
The Genetics of Primary Familial Brain Calcification: A Literature Review
 , and
, and
Abstract
1. Introduction
2. Clinical Presentations
3. Imaging Features
4. Diagnostic Criteria
- Progressive neurological dysfunction, usually including movement and neuropsychiatric manifestations;
- The bilateral calcification of basal ganglia according to neuroimaging, with or without the involvement of other brain regions;
- The exclusion of other causes of calcification, such as metabolic problems, mitochondrial diseases, infectious, toxic, or traumatic causes;
- A positive family history of PFBC [29].
5. Differential Diagnosis
6. Genetics and Disease Mechanism
6.1. SLC20A2
6.2. PDGFRB
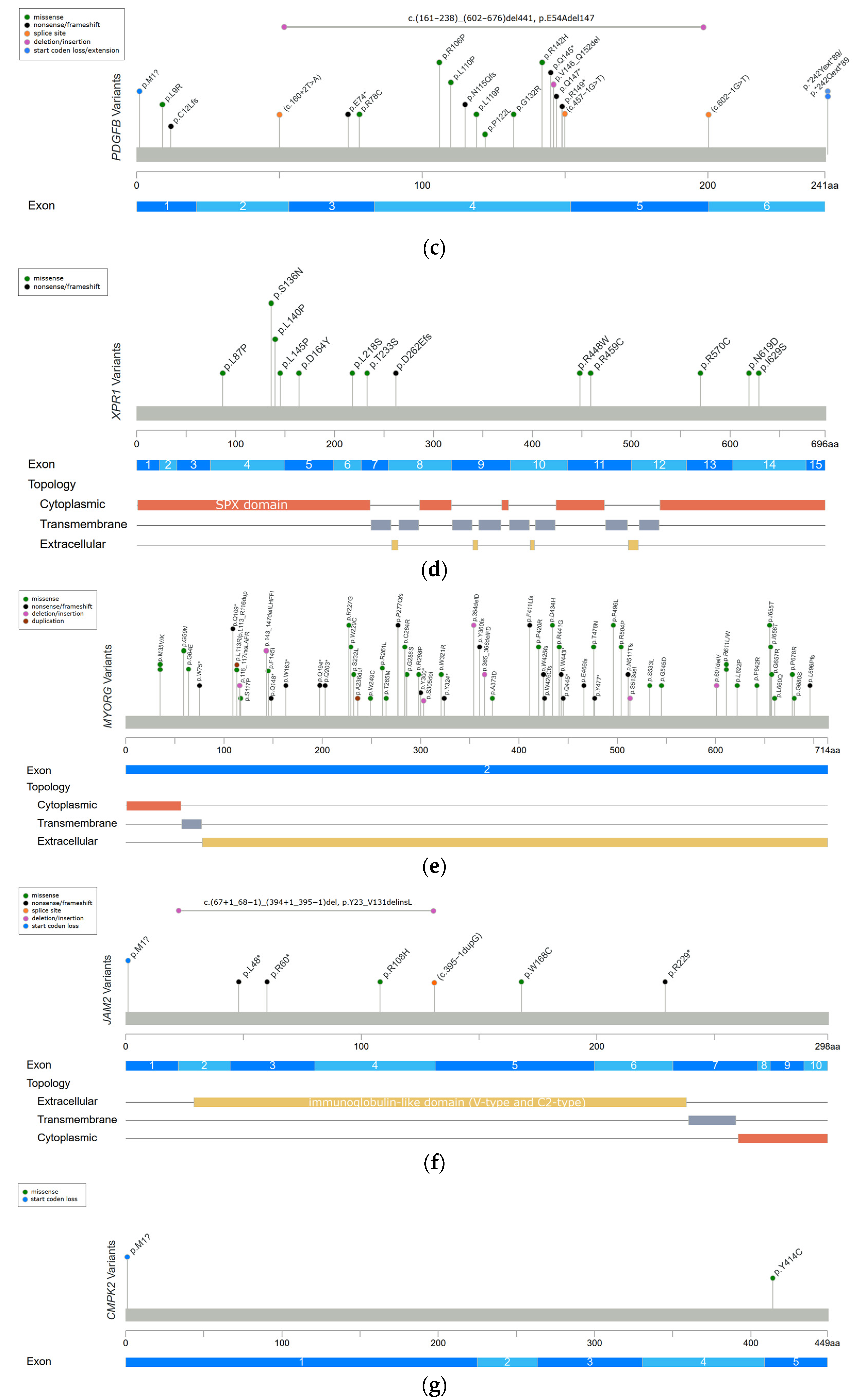
6.3. PDGFB
6.4. XPR1
6.5. MYORG
6.6. JAM2
6.7. CMPK2
6.8. Possible Pathophysiological Mechanisms of PFBC
6.9. Composition of Calcification in PFBC
7. Treatment
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| PFBC | primary familial brain calcification |
| TCS | total calcification score |
| CT | computerized tomography |
| MRI | magnetic resonance imaging |
| SWI | susceptibility weighted imaging |
| Pi | inorganic phosphate |
| PiT1 | inorganic phosphate transporter 1 |
| PiT2 | inorganic phosphate transporter 2 |
| Slc20a2−/− mice | Slc20a2 homozygous knockout mice |
| CSF | cerebrospinal fluid |
| PDGF | platelet-derived growth factor |
| PDGF-Rβ | platelet-derived growth factor receptor-β |
| SCMs | smooth muscle cells |
| BBB | blood–brain barrier |
| XPR1 | xenotropic and polytropic retrovirus receptor 1 |
| MYORG | myogenesis regulating glycosidase |
| JAM2 | junctional-adhesion-molecule-2 |
| UMP-CMPK2 | uridine monophosphate-cytidine monophosphate kinase 2 |
| WT | wide-type |
| NVU | neurovascular unit |
| PDGFBret/ret mice | mice hypomorphic for PFGFB |
| SPARCL1 | secreted protein acidic and rich in cysteine-like 1 |
| AHSG | alpha 2-Heremans-Schmid glycoprotein |
| MGP | matrix gla protein |
| OPN | osteopontin |
References
- Tadic, V.; Westenberger, A.; Domingo, A.; Alvarez-Fischer, D.; Klein, C.; Kasten, M. Primary familial brain calcification with known gene mutations: A systematic review and challenges of phenotypic characterization. JAMA Neurol. 2015, 72, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Westenberger, A.; Balck, A.; Klein, C. Primary familial brain calcifications: Genetic and clinical update. Curr. Opin. Neurol. 2019, 32, 571–578. [Google Scholar] [CrossRef]
- Balck, A.; Schaake, S.; Kuhnke, N.S.; Domingo, A.; Madoev, H.; Margolesky, J.; Dobricic, V.; Alvarez-Fischer, D.; Laabs, B.H.; Kasten, M.; et al. Genotype-Phenotype Relations in Primary Familial Brain Calcification: Systematic MDSGene Review. Mov. Disord. 2021, 36, 2468–2480. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.; Charbonnier, C.; Campion, D.; Veltman, J.A. Estimation of minimal disease prevalence from population genomic data: Application to primary familial brain calcification. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2018, 177, 68–74. [Google Scholar] [CrossRef]
- Chen, S.; Cen, Z.; Fu, F.; Chen, Y.; Chen, X.; Yang, D.; Wang, H.; Wu, H.; Zheng, X.; Xie, F.; et al. Underestimated disease prevalence and severe phenotypes in patients with biallelic variants: A cohort study of primary familial brain calcification from China. Park. Relat. Disord. 2019, 64, 211–219. [Google Scholar] [CrossRef]
- Wang, C.; Li, Y.; Shi, L.; Ren, J.; Patti, M.; Wang, T.; de Oliveira, J.R.; Sobrido, M.J.; Quintans, B.; Baquero, M.; et al. Mutations in SLC20A2 link familial idiopathic basal ganglia calcification with phosphate homeostasis. Nat. Genet. 2012, 44, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.; Pottier, C.; Maltete, D.; Coutant, S.; Rovelet-Lecrux, A.; Legallic, S.; Rousseau, S.; Vaschalde, Y.; Guyant-Marechal, L.; Augustin, J.; et al. Mutation of the PDGFRB gene as a cause of idiopathic basal ganglia calcification. Neurology 2013, 80, 181–187. [Google Scholar] [CrossRef]
- Keller, A.; Westenberger, A.; Sobrido, M.J.; Garcia-Murias, M.; Domingo, A.; Sears, R.L.; Lemos, R.R.; Ordonez-Ugalde, A.; Nicolas, G.; da Cunha, J.E.; et al. Mutations in the gene encoding PDGF-B cause brain calcifications in humans and mice. Nat. Genet. 2013, 45, 1077–1082. [Google Scholar] [CrossRef]
- Legati, A.; Giovannini, D.; Nicolas, G.; Lopez-Sanchez, U.; Quintans, B.; Oliveira, J.R.; Sears, R.L.; Ramos, E.M.; Spiteri, E.; Sobrido, M.J.; et al. Mutations in XPR1 cause primary familial brain calcification associated with altered phosphate export. Nat. Genet. 2015, 47, 579–581. [Google Scholar] [CrossRef]
- Yao, X.P.; Cheng, X.; Wang, C.; Zhao, M.; Guo, X.X.; Su, H.Z.; Lai, L.L.; Zou, X.H.; Chen, X.J.; Zhao, Y.; et al. Biallelic Mutations in MYORG Cause Autosomal Recessive Primary Familial Brain Calcification. Neuron 2018, 98, 1116–1123 e1115. [Google Scholar] [CrossRef]
