
Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim of the Study
2.2. Participants
2.3. Description of the Telemedical Intervention
2.3.1. TelePark-App and Patient Management Platform
2.3.2. Video Visits
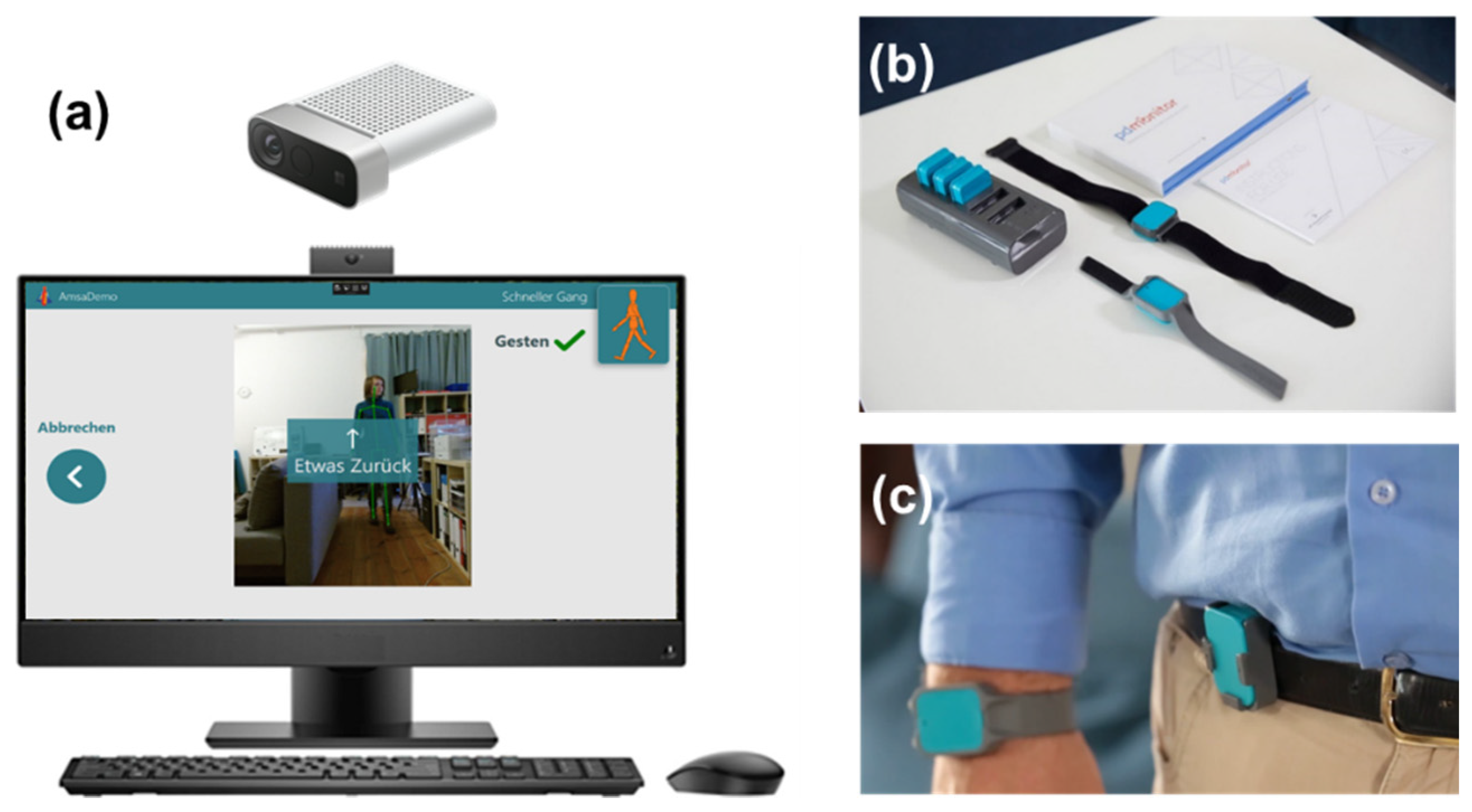
