
Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients

 , , , and
, , , and
Abstract
1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ojo, A.O.; Morales, J.M.; González-Molina, M.; Steffick, D.E.; Luan, F.L.; Merion, R.M.; Ojo, T.; Moreso, F.; Arias, M.; Campistol, J.M.; et al. Comparison of the long-term outcomes of kidney transplantation: USA versus Spain. Nephrol. Dial. Transplant. 2013, 28, 213–220. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moreso, F.; Hernandez, D. Has the survival of the graft improved after renal transplantation in the era of modern immunosuppression? Nefrologia 2013, 33, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Sola, E.; Gonzalez-Molina, M.; Cabello, M.; Burgos, D.; Ramos, J.; Gutierrez, C.; Lopez, V.; Soler, J.; de la Vega, E.; Hernandez, D. Long-term improvement of deceased donor renal allograft survival since 1996: A single transplant center study. Transplantation 2010, 89, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Haas, M.; Solez, K.; Racusen, L.; Glotz, D.; Seron, D.; Nankivell, B.J.; Colvin, R.B.; Afrouzian, M.; Akalin, E.; et al. The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology. Am. J. Transplant. 2017, 17, 28–41. [Google Scholar] [CrossRef]
- Ortiz, F.; Gelpi, R.; Helanterä, I.; Melilli, E.; Honkanen, E.; Bestard, O.; Grinyo, J.M.; Cruzado, J.M. Decreased Kidney Graft Survival in Low Immunological Risk Patients Showing Inflammation in Normal Protocol Biopsies. PLoS ONE 2016, 11, e0159717. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Sood, P.; Hariharan, S. Subclinical Rejection in Renal Transplantation: Reappraised. Transplantation 2016, 100, 1610–1618. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Bhusal, S.; Randhawa, P.; Sood, P.; Cherukuri, A.; Wu, C.; Puttarajappa, C.; Hoffman, W.; Shah, N.; Mangiola, M.; et al. Short-term adverse effects of early subclinical allograft inflammation in kidney transplant recipients with a rapid steroid withdrawal protocol. Am. J. Transplant. 2018, 18, 1710–1717. [Google Scholar] [CrossRef]
- Rush, D.N.; Gibson, I.W. Subclinical Inflammation in Renal Transplantation. Transplantation 2019, 103, e139–e145. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Agrawal, N.; Sharma, A.; Taverniti, A.; P’Ng, C.H.; Shingde, M.; Wong, G.; Chapman, J.R. The clinical and pathological significance of borderline T cell-mediated rejection. Am. J. Transplant. 2019, 19, 1452–1463. [Google Scholar] [CrossRef]
- Shapiro, R.; Randhawa, P.; Jordan, M.L.; Scantlebury, V.P.; Vivas, C.; Jain, A.; Corry, R.J.; McCauley, J.; Johnston, J.; Donaldson, J.; et al. An analysis of early renal transplant protocol biopsies--the high incidence of subclinical tubulitis. Am. J. Transplant. 2001, 1, 47–50. [Google Scholar] [CrossRef]