- Schottlaender, L.V.; Abeti, R.; Jaunmuktane, Z.; Macmillan, C.; Chelban, V.; O’Callaghan, B.; McKinley, J.; Maroofian, R.; Efthymiou, S.; Athanasiou-Fragkouli, A.; et al. Bi-allelic JAM2 Variants Lead to Early-Onset Recessive Primary Familial Brain Calcification. Am. J. Hum. Genet. 2020, 106, 412–421. [Google Scholar] [CrossRef]
- Cen, Z.; Chen, Y.; Chen, S.; Wang, H.; Yang, D.; Zhang, H.; Wu, H.; Wang, L.; Tang, S.; Ye, J.; et al. Biallelic loss-of-function mutations in JAM2 cause primary familial brain calcification. Brain 2020, 143, 491–502. [Google Scholar] [CrossRef]
- Zhao, M.; Su, H.Z.; Zeng, Y.H.; Sun, Y.; Guo, X.X.; Li, Y.L.; Wang, C.; Zhao, Z.Y.; Huang, X.J.; Lin, K.J.; et al. Loss of function of CMPK2 causes mitochondria deficiency and brain calcification. Cell Discov. 2022, 8, 128. [Google Scholar] [CrossRef]
- Xu, X.; Sun, H.; Luo, J.; Cheng, X.; Lv, W.; Luo, W.; Chen, W.J.; Xiong, Z.Q.; Liu, J.Y. The Pathology of Primary Familial Brain Calcification: Implications for Treatment. Neurosci. Bull. 2022, 39, 659–674. [Google Scholar] [CrossRef]
- Carecchio, M.; Mainardi, M.; Bonato, G. The clinical and genetic spectrum of primary familial brain calcification. J. Neurol. 2023, 270, 3270–3277. [Google Scholar] [CrossRef]
- Quintans, B.; Oliveira, J.; Sobrido, M.J. Primary familial brain calcifications. Handb. Clin. Neurol. 2018, 147, 307–317. [Google Scholar] [CrossRef]
- Zhan, F.X.; Tian, W.T.; Zhang, C.; Zhu, Z.Y.; Wang, S.G.; Huang, X.J.; Cao, L. Primary familial brain calcification presenting as paroxysmal kinesigenic dyskinesia: Genetic and functional analyses. Neurosci. Lett. 2020, 714, 134543. [Google Scholar] [CrossRef]
- Zhu, M.; Zhu, X.; Wan, H.; Hong, D. Familial IBGC caused by SLC20A2 mutation presenting as paroxysmal kinesigenic dyskinesia. Park. Relat. Disord. 2014, 20, 353–354. [Google Scholar] [CrossRef]
- Tang, L.O.; Hou, B.H.; Zhang, X.N.; Xi, Z.Y.; Li, C.X.; Xu, L. Biallelic XPR1 mutation associated with primary familial brain calcification presenting as paroxysmal kinesigenic dyskinesia with infantile convulsions. Brain Dev. 2021, 43, 331–336. [Google Scholar] [CrossRef]
- Benke, T.; Karner, E.; Seppi, K.; Delazer, M.; Marksteiner, J.; Donnemiller, E. Subacute dementia and imaging correlates in a case of Fahr’s disease. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1163–1165. [Google Scholar] [CrossRef]
- Nicolas, G.; Pottier, C.; Charbonnier, C.; Guyant-Marechal, L.; Le Ber, I.; Pariente, J.; Labauge, P.; Ayrignac, X.; Defebvre, L.; Maltete, D.; et al. Phenotypic spectrum of probable and genetically-confirmed idiopathic basal ganglia calcification. Brain 2013, 136, 3395–3407. [Google Scholar] [CrossRef] [PubMed]
- Grangeon, L.; Wallon, D.; Charbonnier, C.; Quenez, O.; Richard, A.C.; Rousseau, S.; Budowski, C.; Lebouvier, T.; Corbille, A.G.; Vidailhet, M.; et al. Biallelic MYORG mutation carriers exhibit primary brain calcification with a distinct phenotype. Brain 2019, 142, 1573–1586. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ma, G.; Zhao, Z.; Zhu, M. SCL20A2 mutation presenting with acute ischemic stroke: A case report. BMC Neurol. 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Li, J.; Jiao, B.; Weng, L. Primary familial brain calcification in a patient with a novel compound heterozygous mutation in MYORG presenting with an acute ischemic stroke: A case report. Ann. Transl. Med. 2022, 10, 423. [Google Scholar] [CrossRef]
- Gao, L.; Chen, J.; Dong, H.; Li, X. A novel mutation in MYORG leads to primary familial brain calcification and cerebral infarction. Int. J. Neurosci. 2022, 132, 1182–1186. [Google Scholar] [CrossRef]
- Sadok, S.H.; Borges-Medeiros, R.L.; de Oliveira, D.F.; Zatz, M.; de Oliveira, J.R.M. Report of a young patient with brain calcifications with a novel homozygous MYORG variant. Gene 2023, 859, 147213. [Google Scholar] [CrossRef]
- Song, T.; Zhao, Y.; Wen, G.; Du, J.; Xu, Q. A novel MYORG mutation causes primary familial brain calcification with migraine: Case report and literature review. Front. Neurol. 2023, 14, 1110227. [Google Scholar] [CrossRef]
- Borges-Medeiros, R.L.; de Oliveira, J.R.M. Digenic Variants as Possible Clinical Modifier of Primary Familial Brain Calcification Patients. J. Mol. Neurosci. 2020, 70, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.M.; Oliveira, J.; Sobrido, M.J.; Coppola, G. Primary Familial Brain Calcification. In GeneReviews®; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Chen, Y.; Cen, Z.; Chen, X.; Wang, H.; Chen, S.; Yang, D.; Fu, F.; Wang, L.; Liu, P.; Wu, H.; et al. MYORG Mutation Heterozygosity Is Associated With Brain Calcification. Mov. Disord. 2020, 35, 679–686. [Google Scholar] [CrossRef]
