Abstract
Sleep-disordered breathing (SDB) comprises different diseases characterized by abnormal respiratory patterns during sleep including obstructive sleep apnea. SDB prevalence and impact in patients with chronic respiratory infections have been only marginally studied. The purpose of this narrative review is to report the prevalence and impact of SDB in chronic respiratory infections, including cystic fibrosis (CF), bronchiectasis and mycobacterial infections, and explore the possible pathophysiological mechanisms. Common pathophysiological mechanisms, underlying SDB onset in all chronic respiratory infections, include inflammation, which plays a central role, chronic nocturnal cough and pain, excessive production of mucous plugs, presence of obstructive and/or restrictive ventilatory impairment, upper airways involvement, and comorbidities, such as alteration of nutritional status. SDB may affect about 50% of patients with bronchiectasis. The severity of the disease, e.g., patients colonized with P. aeruginosa and frequent exacerbators, as well as comorbidities, such as chronic obstructive pulmonary disease and primary ciliary dyskinesia, may impact SDB onset. SDB may also frequently complicate the clinical course of both children and adults with CF, impacting the quality of life and disease prognosis, suggesting that their routine assessment should be incorporated into the clinical evaluation of patients from the first stages of the disease regardless of suggestive symptoms, in order to avoid late diagnosis. Finally, although the prevalence of SDB in patients with mycobacterial infections is uncertain, extrapulmonary manifestations, particularly nasopharyngeal locations, and concomitant symptoms, such as body pain and depression, may act as atypical predisposing factors for their development.
1. Introduction
Sleep-disordered breathing (SDB) comprises different diseases characterized by abnormal respiratory patterns during sleep and is often associated with cardio-pulmonary comorbidities such as chronic heart failure, pulmonary embolism and pulmonary hypertension [1,2,3]. The main causes of SDB include obstructive sleep apnea (OSA), sleep hypoventilation, central sleep apnea (CSA) and sleep-related hypoxemia. OSA is the most common sleep disorder and it affects one-third of the population aged between 30 and 70 years in Europe [4], including a huge number of people who have not received a diagnosis yet [4,5,6,7].
Chronic respiratory infections may include difficult-to-treat infections or infections that require long-term antibiotic therapy, such as tuberculosis (TB) and non-tuberculous mycobacterial pulmonary disease (NTM-PD), and also structural lung diseases that predispose to chronic bacterial colonization, such as bronchiectasis and cystic fibrosis (CF). CF is a multisystem disease whose main respiratory manifestations include chronic bacterial colonization, productive cough, progressive bronchial distortion and remodeling leading to bronchiectasis, haemoptysis, atelectasis and pneumothorax. Progressive pulmonary failure continues to be the major cause of morbidity and mortality [8]. Bronchiectasis is a condition characterized by the permanent dilation of bronchi with the destruction of elastic and muscular components of their walls. Although they are primarily a structural lung disease, we discuss bronchiectasis among chronic respiratory infections because they may frequently cause a vicious circle from impaired muco-ciliary clearance with excessive production of mucous plugs leading to chronic airway infections and inflammation with continuous airways remodeling [9]. Mycobacterial infections, including TB and NTM-PD, typically affect patients with structural lung diseases, such as bronchiectasis, patients with risk factors for immunosuppression, and, in the case of TB, patients living in highly endemic countries.
SDB has been extensively evaluated in patients with other chronic obstructive airway diseases, such as chronic obstructive pulmonary disease (COPD) and asthma, but only marginally studied in patients with chronic respiratory infections such as bronchiectasis and mycobacterial infections.
Multiple causes may lay behind this lack of knowledge; first of all, chronic respiratory infections, including NTM-PD, and bronchiectasis have long been considered orphan diseases and, therefore, research on these topics has not flourished until recent years. Secondly, the main and most studied risk factors for SDB, such as obesity, are not so common in patients with chronic respiratory infections, hiding possible concomitant diseases. Thirdly, the typical symptoms that may lead to SDB diagnosis, e.g., excessive daytime sleepiness, snoring and nocturia, are not commonly reported by patients with chronic respiratory infections.
This review aims to evaluate the current evidence on the prevalence and impact of SDB in chronic pulmonary infectious diseases, including bronchiectasis, CF, TB and NTM-PD.
2. Material and Methods
A search of relevant medical literature in the English language was conducted in Medline/PubMed and EMBASE databases including observational, interventional studies and reviews on both adults and children through January 2023. Keywords used to perform the research are reported in Table 1. Editorials, narratives, conference abstracts and pre-print publications were excluded. All studies regarding chronic respiratory infectious diseases, the objective of this review (bronchiectasis, CF and mycobacterial infections) were included. Studies reporting only on other chronic respiratory diseases whose pathogenesis is not directly related to infections, such as COPD and asthma, were excluded. Relevant abstracts and articles were searched and screened independently by three authors (PF, UZ and EP) and, when there was a discrepancy between the authors, the articles were collectively discussed and analyzed for relevance, strengths and limitations. The most relevant literature regarding the three main topics of this review (bronchiectasis, CF and mycobacterial infections) is summarized in Table 2. We included articles in Table 2 (four on CF, two on bronchiectasis and one on mycobacterial infection); three were prospective and four were retrospective observational studies.

Table 1.
Keywords used to perform the research.
Table 2.
Summary of the most relevant literature regarding the three main topics of this review (bronchiectasis, cystic fibrosis and mycobacterial infections).
3. Sleep-Disordered Breathing and Chronic Respiratory Infections: Pathophysiology and Underlying Mechanisms
Sleep-related hypoventilation is common in neuromuscular diseases and chest wall disorders due to the physiologic reduction in ventilation during sleep together with the progressive chronic challenges imposed by the underlying diseases [17,18]. Hypoventilation is first seen during rapid eye movement (REM) sleep before progressing to non-REM sleep and wakefulness [19]. Clinical presentation is nonspecific and daytime respiratory function measures poorly predict nocturnal hypoventilation. The concomitant narrowing of the upper airway induced by apneas may contribute to worsening nocturnal hypoxemia. Central events derive from the instability of the breathing pattern caused by high loop gain, which may, on the other hand, also provoke obstructive events [20,21]. OSA is characterized by a partial or complete collapse of the upper airway during sleep, resulting in reduction or cessation of airflow despite the increased respiratory effort. The repetitive collapse of the pharyngeal airway during sleep leads to impaired gas exchange and intermittent oxygen desaturations that result in arousal from sleep. Intermittent and sustained nocturnal hypoxemia, particularly with concomitant hypercapnia, typical of OSA, CSA and sleep hypoventilation activates the sympathetic nervous system, being the major contributor to cardiovascular comorbidity of SDB [22]. These surges in sympathetic activity also result in ―the release of inflammatory mediators, lipolysis, and worsened insulin resistance, especially in OSA [23].
Mechanisms that may justify the coexistence of SDB, especially OSA, and chronic respiratory infections leading to bronchiectasis are many. In particular, the synergic increases in proinflammatory stimuli and anatomical alterations of the upper airway might be the subjects of a cross-talk mechanism responsible for a bidirectional worsening of the two diseases, Figure 1. An over-sensitive ventilatory control system—or loop gain―and altered arousal threshold represent a predisposing condition for SDB in chronic infectious diseases [24,25,26,27].
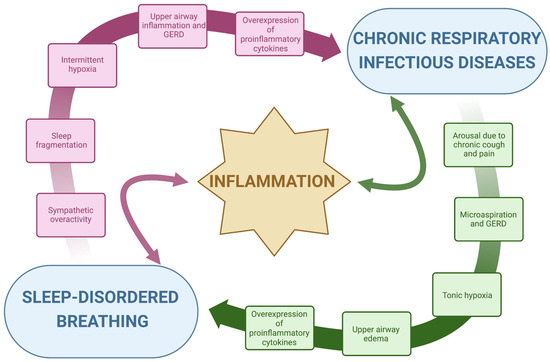
Figure 1.
Inflammation cross-talk between chronic respiratory infectious diseases and sleep-disordered breathing.
- A.
