
Artificial Neural Network for Predicting the Safe Temporary Artery Occlusion Time in Intracranial Aneurysmal Surgery

Abstract
1. Introduction
2. Methods
2.1. Retrospective Cohort, Training, and Testing Set of the Model
2.2. Prospective Cohort and Validation Set of the Model
2.3. Surgical Techniques
2.4. Feature Selection for ANN Model
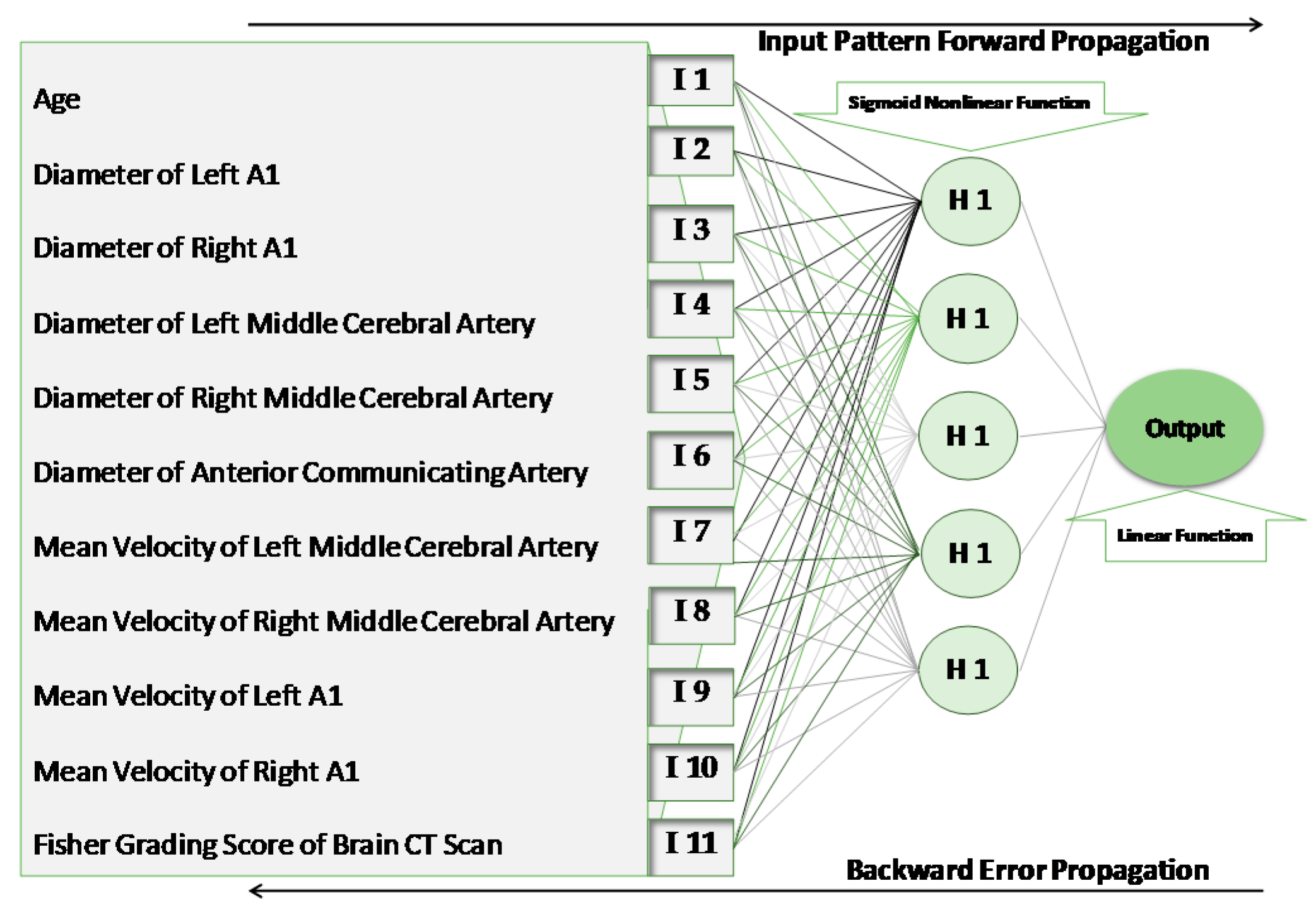
2.5. Structure of the ANN Model
2.6. Training and Validating of the ANN Model
2.7. Importance of Each Clinical Feature in Predicting the SCT
2.8. Estimating the Errors
3. Results
4. Discussion
4.1. Selected Features as Input of the Model
4.2. Limitations and Error Estimation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zhao, J.; Lin, H.; Summers, R.; Yang, M.; Cousins, B.G.; Tsui, J. Current Treatment Strategies for Intracranial Aneurysms: An Overview. Angiology 2018, 69, 17–30. [Google Scholar] [CrossRef]
- Schramm, J.; Cornelia Cedzich, C. Outcome and management of intraoperative aneurysm rupture. Surg. Neurol. 1993, 40, 26–30. [Google Scholar] [CrossRef]
- Taylor, C.L.; Selman, W.R. Temporary vascular occlusion during cerebral aneurysm surgery. Neurosurg. Clin. N. Am. 1998, 9, 673–679. [Google Scholar] [CrossRef]
- Kameda, M.; Hishikawa, T.; Hiramatsu, M.; Yasuhara, T.; Kurozumi, K.; Date, I. Precise MEP monitoring with a reduced interval is safe and useful for detecting permissive duration for temporary clipping. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Staarmann, B.; O’Neal, K.; Magner, M.; Zuccarello, M. Sensitivity and Specificity of Intraoperative Neuromonitoring for Identifying Safety and Duration of Temporary Aneurysm Clipping Based on Vascular Territory, a Multimodal Strategy. World Neurosurg. 2017, 100, 522–530. [Google Scholar] [CrossRef]
- Dumont, T.M.; Rughani, A.I.; Tranmer, B.I. Prediction of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage with an artificial neural network: Feasibility and comparison with logistic regression models. World Neurosurg. 2011, 75, 57–63. [Google Scholar] [CrossRef]
- Hsu, M.-H.; Li, Y.-C.; Chiu, W.-T.; Yen, J.-C. Outcome prediction after moderate and severe head injury using an artificial neural network. Stud. Health Technol. Inform. 2005, 116, 241–246. [Google Scholar] [PubMed]
- Rughani, A.I.; Dumont, T.M.; Lu, Z.; Bongard, J.; Horgan, M.A.; Penar, P.L.; Tranmer, B.I. Use of an artificial neural network to predict head injury outcome. J. Neurosurg. 2010, 113, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Azimi, P.; Mohammadi, H.R.; Benzel, E.C.; Shahzadi, S.; Azhari, S. Use of artificial neural networks to predict recurrent lumbar disk herniation. Clin. Spine Surg. 2015, 28, E161–E165. [Google Scholar] [CrossRef]