- Andretta, S.; Bonato, G.; Mainardi, M.; Salviati, L.; Antonini, A.; Carecchio, M. Symptomatic brain calcifications in two patients with JAM2 monoallelic variants. Mov. Disord. 2022, 37, S379–S380. [Google Scholar]
- Azad, R.; Mittal, P.; Malhotra, A.; Gangrade, S. Detection and Differentiation of Focal Intracranial Calcifications and Chronic Microbleeds Using MRI. J. Clin. Diagn. Res. 2017, 11, TC19–TC23. [Google Scholar] [CrossRef]
- Halefoglu, A.M.; Yousem, D.M. Susceptibility weighted imaging: Clinical applications and future directions. World J. Radiol. 2018, 10, 30–45. [Google Scholar] [CrossRef]
- Moskowitz, M.A.; Winickoff, R.N.; Heinz, E.R. Familial calcification of the basal ganglions: A metabolic and genetic study. N. Engl. J. Med. 1971, 285, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Ellie, E.; Julien, J.; Ferrer, X. Familial idiopathic striopallidodentate calcifications. Neurology 1989, 39, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Manyam, B.V. What is and what is not ‘Fahr’s disease’. Park. Relat. Disord. 2005, 11, 73–80. [Google Scholar] [CrossRef]
- Ferreira, J.B.; Pimentel, L.; Keasey, M.P.; Lemos, R.R.; Santos, L.M.; Oliveira, M.F.; Santos, S.; Jensen, N.; Teixeira, K.; Pedersen, L.; et al. First report of a de novo mutation at SLC20A2 in a patient with brain calcification. J. Mol. Neurosci. 2014, 54, 748–751. [Google Scholar] [CrossRef]
- Forstl, H.; Krumm, B.; Eden, S.; Kohlmeyer, K. Neurological disorders in 166 patients with basal ganglia calcification: A statistical evaluation. J. Neurol. 1992, 239, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Eskandary, H.; Sabba, M.; Khajehpour, F.; Eskandari, M. Incidental findings in brain computed tomography scans of 3000 head trauma patients. Surg. Neurol. 2005, 63, 550–553; discussion 553. [Google Scholar] [CrossRef]
- Yamada, M.; Asano, T.; Okamoto, K.; Hayashi, Y.; Kanematsu, M.; Hoshi, H.; Akaiwa, Y.; Shimohata, T.; Nishizawa, M.; Inuzuka, T.; et al. High frequency of calcification in basal ganglia on brain computed tomography images in Japanese older adults. Geriatr. Gerontol. Int. 2013, 13, 706–710. [Google Scholar] [CrossRef]
- da Silva, R.J.; Pereira, I.C.; Oliveira, J.R. Analysis of gene expression pattern and neuroanatomical correlates for SLC20A2 (PiT-2) shows a molecular network with potential impact in idiopathic basal ganglia calcification (“Fahr’s disease”). J. Mol. Neurosci. 2013, 50, 280–283. [Google Scholar] [CrossRef]
- Larsen, F.T.; Jensen, N.; Autzen, J.K.; Kongsfelt, I.B.; Pedersen, L. Primary Brain Calcification Causal PiT2 Transport-Knockout Variants can Exert Dominant Negative Effects on Wild-Type PiT2 Transport Function in Mammalian Cells. J. Mol. Neurosci. 2017, 61, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Arts, F.A.; Velghe, A.I.; Stevens, M.; Renauld, J.C.; Essaghir, A.; Demoulin, J.B. Idiopathic basal ganglia calcification-associated PDGFRB mutations impair the receptor signalling. J. Cell. Mol. Med. 2015, 19, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Vanlandewijck, M.; Lebouvier, T.; Andaloussi Mae, M.; Nahar, K.; Hornemann, S.; Kenkel, D.; Cunha, S.I.; Lennartsson, J.; Boss, A.; Heldin, C.H.; et al. Functional Characterization of Germline Mutations in PDGFB and PDGFRB in Primary Familial Brain Calcification. PLoS ONE 2015, 10, e0143407. [Google Scholar] [CrossRef]
- Andrae, J.; Gallini, R.; Betsholtz, C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev. 2008, 22, 1276–1312. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.P.; Zhao, M.; Wang, C.; Guo, X.X.; Su, H.Z.; Dong, E.L.; Chen, H.T.; Lai, J.H.; Liu, Y.B.; Wang, N.; et al. Analysis of gene expression and functional characterization of XPR1: A pathogenic gene for primary familial brain calcification. Cell Tissue Res. 2017, 370, 267–273. [Google Scholar] [CrossRef]
- Xu, Y.; Johansson, M.; Karlsson, A. Human UMP-CMP kinase 2, a novel nucleoside monophosphate kinase localized in mitochondria. J. Biol. Chem. 2008, 283, 1563–1571. [Google Scholar] [CrossRef]
- Baker, M.; Strongosky, A.J.; Sanchez-Contreras, M.Y.; Yang, S.; Ferguson, W.; Calne, D.B.; Calne, S.; Stoessl, A.J.; Allanson, J.E.; Broderick, D.F.; et al. SLC20A2 and THAP1 deletion in familial basal ganglia calcification with dystonia. Neurogenetics 2014, 15, 23–30. [Google Scholar] [CrossRef]
- Batla, A.; Stamelou, M. Primary familial brain calcification in the IBGC2 kindred: All linkage roads lead to SLC20A2. Mov. Disord. 2016, 31, 1765–1766. [Google Scholar] [CrossRef]
- Giorgio, E.; Garelli, E.; Carando, A.; Bellora, S.; Rubino, E.; Quarello, P.; Sirchia, F.; Marrama, F.; Gallone, S.; Grosso, E.; et al. Design of a multiplex ligation-dependent probe amplification assay for SLC20A2: Identification of two novel deletions in primary familial brain calcification. J. Hum. Genet. 2019, 64, 1083–1090. [Google Scholar] [CrossRef]
