C.; Woo, J.; Tsang, M.-K.; Raymond, K. Comparison of macular and peripapillary measurements for the detection of glaucoma: An optical coherence tomography study. Ophthalmology 2005, 112, 391–400. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | PGA Continuing (A) | PGA Discontinued (B) | Non-Glaucomatous (C) | p-Value |
|---|---|---|---|---|
| No. of patients (no. of eyes) | 32 (32) | 33 (33) | 58 (58) | |
| Age (years) | 67.8 ± 12.1 | 67.7 ± 9.5 | 68.8 ± 8.8 | 0.865 * |
| Sex (male/female) | 7/25 | 10/23 | 18/40 | 0.630 † |
| Systemic disease, n (%) | ||||
| DM | 9 (28.1) | 9 (27.3) | 17 (29.3) | 0.978 † |
| HTN | 7 (21.9) | 11 (33.3) | 17 (29.3) | 0.581 † |
| CVA | 3 (9.4) | 4 (12.1) | 5 (8.6) | 0.861 † |
| Type of glaucoma, n (%) | 0.557 ‡ | |||
| Normal-tension | 19 (59.4%) | 17 (51.5%) | N/A | |
| Primary open-angle | 8 (25.0%) | 7 (21.2%) | N/A | |
| Pseudoexfoliation | 4 (12.5%) | 5 (15.2%) | N/A | |
| Primary angle-closure | 1 (3.1%) | 4 (12.1%) | N/A | |
| Best-corrected visual acuity (logMAR) | ||||
| Preoperative | 0.41 ± 0.24 | 0.25 ± 0.21 | 0.33 ± 0.27 | 0.069 * |
| Postoperative | 0.09 ± 0.18 | 0.06 ± 0.13 | 0.04 ± 0.08 | 0.186 * |
| Intraocular pressure (mmHg) | ||||
| Preoperative | 18.47 ± 3.28 | 16.70 ± 2.74 | 17.12 ± 3.36 | 0.106 * |
| Postoperative | 17.37 ± 2.44 | 16.50 ± 1.67 | 16.64 ± 3.37 | 0.460 * |
| Central corneal thickness (μm) | 533.40 ± 42.51 | 532.95 ± 37.01 | 548.44 ± 35.59 | 0.141 * |
| Axial length (mm) | 23.27 ± 0.99 | 23.92 ± 1.25 | 23.39 ± 1.07 | 0.100 * |
| Average RNFL thickness (μm) | 73.20 ± 13.96 | 69.00 ± 11.38 | 89.22 ± 10.03 | <0.001 * (A = B < C) |
| Type of PGA (n) | 0.441 ‡ | |||
| Latanoprost 0.005% | 15 | 16 | N/A | |
| Tafluprost 0.0015% | 12 | 15 | N/A | |
| Bimatoprost 0.03% | 5 | 2 | N/A |
| ETDRS Areas | PGA Continuing (A) | PGA Discontinued (B) | Non-Glaucomatous (C) | p-Value * |
|---|---|---|---|---|
| Central | 249.73 ± 19.89 | 257.65 ± 17.88 | 250.20 ± 22.58 | 0.348 (A = B = C) |
| Inner superior | 309.43 ± 14.85 | 309.05 ± 15.95 | 316.46 ± 11.34 | 0.032 (A = B < C) |
| Inner temporal | 290.00 ± 17.46 | 295.35 ± 18.23 | 307.16 ± 16.24 | 0.001 (A = B < C) |
| Inner inferior | 294.93 ± 19.19 | 301.00 ± 17.22 | 314.06 ± 12.02 | 0.001 (A = B < C) |
| Inner nasal | 310.20 ± 16.73 | 315.70 ± 14.99 | 316.90 ± 13.43 | 0.143 (A = B = C) |
| Outer superior | 267.83 ± 17.17 | 258.30 ± 16.22 | 276.10 ± 11.23 | 0.001 (A = B < C) |
| Outer temporal | 248.77 ± 16.59 | 245.45 ± 10.86 | 264.94 ± 13.57 | 0.001 (A = B < C) |
| Outer inferior | 241.77 ± 18.46 | 240.90 ± 13.71 | 260.14 ± 12.25 | 0.001 (A = B < C) |
| Outer nasal | 281.63 ± 19.42 | 278.25 ± 15.74 | 288.02 ± 15.14 | 0.057 (A = B = C) |
| ETDRS Areas | PGA Continuing (A) | PGA Discontinued (B) | Non-Glaucomatous (C) | p-Value * |
|---|---|---|---|---|
| Central | 254.03 ± 20.42 | 263.85 ± 22.75 | 257.26 ± 22.69 | 0.126 (A = B = C) |
| Inner superior | 317.70 ± 15.29 | 316.10 ± 11.61 | 324.86 ± 12.24 | 0.030 (A = B < C) |
| Inner temporal | 299.17 ± 15.37 | 306.20 ± 14.97 | 316.68 ± 13.77 | 0.001 (A = B < C) |
| Inner inferior | 303.07 ± 17.88 | 308.00 ± 13.65 | 321.80 ± 12.02 | 0.002 (A = B < C) |
| Inner nasal | 318.93 ± 15.98 | 321.70 ± 15.61 | 325.28 ± 12.42 | 0.581 (A = B = C) |
| Outer superior | 274.13 ± 16.16 | 266.20 ± 11.92 | 281.70 ± 11.63 | 0.001 (A = B < C) |
| Outer temporal | 255.87 ± 16.07 | 249.55 ± 12.20 | 271.24 ± 14.95 | 0.001 (A = B < C) |
| Outer inferior | 247.73 ± 17.59 | 245.10 ± 9.30 | 266.56 ± 13.17 | 0.001 (A = B < C) |
| Outer nasal | 288.37 ± 15.41 | 283.75 ± 12.57 | 294.33 ± 17.60 | 0.087 (A = B = C) |
