
Relationship between Serum Ferritin and Outcomes in β-Thalassemia: A Systematic Literature Review

 , ,
, ,
Abstract
:1. Introduction
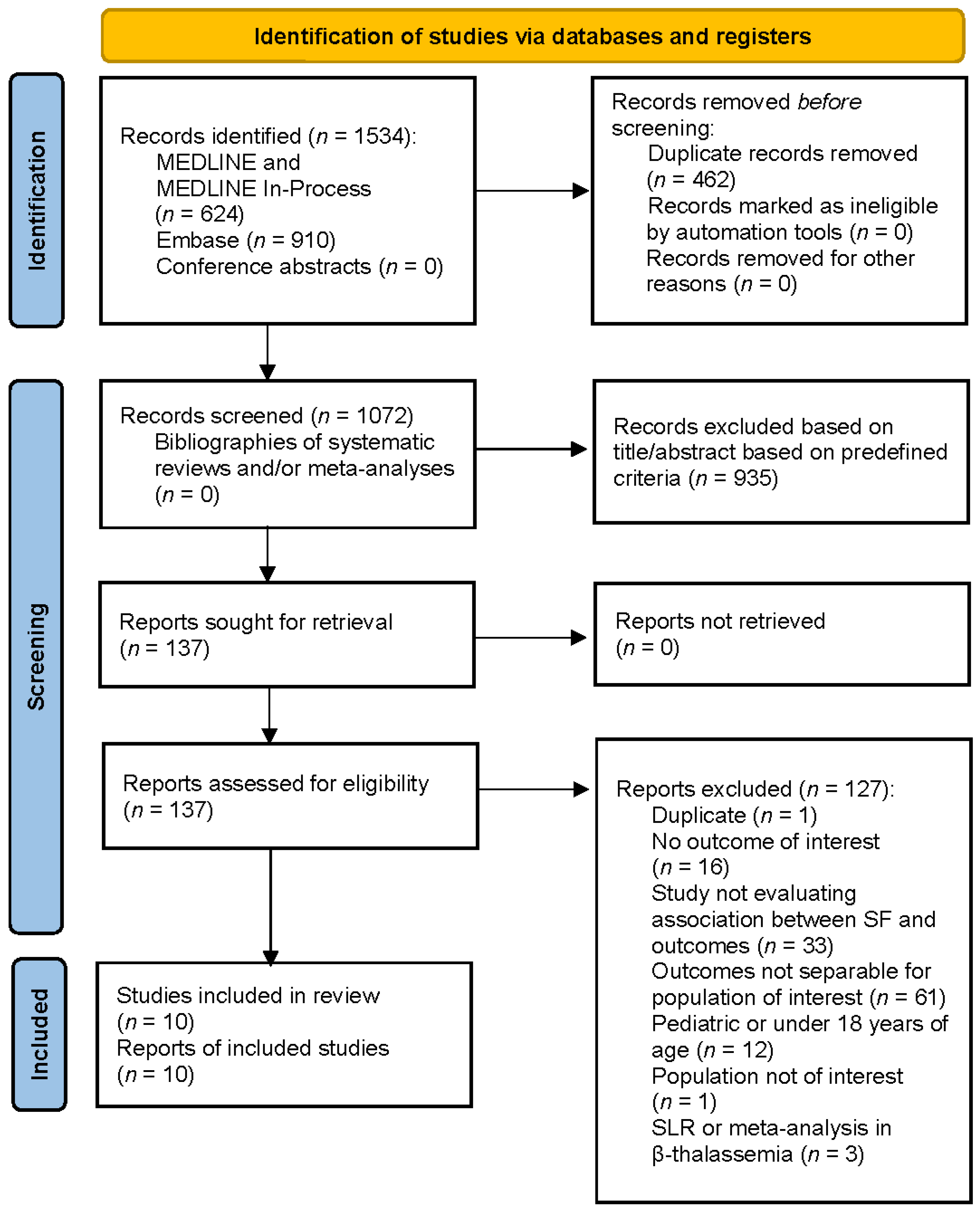
2. Materials and Methods
3. Results
3.1. Mortality
3.2. Hepatic Complications
3.3. Skeletal Complications
3.4. Cardiac Complications
3.5. Endocrine Risk Factors
3.5.1. Endocrine Disorders
3.5.2. Diabetes
3.5.3. Thyroid Function
3.5.4. Hypogonadism
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taher, A.T.; Saliba, A.N. Iron overload in thalassemia: Different organs at different rates. Am. Soc. Hematol. Educ. Program 2017, 1, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colah, R.; Gorakshakar, A.; Nadkarni, A. Global burden, distribution and prevention of beta-thalassemias and hemoglobin E disorders. Expert Rev. Hematol. 2010, 3, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Modell, B.; Darlison, M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull. World Health Organ. 2008, 86, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Ribeil, J.A.; Arlet, J.B.; Dussiot, M.; Moura, I.C.; Courtois, G.; Hermine, O. Ineffective erythropoiesis in beta-thalassemia. Sci. World J. 2013, 2013, 394295. [Google Scholar] [CrossRef] [Green Version]
- Temraz, S.; Santini, V.; Musallam, K.; Taher, A. Iron overload and chelation therapy in myelodysplastic syndromes. Crit. Rev. Oncol. Hematol. 2014, 91, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Mobarra, N.; Shanaki, M.; Ehteram, H.; Nasiri, H.; Sahmani, M.; Saeidi, M.; Goudarzi, M.; Pourkarim, H.; Azad, M. A review of iron chelators in treatment of iron overload syndromes. Int. J. Hematol. Oncol. Stem Cell Res. 2016, 10, 239–247. [Google Scholar] [PubMed]
- Majd, Z.; Haghpanah, S.; Ajami, G.H.; Matin, S.; Namazi, H.; Bardestani, M.; Karimi, M. Serum ferritin levels correlation with heart and liver MRI and LIC in patients with transfusion-dependent thalassemia. Iran. Red Crescent Med. J. 2015, 17, e24959. [Google Scholar] [CrossRef] [Green Version]
- MedlinePlus [Internet]. Ferritin Blood Test; National Library of Medicine (US): Bethesda, MD, USA. Available online: https://medlineplus.gov/ency/article/003490.htm (accessed on 14 January 2020).
- Knovich, M.A.; Storey, J.A.; Coffman, L.G.; Torti, S.V.; Torti, F.M. Ferritin for the clinician. Blood Rev. 2009, 23, 95–104. [Google Scholar] [CrossRef]
- Aguirre, L.G.; Urrunaga-Pastor, D.; Moncada-Mapelli, E.; Guarnizo-Poma, M.; Lazaro-Alcantara, H.; Benites-Zapata, V.A. High serum ferritin levels are associated with insulin resistance but not with impaired glucose tolerance in a healthy people population. Diabetes Metab. Syndr. 2017, 11 (Suppl. S2), S983–S988. [Google Scholar] [CrossRef]
- Olesnevich, M.E.; Kuczmarksi, M.F.; Mason, M.; Fang, C.; Zonderman, A.B.; Evans, M.K. Serum ferritin levels associated with increased risk for developing CHD in a low-income urban population. Public Health Nutr. 2021, 15, 1291–1298. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence (NICE). NICE Guidance PMG9: Guide to the Methods of Technology Appraisal. Available online: https://www.nice.org.uk/process/pmg9/chapter/foreword (accessed on 25 January 2022).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 372, n71. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpstonm, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1. Cochrane. 2011. Available online: https://training.cochrane.org/handbook/archive/v5.1/ (accessed on 25 January 2022).