- Guo, X.X.; Su, H.Z.; Zou, X.H.; Lai, L.L.; Lu, Y.Q.; Wang, C.; Li, Y.L.; Hong, J.M.; Zhao, M.; Lin, K.X.; et al. Identification of SLC20A2 deletions in patients with primary familial brain calcification. Clin. Genet. 2019, 96, 53–60. [Google Scholar] [CrossRef]
- Gagliardi, M.; Morelli, M.; Annesi, G.; Nicoletti, G.; Perrotta, P.; Pustorino, G.; Iannello, G.; Tarantino, P.; Gambardella, A.; Quattrone, A. A new SLC20A2 mutation identified in southern Italy family with primary familial brain calcification. Gene 2015, 568, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.X.; Zou, X.H.; Wang, C.; Yao, X.P.; Su, H.Z.; Lai, L.L.; Chen, H.T.; Lai, J.H.; Liu, Y.B.; Chen, D.P.; et al. Spectrum of SLC20A2, PDGFRB, PDGFB, and XPR1 mutations in a large cohort of patients with primary familial brain calcification. Hum. Mutat. 2019, 40, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.J.; Yao, X.P.; Zhang, Q.J.; Ni, W.; He, J.; Li, H.F.; Liu, X.Y.; Zhao, G.X.; Murong, S.X.; Wang, N.; et al. Novel SLC20A2 mutations identified in southern Chinese patients with idiopathic basal ganglia calcification. Gene 2013, 529, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Nishii, K.; Shimogawa, R.; Kurita, H.; Inden, M.; Kobayashi, M.; Toyoshima, I.; Taguchi, Y.; Ueda, A.; Tamune, H.; Hozumi, I. Partial reduced Pi transport function of PiT-2 might not be sufficient to induce brain calcification of idiopathic basal ganglia calcification. Sci. Rep. 2019, 9, 17288. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.M.; Carecchio, M.; Lemos, R.; Ferreira, J.; Legati, A.; Sears, R.L.; Hsu, S.C.; Panteghini, C.; Magistrelli, L.; Salsano, E.; et al. Primary brain calcification: An international study reporting novel variants and associated phenotypes. Eur. J. Hum. Genet. 2018, 26, 1462–1477. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Tanaka, M.; Takagi, M.; Kobayashi, S.; Taguchi, Y.; Takashima, S.; Tanaka, K.; Touge, T.; Hatsuta, H.; Murayama, S.; et al. Evaluation of SLC20A2 mutations that cause idiopathic basal ganglia calcification in Japan. Neurology 2014, 82, 705–712. [Google Scholar] [CrossRef]
- Ding, Y.; Dong, H.Q. A Novel SLC20A2 Mutation Associated with Familial Idiopathic Basal Ganglia Calcification and Analysis of the Genotype-Phenotype Association in Chinese Patients. Chin. Med. J. 2018, 131, 799–803. [Google Scholar] [CrossRef]
- Koyama, S.; Sato, H.; Kobayashi, R.; Kawakatsu, S.; Kurimura, M.; Wada, M.; Kawanami, T.; Kato, T. Clinical and radiological diversity in genetically confirmed primary familial brain calcification. Sci. Rep. 2017, 7, 12046. [Google Scholar] [CrossRef]
- Magistrelli, L.; Croce, R.; De Marchi, F.; Basagni, C.; Carecchio, M.; Nasuelli, N.; Cantello, R.; Invernizzi, F.; Garavaglia, B.; Comi, C.; et al. Expanding the genetic spectrum of primary familial brain calcification due to SLC2OA2 mutations: A case series. Neurogenetics 2021, 22, 65–70. [Google Scholar] [CrossRef]
- Kasuga, K.; Konno, T.; Saito, K.; Ishihara, A.; Nishizawa, M.; Ikeuchi, T. A Japanese family with idiopathic basal ganglia calcification with novel SLC20A2 mutation presenting with late-onset hallucination and delusion. J. Neurol. 2014, 261, 242–244. [Google Scholar] [CrossRef]
- Carecchio, M.; Barzaghi, C.; Varrasi, C.; Cantello, R.; Garavaglia, B. Adult-Onset Focal Chorea in Fahr’s Disease Resulting From SLC20A2 Mutation: A Novel Phenotype. Mov. Disord. Clin. Pract. 2015, 2, 79–80. [Google Scholar] [CrossRef][Green Version]
- Hsu, S.C.; Sears, R.L.; Lemos, R.R.; Quintans, B.; Huang, A.; Spiteri, E.; Nevarez, L.; Mamah, C.; Zatz, M.; Pierce, K.D.; et al. Mutations in SLC20A2 are a major cause of familial idiopathic basal ganglia calcification. Neurogenetics 2013, 14, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Konno, T.; Blackburn, P.R.; Rozen, T.D.; van Gerpen, J.A.; Ross, O.A.; Atwal, P.S.; Wszolek, Z.K. Anticipation in a family with primary familial brain calcification caused by an SLC20A2 variant. Neurol. Neurochir. Pol. 2018, 52, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, X.; Wu, A. Association between a novel mutation in SLC20A2 and familial idiopathic basal ganglia calcification. PLoS ONE 2013, 8, e57060. [Google Scholar] [CrossRef] [PubMed]
- Lemos, R.R.; Ramos, E.M.; Legati, A.; Nicolas, G.; Jenkinson, E.M.; Livingston, J.H.; Crow, Y.J.; Campion, D.; Coppola, G.; Oliveira, J.R. Update and Mutational Analysis of SLC20A2: A Major Cause of Primary Familial Brain Calcification. Hum. Mutat. 2015, 36, 489–495. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, Z.; Sun, H.; Zhang, S.; Zhang, J.; Wang, Y.; Fang, H.; Xu, Y. Generation of induced pluripotent stem cell line (ZZUi0012-A) from a patient with Fahr’s disease caused by a novel mutation in SLC20A2 gene. Stem Cell Res. 2019, 35, 101395. [Google Scholar] [CrossRef]