- Inflammation: The repetitive collapse of the pharyngeal airway characteristic of OSA leads to intermittent oxygen desaturation, sleep fragmentation and the consequent activation of the sympathetic nervous system, which is the major contributor to the release of systemic inflammatory mediators, Figure 1 [28,29]. Thus, intermittent hypoxia has been largely linked to major pro-inflammatory cytokines, such as tumor necrosis factor α (TNF-α) and interleukin 6 (IL-6), which constitute the classical prototypes of the large spectrum of systemic inflammation [29]. The subsequent cytokine-mediated inflammatory cascade, coupled with mechanical lung injury, damages the lungs and may worsen several conditions, including chronic respiratory infections [30]. Oxidative stress, such as the structural and functional alteration induced by reactive oxygen species, in response to chronic and intermittent hypoxia, is associated with airway damage [31,32]. In bronchiectasis, chronic bronchial infection and inflammation interact with each other and are responsible for progressive lung damage [33]. Oxidative stress and hypoxia in the airway are induced by the consumption of nutrients by inflammatory cells and bacteria and by a reduced supply of oxygenated blood to damaged lung segments [32]. The overexpression of pro-inflammatory cytokines due to SDB, especially in OSA, might accelerate this process precipitating the evolution of chronic respiratory diseases. On the other hand, the persistent inflammation induced by hypoxia, oxidative stress and chronic infections might predispose to SDB by increasing local phlogosis, gastroesophageal reflux disease (GERD) and, thus, upper airway edema. Upper airway inflammation and edema might increase pharyngeal collapsibility, as it will be described subsequentially. Given these premises, inflammation represents the subject of a bidirectional link between SDB and chronic respiratory infectious diseases, Figure 1. The disease-related chronic overexpression of inflammatory cytokines is enhanced in a vicious circle, with a consequent potential worsening of general clinical conditions.
- B.
- Anatomy, upper airway edema and local inflammation: The occurrence of upper airway obstruction during sleep reflects an interplay between the removal of the wakefulness drive (which helps to maintain airway patency) and an individual anatomical predisposition with susceptibility to collapse. Pharyngeal muscle relaxation during sleep and lack of sufficient reactivation are key primary pathophysiological events leading to OSA [34]. Interstitial fluid accumulation in the upper part of the body during the night decreases the pharyngeal size and increases pharyngeal resistance and upper airway collapsibility in predisposed individuals [35,36]. A narrow upper airway importantly contributes to the development of OSA, typically worsened by a fat deposit in the parapharyngeal fat pads and pharyngeal muscles, obesity being one of the major risk factors for OSA, or by edema of the upper airway induced by local acute or chronic inflammation [28,37]. In patients with OSA, upper airway tissue is characterized by subepithelial edema and excessive inflammatory cell infiltration [38,39]. Chronic respiratory infectious diseases are characterized by chronic airway inflammation, which also involves the upper airways, GERD and microaspirations, especially at night time [40,41,42]. Acid regurgitation in the upper airway might contribute to the further narrowing of the pharyngeal region by local inflammation. In turn, OSA swings in intrathoracic pressure during apneas increase the pressure gradient between the esophagus and the stomach displacing the gastric contents into the esophagus, determining GERD. This produces a further pharyngeal spasm in patients with OSA and might decrease pharyngeal dilator muscle responsiveness by reducing specific receptors’ sensibility. GERD can also lead to bronchoconstriction or coughing in patients with lung diseases, by causing microaspiration. Additionally, OSA can also affect airway immunity leading to an increased propensity for respiratory tract infection-mediated exacerbations that can progress underlying chronic airway disease [43,44]. Indeed, the presence of upper airway symptoms was shown to increase disease duration and the exacerbation rate in patients with bronchiectasis [45]. Local upper airway inflammation related to chronic respiratory infections might therefore increase pharyngeal collapsibility, inducing pharyngeal narrowing in predisposed individuals.
- C.
- Ventilatory drive instability and loop gain: respiration regulatory disturbances are essential in SDB pathogenesis, as respiratory control plays an essential role in maintaining stable respiration during sleep in healthy humans. The respiratory control system sensitivity is modulated through a negative feedback mechanism called loop gain [46,47,48]. A high loop gain is a marker of breathing instability and determines an exaggerated increase in ventilation in response to minimal changes in blood gas tension. Changes in respiration consequent to obstructive events (reduction in ventilation) or to arousals (increase in ventilation) evoke an exaggerated respiratory response when the loop gain of the subject is high. This response becomes a disturbance itself and will propagate breathing instability, and thus apneas and hypopneas, in predisposed individuals [49]. The cardinal symptom of chronic respiratory infections is chronic productive cough [50,51,52]. Nocturnal cough arouses the subject determining a sudden increase in respiratory rate and carbon dioxide changes. Accordingly, with the loop gain of the subject, the ventilatory drive may induce an increased response that will propagate respiratory instability and respiratory events in predisposed individuals [24]. Given these premises, cough and pain might be stimuli for SDB propagation in subjects with a high loop gain.
- D.
- Arousals and arousal threshold: Arousals contribute to sleep fragmentation and poor sleep quality in subjects with SDB and chronic respiratory diseases and indirectly worsen the predisposition to develop sleep apnea. As mentioned above, recurrent abrupt arousals during sleep may contribute to the exaggerated post-event ventilatory response, reiterating respiratory instability and, thus, SDB [22,53]. The respiratory arousal threshold is the level of inspiratory mechanical effort required to wake up an individual in response to the narrowing of the upper airway during sleep. Although it has been postulated that a low arousal threshold may contribute to the development of OSA in predisposed subjects [24,54], delaying arousals in subjects with poor pharyngeal muscle responsiveness would increase the risk of severe overnight hypoxemia. Sustained isocapnic hypoxia increases the respiratory arousal threshold [55]. Increased arousal threshold together with sustained nocturnal hypoxemia may further impair the normal defense mechanisms that operate to minimize the result of abnormal breathing and gas exchange during sleep. This may have implications for disorders characterized by sustained nocturnal hypoxia, such as chronic respiratory infections, worsening the baseline hypoxic condition.
The main pathophysiological mechanisms causing SDB in chronic respiratory infections are summarized in Figure 2.
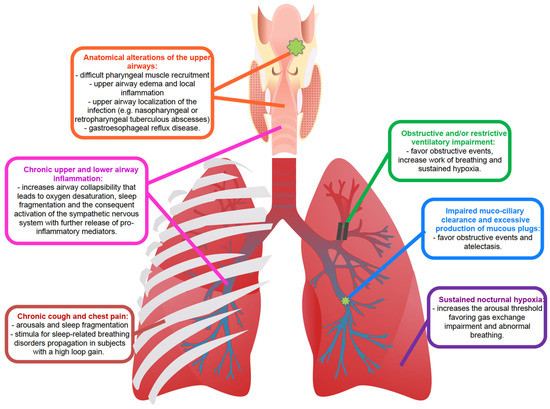
Figure 2.
Summary of the main pathophysiological mechanisms causing SDB in chronic respiratory infections.
4. Sleep-Disordered Breathing and Bronchiectasis
Bronchiectasis is an anatomical alteration with a permanent enlargement of part of the airways. Many different causes may contribute to the development of bronchiectasis, including prior pulmonary infections, such as tuberculosis, autoimmune diseases and impaired host defenses, such as primary ciliary dyskinesia (PCD) or immunodeficiencies. CF-associated bronchiectasis for this review will be addressed in a specific paragraph.
It has been shown that patients with bronchiectasis have multiple risk factors for SDB, such as chronic inflammation and ventilatory impairment due to obstructive and/or restrictive patterns and chronic secretions, caused by impaired muco-ciliary clearance and by excessive production of mucous plugs [56,57]. Only a few studies have thoroughly investigated the prevalence of SDB, particularly OSA, in patients with bronchiectasis [10,11]. Two studies conducted in Brazil and Turkey reported the results of polysomnography (PSG) in 49 and 43 patients with bronchiectasis, respectively. Prevalence of OSA ranged between 41% and 56% and, in more than half cases in both studies, it was of mild severity (apnea-hypopnea index (AHI) 5–15). Risk factors for the presence of OSA were older age, male gender, larger neck circumference and P. aeruginosa colonization [10,11]. Contrary to what was expected, body mass index (BMI), pulmonary functional parameters and the number of prior exacerbations did not differ between patients with or without OSA. Smoking history was not evaluated in these studies, probably because pathophysiological mechanisms for OSA in patients with bronchiectasis may at least in part be different from those of the general population. Recognized markers of bronchiectasis severity, such as the number of exacerbations per year ≥ 3, were associated with longer snoring periods, worse oxygen saturation (SpO2) nadir and higher total sleep time with SpO2 < 90% [10]. To our knowledge, literature is lacking regarding the impact of treating SDB in these patients and whether airway-clearance techniques and pulmonary rehabilitation may have a positive effect on OSA. Regarding diagnosis, typical symptoms suggestive of OSA may not be present in patients with bronchiectasis. In the study by Faria Junior et al., daytime levels of sleepiness evaluated using the Epworth sleepiness scale (ESS) did not differ between patients with and without OSA [11]. Similarly, comparing subjects with bronchiectasis with and without OSA, Borekci et al., did not observe any difference regarding excessive daytime sleepiness and snoring [10]. These findings suggest that patients with bronchiectasis may require screening for OSA regardless of typical risk factors and symptoms.