- Ang, A.L.; Tzoulis, P.; Prescott, E.; Davis, B.A.; Barnard, M.; Shah, F.T. History of myocardial iron loading is a strong risk factor for diabetes mellitus and hypogonadism in adults with beta thalassemia major. Eur. J. Haematol. 2014, 92, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.R.; Ko, H.S.; Chao, T.F.; Liu, H.C.; Kuo, J.Y.; Bulwer, B.E.; Yeh, H.-I.; Hung, C.-L. Relation of myocardial systolic mechanics to serum ferritin level as a prognosticator in thalassemia patients undergoing repeated transfusion. Echocardiography 2015, 32, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Chirico, V.; Lacquaniti, A.; Salpietro, V.; Luca, N.; Ferraù, V.; Piraino, B.; Luciana, R.; Carmelo, S.; Teresa, A. Thyroid dysfunction in thalassaemic patients: Ferritin as a prognostic marker and combined iron chelators as an ideal therapy. Eur. J. Endocrinol. 2013, 169, 785–793. [Google Scholar] [CrossRef] [Green Version]
- Chirico, V.; Rigoli, L.; Lacquaniti, A.; Salpietro, V.; Piraino, B.; Amorini, M.; Salpietro, C.; Arrigo, T. Endocrinopathies, metabolic disorders, and iron overload in major and intermedia thalassemia: Serum ferritin as diagnostic and predictive marker associated with liver and cardiac T2 MRI assessment. Eur. J. Haematol. 2015, 94, 404–412. [Google Scholar] [CrossRef]
- Ebrahimpour, L.; Akhlaghpoor, S.; Azarkayvan, A.; Salehi, M.; Morteza, A.; Alinaghi, R. Correlation between bone mineral densitometry and liver/heart iron overload evaluated by quantitative T2 MRI. Hematology 2012, 17, 297–301. [Google Scholar] [CrossRef]
- Foroughi, A.A.; Ghaffari, H.; Haghpanah, S.; Nazeri, M.; Ghaffari, R.; Bardestani, M.; Karimi, M. Comparative study of radiographic and laboratory findings between beta thalassemia major and beta thalassemia intermedia patients with and without treatment by hydroxyurea. Iran. Red Crescent Med. J. 2015, 17, e23607. [Google Scholar]
- Hahalis, G.; Kourakli, A.; Gerasimidou, I.; Kalogeropoulos, A.P.; Sitafidis, G.; Papageorgiou, U.; Davlouros, P.; Grapsas, N.; Zoumbos, N.C.; Alexopouloset, D. Cardiac mortality in {beta}-thalassemia major: Resting but not dobutamine stress echocardiography predicts mortality among initially cardiac disease-free patients in a prospective 12-year study. Eur. J. Heart Fail. 2009, 11, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Musallam, K.M.; Motta, I.; Salvatori, M.; Fraquelli, M.; Marcon, A.; Taher, A.T.; Cappellini, M.D. Longitudinal changes in serum ferritin levels correlate with measures of hepatic stiffness in transfusion-independent patients with beta-thalassemia intermedia. Blood Cells Mol. Dis. 2012, 49, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Poggi, M.; Sorrentino, F.; Pugliese, P.; Smacchia, M.P.; Daniele, C.; Equitani, F.; Terlizzi, F.; Guitarrini, M.R.; Monti, S.; Maffei, L.; et al. Longitudinal changes of endocrine and bone disease in adults with beta-thalassemia major receiving different iron chelators over 5 years. Ann. Hematol. 