- Huang, Y.T.; Zhang, L.H.; Li, M.F.; Cheng, L.; Zou, G.Y.; Zhou, H.H. A splice site mutation causing exon 6 skipping in SLC20A2 gene in a primary familial brain calcification family. Brain Res. Bull. 2019, 150, 261–265. [Google Scholar] [CrossRef]
- Shen, Y.; Shu, S.; Ren, Y.; Xia, W.; Chen, J.; Dong, L.; Ge, H.; Fan, S.; Shi, L.; Peng, B.; et al. Case Report: Two Novel Frameshift Mutations in SLC20A2 and One Novel Splice Donor Mutation in PDGFB Associated With Primary Familial Brain Calcification. Front. Genet. 2021, 12, 643452. [Google Scholar] [CrossRef]
- Rohani, M.; Poon, Y.Y.; Naranian, T.; Fasano, A. SCL20A2 mutation mimicking fluctuating Parkinson’s disease. Park. Relat. Disord. 2017, 39, 93–94. [Google Scholar] [CrossRef]
- Knowles, J.K.; Santoro, J.D.; Porter, B.E.; Baumer, F.M. Refractory focal epilepsy in a paediatric patient with primary familial brain calcification. Seizure 2018, 56, 50–52. [Google Scholar] [CrossRef]
- Li, M.; Fu, Q.; Xiang, L.; Zheng, Y.; Ping, W.; Cao, Y. SLC20A2-Associated Idiopathic basal ganglia calcification (Fahr disease): A case family report. BMC Neurol. 2022, 22, 438. [Google Scholar] [CrossRef] [PubMed]
- Taglia, I.; Mignarri, A.; Olgiati, S.; Menci, E.; Petrocelli, P.L.; Breedveld, G.J.; Scaglione, C.; Martinelli, P.; Federico, A.; Bonifati, V.; et al. Primary familial brain calcification: Genetic analysis and clinical spectrum. Mov. Disord. 2014, 29, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Paucar, M.; Almqvist, H.; Jelic, V.; Hagman, G.; Jorneskog, G.; Holmin, S.; Bjorkhem, I.; Svenningsson, P. A SLC20A2 gene mutation carrier displaying ataxia and increased levels of cerebrospinal fluid phosphate. J. Neurol. Sci. 2017, 375, 245–247. [Google Scholar] [CrossRef]
- Lemos, R.R.; Oliveira, M.F.; Oliveira, J.R.M. Reporting a new mutation at the SLC20A2 gene in familial idiopathic basal ganglia calcification. Eur. J. Neurol. 2013, 20, e43–e44. [Google Scholar] [CrossRef]
- Uno, A.; Tamune, H.; Kurita, H.; Hozumi, I.; Yamamoto, N. SLC20A2-Associated Idiopathic Basal Ganglia Calcification-Related Recurrent Psychosis Response to Low-Dose Antipsychotics: A Case Report and Literature Review. Cureus 2020, 12, e12407. [Google Scholar] [CrossRef] [PubMed]
- Rubino, E.; Giorgio, E.; Gallone, S.; Pinessi, L.; Orsi, L.; Gentile, S.; Duca, S.; Brusco, A. Novel mutation of SLC20A2 in an Italian patient presenting with migraine. J. Neurol. 2014, 261, 2019–2021. [Google Scholar] [CrossRef][Green Version]
- Coppola, A.; Hernandez-Hernandez, L.; Balestrini, S.; Krithika, S.; Moran, N.; Hale, B.; Cordivari, C.; Sisodiya, S.M. Cortical myoclonus and epilepsy in a family with a new SLC20A2 mutation. J. Neurol. 2020, 267, 2221–2227. [Google Scholar] [CrossRef]
- Brighina, L.; Saracchi, E.; Ferri, F.; Gagliardi, M.; Tarantino, P.; Morzenti, S.; Musarra, M.; Patassini, M.; Annesi, G.; Ferrarese, C. Fahr’s disease linked to a novel SLC20A2 gene mutation manifesting with dynamic aphasia. Neurodegener. Dis. 2014, 14, 133–138. [Google Scholar] [CrossRef]
- Fjaer, R.; Brodtkorb, E.; Oye, A.M.; Sheng, Y.; Vigeland, M.D.; Kvistad, K.A.; Backe, P.H.; Selmer, K.K. Generalized epilepsy in a family with basal ganglia calcifications and mutations in SLC20A2 and CHRNB2. Eur. J. Med. Genet. 2015, 58, 624–628. [Google Scholar] [CrossRef]
- Bu, W.; Hou, L.; Zhu, M.; Zhang, R.; Zhang, X.; Zhang, X.; Tang, J.; Liu, X. SLC20A2-related primary familial brain calcification with purely acute psychiatric symptoms: A case report. BMC Neurol. 2022, 22, 265. [Google Scholar] [CrossRef]
- Sun, H.; Cao, Z.; Gao, R.; Li, Y.; Chen, R.; Du, S.; Ma, T.; Wang, J.; Xu, X.; Liu, J.Y. Severe brain calcification and migraine headache caused by SLC20A2 and PDGFRB heterozygous mutations in a five-year-old Chinese girl. Mol. Genet. Genom. Med. 2021, 9, e1670. [Google Scholar] [CrossRef]
- Sekine, S.I.; Kondo, T.; Murakami, N.; Imamura, K.; Enami, T.; Shibukawa, R.; Tsukita, K.; Funayama, M.; Inden, M.; Kurita, H.; et al. Induced pluripotent stem cells derived from a patient with familial idiopathic basal ganglia calcification (IBGC) caused by a mutation in SLC20A2 gene. Stem Cell Res. 2017, 24, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Taglia, I.; Formichi, P.; Battisti, C.; Peppoloni, G.; Barghigiani, M.; Tessa, A.; Federico, A. Primary familial brain calcification with a novel SLC20A2 mutation: Analysis of PiT-2 expression and localization. J. Cell. Physiol. 2018, 233, 2324–2331. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.C.; Redmond, J.; Bradley, D.; Bede, P. Teaching NeuroImage: Primary Familial Brain Calcification in SLC20A2 Genotype. Neurology 2022, 99, 1008–1009. [Google Scholar] [CrossRef]