The impact of sleep disturbances on the quality of life in both children and adults with bronchiectasis was also investigated through questionnaires [58,59]. Gao et al., applied the Pittsburgh Sleep Quality Index (PSQI), ESS and St. George Respiratory Questionnaire in 144 adults with bronchiectasis and observed that they had a higher prevalence of sleep disturbances (based on the PSQI score > 5), but no difference in daytime sleepiness (based on the ESS score > 10) compared to healthy subjects [58]. Furthermore, compared to patients without sleep disturbances, those with SDB according to the questionnaire response had a more impaired quality of life. Erdem et al., collected the PSQI and the Pediatric Sleep Questionnaire in 54 children with bronchiectasis and age-matched controls [59]. The prevalence of SDB and poor sleep quality was higher in patients with bronchiectasis compared to controls (22 vs. 9% and 37 vs. 17%, respectively). Moreover, patients with chronic symptoms such as sputum production, snoring and wheezing, and those with worse high-resolution computed tomography involvement had poorer sleep scores [59]. Both the studies by Gao et al., and Erdem et al., showed that sleep quality was impaired in a non-negligible percentage of patients with bronchiectasis, regardless of age [59]. However, neither of the two studies performed PSG to definitively confirm the presence of SDB.
Bronchiectasis may also complicate other diseases, such as COPD, and increase the prevalence of OSA. A recent observational study by Yang et al., studied the prevalence of bronchiectasis, with chest computed tomography, and the presence of OSA, through nocturnal PSG, in 124 consecutive patients with COPD, mostly of severe entity [60]. Bronchiectasis were significantly more frequent in patients with COPD-OSA overlap syndrome than in those with COPD without OSA (43 vs. 19%) Furthermore, the co-presence of bronchiectasis and OSA in COPD patients was related to more severe nocturnal hypoxia, evaluated through the percentage of time spent with SpO2 below 90%, and higher systemic inflammation, according to through C-reactive protein levels [60].
Finally, the prevalence of SDB has also been studied in patients with primary ciliary dyskinesia (PCD) a possible cause of both bronchiectasis and chronic rhinosinusitis. Two studies conducted in Italy and Turkey compared children with PCD (16 in the Italian and 29 in the Turkish study) with healthy controls and found a higher rate of SDB and poorer sleep quality in those with PCD [61,62]. In particular, the bronchiectasis severity score was negatively associated with SpO2 in both studies.
In conclusion, according to the limited data available to date, SDB may affect about 50% of patients with bronchiectasis, although they may have been under-reported in many studies. The severity of the disease, e.g., patients colonized with P. aeruginosa and frequent exacerbators, as well as comorbidities, such as COPD and PCD, may impact SDB onset.
5. Sleep-Disordered Breathing and Cystic Fibrosis
SDB has been extensively studied in children and adolescents with CF [63]. Differently, studies on adults affected by CF have been limited due to the small sample sizes and lack of diversity [64]. The main sleep abnormalities observed in both adult and pediatric patients with CF range from nocturnal hypoxemia and/or hypercapnia to increased respiratory rate during sleep and OSA [65]. The pathogenesis of SDB in CF resembles that of bronchiectasis, where chronic infection and inflammation together with accumulation of mucous plugs play a pivotal role.
Different studies have shown that SDB, including OSA, may occur in patients with CF even before daytime clinical manifestations, suggesting that early screening is important in this population [65,66]. SDB and nocturnal episodes of oxygen desaturations have also been described in infants with CF under 3 years of age with mild airway inflammation (rhinitis, cough, red throat) [67].
Furthermore, different from patients with bronchiectasis and mycobacterial infections, patients with CF often manifest poor sleep quality with frequent awakenings and daytime sleepiness, and such disturbances are more frequent with the progression of the disease [68]. Despite this, SDB prevalence is still under-recognized in this population of patients and may impact disease outcomes [69]. As an example, in CF patients with a severe disease complicated by pulmonary hypertension and right ventricular failure, chronic nocturnal hypoxia secondary to untreated SDB may worsen the disease leading to a poor prognosis [70].
Multiple studies have explored the possibility that markers of CF severity, including lung function, may predict SDB presence and severity with conflicting results [13,15,16]. On one hand, Shakkottai et al., in a retrospective analysis of patients with CF did not find any association between OSA detected by PSG and clinical signs of CF severity, suggesting the need for routine PSG to screen for sleep disorders [13,15]. On the other hand, Lumertz et al., found that forced expiratory volume in the 1st second, a marker of obstructive impairment at spirometry, was directly correlated with mean sleep SpO2 and negatively correlated with sleep peak end-tidal carbon dioxide [16].
A recent meta-analysis by Pedrada De Sousa et al., included 6 studies to investigate the prevalence of OSA in children and adolescents with CF and preserved or mildly impaired lung function. The pooled prevalence, considering an obstructive AHI > 2 per hour, was 52%, regardless of lung function impairment [71].
The available literature on adult patients with CF reported a wide range of OSA prevalence. In a cross-sectional study, Perin et al., compared 51 stable adults with CF to 25 age-matched controls to evaluate sleep parameters and to determine predictors of nocturnal desaturation. In this study, the estimated prevalence of OSA in adults with CF was 3.9%, which is less than the general population [64,72]. Similar results were reported by Milross et al., while Welsner et al., reported a higher prevalence (40%) [73,74]. These conflicting results suggest that the prevalence of OSA is still unknown and may be greatly underestimated [75,76].
In contrast, results about the incidence of nocturnal hypoxia in adult patients with CF are more consistent. Perin et al., showed that the incidence of nocturnal desaturation was more common in adult patients with CF than controls (29.4% vs. 0%; p < 0.001) and the best predictor for sleep desaturation was the awake resting SpO2 [64]. The study by Milross et al., reported a similar incidence (25%) of nocturnal desaturation, also describing a correlation between the occurrence of nocturnal hypoxia and the severity of lung involvement in CF. [70].
SDB in children and adults with CF also deeply affects daytime function and quality of life, in fact, the presence and severity of SDB have been inversely associated with exercise capacity and daily physical activity levels [14,64,77]. Moreover, a direct link was detected between nocturnal hypoxemia and exercise intolerance, and between sleep architecture disorders and sedentary physical activity levels [14].
Furthermore, not only respiratory parameters such as lung function but also other systemic parameters, such as nutritional status (overweight/obesity), have been described as major determinants of OSA [15,78]. The development of OSA in patients with CF was not only associated with pulmonary manifestations of the disease but also with the presence of upper airway obstruction caused by chronic rhinosinusitis, nasal polyposis and tonsillar hypertrophy [79].
Supplemental oxygen and non-invasive ventilation (NIV) have been applied in both adults and children with CF and SDB and are considered to be effective in the short term. However, long-term data are still needed [65,80].
To prevent hypoventilation and nocturnal hypoxia, Young et al., examined the role of NIV in adults with CF [81]. This study compared the use of nocturnal NIV to low-flow oxygen and to room air (as a placebo) over 6 weeks in a randomized, placebo-controlled, crossover trial. In comparison to room air, NIV improved chest symptoms (evaluated with the CF Quality of Life Questionnaire), exertional dyspnea and peak exercise capacity in patients with stable CF and awake hypercapnia [81]. Similarly to the aforementioned study, Wadsworth et al., showed the improvement of lung function and the attenuation of hypercapnia in adults with CF using nocturnal NIV [82].
In conclusion, routine checks for SDB should be incorporated into the clinical evaluation of patients with CF from the first stages of the disease. Suggestive symptoms, such as daytime sleepiness, and lung disease severity may lack sensitivity and lead to late diagnosis.