2016, 95, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Vlahos, A.P.; Koutsouka, F.P.; Papamichael, N.D.; Makis, A.; Baltogiannis, G.; Athanasiou, E.; Chaliasos, N.; Bourantas, K.L.; Kolettis, T.M. Determinants of pulmonary hypertension in patients with beta-thalassemia major and normal ventricular function. Acta Haematol. 2012, 128, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Cassinerio, E.; Orofino, N.; Roghi, A.; Duca, L.; Poggiali, E.; Fraquelli, M.; Zanaboni, L.; Cappellini, M.D. Combination of deferasirox and deferoxamine in clinical practice: An alternative scheme of chelation in thalassemia major patients. Blood Cells Mol. Dis. 2014, 53, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Cassinerio, E.; Roghi, A.; Orofino, N.; Pedrotti, P.; Zanaboni, L.; Poggiali, E.; Giuditta, M.; Consonni, D.; Cappellini, M.D. A 5-year follow-up in deferasirox treatment: Improvement of cardiac and hepatic iron overload and amelioration in cardiac function in thalassemia major patients. Ann. Hematol. 2015, 94, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Cassinerio, E.; Roghi, A.; Pedrotti, P.; Brevi, F.; Zanaboni, L.; Graziadei, G.; Pattoneri, P.; Milazzo, A.; Cappellini, M.D. Cardiac iron removal and functional cardiac improvement by different iron chelation regimens in thalassemia major patients. Ann. Hematol. 2012, 91, 1443–1449. [Google Scholar] [CrossRef]
- De Sanctis, V.; Elsedfy, H.; Soliman, A.T.; Elhakim, I.Z.; Kattamis, C.; Soliman, N.A.; Elalaily, R. Clinical and biochemical data of adult thalassemia major patients (TM) with multiple endocrine complications (MEC) versus TM patients with normal endocrine functions: A long-term retrospective study (40 years) in a tertiary care center in Italy. Mediterr. J. Hematol. Infect. Dis. 2016, 8, e2016022. [Google Scholar] [CrossRef] [Green Version]
- Esmaeilzadeh, F.; Azarkeivan, A.; Emamgholipour, S.; Sari, A.A.; Yaseri, M.; Ahmadi, B.; Ghaffari, M. Economic burden of thalassemia major in Iran, 2015. J. Res. Health Sci. 2016, 16, 111–115. [Google Scholar] [PubMed]
- Farmaki, K.; Tzoumari, I.; Pappa, C. Oral chelators in transfusion-dependent thalassemia major patients may prevent or reverse iron overload complications. Blood Cells Mol. Dis. 2011, 47, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Gollo, G.; Savioli, G.; Balocco, M.; Venturino, C.; Boeri, E.; Costantini, M.; Forni, G.L. Changes in the quality of life of people with thalassemia major between 2001 and 2009. Patient Prefer. Adherence 2013, 7, 231–236. [Google Scholar]
- Goulas, V.; Kourakli-Symeonidis, A.; Camoutsis, C. Comparative effects of three iron chelation therapies on the quality of life of Greek patients with homozygous transfusion-dependent beta-thalassemia. ISRN Hematol. 2012, 2012, 139862. [Google Scholar] [CrossRef] [Green Version]
- Hammond, J.; Thompson, A.A.; Fogel, M.A.; Hammond, K.; Kokroko, J.; Kwiatkowski, J.L. Combination oral chelation in adult patients with transfusion-dependent thalassemia and high iron burden. J. Pediatric Hematol. Oncol. 2019, 41, E47–E50. [Google Scholar] [CrossRef]