- Choi, B.S.; Shin, M.J.; Shin, S.J.; Kim, Y.S.; Choi, Y.J.; Moon, I.S.; Kim, S.Y.; Koh, Y.B.; Bang, B.K.; Yang, C.W. Clinical significance of an early protocol biopsy in living-donor renal transplantation: Ten-year experience at a single center. Am. J. Transplant. 2005, 5, 1354–1360. [Google Scholar] [CrossRef]
- Van Loon, E.; Lerut, E.; Senev, A.; Coemans, M.; Pirenne, J.; Monbaliu, D.; Jochmans, I.; Sainz Barriga, M.; De Vusser, K.; Van Craenenbroeck, A.H.; et al. The Histological Picture of Indication Biopsies in the First 2 Weeks after Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2020, 15, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Opelz, G.; Döhler, B. Effect of human leukocyte antigen compatibility on kidney graft survival: Comparative analysis of two decades. Transplantation 2007, 84, 137–143. [Google Scholar] [CrossRef]
- Lim, W.H.; Chadban, S.J.; Clayton, P.; Budgeon, C.A.; Murray, K.; Campbell, S.B.; Cohney, S.; Russ, G.R.; McDonald, S.P. Human leukocyte antigen mismatches associated with increased risk of rejection, graft failure, and death independent of initial immunosuppression in renal transplant recipients. Clin. Transplant. 2012, 26, E428–E437. [Google Scholar] [CrossRef]
- Williams, R.C.; Opelz, G.; McGarvey, C.J.; Weil, E.J.; Chakkera, H.A. The Risk of Transplant Failure with HLA Mismatch in First Adult Kidney Allografts from Deceased Donors. Transplantation 2016, 100, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Kosmoliaptsis, V.; Pochinco, D.; Gibson, I.W.; Ho, J.; Birk, P.E.; Goldberg, A.; Karpinski, M.; Shaw, J.; Rush, D.N.; et al. HLA-DR/DQ molecular mismatch: A prognostic biomarker for primary alloimmunity. Am. J. Transplant. 2019, 19, 1708–1719. [Google Scholar] [CrossRef]
- Wiebe, C.; Rush, D.N.; Gibson, I.W.; Pochinco, D.; Birk, P.E.; Goldberg, A.; Blydt-Hansen, T.; Karpinski, M.; Shaw, J.; Ho, J.; et al. Evidence for the alloimmune basis and prognostic significance of Borderline T cell-mediated rejection. Am. J. Transplant. 2020, 20, 2499–2508. [Google Scholar] [CrossRef]
- Leeaphorn, N.; Pena, J.R.A.; Thamcharoen, N.; Khankin, E.V.; Pavlakis, M.; Cardarelli, F. HLA-DQ Mismatching and Kidney Transplant Outcomes. Clin. J. Am. Soc. Nephrol. 2018, 13, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Ruck, J.M.; Jackson, A.M.; Massie, A.B.; Segev, D.L.; Desai, N.; Garonzik-Wang, J. Temporal Changes in the Impact of HLA Mismatching Among Pediatric Kidney Transplant Recipients. Transplantation 2019, 103, 1267–1271. [Google Scholar] [CrossRef]
- Williams, R.C.; West, L.J.; Opelz, G. The Risk of Failure with HLA Mismatch and Recipient Age in First Pediatric (<18 years) Kidney Transplants. Transplant. Direct. 2018, 4, e365. [Google Scholar] [CrossRef] [PubMed]
- Foroutan, F.; Friesen, E.L.; Clark, K.E.; Motaghi, S.; Zyla, R.; Lee, Y.; Kamran, R.; Ali, E.; De Snoo, M.; Orchanian-Cheff, A.; et al. Risk Factors for 1-Year Graft Loss After Kidney Transplantation: Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1642–1650. [Google Scholar] [CrossRef]