6. Sleep-Disordered Breathing and Mycobacterial Infections
TB is an infectious disease caused by Mycobacterium Tuberculosis Complex (e.g., M. tuberculosis, M. Africanum and M. bovis). It mainly involves the lungs, but in one-fifth of cases can also present with extrapulmonary manifestations. It was recently estimated that about 22% of the world population is infected, with a latent or active form, with M. tuberculosis [83]. Inflammation and proinflammatory mediators strongly impact the severity and progression of the disease [84,85].
Non-tuberculous mycobacterial (NTM) infections are caused by mycobacterial species other than Mycobacterium Tuberculosis Complex. NTM infection mainly involves the lung with rare extrapulmonary manifestations. The incidence worldwide is lower than TB, but it is increasing, particularly in high-income countries [86]. In fact, in the USA, from 2008 to 2015, the annual incidence of NTM-PD increased from 3.1 to 4.7 per 100,000 person-years [87]. Treatment of NTM infection is particularly challenging with high rates of NTM isolation relapse or reinfection (up to 50% of patients who completed treatment), despite an initially successful antibiotic treatment [88]. Furthermore, specific antimicrobial therapy requires at least a 3-to-4 drug regimen administered for at least 15 to 18 months [88]. These above-mentioned characteristics make the NTM-PD effectively a chronic infection.
The prevalence of SDB in mycobacterial infections, as well as the mutual impact of SDB on mycobacterial infection and vice versa, have only scarcely been investigated and the few studies available show discordant results [89,90]. In a recent review, Devassy et al., report that poor sleep quality and restless leg syndrome were higher in patients with TB compared to the general population [89]. Authors also speculated that symptoms associated with SDB may exacerbate chronic infections like TB by impairing immune regulation [89]. A population-based study by Lee et al., evaluated the incidence of TB in patients with OSA using data from the Taiwan National Health Insurance database [90]. They compared the incidence of TB between 6135 patients with OSA and 184,050 control subjects without OSA [90]. The prevalence of TB was significantly higher in the control group (0.56%) than in patients with OSA (0.33%), suggesting that the incidence of TB in patients with OSA is lower than in those without.
Extrapulmonary manifestations of TB may favor SDB onset when localized in the upper airway region. OSA was observed in two patients with nasopharyngeal TB and tuberculous retropharyngeal abscess [91,92]. Considering that nasopharyngeal TB affects 1.9% of patients with pulmonary TB, OSA might complicate the clinical course of these patients. Although rare, cervical masses were reported in 59% of patients with nasopharyngeal tuberculosis [93]. The obstruction of the nasopharynx increases the calibre and resistance of the upper airway, lowering the airflow and eventually causing snoring and OSA.
SDB was also evaluated in patients with sequelae of pulmonary TB, including pleural thickening, prior pulmonary resection and/or atelectasis, fibrosis, bronchiectasis, cavity formation and compensatory emphysematous changes [94]. In these cases, the development of SDB is not directly related to active infection or inflammation, but to their consequences leading to a restrictive ventilatory impairment and, in some cases, chest wall diseases. Sakuma et al., in 1997 reported the characteristics of sleep oxygen desaturations in 38 patients with TB sequelae in comparison to 40 patients with COPD [94]. The baseline nocturnal SpO2 was similar between the two groups, however, the lowest sleep SpO2 was more profound in the TB sequelae group. Most of the patients in the study were treated before the 1960s with thoracoplasty because at the time there was hardly any effective antimicrobial regimen for TB [94]. Therefore, possible reasons for the deeper nocturnal desaturations were mechanical disadvantages (e.g., pulmonary fibrosis and loss of lung volume) secondary to thoracoplasty. However, nowadays the surgical approach for TB is rare since the first-line therapy for TB is multiple antibiotic regimens with lower possibilities of developing permanent structural sequelae [94].
Finally, only one study investigated the presence of SDB in NTM-PD in association with other symptoms, such as depression [95]. In a cross-sectional retrospective study, Matsumura et al., analyzed the prevalence of depressive symptoms and the factors that influenced their development in 114 patients with NTM-PD [95]. The authors found that 32.5% of patients reported depressive symptoms, in which an important role was played by disease duration and sleep disturbances.
In conclusion, several speculations have been made about the possible association between SDB and mycobacterial infections. However, the few studies available are inconclusive regarding the prevalence of SDB. Furthermore, the possible role of extrapulmonary manifestations of the infection (e.g., nasopharyngeal locations) and concomitant symptoms, such as depression, have only been studied and reported anecdotally.
Given that this topic is not supported by high-quality literature and that the few studies available did not implement in their methodology complete sleep studies, we cannot draw any conclusion other than to indicate the need for high-quality prospective studies.
7. Consequences of Coexistence of SDB and Chronic Respiratory Infectious Diseases
- A.
- Misdiagnosis: obesity is an important risk factor for OSA since OSA incidence is directly related to increased BMI [96]. Fat deposits in the upper respiratory tract narrow the airway, leading initially to snoring and, subsequently, resulting in sleep apnea with weight gain and worsening of the obstruction. Patients with chronic respiratory infections are generally normal weight or underweight due to persistent chronic infection and inflammation. The absence of snoring, as a reported symptom, and the absence of a typical OSA patient phenotype might reduce the suspicion of clinicians leading to the underestimation of SDB. Moreover, unexplained chronic cough has been reported in patients who snore and who have SDB and, as previously explained, it is also one of the peculiar symptoms of CF, NTM-PD and bronchiectasis [97]. In certain cases, chronic cough can be the sole manifestation of OSA, when specifically investigated by sleep clinicians during a visit [98]. In patients known for having respiratory diseases, such as bronchiectasis or chronic respiratory infections, cough might be explained by these underlying diseases leading to an underestimation of possible OSA symptoms and determining a misdiagnosis [15].
- B.
- Hypoxia: hypoxia has deleterious effects on the cardiovascular system, the central nervous system and all the organs of the human body [99]. Many chronic respiratory diseases, including COPD, interstitial lung diseases and chronic respiratory infectious diseases, determine normobaric hypoxia based on different pathophysiological mechanisms [99]. Susceptible subjects with chronic respiratory comorbidities show a lower SpO2 than healthy subjects, especially during night-time. Lung infections, such as those mediated by mycobacteria, and bronchiectasis are both characterized by ventilation/perfusion mismatch due to regional lack of ventilation with consequent hypoxia [31]. In the airways of patients with CF, chronic hypoxia is also driven by impaired ventilation due to airway mucus obstruction [100]. As a complication of infections, atelectasis further reduces gas exchanges. The presence of SDB, particularly OSA and CSA, can further worsen tonic hypoxia by adding intermittent episodes of oxygen reduction [11,13,14,101,102]. Thus, CF subjects with SDB had lower SpO2 and each unit increase in AHI was associated with a decline in SpO2 nadir [13]. Oxidative stress and inflammatory pathways induced by intermittent hypoxia can be compounded by inflammation due to persistent infections, airway chronic damage and gas exchange alterations due to chronic lung diseases [44,103]. The high rate of underdiagnosed – and undertreated—OSA in conditions of chronic hypoxia such as in chronic respiratory infectious disease, might act as a cofactor in worsening patients’ nocturnal hypoxia and, thus, general clinical conditions. The overlap of the two diseases represents a risk factor itself for exacerbations and an increased susceptibility to worse respiratory outcomes [14,16].
- C.
- Sleep fragmentation: cough and, secondarily, pain are hallmarks of chronic respiratory infections and when presenting at nighttime, are responsible for waking the patient and inducing sleep fragmentation. As a consequent mechanism, sleep fragmentation has effects on cognitive function, and alterations in the neuroendocrine, immune and inflammatory systems [104]. Sleep fragmentation and deterioration of sleep quality, typical of SDB, further complicate the fatigue and physical exhaustion often experienced by patients with chronic lung diseases [12]. Poor sleep quality will also impact the physiological beneficial effects on the immune system attributable to efficient sleep [105]. Moreover, poor sleep has been shown to increase the perception of pain [106]. Mori and coauthors reported worse pain experiences in subjects with poorer sleep quality [12]. OSA-related nocturnal hypoxemia, sleep fragmentation, and systemic inflammation impact pain perception by influencing the anti-nociceptive mechanism and aggravating both chronic and acute pain [107]. Worsening sleep fragmentation and the co-existence of SDB on top of a chronic respiratory infectious disease might increase systemic inflammation and pain perception aggravating the general clinical condition and patient’s quality of life [12,14,16,108].