- Hatzipantelis, E.S.; Karasmanis, K.; Perifanis, V.; Vlachaki, E.; Tziomalos, K.; Economou, M. Combined chelation therapy with deferoxamine and deferiprone in beta-thalassemia major: Compliance and opinions of young thalassemic patients. Hemoglobin 2014, 38, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Avazpour, A.; Haghpanah, S.; Toosi, F.; Badie, A. Evaluation of proteinuria in beta-thalassemia major patients with and without diabetes mellitus taking deferasirox. J. Pediatric Hematol. Oncol. 2017, 39, e11–e14. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.E.; Grady, R.W.; Vacquer, S.; Pepe, A.; Carta, M.P.; Bina, P.; Sau, F.; Cianciulli, P.; Maggio, A.; Galanello, R.; et al. Increased survival and reversion of iron-induced cardiac disease in patients with thalassemia major receiving intensive combined chelation therapy as compared to desferoxamine alone. Blood Cells Mol. Dis. 2010, 45, 136–139. [Google Scholar] [CrossRef]
- McQuilten, Z.K.; Higgins, A.M.; Burns, K.; Chunilal, S.; Dunstan, T.; Haysom, H.E.; Sau, F.; Cianciulli, P.; Maggio, A.; Galanello, R.; et al. The cost of blood: A study of the total cost of red blood cell transfusion in patients with beta-thalassemia using time-driven activity-based costing. Transfusion 2019, 59, 3386–3395. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Positano, V.; Ruffo, G.B.; Spasiano, A.; D’Ascola, D.G.; Peluso, A.; Keilberg, P.; Restaino, G.; Valeri, G.; Renne, S.; et al. Improvement of heart iron with preserved patterns of iron store by CMR-guided chelation therapy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, A.; Meloni, A.; Capra, M.; Cianciulli, P.; Prossomariti, L.; Malaventura, C.; Putti, M.C.; Lippi, A.; Romeo, M.A.; Bisconte, M.; et al. Deferasirox, deferiprone and desferrioxamine treatment in thalassemia major patients: Cardiac iron and function comparison determined by quantitative magnetic resonance imaging. Haematologica 2011, 96, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, A.; Meloni, A.; Rossi, G.; Midiri, M.; Missere, M.; Valeri, G.; Sorrentino, F.; D’Ascola, D.G.; Spasiano, A.; Filosa, A.; et al. Prediction of cardiac complications for thalassemia major in the widespread cardiac magnetic resonance era: A prospective multicentre study by a multi-parametric approach. Eur. Heart J. Cardiovasc. Imagin 2018, 19, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Pepe, A.; Meloni, A.; Pistoia, L.; Cuccia, L.; Gamberini, M.R.; Lisi, R.; D’Ascola, D.G.; Rosso, R.; Allò, M.; Spasiano, A.; et al. MRI multicentre prospective survey in thalassaemia major patients treated with deferasirox versus deferiprone and desferrioxamine. Br. J. Haematol. 2018, 183, 783–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seyedifar, M.; Dorkoosh, F.A.; Hamidieh, A.A.; Naderi, M.; Karami, H.; Karimi, M.; Fadaiyrayeny, M.; Musavi, M.; Safaei, S.; Ahmadian-Attari, M.M.; et al. Health-related quality of life and health utility values in beta thalassemia major patients receiving different types of iron chelators in Iran. Int. J. Hematol. Oncol. Stem Cell Res. 2016, 10, 224–231. [Google Scholar] [PubMed]
- Shargian-Alon, L.; Pasvolsky, O.; Raanani, P. Thalassemia major and intermedia in patients older than 35 years: A single center experience. Isr. Med. Assoc. J. 2017, 19, 767–771. [Google Scholar] [PubMed]