2.3.3. Wearable Sensors
2.3.4. Camera System
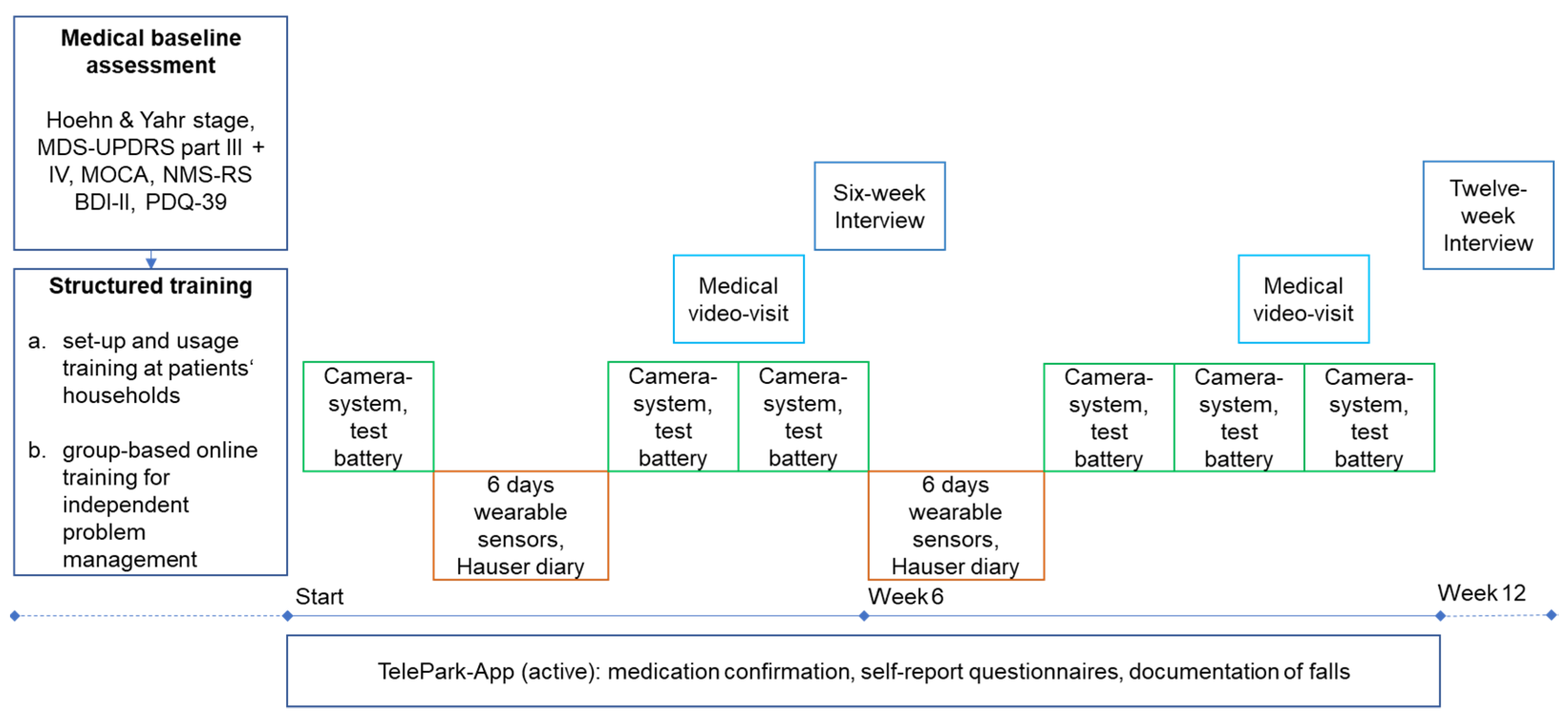
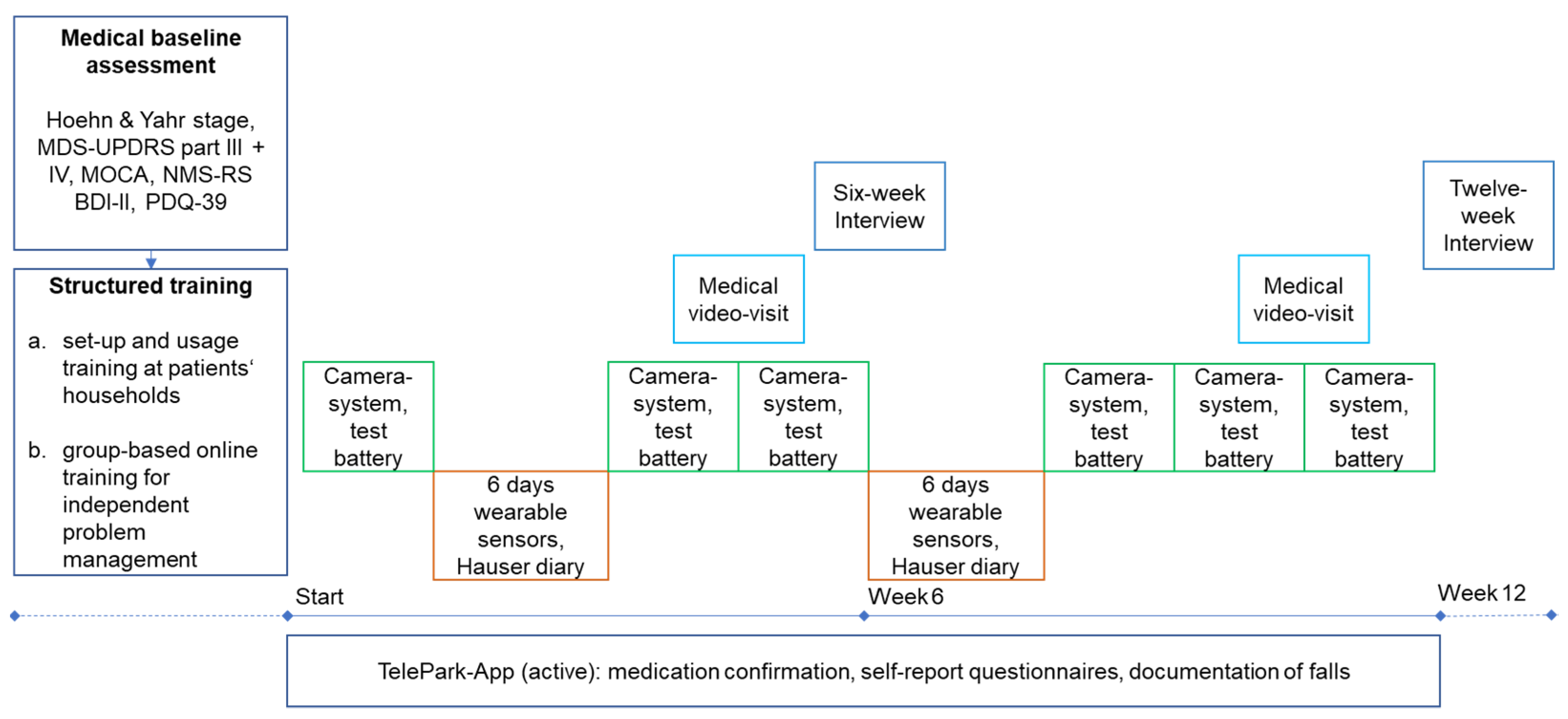
2.4. Course of the Study
2.5. Evaluation
2.5.1. Semi-Standardized Telephone Interview (Six-Week Interview)