8. Limitations
This narrative review has some limitations beyond those inherent in the narrative review, which is the weakest review type. First of all, since the literature on the prevalence and impact of SDB in chronic respiratory infectious diseases is very limited and heterogeneous it was impossible to conduct a methodologically superior review, such as a systematic review. Secondly, given the weak evidence available we specified that some speculations proposed by the authors of this review require stronger research to be confirmed. Thirdly, we did not collect and report information on several studies (i) identified from the research, (ii) screened, and (iii) excluded from the review and this may have introduced potential biases from incomplete reporting. Finally, we did not perform a formal assessment of the quality of the studies.
9. Conclusions
Chronic infectious respiratory diseases and SDB might coexist, aggravating the outcome and the subject’s quality of life due to local and systemic inflammation, intermittent hypoxia, sometimes superimposed to chronic hypoxia, and sleep fragmentation. Disrupted sleep and cough might worsen or induce OSA in susceptible patients by increasing upper airway edema, by determining ventilatory instability, or due to a potentially infectious disease localization in the upper airways, such as nasopharyngeal TB. Proinflammatory stimuli triggered by chronic respiratory diseases and enhanced by over-imposed SDB might worsen the prognosis and patient’s quality of life. Although, in the authors’ opinion, the cross-talk link between the diseases is evident, unfortunately, very few studies thoroughly evaluated this subject.
The limited literature available in this field might be related to the difficult identification of patients at risk of SDB with possible misdiagnosis caused by a lack of common known symptoms typical of OSA. For patients with chronic respiratory disorders, the available evidence suggests that the prompt recognition and treatment of SDB improves their quality of life and may also alter the course of the disease. Since the pathophysiology and the outcomes of the diseases are strictly related, there is now a need for epidemiologic and prognostic studies to better understand the prevalence, risk factors and impact of the superimposition of SDB on chronic respiratory infections. Research should focus first on the epidemiological distribution of SDB among patients with respiratory infectious diseases. Furthermore, the clinical impact of the coexistence of the diseases needs to be confirmed in observational and prognostic studies, also to confirm the pathophysiologic mechanisms underlying the diseases. Researchers also need to focus on the implication of interventions reducing SDB in populations affected by chronic lung infections. The results of these studies will help to drive clinicians to the best diagnostic and therapeutic approach for these patients. According to CF and bronchiectasis prevalence, this might be of particular relevance in the pediatric population.
Author Contributions
Conceptualization, P.F., U.Z., A.M. and E.P.; methodology, P.F., U.Z. and E.P.; investigation, P.F., U.Z. and E.P.; data curation, P.F., U.Z., A.M. and E.P.; writing—original draft preparation, P.F., U.Z., A.M. and E.P.; writing—review and editing, all authors; supervision, F.L., C.L. and G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AHI | apnea-hypopnea index |
| BMI | body mass index |
| CF | cystic fibrosis |
| COPD | chronic obstructive pulmonary disease |
| CSA | central sleep apnea |
| ESS | Epworth sleepiness scale |
| GERD | gastroesophageal reflux disease |
| NIV | non-invasive ventilation |
| NTM | non-tuberculous mycobacterial |
| NTM-PD | non-tuberculous mycobacterial pulmonary disease |
| OSA | obstructive sleep |
| PCD | primary ciliary dyskinesia |
| PSQI | Pittsburgh Sleep Quality Index |
| REM | rapid eye movement |
| SDB | sleep-disordered breathing |
| SpO2 | oxygen saturation |
| TB | tuberculosis |
References
- García-Ortega, A.; Mañas, E.; López-Reyes, R.; Selma, M.J.; García-Sánchez, A.; Oscullo, G.; Jiménez, D.; Martínez-García, M.Á. Obstructive Sleep Apnoea and Venous Thromboembolism: Pathophysiological Links and Clinical Implications. Eur. Respir. J. 2019, 53, 1800893. [Google Scholar] [CrossRef]
- Lyons, O.D.; Bradley, T.D. Heart Failure and Sleep Apnea. Can. J. Cardiol. 2015, 31, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.M. Complications and Consequences of Obstructive Sleep Apnea. Curr. Opin. Pulm. Med. 2000, 6, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea: A Literature-Based Analysis. Lancet. Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef]
- Young, T.; Palta, M.; Dempsey, J.; Peppard, P.E.; Nieto, F.J.; Hla, K.M. Burden of Sleep Apnea: Rationale, Design, and Major Findings of the Wisconsin Sleep Cohort Study. WMJ 2009, 108, 246–249. [Google Scholar] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of Sleep-Disordered Breathing in the General Population: The HypnoLaus Study. Lancet. Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Dickinson, K.M.; Collaco, J.M. Cystic Fibrosis. Pediatr. Rev. 2021, 42, 55–67. [Google Scholar] [CrossRef]
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society Guidelines for the Management of Adult Bronchiectasis. Eur. Respir. J. 2017, 50, 1700629. [Google Scholar] [CrossRef]
- Borekci, S.; Sekibag, Y.; Harbiyeli, D.O.; Musellim, B. The Frequency of Obstructive Sleep Apnea in Patients with Non-Cystic Fibrosis Bronchiectasis. Turkish Thorac. J. 2021, 22, 333–338. [Google Scholar] [CrossRef]
- Júnior, N.S.F.; Urbano, J.J.; Santos, I.R.; Silva, A.S.; Perez, E.A.; Souza, H.; Nascimento, O.A.; Jardim, J.R.; Insalaco, G.; Oliveira, L.V.F.; et al. Evaluation of Obstructive Sleep Apnea in Non-Cystic Fibrosis Bronchiectasis: A Cross-Sectional Study. PLoS ONE 2017, 12, e0185413. [Google Scholar] [CrossRef]
- Mori, K.; Tabusadani, M.; Yamane, K.; Takao, S.; Kuroyama, Y.; Matsumura, Y.; Ono, K.; Kawahara, K.; Omatsu, S.; Fujiwara, K.; et al. Effects of Pain on Depression, Sleep, Exercise Tolerance, and Quality of Life in Patients with Nontuberculous Mycobacterial Pulmonary Disease. Medicine 2021, 100, e26249. [Google Scholar] [CrossRef]
- Shakkottai, A.; Nasr, S.Z.; Hassan, F.; Irani, S.; O’Brien, L.M.; Chervin, R.D. Sleep-Disordered Breathing in Cystic Fibrosis. Sleep Med. 2020, 74, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, R.R.B.; Liberato, F.M.G.; de Freitas Coelho, P.; Vidal, P.D.R.; de Carvalho, R.B.C.O.; Donadio, M.V.F. Sleep-Disordered Breathing and Markers of Morbidity in Children and Adolescents with Cystic Fibrosis. Pediatr. Pulmonol. 2020, 55, 1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Shakkottai, A.; Irani, S.; Nasr, S.Z.; O’Brien, L.M.; Chervin, R.D. Risk Factors for Obstructive Sleep Apnea in Cystic Fibrosis. Pediatr. Pulmonol. 2022, 57, 926–934. [Google Scholar] [CrossRef]