- Azimi, P.; Mohammadi, H.R. Predicting endoscopic third ventriculostomy success in childhood hydrocephalus: An artificial neural network analysis. J. Neurosurg. Pediatr. 2014, 13, 426–432. [Google Scholar] [CrossRef]
- Tanioka, S.; Ishida, F.; Yamamoto, A.; Shimizu, S.; Sakaida, H.; Toyoda, M.; Kashiwagi, N.; Suzuki, H. Machine Learning Classification of Cerebral Aneurysm Rupture Status with Morphologic Variables and Hemodynamic Parameters. Radiol. Artif. Intell. 2020, 2, e190077. [Google Scholar] [CrossRef]
- Detmer, F.J.; Lückehe, D.; Mut, F.; Slawski, M.; Hirsch, S.; Bijlenga, P.; von Voigt, G.; Cebral, J.R. Comparison of statistical learning approaches for cerebral aneurysm rupture assessment. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Huang, L.; Qian, Y.; Xia, S.; Chong, W.; Liu, J.; Di Ieva, A.; Hou, X.; Ou, C. Deep learning for automated cerebral aneurysm detection on computed tomography images. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 715–723. [Google Scholar] [CrossRef]
- Dorronsoro, J.R.; López, V.; Cruz, C.S.; Siguenza, J.A. Autoassociative neural networks and noise filtering. IEEE Trans. Signal Process. 2003, 51, 1431–1438. [Google Scholar] [CrossRef]
- Long, Q.; Luppi, L.; König, C.S.; Rinaldo, V.; Das, S.K. Study of the collateral capacity of the circle of Willis of patients with severe carotid artery stenosis by 3D computational modeling. J. Biomech. 2008, 41, 2735–2742. [Google Scholar] [CrossRef] [PubMed]
- Sacca, A.; Pedrini, L.; Vitacchiano, G.; Pisano, E.; Zagni, P.; Bellanova, B.; Dondi, M.; Monetti, N. Cerebral SPECT with 99mTc-HMPAO in extracranial carotid pathology: Evaluation of changes in the ischemic area after carotid endarterectomy. Int. Angiol. J. Int. Union Angiol. 1992, 11, 117–121. [Google Scholar]
- Vanninen, R.; Koivisto, K.; Tulla, H.; Manninen, H.; Partanen, K. Hemodynamic effects of carotid endarterectomy by magnetic resonance flow quantification. Stroke 1995, 26, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, F.; Pasqualetti, P.; Matteis, M.; Passarelli, F.; Troisi, E.; Rossini, P.M.; Caltagirone, C.; Silvestrini, M. Effect of collateral blood flow and cerebral vasomotor reactivity on the outcome of carotid artery occlusion. Stroke 2001, 32, 1552–1558. [Google Scholar] [CrossRef]
- Faber, J.E.; Zhang, H.; Lassance-Soares, R.M.; Prabhakar, P.; Najafi, A.H.; Burnett, M.S.; Epstein, S.E. Aging causes collateral rarefaction and increased severity of ischemic injury in multiple tissues. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1748–1756. [Google Scholar] [CrossRef]
