

Markers of Kidney Injury: Proenkephalin A and Uromodulin, but Not Dickkopf-3, Are Elevated in Patients After Hematopoietic Stem Cell Transplantation
 , , ,
, , , 
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, E.D.; Lochte, H.L., Jr.; Lu, W.C.; Ferrebee, J.W. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957, 257, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Appelbaum, F.R. Hematopoietic-cell transplantation at 50. N. Engl. J. Med. 2007, 357, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Haematopoietic Stem Cell Transplantation HSCtx; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Bazinet, A.; Popradi, G. A general practitioner’s guide to hematopoietic stem-cell transplantation. Curr. Oncol. 2019, 26, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.D.; Buckner, C.D.; Banaji, M.; Clift, R.A.; Fefer, A.; Flournoy, N.; Goodell, B.W.; Hickman, R.O.; Lerner, K.G.; Neiman, P.E.; et al. One hundred patients with acute leukemia treated by chemotherapy, total body irradiation, and allogeneic marrow transplantation. Blood 1977, 49, 511–533. [Google Scholar] [CrossRef]
- Gertz, M.A. Current status of stem cell mobilization. Br. J. Haematol. 2010, 150, 647–662. [Google Scholar] [CrossRef]
- Stem Cell Trialists’ Collaborative Group. Allogeneic peripheral blood stem-cell compared with bone marrow transplantation in the management of hematologic malignancies: An individual patient data meta-analysis of nine randomized trials. J. Clin. Oncol. 2005, 23, 5074–5087. [Google Scholar] [CrossRef]
- Renaghan, A.D.; Jaimes, E.A.; Malyszko, J.; Perazella, M.A.; Sprangers, B.; Rosner, M.H. Acute Kidney Injury and CKD Associated with Hematopoietic Stem Cell Transplantation. Clin. J. Am. Soc. Nephrol. 2020, 15, 289–297. [Google Scholar] [CrossRef]
- Kępska-Dzilińska, M.; Zhymaila, A.; Malyszko, J. Kidney damage in patients after allogeneic stem cell transplantation. Wiad Lek 2022, 75 Pt 1, 877–880. [Google Scholar] [CrossRef]
- Saddadi, F.; Hakemi, M.; Najafi, I.; Moghadam, K.; Ghavamzadeh, A.; Jahani, M.; Ganji, M.; Amini, M.; Soleimanian, T. Chronic kidney disease after hematopoietic cell transplantation: Frequency, risk factors, and outcomes. Transpl. Proc. 2009, 41, 2895–2897. [Google Scholar] [CrossRef]