- Shawkat, A.J.; Jwaid, A.H.; Awad, G.M. Evaluating health-related quality of life (HRQOL) in Iraqi adult and pediatric patients with beta-thalassemia major using two different iron chelation therapies. Iraqi J. Pharm. Sci. 2019, 28, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Soliman, A.T.; Yassin, M.A.; De Sanctis, V. Final adult height and endocrine complications in young adults with beta-thalassemia major (TM) who received oral iron chelation (OIC) in comparison with those who did not use OIC. Acta Biomed. 2018, 89 (Suppl. S2), 27–32. [Google Scholar] [PubMed]
- Lee, K.T.; Lim, S.L.; Goh, A.S. Prevalence of endocrine complications in transfusion dependent thalassemia in Hospital Pulau Pinang: A pilot study. Med. J. Malays. 2020, 75, 33–37. [Google Scholar]
- Vitrano, A.; Calvaruso, G.; Lai, E.; Colletta, G.; Quota, A.; Gerardi, C.; Rigoli, L.C.; Pitrolo, L.; Cuccia, L.; Gagliardotto, F.; et al. The era of comparable life expectancy between thalassaemia major and intermedia: Is it time to revisit the major-intermedia dichotomy? Br. J. Haematol. 2017, 176, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Author, Year | Study Design | Country | Setting | Duration of Follow-Up | Sample Size (n) | Outcomes of Interest Reported |
|---|---|---|---|---|---|---|
| Ang, 2014 [17] | Retrospective cohort | UK | Hospital | NR | 92 | Endocrine complications |
| Chen, 2015 [18] | Retrospective case-control | Taiwan | NR | Median: 2.8 years | 37 | Cardiac outcomes |
| Chirico, 2013 [19] | Prospective cohort with randomized phase | Italy | Outpatient or clinic | NR | Total: 72 TM: 51 TI: 21 | Endocrine complications |
| Chirico, 2015 [20] | Prospective cohort | Italy | Outpatient or clinic | NR | Overall: 72 TM: 51 TI: 21 | Endocrine complications |
| Ebrahimpour, 2012 [21] | Prospective cross-sectional | Iran | Outpatient or clinic | NR | Overall: 80 Subgroup with normal BMD: 50 Subgroup with osteomalacia/osteoporosis: 30 | Skeletal outcomes |
| Foroughi, 2015 [22] | Cross-sectional | Iran | Outpatient or clinic | NR | Total: 86 TM: 39 TI: 47 | Skeletal outcomes |
| Hahalis, 2009 [23] | Prospective case-control | Greece | Outpatient or clinic | Mean: 10.7 years | 36 | Mortality |
| Musallam, 2012 [24] | Retrospective cohort | Italy | Outpatient or clinic | 4 years | Overall: 42 Non-chelated: 28 Chelated: 14 | Liver outcomes |
| Poggi, 2016 [25] | Retrospective cohort | Italy | Outpatient or clinic | NR | 165 | Endocrine complications |
| Vlahos, 2012 [26] | Prospective cohort | Greece | Hospital | NR | 27 | Pulmonary outcomes |
| Age | Male Sex | Time Since Diagnosis | TM Patients | TI Patients | Definition of TD/ TD Patients | Patients Receiving Transfusion | Baseline Serum Ferritin |
|---|---|---|---|---|---|---|---|
| Chirico, 2013 [19]; Italy | |||||||
| TM, mean (SD): 34.4 (9.7) years TI, mean (SD): 38.5 (19.4) years | Overall: 47.2% | NR | 70.8% | 29.2% | Definition NR (TM patients presumed TD) TM: 100% TI: 48% | TM: 100% TI: 76% | TM, mean (range): 872 (541–1921) µg/L TI, mean (range): 670 (480–1345) µg/L |
| Foroughi, 2015 [22]; Iran | |||||||
| β-TI with hydroxyurea, mean (SD): 26.7 (7.8) years β-TI without hydroxyurea, mean (SD): 20.7 (7.2) years | β-TI with hydroxyurea: 64% β-TI without hydroxyurea: 50% | NR | 0 | 100% | NR NR | NR | β-TI with hydroxyurea, mean (SD): 762 (602) ng/cc β-TI without hydroxyurea, mean (SD): 518 (461) ng/cc |