- Jensen, N.; Schroder, H.D.; Hejbol, E.K.; Fuchtbauer, E.M.; de Oliveira, J.R.; Pedersen, L. Loss of function of Slc20a2 associated with familial idiopathic Basal Ganglia calcification in humans causes brain calcifications in mice. J. Mol. Neurosci. 2013, 51, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Jensen, N.; Schroder, H.D.; Hejbol, E.K.; Thomsen, J.S.; Bruel, A.; Larsen, F.T.; Vinding, M.C.; Orlowski, D.; Fuchtbauer, E.M.; Oliveira, J.R.M.; et al. Mice Knocked Out for the Primary Brain Calcification-Associated Gene Slc20a2 Show Unimpaired Prenatal Survival but Retarded Growth and Nodules in the Brain that Grow and Calcify Over Time. Am. J. Pathol. 2018, 188, 1865–1881. [Google Scholar] [CrossRef]
- Kimura, T.; Miura, T.; Aoki, K.; Saito, S.; Hondo, H.; Konno, T.; Uchiyama, A.; Ikeuchi, T.; Takahashi, H.; Kakita, A. Familial idiopathic basal ganglia calcification: Histopathologic features of an autopsied patient with an SLC20A2 mutation. Neuropathology 2016, 36, 365–371. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, Y.; Zhang, Y.; Li, Y.; Xu, C.; Peng, Z.; Jia, Y.; Qiao, S.; Zhang, Z.; Shi, L. T-cell infiltration in the central nervous system and their association with brain calcification in Slc20a2-deficient mice. Front. Mol. Neurosci. 2023, 16, 1073723. [Google Scholar] [CrossRef]
- Guerreiro, P.M.; Bataille, A.M.; Parker, S.L.; Renfro, J.L. Active removal of inorganic phosphate from cerebrospinal fluid by the choroid plexus. Am. J. Physiol. Renal. Physiol. 2014, 306, F1275–F1284. [Google Scholar] [CrossRef]
- Jensen, N.; Autzen, J.K.; Pedersen, L. SLC20A2 is critical for maintaining a physiologic inorganic phosphate level in cerebrospinal fluid. Neurogenetics 2016, 17, 125–130. [Google Scholar] [CrossRef]
- Hozumi, I.; Kurita, H.; Ozawa, K.; Furuta, N.; Inden, M.; Sekine, S.I.; Yamada, M.; Hayashi, Y.; Kimura, A.; Inuzuka, T.; et al. Inorganic phosphorus (Pi) in CSF is a biomarker for Slc20a2-associated idiopathic basal ganglia calcification (IBGC1). J. Neurol. Sci. 2018, 388, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yao, X.P.; Chen, H.T.; Lai, J.H.; Guo, X.X.; Su, H.Z.; Dong, E.L.; Zhang, Q.J.; Wang, N.; Chen, W.J. Novel mutations of PDGFRB cause primary familial brain calcification in Chinese families. J. Hum. Genet. 2017, 62, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Contreras, M.; Baker, M.C.; Finch, N.A.; Nicholson, A.; Wojtas, A.; Wszolek, Z.K.; Ross, O.A.; Dickson, D.W.; Rademakers, R. Genetic screening and functional characterization of PDGFRB mutations associated with basal ganglia calcification of unknown etiology. Hum. Mutat. 2014, 35, 964–971. [Google Scholar] [CrossRef]
- Villa-Bellosta, R.; Levi, M.; Sorribas, V. Vascular smooth muscle cell calcification and SLC20 inorganic phosphate transporters: Effects of PDGF, TNF-alpha, and Pi. Pflug. Arch. 2009, 458, 1151–1161. [Google Scholar] [CrossRef]
- Kakita, A.; Suzuki, A.; Nishiwaki, K.; Ono, Y.; Kotake, M.; Ariyoshi, Y.; Miura, Y.; Ltoh, M.; Oiso, Y. Stimulation of Na-dependent phosphate transport by platelet-derived growth factor in rat aortic smooth muscle cells. Atherosclerosis 2004, 174, 17–24. [Google Scholar] [CrossRef]
- Sekine, S.I.; Kaneko, M.; Tanaka, M.; Ninomiya, Y.; Kurita, H.; Inden, M.; Yamada, M.; Hayashi, Y.; Inuzuka, T.; Mitsui, J.; et al. Functional evaluation of PDGFB-variants in idiopathic basal ganglia calcification, using patient-derived iPS cells. Sci. Rep. 2019, 9, 5698. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Legati, A.; Nishikawa, T.; Coppola, G. First Japanese family with primary familial brain calcification due to a mutation in the PDGFB gene: An exome analysis study. Psychiatry Clin. Neurosci. 2015, 69, 77–83. [Google Scholar] [CrossRef]
- Nicolas, G.; Jacquin, A.; Thauvin-Robinet, C.; Rovelet-Lecrux, A.; Rouaud, O.; Pottier, C.; Aubriot-Lorton, M.H.; Rousseau, S.; Wallon, D.; Duvillard, C.; et al. A de novo nonsense PDGFB mutation causing idiopathic basal ganglia calcification with laryngeal dystonia. Eur. J. Hum. Genet. 2014, 22, 1236–1238. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Keogh, M.J.; Pyle, A.; Daud, D.; Griffin, H.; Douroudis, K.; Eglon, G.; Miller, J.; Horvath, R.; Chinnery, P.F. Clinical heterogeneity of primary familial brain calcification due to a novel mutation in PDGFB. Neurology 2015, 84, 1818–1820. [Google Scholar] [CrossRef]
- Biyajima, M.; Kobayashi, Y.; Nakafuji, K.; Watanabe, R.; Tazawa, K.; Ishii, W.; Satoh, S.; Hoshi, K.; Kurita, H.; Hozumi, I.; et al. Seronegative neuromyelitis optica spectrum disorder in primary familial brain calcification with PDGFB variant. eNeurologicalSci 2022, 27, 100406. [Google Scholar] [CrossRef]