- Bennett, M.; Dent, C.L.; Ma, Q.; Dastrala, S.; Grenier, F.; Workman, R.; Syed, H.; Ali, S.; Barasch, J.; Devarajan, P. Urine NGAL predicts severity of acute kidney injury after cardiac surgery: A prospective study. Clin. J. Am. Soc. Nephrol. 2008, 3, 665–673. [Google Scholar] [CrossRef]
- Wen, Y.; Parikh, C.R. Current concepts and advances in biomarkers of acute kidney injury. Crit. Rev. Clin. Lab. Sci. 2021, 58, 354–368. [Google Scholar] [CrossRef] [PubMed]
- Schrezenmeier, E.V.; Barasch, J.; Budde, K.; Westhoff, T.; Schmidt-Ott, K.M. Biomarkers in acute kidney injury—Pathophysiological basis and clinical performance. Acta Physiol. 2017, 219, 554–572. [Google Scholar] [CrossRef] [PubMed]
- Endre, Z.H. Assessing renal recovery after acute kidney injury: Can biomarkers help? Nephron 2018, 140, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Denning, G.M.; Ackermann, L.W.; Barna, T.J.; Armstrong, J.G.; Stoll, L.L.; Weintraub, N.L.; Dickson, E.W. Proenkephalin expression and enkephalin release are widely observed in non-neuronal tissues. Peptides 2008, 29, 83–92. [Google Scholar] [CrossRef]
- Shah, K.S.; Taub, P.; Patel, M.; Rehfeldt, M.; Struck, J.; Clopton, P.; Mehta, R.L.; Maisel, A.S. Proenkephalin predicts acute kidney injury in cardiac surgery patients. Clin. Nephrol. 2015, 83, 29–35. [Google Scholar] [CrossRef]
- Marino, R.; Struck, J.; Hartmann, O.; Maisel, A.S.; Rehfeldt, M.; Magrini, L.; Melander, O.; Bergmann, A.; Di Somma, S. Diagnostic and short-term prognostic utility of plasma pro-enkephalin (pro-ENK) for acute kidney injury in patients admitted with sepsis in the emergency department. J. Nephrol. 2015, 28, 717–724. [Google Scholar] [CrossRef]
- Schulz, C.-A.; Christensson, A.; Ericson, U.; Almgren, P.; Hindy, G.; Nilsson, P.M.; Struck, J.; Bergmann, A.; Melander, O.; Orho-Melander, M. High level of fasting plasma proenkephalin-A predicts deterioration of kidney function and incidence of CKD. J. Am. Soc. Nephrol. 2017, 28, 291–303. [Google Scholar] [CrossRef]
- Zewinger, S.; Rauen, T.; Rudnicki, M.; Federico, G.; Wagner, M.; Triem, S.; Schunk, S.J.; Petrakis, I.; Schmit, D.; Wagenpfeil, S.; et al. Dickkopf-3 (DKK3) in Urine Identifies Patients with Short-Term Risk of eGFR Loss. J. Am. Soc. Nephrol. 2018, 29, 2722–2733. [Google Scholar] [CrossRef]
- Schunk, S.J.; Speer, T.; Petrakis, I.; Fliser, D. Dickkopf 3-a novel biomarker of the ‘kidney injury continuum’. Nephrol. Dial. Transpl. 2021, 36, 761–767. [Google Scholar] [CrossRef]