- Su, X.; Zenios, S.A.; Chakkera, H.; Milford, E.L.; Chertow, G.M. Diminishing significance of HLA matching in kidney transplantation. Am. J. Transplant. 2004, 4, 1501–1508. [Google Scholar] [CrossRef]
- Morales, J.M.; Marcén, R.; Andrés, A.; Molina, M.G.; Castillo, D.D.; Cabello, M.; Capdevila, L.; Campistol, J.M.; Oppenheimer, F.; Serón, D.; et al. Renal transplantation in the modern immunosuppressive era in Spain: Four-year results from a multicenter database focus on post-transplant cardiovascular disease. Kidney Int. Suppl. 2008, S94–S99. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ashby, V.B.; Port, F.K.; Wolfe, R.A.; Wynn, J.J.; Williams, W.W.; Roberts, J.P.; Leichtman, A.B. Transplanting kidneys without points for HLA-B matching: Consequences of the policy change. Am. J. Transplant. 2011, 11, 1712–1718. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.H.; Chapman, J.R.; Coates, P.T.; Lewis, J.R.; Russ, G.R.; Watson, N.; Holdsworth, R.; Wong, G. HLA-DQ Mismatches and Rejection in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2016, 11, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Rush, D.; Arlen, D.; Boucher, A.; Busque, S.; Cockfield, S.M.; Girardin, C.; Knoll, G.; Lachance, J.G.; Landsberg, D.; Shapiro, J.; et al. Lack of benefit of early protocol biopsies in renal transplant patients receiving TAC and MMF: A randomized study. Am. J. Transplant. 2007, 7, 2538–2545. [Google Scholar] [CrossRef] [PubMed]
- Filippone, E.J.; Farber, J.L. Humoral Immune Response and Allograft Function in Kidney Transplantation. Am. J. Kidney Dis. 2015, 66, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.; Jouve, T.; Malvezzi, P.; Süsal, C.; Rostaing, L. Transplantation of Marginal Organs: Immunological Aspects and Therapeutic Perspectives in Kidney Transplantation. Front. Immunol. 2019, 10, 3142. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, J.J.; Ciancio, G.; Guerra, G.; Sageshima, J.; Roth, D.; Goldstein, M.J.; Chen, L.; Kupin, W.; Mattiazzi, A.; Tueros, L.; et al. Lower tacrolimus trough levels are associated with subsequently higher acute rejection risk during the first 12 months after kidney transplantation. Transpl. Int. 2016, 29, 216–226. [Google Scholar] [CrossRef]
- Hill, P.; Cross, N.B.; Barnett, A.N.; Palmer, S.C.; Webster, A.C. Polyclonal and monoclonal antibodies for induction therapy in kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 1, Cd004759. [Google Scholar] [CrossRef]
- de Sandes-Freitas, T.V.; Mazzali, M.; Manfro, R.C.; de Andrade, L.G.M.; Vicari, A.R.; Vinicius de Sousa, M.; Medina Pestana, J.O.; Garcia, V.D.; Rosa de Boni Monteiro de Carvalho, D.; de Matos Esmeraldo, R.; et al. Exploring the causes of the high incidence of delayed graft function after kidney transplantation in Brazil: A multicenter study. Transpl. Int. 2021. [Google Scholar] [CrossRef]