2.5.2. Semi-Standardized Telephone Interview (Twelve-Week Interview)
2.5.3. Statistical Analyses
3. Results
3.1. Demographic Data and Study Completion
3.2. Effects on Quality of Life
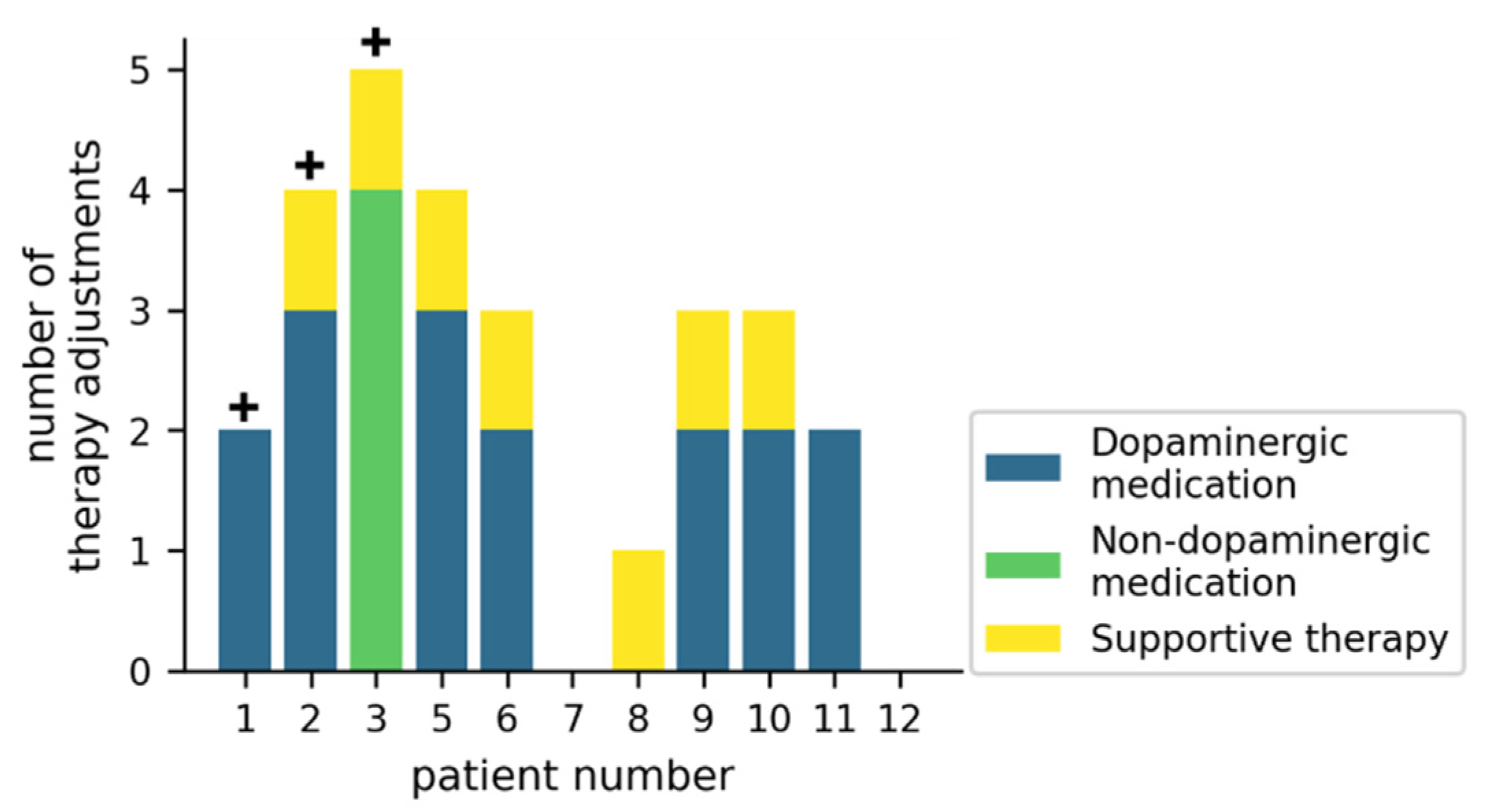