- Schunk, S.J.; Floege, J.; Fliser, D.; Speer, T. WNT–β-catenin signaling—A versatile player in kidney injury and repair. Nature 2021, 17, 172–184. [Google Scholar] [CrossRef]
- Dawnay, A.B.; Cattell, W.R. Serum Tamm-Horsfall Glycoprotein Levels in Health and in Renal Disease. Clin. Nephrol. 1981, 15, 5–8. [Google Scholar] [PubMed]
- Usui, R.; Ogawa, T.; Takahashi, H.; Iwasaki, C.; Koike, M.; Morito, T.; Hatano, M.; Nitta, K. Serum Uromodulin Is a Novel Renal Function Marker in the Japanese Population. Clin. Exp. Nephrol. 2021, 25, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Steubl, D.; Block, M.; Herbst, V.; Nockher, W.A.; Schlumberger, W.; Satanovskij, R.; Angermann, S.; Hasenau, A.-L.; Stecher, L.; Heemann, U.; et al. Plasma Uromodulin Correlates with Kidney Function and Identifies Early Stages in Chronic Kidney Disease Patients. Medicine 2016, 95, e3011. [Google Scholar] [CrossRef] [PubMed]
- Smirnov, A.V.; Khasun, M.; Kayukov, I.G.; Galkina, O.V.; Sipovski, V.G.; Parastaeva, M.M.; Bogdanova, E.O. Serum Uromodulin as an Early Biomarker of Tubular Atrophy and Interstitial Fibrosis in Patients with Glomerulopathies. Ter. Arkhiv 2018, 90, 41–47. [Google Scholar] [CrossRef]
- Forni, L.G.; Darmon, M.; Ostermann, M.; Oudemans-van Straaten, H.M.; Pettilä, V.; Prowle, J.R.; Schetz, M.; Joannidis, M. Renal recovery after acute kidney injury. Intensive Care Med. 2017, 43, 855–866. [Google Scholar] [CrossRef]
- Kellum, J.A.; Sileanu, F.E.; Bihorac, A.; Hoste, E.A.; Chawla, L.S. Recovery after acute kidney injury. Am. J. Respir. Crit. Care Med. 2017, 195, 784–791. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Hansrivijit, P.; Kovvuru, K.; Kanduri, S.R.; Torres-Ortiz, A.; Acharya, P.; Gonzalez-Suarez, M.L.; Kaewput, W.; Bathini, T.; Cheungpasitporn, W. Diagnostics, risk factors, treatment and outcomes of acute kidney injury in a new paradigm. J. Clin. Med. 2020, 9, 1104. [Google Scholar] [CrossRef]
- Coca, S.G.; King, J.T., Jr.; Rosenthal, R.A.; Perkal, M.F.; Parikh, C.R. The duration of postoperative acute kidney injury is an additional parameter predicting long-term survival in diabetic veterans. Kidney Int. 2010, 78, 926–933. [Google Scholar] [CrossRef]
- Cerdá, J.; Liu, K.D.; Cruz, D.N.; Jaber, B.L.; Koyner, J.L.; Heung, M.; Okusa, M.D.; Faubel, S. Promoting kidney function recovery in patients with AKI requiring RRT. Clin. J. Am. Soc. Nephrol. 2015, 10, 1859–1867. [Google Scholar] [CrossRef]