- Nankivell, B.J.; P’Ng, C.H.; Chapman, J.R. Does tubulitis without interstitial inflammation represent borderline acute T cell mediated rejection? Am. J. Transplant. 2019, 19, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Tambur, A.R. Human leukocyte antigen matching in organ transplantation: What we know and how can we make it better (Revisiting the past, improving the future). Curr. Opin. Organ Transplant. 2018, 23, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Wehmeier, C.; Amico, P.; Hirt-Minkowski, P.; Georgalis, A.; Hoenger, G.; Menter, T.; Mihatsch, M.; Burkhalter, F.; Steiger, J.; Dickenmann, M.; et al. Acute Rejection Phenotypes in the Current Era of Immunosuppression: A Single-Center Analysis. Transplant. Direct 2017, 3, e136. [Google Scholar] [CrossRef]
- Moreso, F.; Ibernon, M.; Goma, M.; Carrera, M.; Fulladosa, X.; Hueso, M.; Gil-Vernet, S.; Cruzado, J.M.; Torras, J.; Grinyo, J.M.; et al. Subclinical rejection associated with chronic allograft nephropathy in protocol biopsies as a risk factor for late graft loss. Am. J. Transplant. 2006, 6, 747–752. [Google Scholar] [CrossRef]
- Mehta, R.B.; Tandukar, S.; Jorgensen, D.; Randhawa, P.; Sood, P.; Puttarajappa, C.; Zeevi, A.; Tevar, A.D.; Hariharan, S. Early subclinical tubulitis and interstitial inflammation in kidney transplantation have adverse clinical implications. Kidney Int. 2020, 98, 436–447. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. S3), S1–S155. [Google Scholar] [CrossRef]
- Senev, A.; Coemans, M.; Lerut, E.; Van Sandt, V.; Kerkhofs, J.; Daniëls, L.; Driessche, M.V.; Compernolle, V.; Sprangers, B.; Van Loon, E.; et al. Eplet Mismatch Load and De Novo Occurrence of Donor-Specific Anti-HLA Antibodies, Rejection, and Graft Failure after Kidney Transplantation: An Observational Cohort Study. J. Am. Soc. Nephrol. 2020, 31, 2193–2204. [Google Scholar] [CrossRef]
- Wiebe, C.; Nickerson, P. Strategic Use of Epitope Matching to Improve Outcomes. Transplantation 2016, 100, 2048–2052. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n = 105) | NI (n = 51) | SCI (n = 54) | p Value | |
|---|---|---|---|---|
| Donor age (yr) | 53.7 ± 12.6 | 52.4 ± 13.3 | 55.0 ± 11.8 | 0.311 |
| ECD (%) | 42.7 | 36.0 | 49.1 | 0.181 |
| Recipient age (yr) | 53.4 ± 12.4 | 53.5 ± 12.0 | 53.4 ± 12.9 | 0.980 |
| Recipient BMI (kg/m2) | 27.0 ± 4.4 | 28.0 ± 4.4 | 26.1 ± 4.3 | 0.030 * |
| Male (%) | 73.3 | 72.5 | 74.1 | 0.860 |
| Living donor (%) | 14.6 | 16.0 | 13.2 | 0.688 |
| Prior CVD (%) | 19.4 | 18.0 | 20.8 | 0.724 |
| Hemodialysis (%) | 68.3 | 72.0 | 64.8 | 0.686 |
| Cause of ESRD (%) | ||||
| Glomerulonephritis | 21.0 | 17.6 | 24.1 | 0.357 |
| Diabetes | 16.2 | 23.5 | 9.3 | |
| APKD | 22.9 | 23.5 | 22.2 | |
| Interstitial nephropathy | 6.7 | 3.9 | 9.3 | |