- Yao, X.P.; Wang, C.; Su, H.Z.; Guo, X.X.; Lu, Y.Q.; Zhao, M.; Liu, Y.B.; Lai, J.H.; Chen, H.T.; Wang, N.; et al. Mutation screening of PDGFB gene in Chinese population with primary familial brain calcification. Gene 2016, 597, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Ma, X.; Xu, X.; Huang, B.; Sun, H.; Li, L.; Zhang, M.; Liu, J.Y. A PDGFB mutation causes paroxysmal nonkinesigenic dyskinesia with brain calcification. Mov. Disord. 2017, 32, 1104–1106. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.; Rovelet-Lecrux, A.; Pottier, C.; Martinaud, O.; Wallon, D.; Vernier, L.; Landemore, G.; Chapon, F.; Prieto-Morin, C.; Tournier-Lasserve, E.; et al. PDGFB partial deletion: A new, rare mechanism causing brain calcification with leukoencephalopathy. J. Mol. Neurosci. 2014, 53, 171–175. [Google Scholar] [CrossRef]
- Biancheri, R.; Severino, M.; Robbiano, A.; Iacomino, M.; Del Sette, M.; Minetti, C.; Cervasio, M.; Del Basso De Caro, M.; Striano, P.; Zara, F. White matter involvement in a family with a novel PDGFB mutation. Neurol. Genet. 2016, 2, e77. [Google Scholar] [CrossRef] [PubMed]
- Anheim, M.; Lopez-Sanchez, U.; Giovannini, D.; Richard, A.C.; Touhami, J.; N’Guyen, L.; Rudolf, G.; Thibault-Stoll, A.; Frebourg, T.; Hannequin, D.; et al. XPR1 mutations are a rare cause of primary familial brain calcification. J. Neurol. 2016, 263, 1559–1564. [Google Scholar] [CrossRef]
- Lopez-Sanchez, U.; Nicolas, G.; Richard, A.C.; Maltete, D.; Charif, M.; Ayrignac, X.; Goizet, C.; Touhami, J.; Labesse, G.; Battini, J.L.; et al. Characterization of XPR1/SLC53A1 variants located outside of the SPX domain in patients with primary familial brain calcification. Sci. Rep. 2019, 9, 6776. [Google Scholar] [CrossRef]
- Chelban, V.; Carecchio, M.; Rea, G.; Bowirrat, A.; Kirmani, S.; Magistrelli, L.; Efthymiou, S.; Schottlaender, L.; Vandrovcova, J.; Salpietro, V.; et al. MYORG-related disease is associated with central pontine calcifications and atypical parkinsonism. Neurol. Genet. 2020, 6, e399. [Google Scholar] [CrossRef]
- Zeng, Y.H.; Lin, B.W.; Su, H.Z.; Guo, X.X.; Li, Y.L.; Lai, L.L.; Chen, W.J.; Zhao, M.; Yao, X.P. Mutation Analysis of MYORG in a Chinese Cohort With Primary Familial Brain Calcification. Front. Genet. 2021, 12, 732389. [Google Scholar] [CrossRef]
- Forouhideh, Y.; Muller, K.; Ruf, W.; Assi, M.; Seker, T.; Tunca, C.; Knehr, A.; Strom, T.M.; Gorges, M.; Schradt, F.; et al. A biallelic mutation links MYORG to autosomal-recessive primary familial brain calcification. Brain 2019, 142, e4. [Google Scholar] [CrossRef]
- Ramos, E.M.; Roca, A.; Chumchim, N.; Dokuru, D.R.; Van Berlo, V.; De Michele, G.; Lieto, M.; Tedeschi, E.; De Michele, G.; Coppola, G. Primary familial brain calcification caused by a novel homozygous MYORG mutation in a consanguineous Italian family. Neurogenetics 2019, 20, 99–102. [Google Scholar] [CrossRef]
- Chen, Y.; Fu, F.; Chen, S.; Cen, Z.; Tang, H.; Huang, J.; Xie, F.; Zheng, X.; Yang, D.; Wang, H.; et al. Evaluation of MYORG mutations as a novel cause of primary familial brain calcification. Mov. Disord. 2019, 34, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Wang, P.; Chen, Z.; Jiang, H. A novel mutation in MYORG causes primary familial brain calcification with central neuropathic pain. Clin. Genet. 2019, 95, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Arkadir, D.; Lossos, A.; Rahat, D.; Abu Snineh, M.; Schueler-Furman, O.; Nitschke, S.; Minassian, B.A.; Sadaka, Y.; Lerer, I.; Tabach, Y.; et al. MYORG is associated with recessive primary familial brain calcification. Ann. Clin. Transl. Neurol. 2019, 6, 106–113. [Google Scholar] [CrossRef]
- Fei, B.N.; Su, H.Z.; Yao, X.P.; Ding, J.; Wang, X. Idiopathic basal ganglia calcification associated with new MYORG mutation site: A case report. World J. Clin. Cases 2021, 9, 7169–7174. [Google Scholar] [CrossRef]
- Tekin Orgun, L.; Besen, S.; Sangun, O.; Bisgin, A.; Alkan, O.; Erol, I. First pediatric case with primary familial brain calcification due to a novel variant on the MYORG gene and review of the literature. Brain Dev. 2021, 43, 789–797. [Google Scholar] [CrossRef]
- Chen, S.Y.; Lin, W.C.; Chang, Y.Y.; Lin, T.K.; Lan, M.Y. Brain hypoperfusion and nigrostriatal dopaminergic dysfunction in primary familial brain calcification caused by novel MYORG variants: Case report. BMC Neurol. 2020, 20, 329. [Google Scholar] [CrossRef]
- Kume, K.; Takata, T.; Morino, H.; Matsuda, Y.; Ohsawa, R.; Tada, Y.; Kurashige, T.; Kawakami, H. The first Japanese case of primary familial brain calcification caused by an MYORG variant. J. Hum. Genet. 2020, 65, 917–920. [Google Scholar] [CrossRef]
- Muoio, V.; Persson, P.B.; Sendeski, M.M. The neurovascular unit—Concept review. Acta Physiol. 2014, 210, 790–798. [Google Scholar] [CrossRef]
- Schaeffer, S.; Iadecola, C. Revisiting the neurovascular unit. Nat. Neurosci. 2021, 24, 1198–1209. [Google Scholar] [CrossRef] [PubMed]