- Kanduri, S.R.; Cheungpasitporn, W.; Thongprayoon, C.; Bathini, T.; Kovvuru, K.; Garla, V.; Medaura, J.; Vaitla, P.; Kashani, K.B. Incidence and mortality of acute kidney injury in patients undergoing hematopoietic stem cell transplantation: A systematic review and meta-analysis. QJM Int. J. Med. 2020, 113, 621–632. [Google Scholar] [CrossRef]
- Hingorani, S. Renal complications of hematopoietic-cell transplantation. N. Engl. J. Med. 2016, 374, 2256–2267. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.; Gorab, D.L.; Fernandes, C.R.; Macedo, E. Role of proenkephalin in the diagnosis of severe and subclinical acute kidney injury during the perioperative period of liver transplantation. Pract. Lab Med. 2022, 31, e00278. [Google Scholar] [CrossRef] [PubMed]
- Beunders, R.; van Groenendael, R.; Leijte, G.P.; Kox, M.; Pickkers, P. Proenkephalin Compared to Conventional Methods to Assess Kidney Function in Critically Ill Sepsis Patients. Shock 2020, 54, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Kieneker, L.M.; Hartmann, O.; Struck, J.; Bergmann, A.; Gansevoort, R.T.; Joosten, M.M.; van den Berg, E.; de Boer, R.A.; Bakker, S.J. Plasma Proenkephalin and Poor Long-Term Outcome in Renal Transplant Recipients. Transpl. Direct 2017, 3, e190. [Google Scholar] [CrossRef]
- Beunders, R.; Donato, L.J.; van Groenendael, R.; Arlt, B.; Carvalho-Wodarz, C.; Schulte, J.; Coolen, A.C.; Lieske, J.C.; Meeusen, J.W.; Jaffe, A.S.; et al. Assessing GFR with Proenkephalin. Kidney Int. Rep. 2023, 8, 2345–2355. [Google Scholar] [CrossRef]
- Nilsson, C.; Christensson, A.; Nilsson, P.M.; Melander, O.; Bennet, L. Pro-Enkephalin and its association with renal function in Middle Eastern immigrants and native Swedes. Scand. J. Clin. Lab. Investig. 2021, 81, 573–578. [Google Scholar] [CrossRef]
- Khorashadi, M.; Beunders, R.; Pickkers, P.; Legrand, M. Proenkephalin: A New Biomarker for Glomerular Filtration Rate and Acute Kidney Injury. Nephron 2020, 144, 655–661. [Google Scholar] [CrossRef]
- Smeets, N.J.L.; Hartmann, O.; Schulte, J.; Schreuder, M.F.; de Wildt, S.N. Proenkephalin A as a marker for glomerular filtration rate in critically ill children: Validation against gold standard iohexol GFR measurements. Clin. Chem. Lab. Med. 2022, 61, 104–111. [Google Scholar] [CrossRef]