| Nephrosclerosis | 9.5 | 11.8 | 7.4 | |
| Unknown | 12.4 | 9.8 | 14.8 | |
| Other | 11.4 | 9.8 | 13.0 | |
| Induction therapy (%) | ||||
| Basiliximab | 59 | 51 | 66.7 | 0.112 |
| Thymoglobulin | 41 | 49 | 33.3 | |
| Transfusion prior KT | 15.1 | 18.6 | 12.0 | 0.375 |
| DGF (%) | 25.5 | 24.0 | 26.9 | 0.735 |
| Tacrolimus levels (ng/mL) | 9.4 ± 2.5 | 9.7 ± 2.9 | 9.2 ± 2.1 | 0.286 |
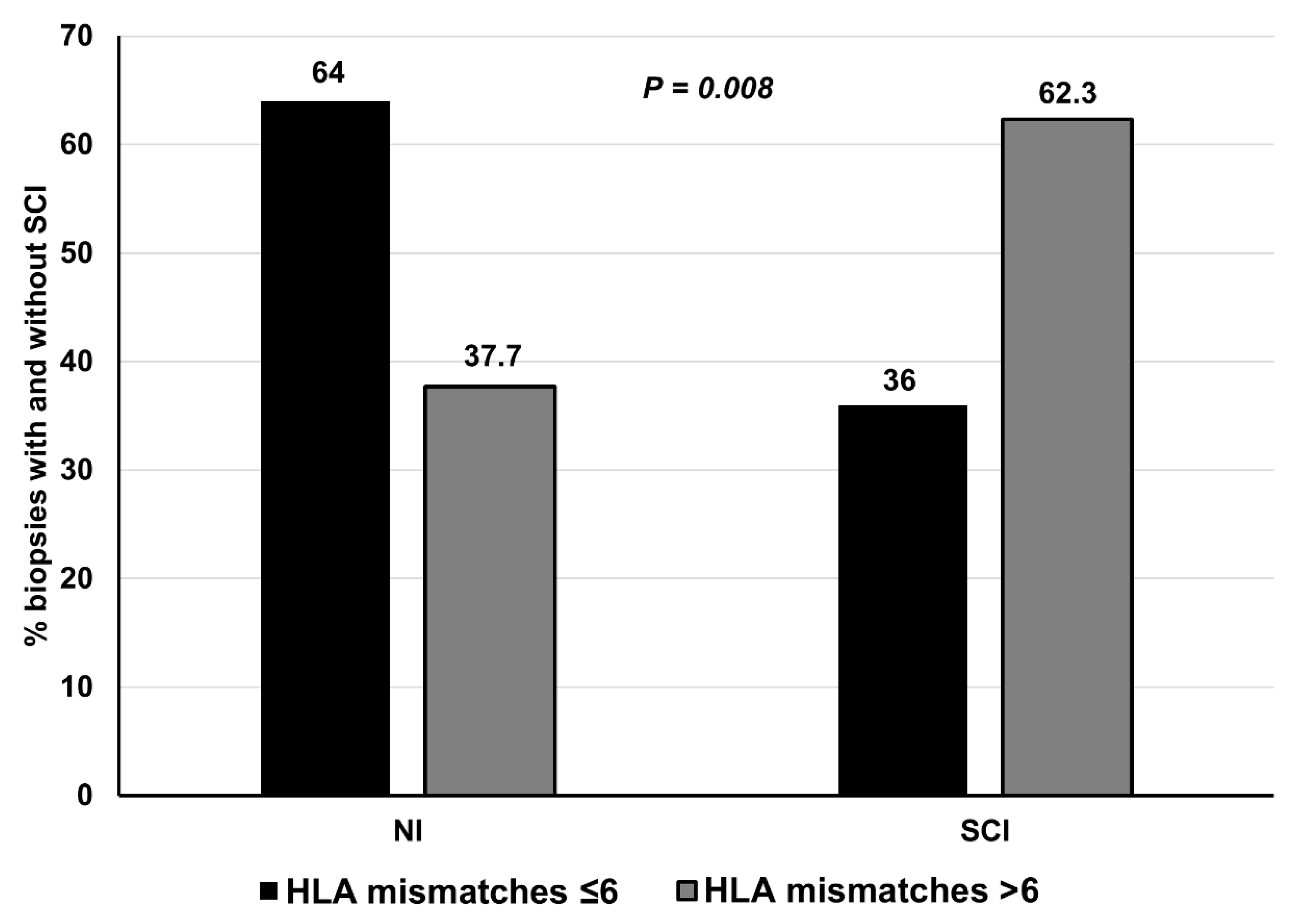
| Total HLA mismatches †, median (IQR) | 6 (5–8) | 5.5 (4–7) | 7 (6–8.5) | 0.008 * |
| Class I HLA mismatches #, median (IQR) | 4 (3–5) | 4 (3–5) | 4 (3–5) | 0.200 |
| Class II HLA mismatches ^, median (IQR) | 2 (1–3) | 2 (1–2) | 2 (2–3.5) | 0.004 * |
| Proteinuria (mg/dL) | 286.2 ± 224.9 | 297 ± 229 | 279 ± 225 | 0.763 |
| Creatinine (mg/dL) | 1.5 ± 0.4 | 1.4 ± 0.5 | 1.6 ± 0.4 | 0.018 * |
| MDRD-4 (mL/min) | 54.1 ± 19.7 | 60.0 ± 23.4 | 48.5 ± 13.6 | 0.003 * |
| OR | 95% CI | p Value | |
|---|---|---|---|
| Model 1 | |||
| Recipient age | 1.00 | 0.96–1.04 | 0.924 |
| DGF | 1.53 | 0.55–4.26 | 0.414 |
| Transfusion prior KT | 0.68 | 0.21–2.26 | 0.530 |
| Tacrolimus levels | 0.89 | 0.75–1.07 | 0.212 |
| Total HLA mismatches † | 1.32 | 1.06–1.64 | 0.013 * |
| Model 2 | |||
| Recipient age | 1.00 | 0.97–1.04 | 0.964 |
| DGF | 1.53 | 0.56–4.21 | 0.409 |
| Transfusion prior KT | 0.73 | 0.22–2.47 | 0.614 |
| Tacrolimus levels | 0.89 | 0.75–1.06 | 0.192 |
| Class II HLA mismatches ^ | 1.51 | 1.04–2.19 | 0.032 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández, D.; Vázquez, T.; Alonso-Titos, J.; León, M.; Caballero, A.; Cobo, M.A.; Sola, E.; López, V.; Ruiz-Esteban, P.; Cruzado, J.M.; et al. Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 1934. https://doi.org/10.3390/jcm10091934
Hernández D, Vázquez T, Alonso-Titos J, León M, Caballero A, Cobo MA, Sola E, López V, Ruiz-Esteban P, Cruzado JM, et al. Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients. Journal of Clinical Medicine. 2021; 10(9):1934. https://doi.org/10.3390/jcm10091934
Chicago/Turabian StyleHernández, Domingo, Teresa Vázquez, Juana Alonso-Titos, Myriam León, Abelardo Caballero, María Angeles Cobo, Eugenia Sola, Verónica López, Pedro Ruiz-Esteban, Josep María Cruzado, and et al. 2021. "Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients" Journal of Clinical Medicine 10, no. 9: 1934. https://doi.org/10.3390/jcm10091934
APA StyleHernández, D., Vázquez, T., Alonso-Titos, J., León, M., Caballero, A., Cobo, M. A., Sola, E., López, V., Ruiz-Esteban, P., Cruzado, J. M., Sellarés, J., Moreso, F., Manonelles, A., Torio, A., Cabello, M., Delgado-Burgos, J., Casas, C., Gutiérrez, E., Jironda, C., ... Torres, A. (2021). Impact of HLA Mismatching on Early Subclinical Inflammation in Low-Immunological-Risk Kidney Transplant Recipients. Journal of Clinical Medicine, 10(9), 1934. https://doi.org/10.3390/jcm10091934