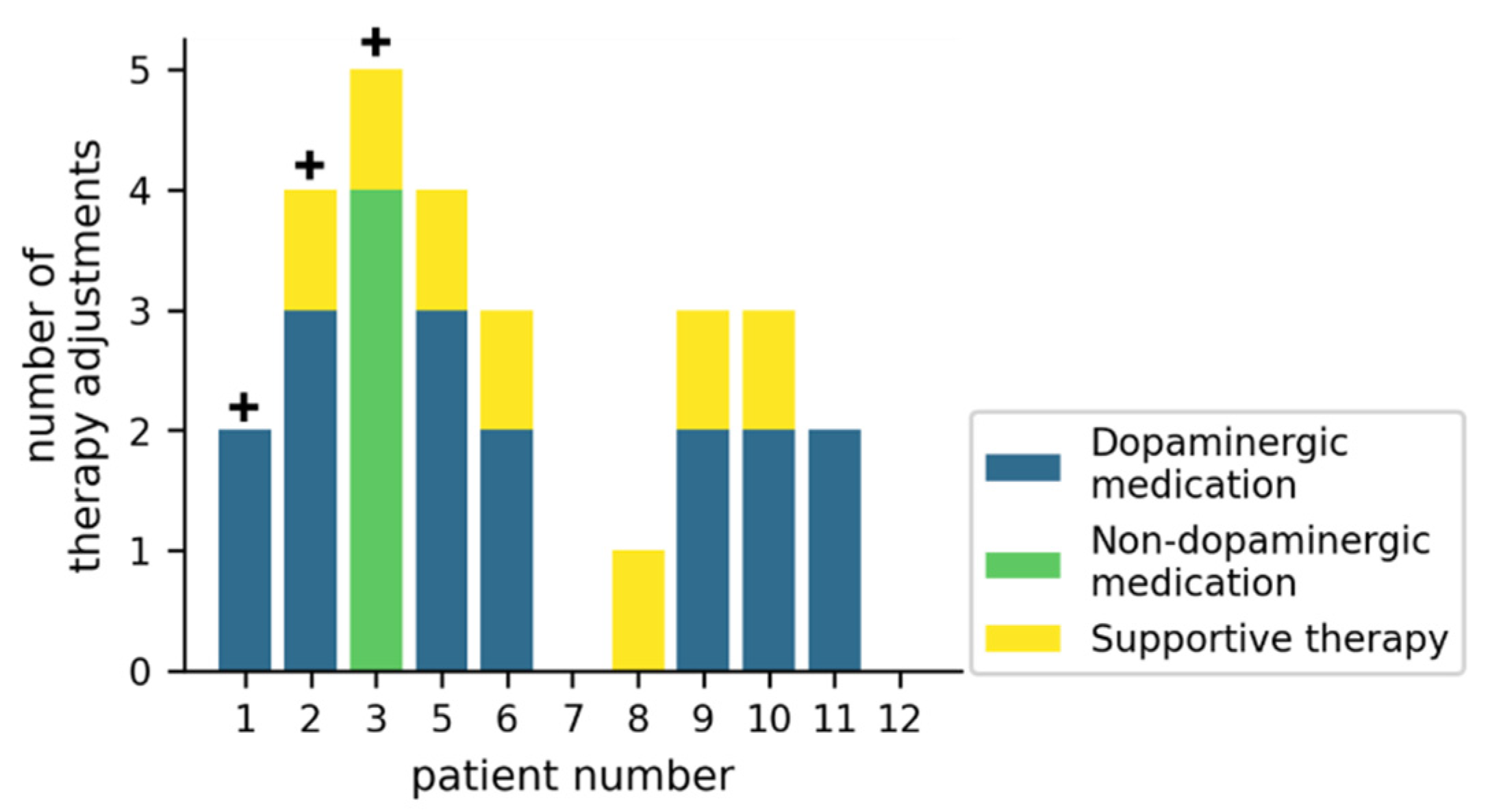
3.3. Effects on Medication and Supportive Therapy
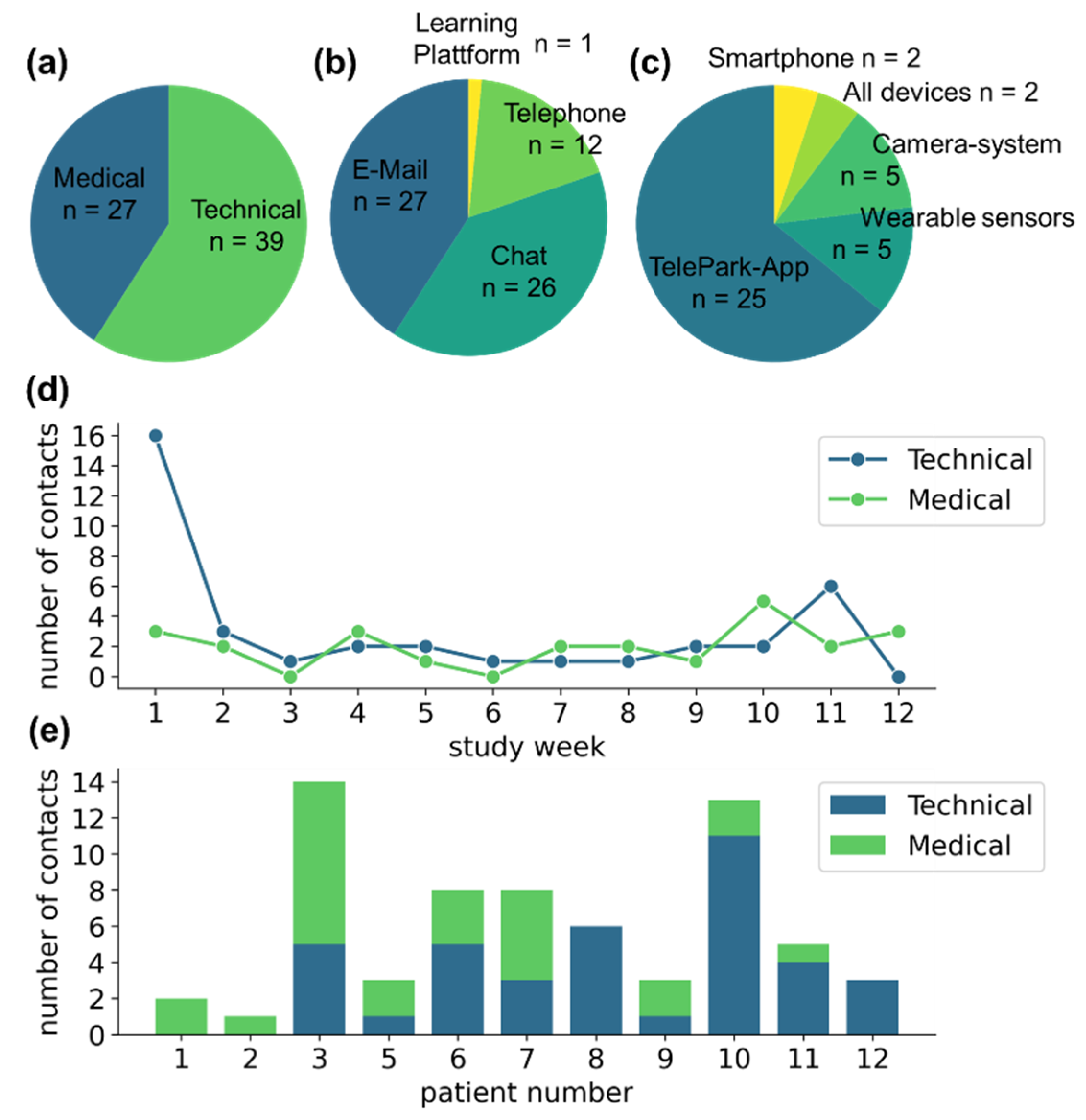
3.4. Contacts with the TelePark-Team
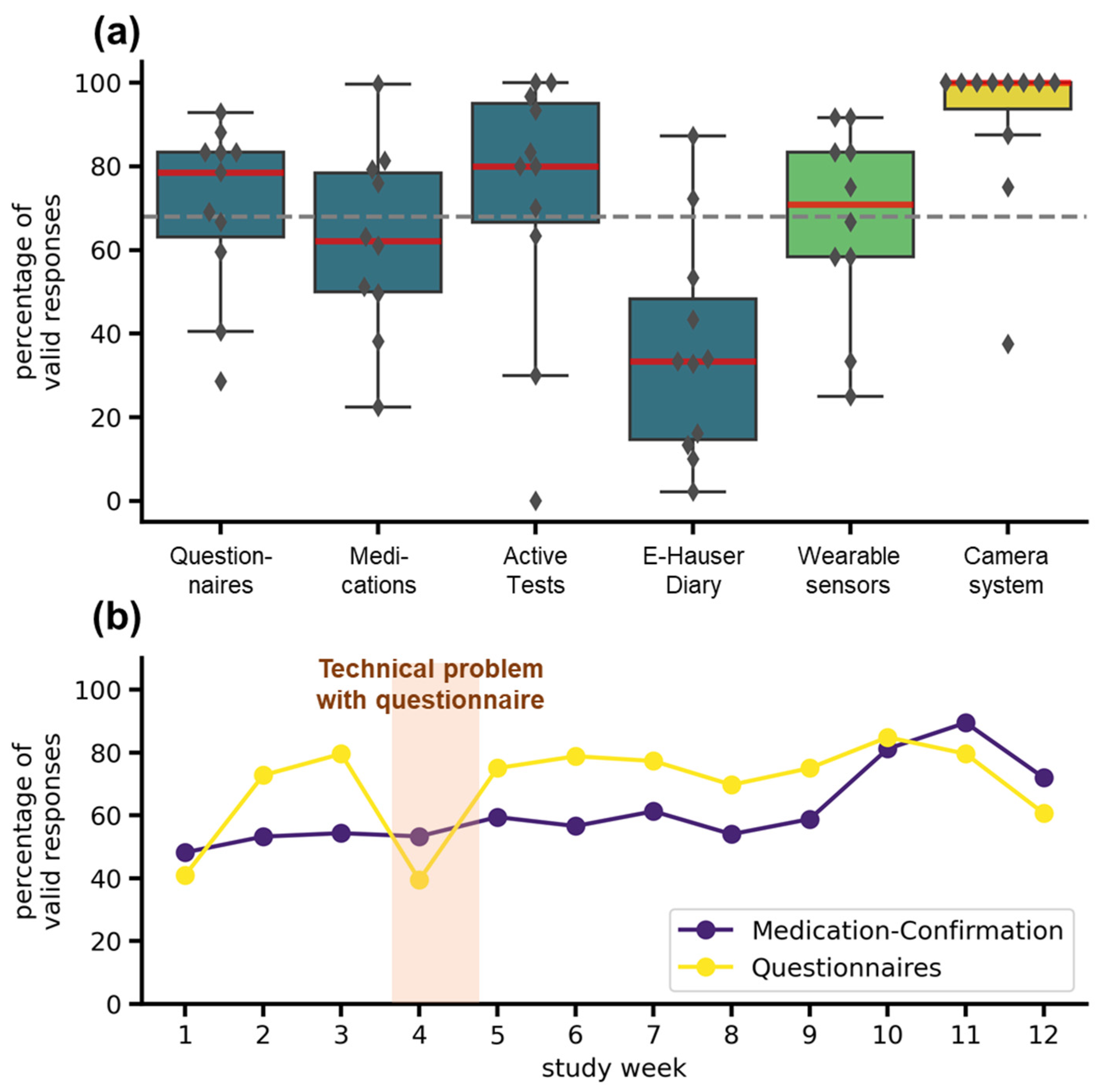