- Caironi, P.; Latini, R.; Struck, J.; Hartmann, O.; Bergmann, A.; Bellato, V.; Ferraris, S.; Tognoni, G.; Pesenti, A.; Gattinoni, L.; et al. Circulating Proenkephalin, Acute Kidney Injury, and Its Improvement in Patients with Severe Sepsis or Shock. Clin. Chem. 2018, 64, 1361–1369. [Google Scholar] [CrossRef]
- Donato, L.J.; Meeusen, J.W.; Lieske, J.C.; Bergmann, D.; Sparwaßer, A.; Jaffe, A.S. Analytical performance of an immunoassay to measure proenkephalin. Clin. Biochem. 2018, 58, 72–77. [Google Scholar] [CrossRef]
- Tichy, J.; Hausmann, A.; Lanzerstorfer, J.; Ryz, S.; Wagner, L.; Lassnigg, A.; Bernardi, M.H. Prediction of Successful Liberation from Continuous Renal Replacement Therapy Using a Novel Biomarker in Patients with Acute Kidney Injury after Cardiac Surgery-An Observational Trial. Int. J. Mol. Sci. 2024, 25, 10873. [Google Scholar] [CrossRef] [PubMed]
- Von Groote, T.; Albert, F.; Meersch, M.; Koch, R.; Gerss, J.; Arlt, B.; Sadjadi, M.; Porschen, C.; Pickkers, P.; Zarbock, A.; et al. Evaluation of Proenkephalin A 119–159 for liberation from renal replacement therapy: An external, multicenter pilot study in critically ill patients with acute kidney injury. Crit. Care 2023, 27, 276. [Google Scholar] [CrossRef] [PubMed]
- Dépret, F.; Hollinger, A.; Cariou, A.; Deye, N.; Vieillard-Baron, A.; Fournier, M.C.; Jaber, S.; Damoisel, C.; Lu, Q.; Monnet, X.; et al. Incidence and Outcome of Subclinical Acute Kidney Injury Using penKid in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2020, 202, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Bullen, A.L.; Katz, R.; Poursadrolah, S.; Short, S.A.P.; Long, D.L.; Cheung, K.L.; Sharma, S.; Al-Rousan, T.; Fregoso, A.; Schulte, J.; et al. Plasma proenkephalin A and incident chronic kidney disease and albuminuria in the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort. BMC Nephrol. 2024, 25, 16. [Google Scholar] [CrossRef]
- Walczak-Wieteska, P.; Zuzda, K.; Małyszko, J.; Andruszkiewicz, P. Proenkephalin A 119–159 in Perioperative and Intensive Care-A Promising Biomarker or Merely Another Option? Diagnostics 2024, 14, 2364. [Google Scholar] [CrossRef]
- Grycuk, W.; Jakubowska, Z.; Malyszko, J. Proenkephalin (PENK): A functional biomarker in chronic kidney diseases—Hope or just a new bystander? J. Nephrol. 2025. accepted. [Google Scholar]