- Liebeskind, D.S. Collateral circulation. Stroke 2003, 34, 2279–2284. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Peng, X.; Lassance-Soares, R.M.; Najafi, A.H.; Alderman, L.O.; Sood, S.; Xue, Z.; Chan, R.; Faber, J.E.; Epstein, S.E. Aging-induced collateral dysfunction: Impaired responsiveness of collaterals and susceptibility to apoptosis via dysfunctional eNOS signaling. J. Cardiovasc. Transl. Res. 2011, 4, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Yang, Y.; Cao, T.; Li, Z. Differences in left and right carotid intima–media thickness and the associated risk factors. Clin. Radiol. 2011, 66, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Manbachi, A.; Hoi, Y.; Wasserman, B.A.; Lakatta, E.G.; Steinman, D.A. On the shape of the common carotid artery with implications for blood velocity profiles. Physiol. Meas. 2011, 32, 1885. [Google Scholar] [CrossRef] [PubMed]
- Alnæs, M.S.; Isaksen, J.; Mardal, K.-A.; Romner, B.; Morgan, M.K.; Ingebrigtsen, T. Computation of hemodynamics in the circle of Willis. Stroke 2007, 38, 2500–2505. [Google Scholar] [CrossRef] [PubMed]
- Kulcsár, Z.; Ugron, A.; Marosfői, M.; Berentei, Z.; Paal, G.; Szikora, I. Hemodynamics of cerebral aneurysm initiation: The role of wall shear stress and spatial wall shear stress gradient. Am. J. Neuroradiol. 2011, 32, 587–594. [Google Scholar] [CrossRef]
- Metaxa, E.; Tremmel, M.; Natarajan, S.K.; Xiang, J.; Paluch, R.A.; Mandelbaum, M.; Siddiqui, A.H.; Kolega, J.; Mocco, J.; Meng, H. Characterization of critical hemodynamics contributing to aneurysmal remodeling at the basilar terminus in a rabbit model. Stroke 2010, 41, 1774–1782. [Google Scholar] [CrossRef]
- Valencia, A.; Morales, H.; Rivera, R.; Bravo, E.; Galvez, M. Blood flow dynamics in patient-specific cerebral aneurysm models: The relationship between wall shear stress and aneurysm area index. Med. Eng. Phys. 2008, 30, 329–340. [Google Scholar] [CrossRef]
- Farnoush, A.; Qian, Y.; Avolio, A. Effect of inflow on computational fluid dynamic simulation of cerebral bifurcation aneurysms. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 1025–1028. [Google Scholar]
- Hassan, T.; Hassan, A.A.; Ahmed, Y.M. Influence of parent vessel dominancy on fluid dynamics of anterior communicating artery aneurysms. Acta Neurochir. 2011, 153, 305–310. [Google Scholar] [CrossRef]
- Jou, L.-D.; Lee, D.H.; Mawad, M.E. Cross-flow at the anterior communicating artery and its implication in cerebral aneurysm formation. J. Biomech. 2010, 43, 2189–2195. [Google Scholar] [CrossRef]
- Silva, P.A.; Cerejo, A.; Vilarinho, A.; Dias, C.; Vaz, R. Regional variations in brain oxygenation during temporary clipping in aneurysm surgery. Neurol. Res. 2012, 34, 971–976. [Google Scholar] [CrossRef]
- Nixon, A.M.; Gunel, M.; Sumpio, B.E. The critical role of hemodynamics in the development of cerebral vascular disease: A review. J. Neurosurg. 2010, 112, 1240–1253. [Google Scholar] [CrossRef] [PubMed]