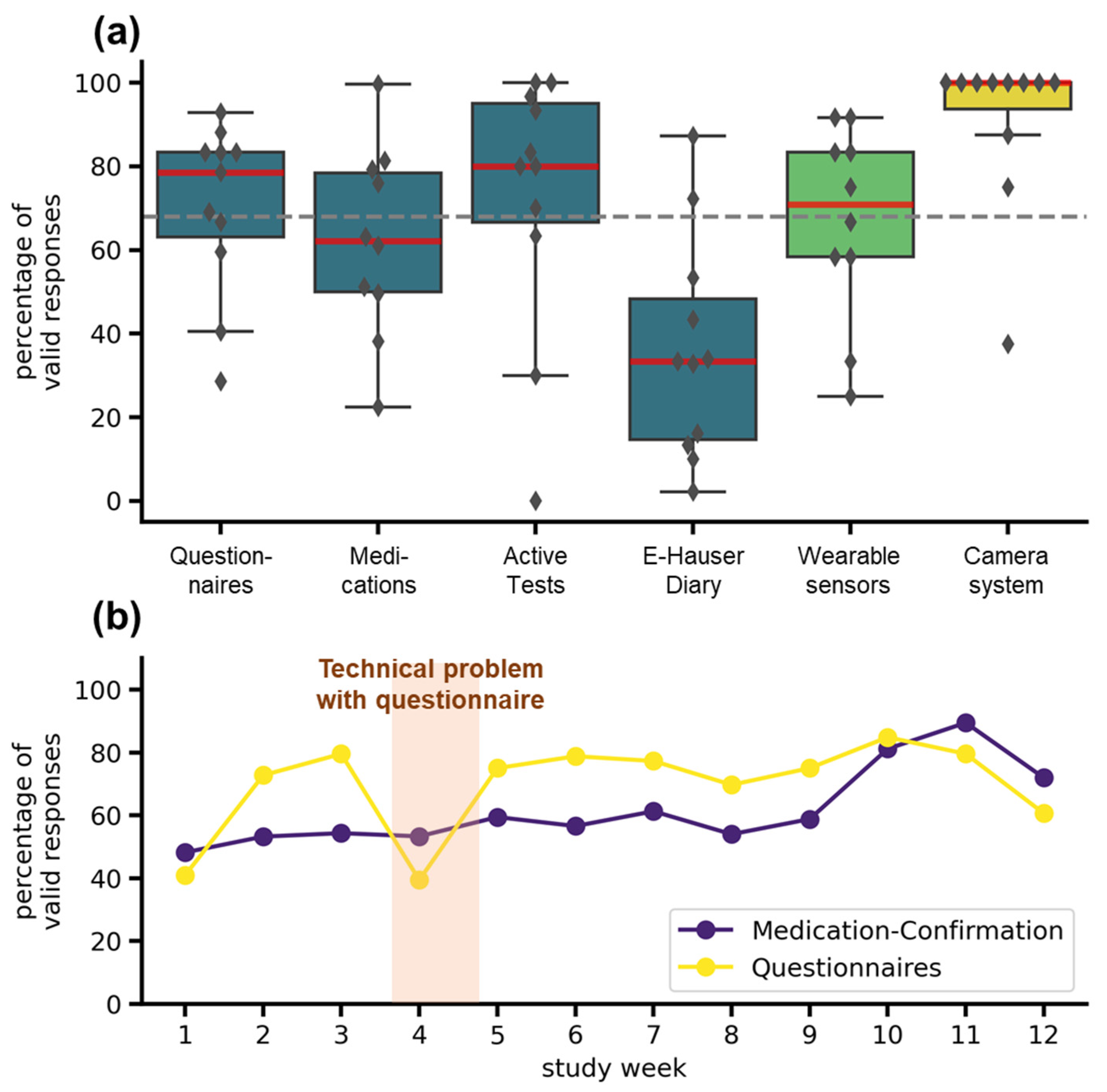
3.5. Adherence
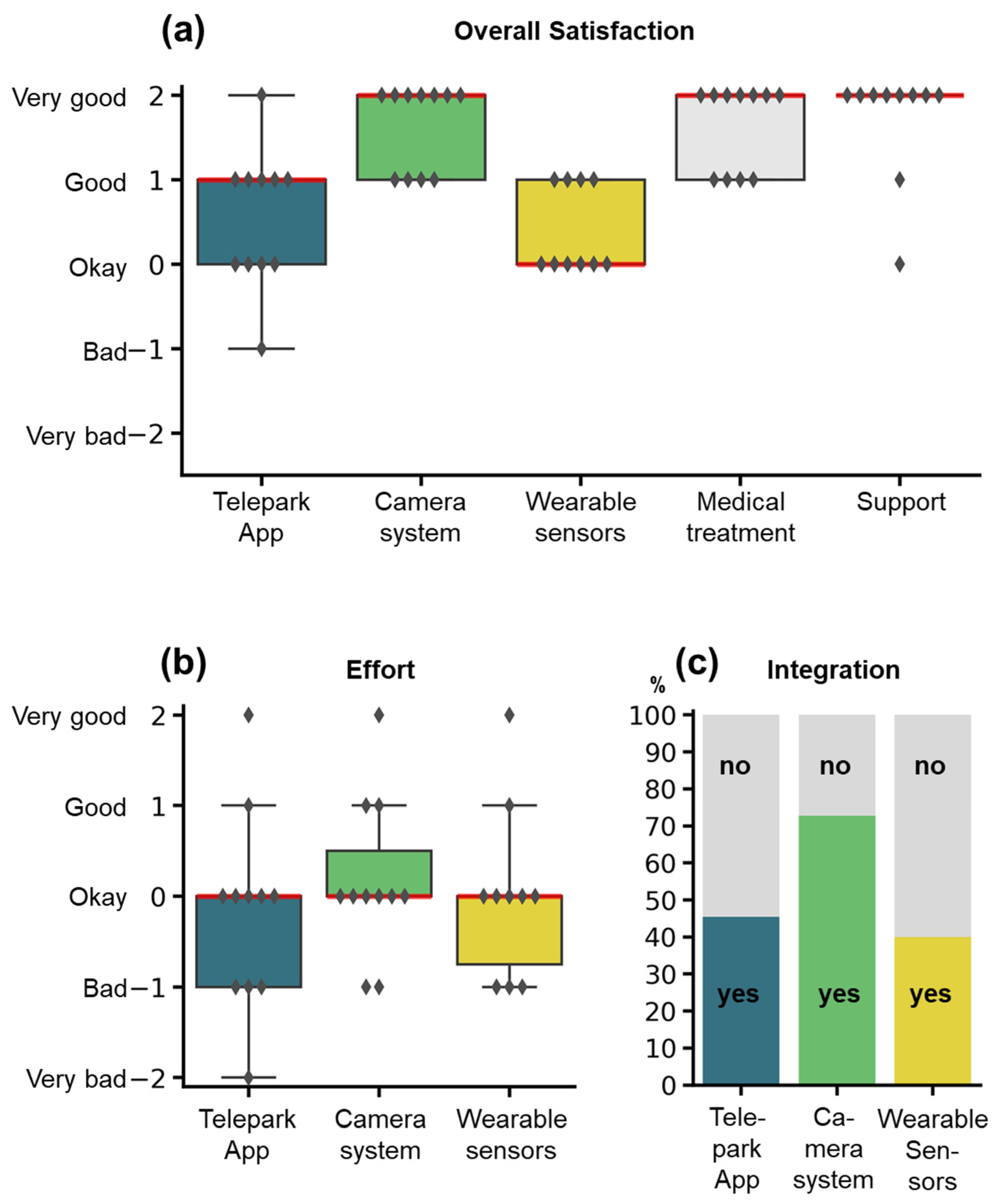
3.6. Participant Experience and Usability
3.6.1. Six-Week Interview
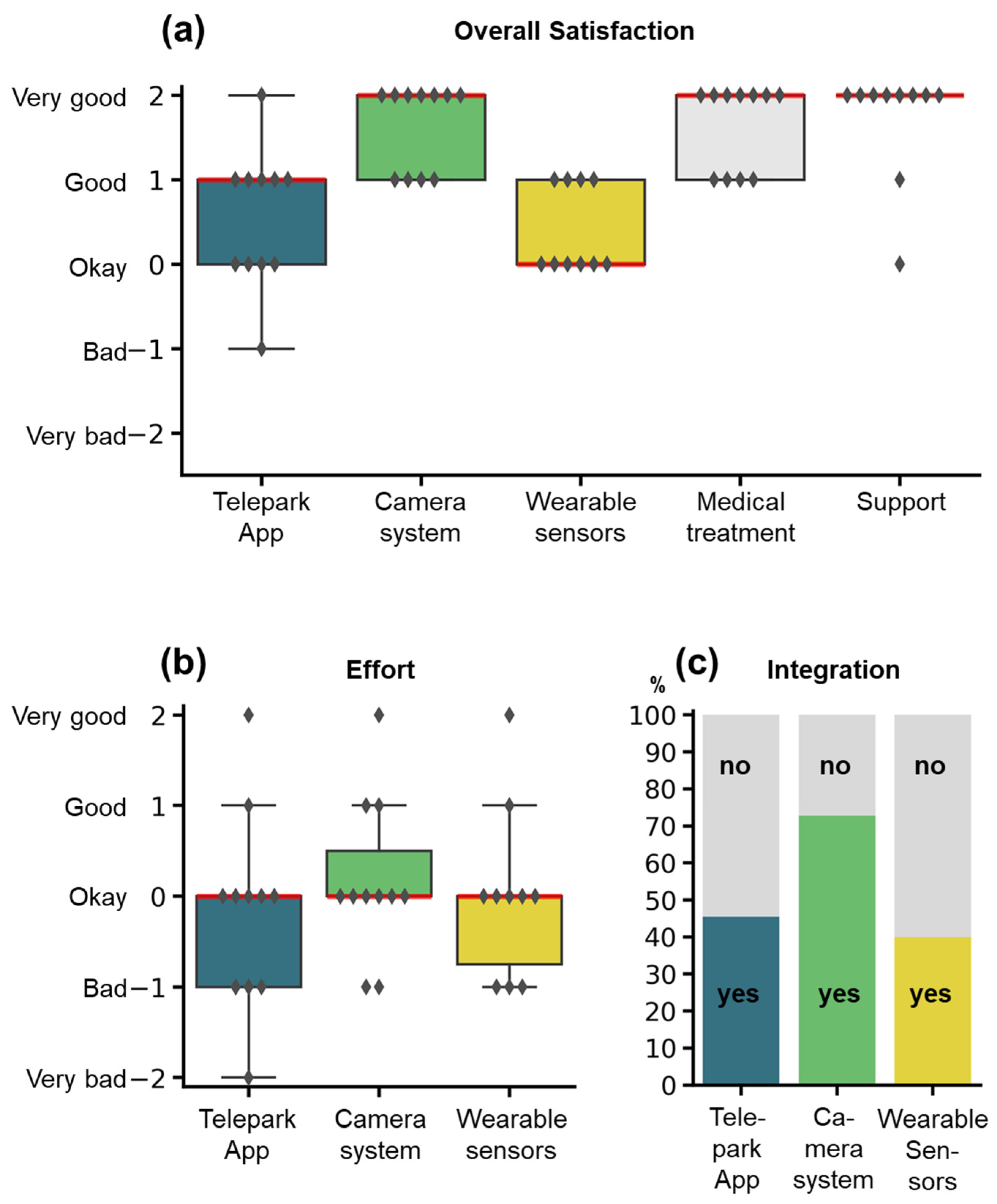
3.6.2. Twelve-Week Interview
Pat_02: “I found the exercises [from the camera-system] and also the gesture control very interesting.”
Pat_06: “Now that I’m not exactly slim built, the belly sensor was a little too tight for me.”
Pat_09: “I often received silly looks from outsiders.”