| Ang, 2014 [17]; UK | |||||||
| Mean (range): 36 (18–59) years | 48% | NR | 100% | 0 | Definition NR (TM patients presumed TD) 100% | 100% | Median 10-year average (range): 2042 (501–10,101) µg/L |
| Chen, 2015 [18]; Taiwan | |||||||
| Mean (SD): 24.2 (5.5) years | 56.8% | Mean (SD): 22.04 (6.5) years (time from disease onset) | NR | NR | NA NR | 100% | Mean (SD): 2476.8 (300.6) |
| Chirico, 2015 [20]; Italy | |||||||
| TM, mean (SD): 34.4 (9.7) years TI, mean (SD): 38.5 (19.4) years | TM: 51% TI: 38% | NR | Of overall: 70.8% | Of overall: 29.2% | Definition NR For TI: 48% dependent on hemotransfusion, 28% occasionally transfused | Of overall: 93% | TM, mean (range): 872 (541–1921) µg/L TI, mean (range): 670 (480–1345) µg/L |
| Ebrahimpour, 2012 [21]; Iran | |||||||
| Normal BMD, mean (SD): 24.55 (0.75) years Osteomalacia/ osteoporosis, mean (SD): 28.69 (1.56) years | Normal BMD: 57% Osteomalacia/ osteoporosis: 52% | NR | 61% | 39% | Regular transfusion therapy: 100% | 100% | Normal BMD, mean (SD): 1912.21 (247.95) mg/g/dw Osteomalacia/ osteoporosis, mean (SD): 1293.39 (249.76) mg/g/dw |
| Hahalis, 2009 [23]; Greece | |||||||
| At study start, mean (SD): 23 (5) years At study termination, mean (SD): 37 (6) years At time of death, mean (SD): 25 (3) years | 44% | NR | 100% | 0 | Need for regular transfusions since the first months of life: 100% | 100% | Median (IQR), ng/mL: 3140 (2150–3880) |
| Musallam, 2012 [24]; Italy | |||||||
| Overall, median (range): 38 (26–54) years | 50% | NR | 0 | 100% | NR 0 | NR | Overall: first measurement, µg/L; median (IQR): 580.0 (332.3–925.3) Non-chelated: first measurement, µg/L; median (IQR): 515.0 (302.5–901.3) Chelated: first measurement, µg/L; median (IQR): 636.5 (415.5–1554.5) |
| Poggi, 2016 [25]; Italy | |||||||
| Mean (SD): 39.9 (8.3) years | 43% | NR | 100% | 0 | Definition NR (TM): 100% | 100% | Median (range) over 5 years: 555 ng/mL (63–6140) |
| Vlahos, 2012 [26]; Greece | |||||||
| Pulmonary HTN absent, mean (SD): 37.7 (7.7) years Pulmonary HTN present, mean (SD): 42.6 (14.5) years | Pulmonary HTN absent: 68.2% Pulmonary HTN present: 80% | NR | 100% | 0 | Definition NR (TM patients): 100% | 100% | Pulmonary HTN absent, mean (SD): 1181 (755) µg/L Pulmonary HTN present, mean (SD): 2440 (1836) µg/L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, F.; Huey, K.; Deshpande, S.; Turner, M.; Chitnis, M.; Schiller, E.; Yucel, A.; Moro Bueno, L.; Oliva, E.N. Relationship between Serum Ferritin and Outcomes in β-Thalassemia: A Systematic Literature Review. J. Clin. Med. 2022, 11, 4448. https://doi.org/10.3390/jcm11154448
Shah F, Huey K, Deshpande S, Turner M, Chitnis M, Schiller E, Yucel A, Moro Bueno L, Oliva EN. Relationship between Serum Ferritin and Outcomes in β-Thalassemia: A Systematic Literature Review. Journal of Clinical Medicine. 2022; 11(15):4448. https://doi.org/10.3390/jcm11154448
Chicago/Turabian StyleShah, Farrukh, Krystal Huey, Sohan Deshpande, Monica Turner, Madhura Chitnis, Emma Schiller, Aylin Yucel, Luciana Moro Bueno, and Esther Natalie Oliva. 2022. "Relationship between Serum Ferritin and Outcomes in β-Thalassemia: A Systematic Literature Review" Journal of Clinical Medicine 11, no. 15: 4448. https://doi.org/10.3390/jcm11154448