- Shi, K.; Jiang, W.; Song, L.; Li, X.; Zhang, C.; Li, L.; Feng, Y.; Yang, J.; Wang, T.; Wang, H.; et al. Persistent acute kidney injury biomarkers: A systematic review and meta-analysis. Clin. Chim. Acta 2025, 564, 119907. [Google Scholar] [CrossRef]
- Canki, E.; Kho, E.; Hoenderop, J.G.J. Urinary biomarkers in kidney disease. Clin. Chim. Acta 2024, 555, 117798. [Google Scholar] [CrossRef]
- Dziamałek-Macioszczyk, P.; Winiarska, A.; Pawłowska, A.; Wojtacha, P.; Stompór, T. Patterns of Dickkopf-3 Serum and Urine Levels at Different Stages of Chronic Kidney Disease. J. Clin. Med. 2023, 12, 4705. [Google Scholar] [CrossRef]
- Sun, Y.; Xiao, Z.; Yang, S.; Hao, C.; Zhao, H.; An, Y. Advances and insights for DKK3 in non-cancerous diseases: A systematic review. PeerJ 2025, 13, e18935. [Google Scholar] [CrossRef]
- Schunk, S.J.; Zarbock, A.; Meersch, M.; Küllmar, M.; Kellum, J.A.; Schmit, D.; Wagner, M.; Triem, S.; Wagenpfeil, S.; Gröne, H.J.; et al. Association between urinary dickkopf-3, acute kidney injury, and subsequent loss of kidney function in patients undergoing cardiac surgery: An observational cohort study. Lancet 2019, 394, 488–496. [Google Scholar] [CrossRef]
- González, J.; Jatem, E.; Roig, J.; Valtierra, N.; Ostos, E.; Abó, A.; Santacana, M.; García, A.; Segarra, A. Usefulness of urinary biomarkers to estimate the interstitial fibrosis surface in diabetic nephropathy with normal kidney function. Nephrol. Dial Transpl. 2022, 37, 2102–2110. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Watchorn, J.C.; Zarbock, A.; Forni, L.G. Prognostic Biomarkers and AKI: Potential to Enhance the Identification of Post-Operative Patients at Risk of Loss of Renal Function. Res. Rep. Urol. 2024, 16, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Jiang, Z.; Wu, Y.; Ou, S.; Qin, J.; Xue, L.; Wu, W. The role of urinary Dickkopf-3 in the prediction of acute kidney injury: A systematic review meta-analysis. Int. Urol. Nephrol. 2023, 55, 3175–3188. [Google Scholar] [CrossRef] [PubMed]
- Seibert, F.S.; Heringhaus, A.; Pagonas, N.; Rohn, B.; Bauer, F.; Trappe, H.J.; Landmesser, U.; Babel, N.; Westhoff, T.H. Dickkopf-3 in the prediction of contrast media induced acute kidney injury. J. Nephrol. 2021, 34, 821–828. [Google Scholar] [CrossRef]
- Roscigno, G.; Quintavalle, C.; Biondi-Zoccai, G.; De Micco, F.; Frati, G.; Affinito, A.; Nuzzo, S.; Condorelli, G.; Briguori, C. Urinary Dickkopf-3 and Contrast-Associated Kidney Damage. J. Am. Coll. Cardiol. 2021, 77, 2667–2676. [Google Scholar] [CrossRef]