| ETDRS Areas | PGA Continuing (A) | p-Value | PGA Discontinued (B) | p-Value | Non-Glaucomatous (C) | p-Value | p-Value * |
|---|---|---|---|---|---|---|---|
| Central | 4.30 ± 8.01 | 0.001 | 6.20 ± 10.88 | 0.008 | 7.06 ± 7.02 | 0.006 | 0.161 (A = B = C) |
| Inner superior | 8.27 ± 9.33 | 0.001 | 7.05 ± 10.58 | 0.001 | 8.40 ± 6.48 | 0.001 | 0.909 (A = B = C) |
| Inner temporal | 9.16 ± 12.51 | 0.001 | 10.85 ± 13.87 | 0.008 | 9.52 ± 10.59 | 0.002 | 0.465 (A = B = C) |
| Inner inferior | 8.13 ± 9.65 | 0.001 | 7.00 ± 11.69 | 0.012 | 7.74 ± 6.41 | 0.001 | 0.942 (A = B = C) |
| Inner nasal | 8.73 ± 15.78 | 0.001 | 6.00 ± 14.97 | 0.030 | 8.38 ± 10.63 | 0.002 | 0.541 (A = B = C) |
| Outer superior | 6.30 ± 8.07 | 0.001 | 7.90 ± 9.27 | 0.004 | 5.60 ± 6.36 | 0.004 | 0.632 (A = B = C) |
| Outer temporal | 7.10 ± 9.25 | 0.001 | 4.10 ± 16.35 | 0.008 | 6.30 ± 10.31 | 0.001 | 0.147 (A = B = C) |
| Outer inferior | 5.97 ± 10.92 | 0.001 | 4.20 ± 11.61 | 0.041 | 6.42 ± 7.42 | 0.001 | 0.120 (A = B = C) |
| Outer nasal | 6.73 ± 13.38 | 0.002 | 5.50 ± 12.84 | 0.026 | 6.31 ± 13.16 | 0.001 | 0.772 (A = B = C) |
| Clinical Factors | r | β | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| Age (years) | 0.066 | 0.060 | −0.123 to 0.244 | 0.515 |
| Sex (male) | 0.071 | 1.317 | −2.389 to 5.022 | 0.482 |
| Systemic disease | ||||
| DM | 0.086 | −1.693 | −5.972 to 2.586 | 0.434 |
| HTN | 0.161 | −2.895 | −6.664 to 0.874 | 0.131 |
| CVA | 0.008 | −0.224 | −6.682 to 6.234 | 0.945 |
| Type of glaucoma, n * | ||||
| Normal-tension | 0.250 | 5.456 | −0.682 to 11.595 | 0.080 |
| Primary open-angle | 0.093 | −2.431 | −9.951 to 5.089 | 0.519 |
| Pseudoexfoliation | 0.090 | −2.794 | −11.775 to 6.186 | 0.535 |
| Primary angle-closure | 0.225 | −10.206 | −23.043 to 2.632 | 0.117 |
| Preoperative BCVA (mmHg) | 0.057 | 2.015 | −5.015 to 9.045 | 0.571 |
| Preoperative IOP (mmHg) | 0.014 | −0.039 | −0.572 to 0.495 | 0.886 |
| CCT (μm) | 0.055 | −0.013 | −0.061 to 0.034 | 0.586 |
| Axial length (mm) | 0.140 | 1.133 | −0.470 to 2.735 | 0.164 |
| Average RNFL thickness (um) | 0.073 | 0.046 | −0.080 to 0.171 | 0.472 |
| PGA continuing | 0.115 | 1.195 | −0.879 to 3.269 | 0.256 |
| Type of PGA * | ||||
| Latanoprost 0.005% | 0.218 | 4.708 | −1.403 to 10.820 | 0.128 |
| Tafluprost 0.0015% | 0.005 | −1.438 | −7.870 to 4.994 | 0.655 |
| Bimatoprost 0.03% | 0.224 | −6.947 | −15.736 to 1.842 | 0.119 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.S.; Kim, K.N.; Kim, K.M.; Lee, H.M.; Lee, S.B.; Lee, N.H.; Kim, C.-S. Effects of Topical Prostaglandin Analog on Macular Thickness Following Cataract Surgery with Postoperative Topical Bromfenac Treatment. J. Clin. Med. 2020, 9, 2883. https://doi.org/10.3390/jcm9092883
Park KS, Kim KN, Kim KM, Lee HM, Lee SB, Lee NH, Kim C-S. Effects of Topical Prostaglandin Analog on Macular Thickness Following Cataract Surgery with Postoperative Topical Bromfenac Treatment. Journal of Clinical Medicine. 2020; 9(9):2883. https://doi.org/10.3390/jcm9092883
Chicago/Turabian StylePark, Kee Sup, Kyoung Nam Kim, Kyeung Min Kim, Han Min Lee, Sung Bok Lee, Nam Ho Lee, and Chang-Sik Kim. 2020. "Effects of Topical Prostaglandin Analog on Macular Thickness Following Cataract Surgery with Postoperative Topical Bromfenac Treatment" Journal of Clinical Medicine 9, no. 9: 2883. https://doi.org/10.3390/jcm9092883
APA StylePark, K. S., Kim, K. N., Kim, K. M., Lee, H. M., Lee, S. B., Lee, N. H., & Kim, C.-S. (2020). Effects of Topical Prostaglandin Analog on Macular Thickness Following Cataract Surgery with Postoperative Topical Bromfenac Treatment. Journal of Clinical Medicine, 9(9), 2883. https://doi.org/10.3390/jcm9092883