- Nahar, K.; Lebouvier, T.; Andaloussi Mae, M.; Konzer, A.; Bergquist, J.; Zarb, Y.; Johansson, B.; Betsholtz, C.; Vanlandewijck, M. Astrocyte-microglial association and matrix composition are common events in the natural history of primary familial brain calcification. Brain Pathol. 2020, 30, 446–464. [Google Scholar] [CrossRef]
- Zarb, Y.; Weber-Stadlbauer, U.; Kirschenbaum, D.; Kindler, D.R.; Richetto, J.; Keller, D.; Rademakers, R.; Dickson, D.W.; Pasch, A.; Byzova, T.; et al. Ossified blood vessels in primary familial brain calcification elicit a neurotoxic astrocyte response. Brain 2019, 142, 885–902. [Google Scholar] [CrossRef]
- Maheshwari, U.; Huang, S.F.; Sridhar, S.; Keller, A. The Interplay Between Brain Vascular Calcification and Microglia. Front. Aging Neurosci. 2022, 14, 848495. [Google Scholar] [CrossRef] [PubMed]
- Zarb, Y.; Sridhar, S.; Nassiri, S.; Utz, S.G.; Schaffenrath, J.; Maheshwari, U.; Rushing, E.J.; Nilsson, K.P.R.; Delorenzi, M.; Colonna, M.; et al. Microglia control small vessel calcification via TREM2. Sci. Adv. 2021, 7, eabc4898. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.R.; Oliveira, M.F. Primary brain calcification in patients undergoing treatment with the biphosphanate alendronate. Sci. Rep. 2016, 6, 22961. [Google Scholar] [CrossRef] [PubMed]
- Inden, M.; Kurita, H.; Hozumi, I. Characteristics and therapeutic potential of sodium-dependent phosphate cotransporters in relation to idiopathic basal ganglia calcification. J. Pharmacol. Sci. 2022, 148, 152–155. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Gene | Locus | Mode of Inheritance | Protein | Expression | Function | Effect of Variant | Most Common Variant Type | References |
|---|---|---|---|---|---|---|---|---|
| SLC20A2 | Chr 8 | AD | Type III sodium-dependent inorganic phosphate transporter 2 (PiT2) | Ubiquitously, higher level in the brain | Uptake of inorganic phosphate (Pi) into cells | Loss of function | Missense | [3,6,41,42] |
| PDGFRB | Chr 5 | AD | Platelet-derived growth factor receptor-β (PDGFRB) | Neurons, vascular smooth muscle cells (SCMs), pericytes in the brain | Cell-surface tyrosine kinase receptors for the PDGF family, especially for homodimeric PDGF-B and PDGF-D; Essential for angiogenesis and formation of the blood–brain barrier (BBB) | Loss of function | Only missense | [2,3,7,43] |
| PDGFB | Chr 22 | AD | Platelet-derived growth factor subunit B (PDGFB) | Neurons and endothelial cells in the brain | Growth factors for mesenchymal cells; Crucial role in the proliferation and recruitment of pericytes and vascular SCMs | Loss of function | Missense | [3,8,44,45] |
| XPR1 | Chr 1 | AD | Xenotropic and polytropic retrovirus receptor 1 (XPR1) | Ubiquitously, higher level in the brain | Pi efflux from cells | Loss of function | Missense | [3,9,46] |
| MYORG | Chr 9 | AR | Myogenesis regulating glycosidase (MYORG) | Endoplasmic reticulum of the astrocytes in the brain | Member of the glycosyl hydrolase 31 family; Regulate protein glycosylation | Loss of function | Missense | [3,10] |
| JAM2 | Chr 21 | AR | Junctional-adhesion-molecule-2 (JAM2) | Endothelial cells and astrocytes in the brain | Member of the junctional adhesion molecules family; Crucial role in the regulation of cell polarity, endothelium permeability, leukocyte migration, and BBB function | Loss of function | Nonsense | [3,11,12] |
| CMPK2 | Chr 2 | AR | Uridine monophosphate-cytidine monophosphate kinase 2 (UMP-CMPK2) | Neurons and endothelial cells in the brain | Takes part in the salvage pathway for phosphorylation of dCMP, dUMP, CMP, and UMP in the mitochondria | Loss of function | Missense and start-codon loss | [13,47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-Y.; Ho, C.-J.; Lu, Y.-T.; Lin, C.-H.; Lan, M.-Y.; Tsai, M.-H. The Genetics of Primary Familial Brain Calcification: A Literature Review. Int. J. Mol. Sci. 2023, 24, 10886. https://doi.org/10.3390/ijms241310886
Chen S-Y, Ho C-J, Lu Y-T, Lin C-H, Lan M-Y, Tsai M-H. The Genetics of Primary Familial Brain Calcification: A Literature Review. International Journal of Molecular Sciences. 2023; 24(13):10886. https://doi.org/10.3390/ijms241310886
Chicago/Turabian StyleChen, Shih-Ying, Chen-Jui Ho, Yan-Ting Lu, Chih-Hsiang Lin, Min-Yu Lan, and Meng-Han Tsai. 2023. "The Genetics of Primary Familial Brain Calcification: A Literature Review" International Journal of Molecular Sciences 24, no. 13: 10886. https://doi.org/10.3390/ijms241310886
APA StyleChen, S.-Y., Ho, C.-J., Lu, Y.-T., Lin, C.-H., Lan, M.-Y., & Tsai, M.-H. (2023). The Genetics of Primary Familial Brain Calcification: A Literature Review. International Journal of Molecular Sciences, 24(13), 10886. https://doi.org/10.3390/ijms241310886