- Alfano, J.M.; Kolega, J.; Natarajan, S.K.; Xiang, J.; Paluch, R.A.; Levy, E.I.; Siddiqui, A.H.; Meng, H. Intracranial aneurysms occur more frequently at bifurcation sites that typically experience higher hemodynamic stresses. Neurosurgery 2013, 73, 497–505. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Retrospective Dataset (n = 105) | Prospective Dataset (n = 20) |
|---|---|---|
| Age; Mean (Range); Years | 48.7 (30–72) | 50.2 (30–76) |
| Men; n (%) | 32 (30.4%) | 9 (45%) |
| Location of Aneurysm | ||
| Middle Cerebral Artery; n (%) | 80 (76.1%) | 14 (70%) |
| Anterior Communicating Artery; n (%) | 25 (23.9%) | 6 (30%) |
| Fisher Grading Scale of CT Scan Images | ||
| One; n (%) | 28 (26.66%) | 1 (5%) |
| Two; n (%) | 46 (43.8%) | 9 (45%) |
| Three; n (%) | 23 (21.9%) | 4 (20%) |
| Four; n (%) | 8 (7.61%) | 6 (30%) |
| Site of Obstruction | Safe Time Interval (Seconds) |
|---|---|
| Overall | 90–960 |
| Right Middle Cerebral Artery | 240–960 |
| Left Middle Cerebral Artery | 90–950 |
| Anterior Communicating Artery | 120–932 |
| Rank | Input Value | Sensitivity (%) |
|---|---|---|
| 1 | Mean velocity of flow at left MCA (middle cerebral arteries) | 73.82 ± 1.95 |
| 2 | Mean velocity of flow at left ACA (anterior cerebral arteries) | 67.23 ± 2.74 |
| 3 | Fisher grading scale of brain CT scan | 65.71 ± 5.31 |
| 4 | Mean velocity of flow at right ACA | 63.87 ± 4.82 |
| 5 | Diameter of right MCA | 59.22 ± 5.24 |
| 6 | Diameter of AcomA (anterior communicating artery) | 57.56 ± 3.13 |
| 7 | Diameter of left MCA | 55.59 ± 3.13 |
| 8 | Diameter of left A1 | 45.74 ± 2.47 |
| 9 | Age | 41.35 ± 1.78 |
| 10 | Mean velocity of flow at right MCA | 32.19 ± 3.62 |
| 11 | Diameter of right A1 | 23.45 ± 2.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahjouei, S.; Ghodsi, S.M.; Zangeneh Soroush, M.; Ansari, S.; Kamali-Ardakani, S. Artificial Neural Network for Predicting the Safe Temporary Artery Occlusion Time in Intracranial Aneurysmal Surgery. J. Clin. Med. 2021, 10, 1464. https://doi.org/10.3390/jcm10071464
Shahjouei S, Ghodsi SM, Zangeneh Soroush M, Ansari S, Kamali-Ardakani S. Artificial Neural Network for Predicting the Safe Temporary Artery Occlusion Time in Intracranial Aneurysmal Surgery. Journal of Clinical Medicine. 2021; 10(7):1464. https://doi.org/10.3390/jcm10071464
Chicago/Turabian StyleShahjouei, Shima, Seyed Mohammad Ghodsi, Morteza Zangeneh Soroush, Saeed Ansari, and Shahab Kamali-Ardakani. 2021. "Artificial Neural Network for Predicting the Safe Temporary Artery Occlusion Time in Intracranial Aneurysmal Surgery" Journal of Clinical Medicine 10, no. 7: 1464. https://doi.org/10.3390/jcm10071464
APA StyleShahjouei, S., Ghodsi, S. M., Zangeneh Soroush, M., Ansari, S., & Kamali-Ardakani, S. (2021). Artificial Neural Network for Predicting the Safe Temporary Artery Occlusion Time in Intracranial Aneurysmal Surgery. Journal of Clinical Medicine, 10(7), 1464. https://doi.org/10.3390/jcm10071464