- Lumertz, M.S.; Pinto, L.A. Sleep-Disordered Breathing in Cystic Fibrosis Pediatric Subjects. Sleep Sci. 2019, 12, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Piper, A.J.; Grunstein, R.R. Obesity Hypoventilation Syndrome: Mechanisms and Management. Am. J. Respir. Crit. Care Med. 2011, 183, 292–298. [Google Scholar] [CrossRef]
- Ward, S.; Chatwin, M.; Heather, S.; Simonds, A.K. Randomised Controlled Trial of Non-Invasive Ventilation (NIV) for Nocturnal Hypoventilation in Neuromuscular and Chest Wall Disease Patients with Daytime Normocapnia. Thorax 2005, 60, 1019–1024. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Hansson, D.; Schiza, S.; Grote, L. Sleep in Chronic Respiratory Disease: COPD and Hypoventilation Disorders. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2019, 28, 190064. [Google Scholar] [CrossRef]
- Dempsey, J.A.; Xie, A.; Patz, D.S.; Wang, D. Physiology in Medicine: Obstructive Sleep Apnea Pathogenesis and Treatment—Considerations beyond Airway Anatomy. J. Appl. Physiol. 2014, 116, 3–12. [Google Scholar] [CrossRef]
- Malhotra, A.; Owens, R.L. What Is Central Sleep Apnea? Respir. Care 2010, 55, 1168–1178. [Google Scholar]
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of Sleep Apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-de-la-Torre, M.; Campos-Rodriguez, F.; Barbé, F. Obstructive Sleep Apnoea and Cardiovascular Disease. Lancet. Respir. Med. 2013, 1, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining Phenotypic Causes of Obstructive Sleep Apnea. Identification of Novel Therapeutic Targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Wellman, A.; Eckert, D.J.; Jordan, A.S.; Edwards, B.A.; Passaglia, C.L.; Jackson, A.C.; Gautam, S.; Owens, R.L.; Malhotra, A.; White, D.P. A Method for Measuring and Modeling the Physiological Traits Causing Obstructive Sleep Apnea. J. Appl. Physiol. 2011, 110, 1627–1637. [Google Scholar] [CrossRef] [PubMed]
- Wellman, A.; Edwards, B.A.; Sands, S.A.; Owens, R.L.; Nemati, S.; Butler, J.; Passaglia, C.L.; Jackson, A.C.; Malhotra, A.; White, D.P. A Simplified Method for Determining Phenotypic Traits in Patients with Obstructive Sleep Apnea. J. Appl. Physiol. 2013, 114, 911–922. [Google Scholar] [CrossRef] [PubMed]
- Younes, M. Contributions of Upper Airway Mechanics and Control Mechanisms to Severity of Obstructive Apnea. Am. J. Respir. Crit. Care Med. 2003, 168, 645–658. [Google Scholar] [CrossRef] [PubMed]
- Vicente, E.; Marin, J.M.; Carrizo, S.J.; Osuna, C.S.; González, R.; Marin-Oto, M.; Forner, M.; Vicente, P.; Cubero, P.; Gil, A.V.; et al. Upper Airway and Systemic Inflammation in Obstructive Sleep Apnoea. Eur. Respir. J. 2016, 48, 1108–1117. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Gozal, D. Obstructive Sleep Apnea and Inflammation: Proof of Concept Based on Two Illustrative Cytokines. Int. J. Mol. Sci. 2019, 20, 459. [Google Scholar] [CrossRef]
- Goldbart, A.D.; Krishna, J.; Li, R.C.; Serpero, L.D.; Gozal, D. Inflammatory Mediators in Exhaled Breath Condensate of Children with Obstructive Sleep Apnea Syndrome. Chest 2006, 130, 143–148. [Google Scholar] [CrossRef]
- Ravimohan, S.; Kornfeld, H.; Weissman, D.; Bisson, G.P. Tuberculosis and Lung Damage: From Epidemiology to Pathophysiology. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2018, 27, 170077. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Chang, A.B.; Chotirmall, S.H.; Dhar, R.; McShane, P.J. Bronchiectasis. Nat. Rev. Dis. Prim. 2018, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Fuschillo, S.; De Felice, A.; Balzano, G. Mucosal Inflammation in Idiopathic Bronchiectasis: Cellular and Molecular Mechanisms. Eur. Respir. J. 2008, 31, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Horner, R.L.; Hughes, S.W.; Malhotra, A. State-Dependent and Reflex Drives to the Upper Airway: Basic Physiology with Clinical Implications. J. Appl. Physiol. 2014, 116, 325–336. [Google Scholar] [CrossRef]
- Perger, E.; Jutant, E.-M.; Redolfi, S. Targeting Volume Overload and Overnight Rostral Fluid Shift: A New Perspective to Treat Sleep Apnea. Sleep Med. Rev. 2018, 42, 160–170. [Google Scholar] [CrossRef]
- Redolfi, S.; Yumino, D.; Ruttanaumpawan, P.; Yau, B.; Su, M.-C.; Lam, J.; Bradley, T.D. Relationship between Overnight Rostral Fluid Shift and Obstructive Sleep Apnea in Nonobese Men. Am. J. Respir. Crit. Care Med. 2009, 179, 241–246. [Google Scholar] [CrossRef]
- Kim, A.M.; Keenan, B.T.; Jackson, N.; Chan, E.L.; Staley, B.; Poptani, H.; Torigian, D.A.; Pack, A.I.; Schwab, R.J. Tongue Fat and Its Relationship to Obstructive Sleep Apnea. Sleep 2014, 37, 1639–1648. [Google Scholar] [CrossRef]
- Paulsen, F.P.; Steven, P.; Tsokos, M.; Jungmann, K.; Müller, A.; Verse, T.; Pirsig, W. Upper Airway Epithelial Structural Changes in Obstructive Sleep-Disordered Breathing. Am. J. Respir. Crit. Care Med. 2002, 166, 501–509. [Google Scholar] [CrossRef]
- Boyd, J.H.; Petrof, B.J.; Hamid, Q.; Fraser, R.; Kimoff, R.J. Upper Airway Muscle Inflammation and Denervation Changes in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2004, 170, 541–546. [Google Scholar] [CrossRef]
- McDonnell, M.J.; O’Toole, D.; Ward, C.; Pearson, J.P.; Lordan, J.L.; De Soyza, A.; Loebinger, M.; Chalmers, J.D.; Laffey, J.G.; Rutherford, R.M. A Qualitative Synthesis of Gastro-Oesophageal Reflux in Bronchiectasis: Current Understanding and Future Risk. Respir. Med. 2018, 141, 132–143. [Google Scholar] [CrossRef]
- Ledson, M.J.; Wilson, G.E.; Tran, J.; Walshaw, M.J. Tracheal Microaspiration in Adult Cystic Fibrosis. J. R. Soc. Med. 1998, 91, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.S.; Lee, J.S.; He, Z.; Ryu, J.H. Reflux-Aspiration in Chronic Lung Disease. Ann. Am. Thorac. Soc. 2020, 17, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.D.; Walters, E.H.; Simpson, J.L.; Keely, S.; Wark, P.A.B.; O’Toole, R.F.; Hansbro, P.M. Hypoxia-Inducible Factor and Bacterial Infections in Chronic Obstructive Pulmonary Disease. Respirology 2020, 25, 53–63. [Google Scholar] [CrossRef]
- Locke, B.W.; Lee, J.J.; Sundar, K.M. OSA and Chronic Respiratory Disease: Mechanisms and Epidemiology. Int. J. Environ. Res. Public Health 2022, 19, 5473. [Google Scholar] [CrossRef]
- Shteinberg, M.; Nassrallah, N.; Jrbashyan, J.; Uri, N.; Stein, N.; Adir, Y. Upper Airway Involvement in Bronchiectasis Is Marked by Early Onset and Allergic Features. ERJ Open Res. 2018, 4, 00115–2017. [Google Scholar] [CrossRef]
- Javaheri, S.; Kazemi, H. Metabolic Alkalosis and Hypoventilation in Humans. Am. Rev. Respir. Dis. 1987, 136, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Khoo, M.C.; Kronauer, R.E.; Strohl, K.P.; Slutsky, A.S. Factors Inducing Periodic Breathing in Humans: A General Model. J. Appl. Physiol. 1982, 53, 644–659. [Google Scholar] [CrossRef]
- Ghazanshahi, S.D.; Khoo, M.C. Estimation of Chemoreflex Loop Gain Using Pseudorandom Binary CO2 Stimulation. IEEE Trans. Biomed. Eng. 1997, 44, 357–366. [Google Scholar] [CrossRef]