Pat_03: “The constant beeping [of the smartphone], no matter where you were, that was of course annoying over time.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ray Dorsey, E.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.Y.J.; Collado-Mateo, D.; et al. Global, Regional, and National Burden of Parkinson’s Disease, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet. Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Berger, K.; Chen, H.; Leslie, D.; Mailman, R.B.; Huang, X. Projection of the Prevalence of Parkinson’s Disease in the Coming Decades: Revisited. Mov. Disord. 2018, 33, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Wanneveich, M.; Moisan, F.; Jacqmin-Gadda, H.; Elbaz, A.; Joly, P. Projections of Prevalence, Lifetime Risk, and Life Expectancy of Parkinson’s Disease (2010–2030) in France. Mov. Disord. 2018, 33, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.L.; Bush, E.J.; Mary Jo Cooley, H.; Phillips Carrico, C.; Sundin, S. Considering Health Care Needs in a Rural Parkinson Disease Community. Prog. Community Health Partnersh. Res. Educ. Action 2020, 14, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Dorsey, E.R.; Bloem, B.R. The Parkinson Pandemic—A Call to Action. JAMA Neurol. 2018, 75, 9–10. [Google Scholar] [CrossRef]
- Powers, R.; Etezadi-Amoli, M.; Arnold, E.M.; Kianian, S.; Mance, I.; Gibiansky, M.; Trietsch, D.; Alvarado, A.S.; Kretlow, J.D.; Herrington, T.M.; et al. Smartwatch Inertial Sensors Continuously Monitor Real-World Motor Fluctuations in Parkinson’s Disease. Sci. Transl. Med. 2021, 13, 7865. [Google Scholar] [CrossRef]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers, E.M.J.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of Free-Living Gait in Older Adults With and Without Parkinson’s Disease and With and Without a History of Falls: Identifying Generic and Disease-Specific Characteristics. J. Gerontol. Ser. A 2019, 74, 500–506. [Google Scholar] [CrossRef]
- Ossig, C.; Gandor, F.; Fauser, M.; Bosredon, C.; Churilov, L.; Reichmann, H.; Horne, M.K.; Ebersbach, G.; Storch, A. Correlation of Quantitative Motor State Assessment Using a Kinetograph and Patient Diaries in Advanced PD: Data from an Observational Study. PLoS ONE 2016, 11, e0161559. [Google Scholar] [CrossRef]
- Omberg, L.; Chaibub Neto, E.; Perumal, T.M.; Pratap, A.; Tediarjo, A.; Adams, J.; Bloem, B.R.; Bot, B.M.; Elson, M.; Goldman, S.M.; et al. Remote Smartphone Monitoring of Parkinson’s Disease and Individual Response to Therapy. Nat. Biotechnol. 2021, 33, 1–8. [Google Scholar] [CrossRef]
- Lipsmeier, F.; Taylor, K.I.; Kilchenmann, T.; Wolf, D.; Scotland, A.; Schjodt-Eriksen, J.; Cheng, W.Y.; Fernandez-Garcia, I.; Siebourg-Polster, J.; Jin, L.; et al. Evaluation of Smartphone-Based Testing to Generate Exploratory Outcome Measures in a Phase 1 Parkinson’s Disease Clinical Trial. Mov. Disord. 2018, 33, 1287–1297. [Google Scholar] [CrossRef]
- Myers, T.L.; Tarolli, C.G.; Adams, J.L.; Barbano, R.; Cristina Gil-Díaz, M.; Spear, K.L.; Lowell, J.; Daeschler, M.; Riley, L.; Amondikar, N.; et al. Video-Based Parkinson’s Disease Assessments in a Nationwide Cohort of Fox Insight Participants. Clin. Park. Relat. Disord. 2021, 4, 100094. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.A.; Beran, D.B.; Biglan, K.M.; Boyd, C.M.; Dorsey, E.R.; Schmidt, P.N.; Simone, R.; Willis, A.W.; Galifianakis, N.B.; Katz, M.; et al. National Randomized Controlled Trial of Virtual House Calls for Parkinson Disease. Neurology 2017, 89, 1152. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.; Zeeshan, A.; Dougherty, M. A Novel Method for Automatic Classification of Parkinson Gait Severity Using Front-View Video Analysis. Technol. HealthCare 2021, 29, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, J.; Hu, C.; Ma, Y.; Ge, D.; Miao, S.; Xue, Y.; Li, L. Vision-Based Method for Automatic Quantification of Parkinsonian Bradykinesia. IEEE Trans. Neural. Syst. Rehabil. Eng. 2019, 27, 1952–1961. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Qu, Y.; Zhang, L.; Gao, Z. Diagnosing Parkinson Disease Through Facial Expression Recognition: Video Analysis. J. Med. Internet Res. 2020, 22, e18697. [Google Scholar] [CrossRef] [PubMed]
- Sica, M.; Tedesco, S.; Crowe, C.; Kenny, L.; Moore, K.; Timmons, S.; Barton, J.; O’Flynn, B.; Komaris, D.S. Continuous Home Monitoring of Parkinson’s Disease Using Inertial Sensors: A Systematic Review. PLoS ONE 2021, 16, e0246528. [Google Scholar] [CrossRef]
- Sibley, K.G.; Girges, C.; Hoque, E.; Foltynie, T. Video-Based Analyses of Parkinson’s Disease Severity: A Brief Review. J. Park. Dis. 2021, 11, S83–S93. [Google Scholar] [CrossRef]
- Little, M.A. Smartphones for Remote Symptom Monitoring of Parkinson’s Disease. J. Park. Dis. 2021, 11 (Suppl. 1), S49–S53. [Google Scholar] [CrossRef]
- Gatsios, D.; Antonini, A.; Gentile, G.; Marcante, A.; Pellicano, C.; MacChiusi, L.; Assogna, F.; Spalletta, G.; Gage, H.; Touray, M.; et al. Feasibility and Utility of MHealth for the Remote Monitoring of Parkinson Disease: Ancillary Study of the PD_manager Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e16414. [Google Scholar] [CrossRef]
- Isaacson, S.H.; Boroojerdi, B.; Waln, O.; McGraw, M.; Kreitzman, D.L.; Klos, K.; Revilla, F.J.; Heldman, D.; Phillips, M.; Terricabras, D.; et al. Effect of Using a Wearable Device on Clinical Decision-Making and Motor Symptoms in Patients with Parkinson’s Disease Starting Transdermal Rotigotine Patch: A Pilot Study. Park. Relat. Disord. 2019, 64, 132–137. [Google Scholar] [CrossRef]