- Enko, D.; Meinitzer, A.; Scherberich, J.E.; März, W.; Herrmann, M.; Artinger, K.; Rosenkranz, A.R.; Zitta, S. Individual Uromodulin Serum Concentration Is Independent of Glomerular Filtration Rate in Healthy Kidney Donors. Clin. Chem. Lab. Med. CCLM 2021, 59, 563–570. [Google Scholar] [CrossRef]
- Garimella, P.S.; Biggs, M.L.; Katz, R.; Ix, J.H.; Bennett, M.R.; Devarajan, P.; Kestenbaum, B.R.; Siscovick, D.S.; Jensen, M.K.; Shlipak, M.G.; et al. Urinary Uromodulin, Kidney Function, and Cardiovascular Disease in Elderly Adults. Kidney Int. 2015, 88, 1126–1134. [Google Scholar] [CrossRef]
- Steubl, D.; Block, M.; Herbst, V.; Nockher, W.A.; Schlumberger, W.; Kemmner, S.; Bachmann, Q.; Angermann, S.; Wen, M.; Heemann, U.; et al. Urinary Uromodulin Independently Predicts End-Stage Renal Disease and Rapid Kidney Function Decline in a Cohort of Chronic Kidney Disease Patients. Medicine 2019, 98, e15808. [Google Scholar] [CrossRef]
- Vonbrunn, E.; Ebert, N.; Cordasic, N.; Amann, K.; Büttner, A.; Büttner-Herold, M.; Scherberich, J.E.; Daniel, C. Serum Uromodulin as early marker for ischemic acute kidney injury and nephron loss: Association with kidney tissue distribution pattern. J. Transl. Med. 2025, 23, 323. [Google Scholar] [CrossRef]
- Kaszynska, A.; Kepska-Dzilinska, M.; Karakulska-Prystupiuk, E.; Tomaszewska, A.; Basak, G.; Zorawski, M.; Drozak, I.; Jakubowska, Z.; Malyszko, J. 226.9: Proenkephalin and DKK-3 levels and kidney function in patients after hematopoietic stem cell transplantation. Transplantation 2024, 108. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; Zeeuw, D.D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from kidney disease: Improving global outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | HSCT | |
|---|---|---|
| Age (years) | 49 ± 10 | 48 ± 14 |
| Time after transplantation (months) | NA | 103.3 ± 50.5 |
| Hemoglobin (g/dL) | 13.87 ± 0.89 | 12.87 ± 1.99 |
| Acute myeloid leukemia (%) | NA | 43 |
| serum creatinine (mg/dL) | 0.86 ± 0.35 | 1.1 ± 0.37 * |
| eGFR by CKD-EPI (mL/min/1.72 m2) | 96.9 ± 13.0 | 73.5 ± 23.5 ** |
| Erythrocyturia (%) | 0 | 11 |
| Leukocyturia (%) | 0 | 6.25 |
| HSCT with eGFR > 60 (mL/min/1.72 m2) | HSCT with eGFR < 60 (mL/min/1.72 m2) | |
|---|---|---|