- White, D.P. Pathogenesis of Obstructive and Central Sleep Apnea. Am. J. Respir. Crit. Care Med. 2005, 172, 1363–1370. [Google Scholar] [CrossRef]
- Rosen, M.J. Chronic Cough Due to Bronchiectasis: ACCP Evidence-Based Clinical Practice Guidelines. Chest 2006, 129, 122S–131S. [Google Scholar] [CrossRef]
- Penketh, A.R.; Wise, A.; Mearns, M.B.; Hodson, M.E.; Batten, J.C. Cystic Fibrosis in Adolescents and Adults. Thorax 1987, 42, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.D. Cough in Pulmonary Tuberculosis: Existing Knowledge and General Insights. Pulm. Pharmacol. Ther. 2019, 55, 89–94. [Google Scholar] [CrossRef]
- Horner, R.L.; Sanford, L.D.; Pack, A.I.; Morrison, A.R. Activation of a Distinct Arousal State Immediately after Spontaneous Awakening from Sleep. Brain Res. 1997, 778, 127–134. [Google Scholar] [CrossRef]
- Malhotra, A.; Mesarwi, O.; Pepin, J.-L.; Owens, R.L. Endotypes and Phenotypes in Obstructive Sleep Apnea. Curr. Opin. Pulm. Med. 2020, 26, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Hlavac, M.C.; Catcheside, P.G.; McDonald, R.; Eckert, D.J.; Windler, S.; McEvoy, R.D. Hypoxia Impairs the Arousal Response to External Resistive Loading and Airway Occlusion during Sleep. Sleep 2006, 29, 624–631. [Google Scholar]
- Júnior, N.S.F.; Oliveira, L.V.F.; Perez, E.A.; De Oliveira, E.F.; Apostolico, N.; Pereira, N.A.; Santos, I.D.R.D.; Urbano, J.J.; Souza, I.D.; Polonio, I.B.; et al. Observational Study of Sleep, Respiratory Mechanics and Quality of Life in Patients with Non-Cystic Fibrosis Bronchiectasis: A Protocol Study. BMJ Open 2015, 5, e008183. [Google Scholar] [CrossRef]
- Radovanovic, D.; Santus, P.; Blasi, F.; Sotgiu, G.; D’Arcangelo, F.; Simonetta, E.; Contarini, M.; Franceschi, E.; Goeminne, P.C.; Chalmers, J.D.; et al. A Comprehensive Approach to Lung Function in Bronchiectasis. Respir. Med. 2018, 145, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Guan, W.; Xu, G.; Lin, Z.; Tang, Y.; Lin, Z.; Li, H.; Gao, Y.; Luo, Q.; Zhong, N.; et al. Sleep Disturbances and Health-Related Quality of Life in Adults with Steady-State Bronchiectasis. PLoS ONE 2014, 9, e102970. [Google Scholar] [CrossRef] [PubMed]
- Erdem, E.; Ersu, R.; Karadag, B.; Karakoc, F.; Gokdemir, Y.; Ay, P.; Akpinar, I.N.; Dagli, E. Effect of Night Symptoms and Disease Severity on Subjective Sleep Quality in Children with Non-Cystic-Fibrosis Bronchiectasis. Pediatr. Pulmonol. 2011, 46, 919–926. [Google Scholar] [CrossRef]
- Yang, X.; Tang, X.; Cao, Y.; Dong, L.; Wang, Y.; Zhang, J.; Cao, J. The Bronchiectasis in COPD-OSA Overlap Syndrome Patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 605–611. [Google Scholar] [CrossRef]
- Oktem, S.; Karadag, B.; Erdem, E.; Gokdemir, Y.; Karakoc, F.; Dagli, E.; Ersu, R. Sleep Disordered Breathing in Patients with Primary Ciliary Dyskinesia. Pediatr. Pulmonol. 2013, 48, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, F.; Esposito, M.; Montella, S.; Cantone, E.; Mollica, C.; De Stefano, S.; Mirra, V.; Carotenuto, M. Sleep Disordered Breathing and Airway Disease in Primary Ciliary Dyskinesia. Respirology 2014, 19, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Reiter, J.; Gileles-Hillel, A.; Cohen-Cymberknoh, M.; Rosen, D.; Kerem, E.; Gozal, D.; Forno, E. Sleep Disorders in Cystic Fibrosis: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2020, 51, 101279. [Google Scholar] [CrossRef] [PubMed]
- Perin, C.; Fagondes, S.C.; Casarotto, F.C.; Pinotti, A.F.F.; Barreto, S.S.M.; Dalcin, P.d.T.R. Sleep Findings and Predictors of Sleep Desaturation in Adult Cystic Fibrosis Patients. Sleep Breath. 2012, 16, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Shakkottai, A.; O’Brien, L.M.; Nasr, S.Z.; Chervin, R.D. Sleep Disturbances and Their Impact in Pediatric Cystic Fibrosis. Sleep Med. Rev. 2018, 42, 100–110. [Google Scholar] [CrossRef]
- Spicuzza, L.; Sciuto, C.; Leonardi, S.; La Rosa, M. Early Occurrence of Obstructive Sleep Apnea in Infants and Children with Cystic Fibrosis. Arch. Pediatr. Adolesc. Med. 2012, 166, 1165–1169. [Google Scholar] [CrossRef]
- Villa, M.P.; Pagani, J.; Lucidi, V.; Palamides, S.; Ronchetti, R. Nocturnal Oximetry in Infants with Cystic Fibrosis. Arch. Dis. Child. 2001, 84, 50–54. [Google Scholar] [CrossRef]
- Reiter, J.; Breuer, O.; Cohen-Cymberknoh, M.; Forno, E.; Gileles-Hillel, A. Sleep in Children with Cystic Fibrosis: More under the Covers. Pediatr. Pulmonol. 2022, 57, 1944–1951. [Google Scholar] [CrossRef]
- Jagpal, S.K.; Jobanputra, A.M.; Ahmed, O.H.; Santiago, T.V.; Ramagopal, M. Sleep-Disordered Breathing in Cystic Fibrosis. Pediatr. Pulmonol. 2021, 56 (Suppl. S1), S23–S31. [Google Scholar] [CrossRef]
- Milross, M.A.; Piper, A.J.; Dobbin, C.J.; Bye, P.T.P.; Grunstein, R.R. Sleep Disordered Breathing in Cystic Fibrosis. Sleep Med. Rev. 2004, 8, 295–308. [Google Scholar] [CrossRef]
- de Sousa, L.P.; Liberato, F.M.G.; Vendrusculo, F.M.; Donadio, M.V.F.; Barbosa, R.R.B. Obstructive Sleep Apnea in Children and Adolescents with Cystic Fibrosis and Preserved Lung Function or Mild Impairment: A Systematic Review and Meta-Analysis of Prevalence. Sleep Med. 2021, 88, 36–43. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of Obstructive Sleep Apnea in the General Population: A Systematic Review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Milross, M.A.; Piper, A.J.; Norman, M.; Willson, G.N.; Grunstein, R.R.; Sullivan, C.E.; Bye, P.T. Predicting Sleep-Disordered Breathing in Patients with Cystic Fibrosis. Chest 2001, 120, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Welsner, M.; Dietz-Terjung, S.; Stehling, F.; Schulte, T.; Niehammer, U.; Gahbiche, F.-E.; Taube, C.; Strassburg, S.; Schoebel, C.; Weinreich, G.; et al. Obstructive Sleep Apnea and Nocturnal Hypoxemia in Adult Patients with Cystic Fibrosis. BMC Pulm. Med. 2022, 22, 446. [Google Scholar] [CrossRef] [PubMed]
- McKone, E.F.; Ariti, C.; Jackson, A.; Zolin, A.; Carr, S.B.; Orenti, A.; van Rens, J.G.; Lemonnier, L.; Macek, M.J.; Keogh, R.H.; et al. Survival Estimates in European Cystic Fibrosis Patients and the Impact of Socioeconomic Factors: A Retrospective Registry Cohort Study. Eur. Respir. J. 2021, 58, 2002288. [Google Scholar] [CrossRef] [PubMed]
- Kutney, K.A.; Sandouk, Z.; Desimone, M.; Moheet, A. Obesity in Cystic Fibrosis. J. Clin. Transl. Endocrinol. 2021, 26, 100276. [Google Scholar] [CrossRef]
- Bouka, A.; Tiede, H.; Liebich, L.; Dumitrascu, R.; Hecker, C.; Reichenberger, F.; Mayer, K.; Seeger, W.; Schulz, R. Quality of Life in Clinically Stable Adult Cystic Fibrosis Out-Patients: Associations with Daytime Sleepiness and Sleep Quality. Respir. Med. 2012, 106, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Veronezi, J.; Carvalho, A.P.; Ricachinewsky, C.; Hoffmann, A.; Kobayashi, D.Y.; Piltcher, O.B.; Abreu e Silva, F.A.; Martinez, D. Sleep-Disordered Breathing in Patients with Cystic Fibrosis. J. Bras. Pneumol. Publicacao Of. Soc. Bras. Pneumol. Tisilogia 2015, 41, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.T.T.; Salles, C.; Gregório, P.B.; Barros, A.T.; Santana, A.; Araújo-Filho, J.B.; Acosta, A.X. Evaluation of the Upper Airway in Children and Adolescents with Cystic Fibrosis and Obstructive Sleep Apnea Syndrome. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1780–1785. [Google Scholar] [CrossRef]