- Van den Bergh, R.; Bloem, B.R.; Meinders, M.J.; Evers, L.J.W. The State of Telemedicine for Persons with Parkinson’s Disease. Curr. Opin. Neurol. 2021, 34, 589–597. [Google Scholar] [CrossRef] [PubMed]
- De Lima, A.L.S.; Hahn, T.; Evers, L.J.W.; De Vries, N.M.; Cohen, E.; Afek, M.; Bataille, L.; Daeschler, M.; Claes, K.; Boroojerdi, B.; et al. Feasibility of Large-Scale Deployment of Multiple Wearable Sensors in Parkinson’s Disease. PLoS ONE 2017, 12, e0189161. [Google Scholar] [CrossRef] [Green Version]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s Disease Questionnaire (PDQ-39): Development and Validation of a Parkinson’s Disease Summary Index Score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Berger, K.; Broll, S.; Winkelmann, J.; Heberlein, I.; Müller, T.; Ries, V. Reliability Analysis of the PDQ-39 (German Version). Aktuelle Neurol. 1999, 26, 180–184. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple-Alford, J.C.; MacAskill, M.R.; Nakas, C.T.; Livingston, L.; Graham, C.; Crucian, G.P.; Melzer, T.R.; Kirwan, J.; Keenan, R.; Wells, S.; et al. The MoCA. Neurology 2010, 75, 1717–1725. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, Progression and Mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Rodriguez-Blazquez, C.; Kurtis, M.M.; Chaudhuri, K.R. The Impact of Non-Motor Symptoms on Health-Related Quality of Life of Patients with Parkinson’s Disease. Mov. Disord. 2011, 26, 399–406. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories -IA and -II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.A.; Friedlander, J.; Zesiewicz, T.A.; Adler, C.H.; Seeberger, L.C.; O’Brien, C.F.; Molho, E.S.; Factor, S.A. A Home Diary to Assess Functional Status in Patients with Parkinson’s Disease with Motor Fluctuations and Dyskinesia. Clin. Neuropharmacol. 2000, 23, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Hartelt, E.; Scherbaum, R.; Kinkel, M.; Gold, R.; Muhlack, S.; Tönges, L. Parkinson’s Disease Multimodal Complex Treatment (PD-MCT): Analysis of Therapeutic Effects and Predictors for Improvement. J. Clin. Med. 2020, 9, 1874. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Bolling, K.; Mao, W.; Reichstadt, J.; Jeste, D.; Kim, H.-C.; Nebeker, C. Technology to Support Aging in Place: Older Adults’ Perspectives. Healthcare 2019, 7, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouça-machado, R.; Pona-ferreira, F.; Leitão, M.; Clemente, A.; Vila-viçosa, D.; Kauppila, L.A.; Costa, R.M.; Matias, R.; Ferreira, J.J. Feasibility of a Mobile-based System for Unsupervised Monitoring in Parkinson’s Disease. Sensors 2021, 21, 4972. [Google Scholar] [CrossRef]
- Pérez-Jover, V.; Sala-González, M.; Guilabert, M.; Mira, J.J. Mobile Apps for Increasing Treatment Adherence: Systematic Review. J. Med. Internet Res. 2019, 21, e12505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakshminarayana, R.; Wang, D.; Burn, D.; Chaudhuri, K.R.; Galtrey, C.; Guzman, N.V.; Hellman, B.; James, B.; Pal, S.; Stamford, J.; et al. Using a Smartphone-Based Self-Management Platform to Support Medication Adherence and Clinical Consultation in Parkinson’s Disease. NPJ Park. Dis. 2017, 3, 2. [Google Scholar] [CrossRef]
- Llorens-Vernet, P.; Miró, J. Standards for Mobile Health-Related Apps: Systematic Review and Development of a Guide. JMIR mHealth uHealth 2020, 8, e13057. [Google Scholar] [CrossRef]
- Chatzipavlou, I.A.; Christoforidou, S.A.; Vlachopoulou, M. A Recommended Guideline for the Development of MHealth Apps. mHealth 2016, 2, 21. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Study Cohort |
|---|---|
| Number of patients, n | 11 |
| Age, mean (SD) | 65 (9.2) |
| Sex, n: female; male | 5; 6 |
| Hoehn and Yahr stage, median (Range) | 2 (1–4) |
| Disease duration, mean (SD) | 7 (5.7) |
| MDS-UPDRS III score, mean (SD) | 30 (18.1) |
| MDS-UPDRS IV score, mean (SD) | 4 (6.0) |
| NMS-RS score, mean (SD) | 70 (34.3) |
| MOCA score, mean (SD) | 27 (2.9) |
| BDI-II score, mean (SD) | 15 (10.7) |
| PDQ-39 score, mean (SD) | 20 (9.5) |
| TelePark-App | Wearable Sensors | Camera-System | |
|---|---|---|---|
| Frequency of difficulties * concerning | |||
| Technical operability, n | 10 | 9 | 4 |
| Legibility of the font/recognizability of operating elements, n | 5 | NA | 0 |
| Navigation/fault tolerance, n | 7 | NA | 1 |
| Understanding the functioning, n | 4 | 2 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendig, J.; Wolf, A.-S.; Mark, T.; Frank, A.; Mathiebe, J.; Scheibe, M.; Müller, G.; Stahr, M.; Schmitt, J.; Reichmann, H.; et al. Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study. J. Clin. Med. 2022, 11, 1074. https://doi.org/10.3390/jcm11041074
Bendig J, Wolf A-S, Mark T, Frank A, Mathiebe J, Scheibe M, Müller G, Stahr M, Schmitt J, Reichmann H, et al. Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study. Journal of Clinical Medicine. 2022; 11(4):1074. https://doi.org/10.3390/jcm11041074
Chicago/Turabian StyleBendig, Jonas, Anna-Sophie Wolf, Tony Mark, Anika Frank, Josephine Mathiebe, Madlen Scheibe, Gabriele Müller, Marcus Stahr, Jochen Schmitt, Heinz Reichmann, and et al. 2022. "Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study" Journal of Clinical Medicine 11, no. 4: 1074. https://doi.org/10.3390/jcm11041074
APA StyleBendig, J., Wolf, A.-S., Mark, T., Frank, A., Mathiebe, J., Scheibe, M., Müller, G., Stahr, M., Schmitt, J., Reichmann, H., Loewenbrück, K. F., & Falkenburger, B. H. (2022). Feasibility of a Multimodal Telemedical Intervention for Patients with Parkinson’s Disease—A Pilot Study. Journal of Clinical Medicine, 11(4), 1074. https://doi.org/10.3390/jcm11041074