| Age (years) | 46 ± 10 | 50 ± 17 |
| Time after transplantation (months) | 87 ± 43 | 119 ± 52 * |
| Hemoglobin (g/dL) | 13.01 ± 0.91 | 12.03 ± 1.01 * |
| Acute myeloid leukemia | 27 | 7 ** |
| Acute lymphocytic leukemia | 10 | 8 |
| Lymphoma | 4 | 4 |
| serum creatinine (mg/dL) | 0.95 ± 0.21 | 1.55 ± 0.30 ** |
| eGFR by CKD-EPI (ml/min/1.72 m2) | 85.28 ± 16.42 | 46.10 ± 7.80 ** |
| Erythrocyturia (%) | 0 | 11 |
| Leukocyturia (%) | 0 | 6.25 |
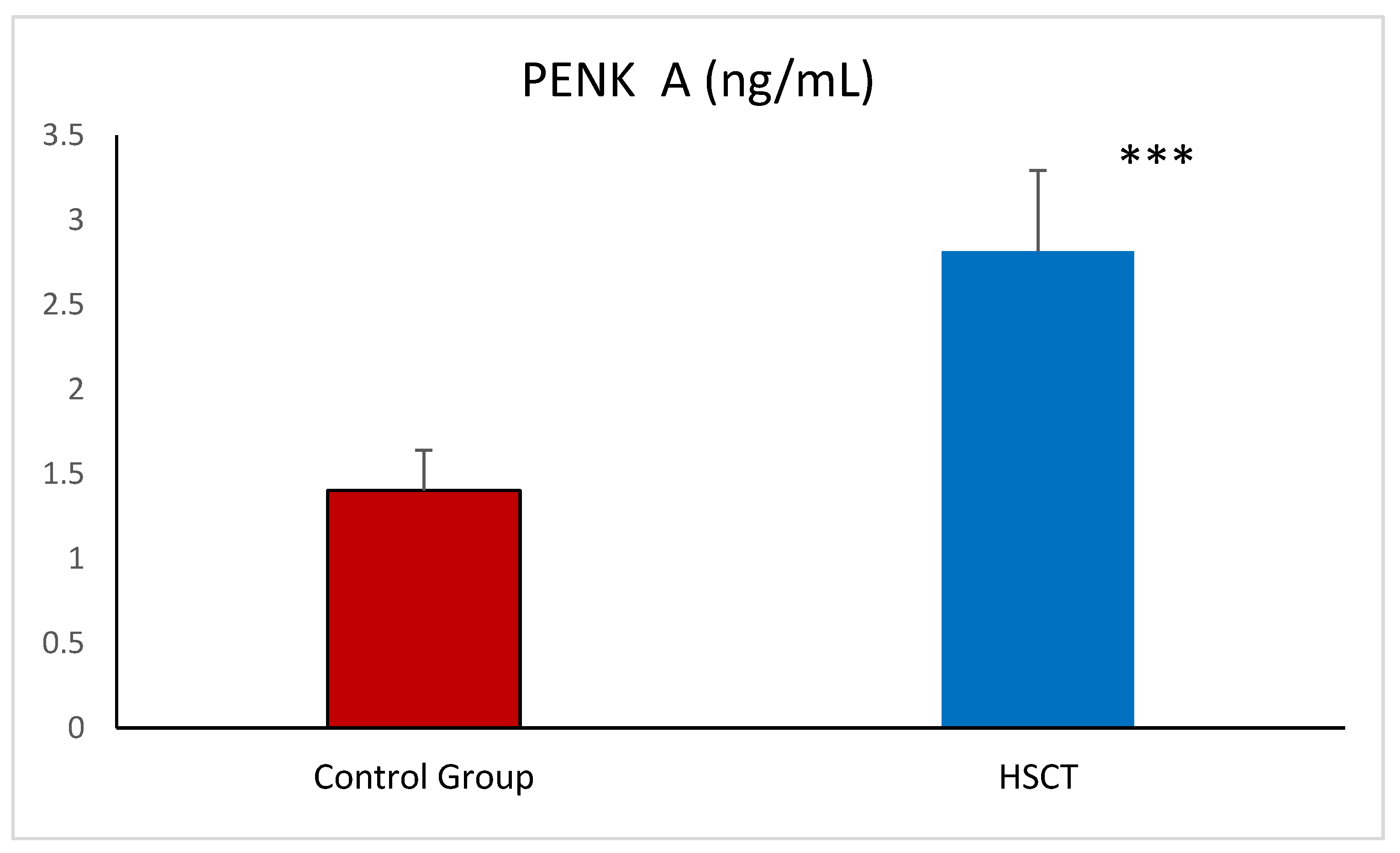
| PENK A (ng/mL) | 2.57 ± 0.43 | 2.90 ± 0.44 * |
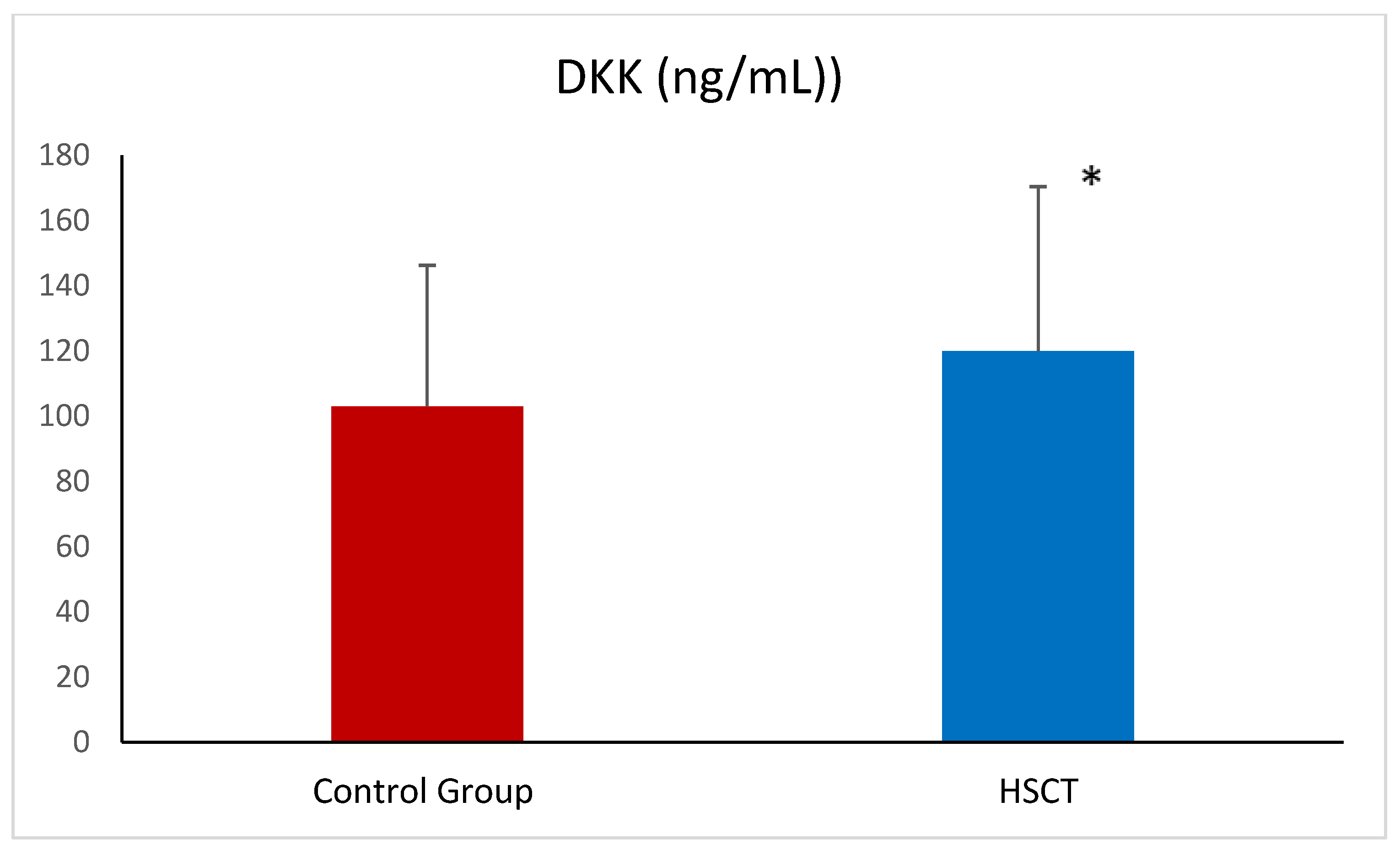
| DKK-3 (ng/mL)) | 47.69 ± 13.25 | 49.15 ± 14.65 |
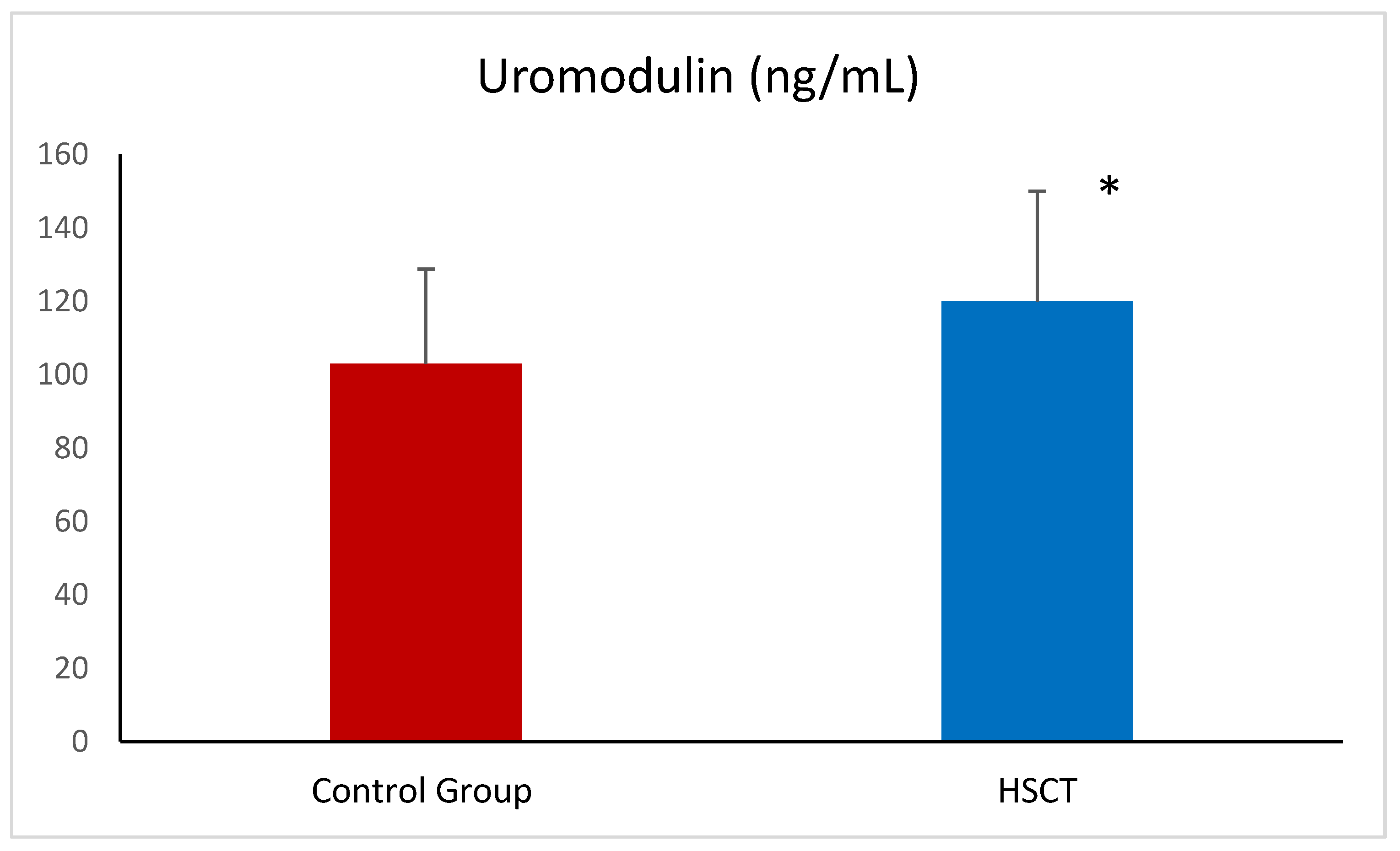
| Uromodulin (ng/mL) | 101.77 ± 28.12 | 119.70 ± 27.73 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaszyńska, A.; Kępska-Dzilińska, M.; Karakulska-Prystupiuk, E.; Tomaszewska, A.; Basak, G.W.; Żórawski, M.; Jakubowska, Z.; Małyszko, J. Markers of Kidney Injury: Proenkephalin A and Uromodulin, but Not Dickkopf-3, Are Elevated in Patients After Hematopoietic Stem Cell Transplantation. Int. J. Mol. Sci. 2025, 26, 3581. https://doi.org/10.3390/ijms26083581
Kaszyńska A, Kępska-Dzilińska M, Karakulska-Prystupiuk E, Tomaszewska A, Basak GW, Żórawski M, Jakubowska Z, Małyszko J. Markers of Kidney Injury: Proenkephalin A and Uromodulin, but Not Dickkopf-3, Are Elevated in Patients After Hematopoietic Stem Cell Transplantation. International Journal of Molecular Sciences. 2025; 26(8):3581. https://doi.org/10.3390/ijms26083581
Chicago/Turabian StyleKaszyńska, Aleksandra, Małgorzata Kępska-Dzilińska, Ewa Karakulska-Prystupiuk, Agnieszka Tomaszewska, Grzegorz Władysław Basak, Marcin Żórawski, Zuzanna Jakubowska, and Jolanta Małyszko. 2025. "Markers of Kidney Injury: Proenkephalin A and Uromodulin, but Not Dickkopf-3, Are Elevated in Patients After Hematopoietic Stem Cell Transplantation" International Journal of Molecular Sciences 26, no. 8: 3581. https://doi.org/10.3390/ijms26083581
APA StyleKaszyńska, A., Kępska-Dzilińska, M., Karakulska-Prystupiuk, E., Tomaszewska, A., Basak, G. W., Żórawski, M., Jakubowska, Z., & Małyszko, J. (2025). Markers of Kidney Injury: Proenkephalin A and Uromodulin, but Not Dickkopf-3, Are Elevated in Patients After Hematopoietic Stem Cell Transplantation. International Journal of Molecular Sciences, 26(8), 3581. https://doi.org/10.3390/ijms26083581