- Katz, E.S. Cystic Fibrosis and Sleep. Clin. Chest Med. 2014, 35, 495–504. [Google Scholar] [CrossRef]
- Young, A.C.; Wilson, J.W.; Kotsimbos, T.C.; Naughton, M.T. Randomised Placebo Controlled Trial of Non-Invasive Ventilation for Hypercapnia in Cystic Fibrosis. Thorax 2008, 63, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, L.E.; Belcher, J.; Bright-Thomas, R.J. Non-Invasive Ventilation Is Associated with Long-Term Improvements in Lung Function and Gas Exchange in Cystic Fibrosis Adults with Hypercapnic Respiratory Failure. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2021, 20, e40–e45. [Google Scholar] [CrossRef] [PubMed]
- Houben, R.M.G.J.; Dodd, P.J. The Global Burden of Latent Tuberculosis Infection: A Re-Estimation Using Mathematical Modelling. PLoS Med. 2016, 13, e1002152. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, E.D.D.; Gil-Santana, L.; Ramalho, D.; Tonomura, E.; Silva, E.C.; Oliveira, M.M.; Andrade, B.B.; Kritski, A. Associations between Systemic Inflammation, Mycobacterial Loads in Sputum and Radiological Improvement after Treatment Initiation in Pulmonary TB Patients from Brazil: A Prospective Cohort Study. BMC Infect. Dis. 2016, 16, 368. [Google Scholar] [CrossRef]
- Kaufmann, S.H.E.; Dorhoi, A. Inflammation in Tuberculosis: Interactions, Imbalances and Interventions. Curr. Opin. Immunol. 2013, 25, 441–449. [Google Scholar] [CrossRef]
- Sharma, S.K.; Upadhyay, V. Epidemiology, Diagnosis & Treatment of Non-Tuberculous Mycobacterial Diseases. Indian J. Med. Res. 2020, 152, 185–226. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Marras, T.K.; Adjemian, J.; Zhang, H.; Wang, P.; Zhang, Q. Incidence and Prevalence of Nontuberculous Mycobacterial Lung Disease in a Large U.S. Managed Care Health Plan, 2008–2015. Ann. Am. Thorac. Soc. 2020, 17, 178–185. [Google Scholar] [CrossRef]
- Faverio, P.; Stainer, A.; Bonaiti, G.; Zucchetti, S.C.; Simonetta, E.; Lapadula, G.; Marruchella, A.; Gori, A.; Blasi, F.; Codecasa, L.; et al. Characterizing Non-Tuberculous Mycobacteria Infection in Bronchiectasis. Int. J. Mol. Sci. 2016, 17, 1913. [Google Scholar] [CrossRef]
- Vadakkan Devassy, T.; Ps, N.; Sharma, D.; Thomas, A.M. Sleep Disorders in Elderly Population Suffering from TB and Respiratory Diseases. Indian J. Tuberc. 2022, 69 (Suppl. S2), S272–S279. [Google Scholar] [CrossRef]
- Lee, T.; Tsai, M.-J.; Chung, Y.-C.; Huang, H.-L.; Chang, W.-A.; Chong, I.-W.; Huang, M.-S. Association between Sleep Apnea and Tuberculosis—A Nationwide Population-Based Study. Eur. Respir. J. 2014, 44, P2658. [Google Scholar]
- Patel, A.B.; Hinni, M.L. Tuberculous Retropharyngeal Abscess Presenting with Symptoms of Obstructive Sleep Apnea. Eur. Arch. Oto-Rhino-Laryngology 2013, 270, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.F.; Tezer, M.S.; Titiz, A.; Özlügedik, S.; Yalçin, F.; Ünal, A. Snoring and Obstructive Sleep Apnea Due to Nasopharyngeal Tuberculosis. Gazi Med. J. 2005, 16, 47–49. [Google Scholar]
- Sharma, H.S.; Kurl, D.N.; Kamal, M.Z. Tuberculoid Granulomatous Lesion of the Pharynx--Review of the Literature. Auris. Nasus. Larynx 1998, 25, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, T.; Tatsumi, K.; Kimura, H.; Honda, Y.; Kuriyama, T. Sleep Oxygen Desaturation in Late Sequelae of Pulmonary Tuberculosis. Intern. Med. 1996, 35, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Tabusadani, M.; Yamane, K.; Takao, S.; Kuroyama, Y.; Mori, K.; Ono, K.; Kawahara, K.; Omatsu, S.; Furuuchi, K.; et al. Prevalence of and Risk Factors for Depressive Symptoms in Non-Tuberculous Mycobacterial Pulmonary Disease. Int. J. Tuberc. Lung Dis. 2022, 26, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.R.; McNicholas, W.T.; Montserrat, J.M.; Eckel, J. Adipose Tissue in Obesity and Obstructive Sleep Apnoea. Eur. Respir. J. 2012, 39, 746–767. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.K.Y.; Ing, A.J.; Laks, L.; Cossa, G.; Rogers, P.; Birring, S.S. Chronic Cough in Patients with Sleep-Disordered Breathing. Eur. Respir. J. 2010, 35, 368–372. [Google Scholar] [CrossRef]
- Birring, S.S.; Ing, A.J.; Chan, K.; Cossa, G.; Matos, S.; Morgan, M.D.L.; Pavord, I.D. Obstructive Sleep Apnoea: A Cause of Chronic Cough. Cough 2007, 3, 7. [Google Scholar] [CrossRef]
- Eltzschig, H.K.; Carmeliet, P. Hypoxia and Inflammation. N. Engl. J. Med. 2011, 364, 656–665. [Google Scholar] [CrossRef]
- Montgomery, S.T.; Mall, M.A.; Kicic, A.; Stick, S.M. Hypoxia and Sterile Inflammation in Cystic Fibrosis Airways: Mechanisms and Potential Therapies. Eur. Respir. J. 2017, 49, 1600903. [Google Scholar] [CrossRef]
- Perger, E.; Baillieul, S.; Esteve, F.; Pichon, A.; Bilo, G.; Soranna, D.; Doutreleau, S.; Savina, Y.; Ulliel-Roche, M.; Brugniaux, J.V.; et al. Nocturnal Hypoxemia, Blood Pressure, Vascular Status and Chronic Mountain Sickness in the Highest City in the World. Ann. Med. 2022, 54, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Perger, E.; Soranna, D.; Pengo, M.; Meriggi, P.; Lombardi, C.; Parati, G. Sleep-Disordered Breathing among Hospitalized Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2021, 203, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, K.; Liu, K.; Li, Z.; Yang, J.; Dong, Y.; Nie, M.; Chen, J.; Ruan, Y.; Kang, J. Obstructive Sleep Apnea Exacerbates Airway Inflammation in Patients with Chronic Obstructive Pulmonary Disease. Sleep Med. 2015, 16, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Faraut, B.; Boudjeltia, K.Z.; Vanhamme, L.; Kerkhofs, M. Immune, Inflammatory and Cardiovascular Consequences of Sleep Restriction and Recovery. Sleep Med. Rev. 2012, 16, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and Immune Function. Pflugers Arch. 2012, 463, 121–137. [Google Scholar] [CrossRef]
- Allen, J.M.; Graef, D.M.; Ehrentraut, J.H.; Tynes, B.L.; Crabtree, V.M. Sleep and Pain in Pediatric Illness: A Conceptual Review. CNS Neurosci. Ther. 2016, 22, 880–893. [Google Scholar] [CrossRef]
- Kaczmarski, P.; Karuga, F.F.; Szmyd, B.; Sochal, M.; Białasiewicz, P.; Strzelecki, D.; Gabryelska, A. The Role of Inflammation, Hypoxia, and Opioid Receptor Expression in Pain Modulation in Patients Suffering from Obstructive Sleep Apnea. Int. J. Mol. Sci. 2022, 23, 9080. [Google Scholar] [CrossRef]
- Tuleta, I.; Stöckigt, F.; Juergens, U.R.; Pizarro, C.; Schrickel, J.W.; Kristiansen, G.; Nickenig, G.; Skowasch, D. Intermittent Hypoxia Contributes to the Lung Damage by Increased Oxidative Stress, Inflammation, and Disbalance in Protease/Antiprotease System. Lung 2016, 194, 1015–1020. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).