
Prenatal Exposure to Air Pollutants and Attentional Deficit Hyperactivity Disorder Development in Children: A Systematic Review
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Process
2.2. Data Extraction
2.3. Quality and Risk of Bias Assessment
3. Results
3.1. Study Selection
3.2. Studies Characteristics
3.3. Studies Results
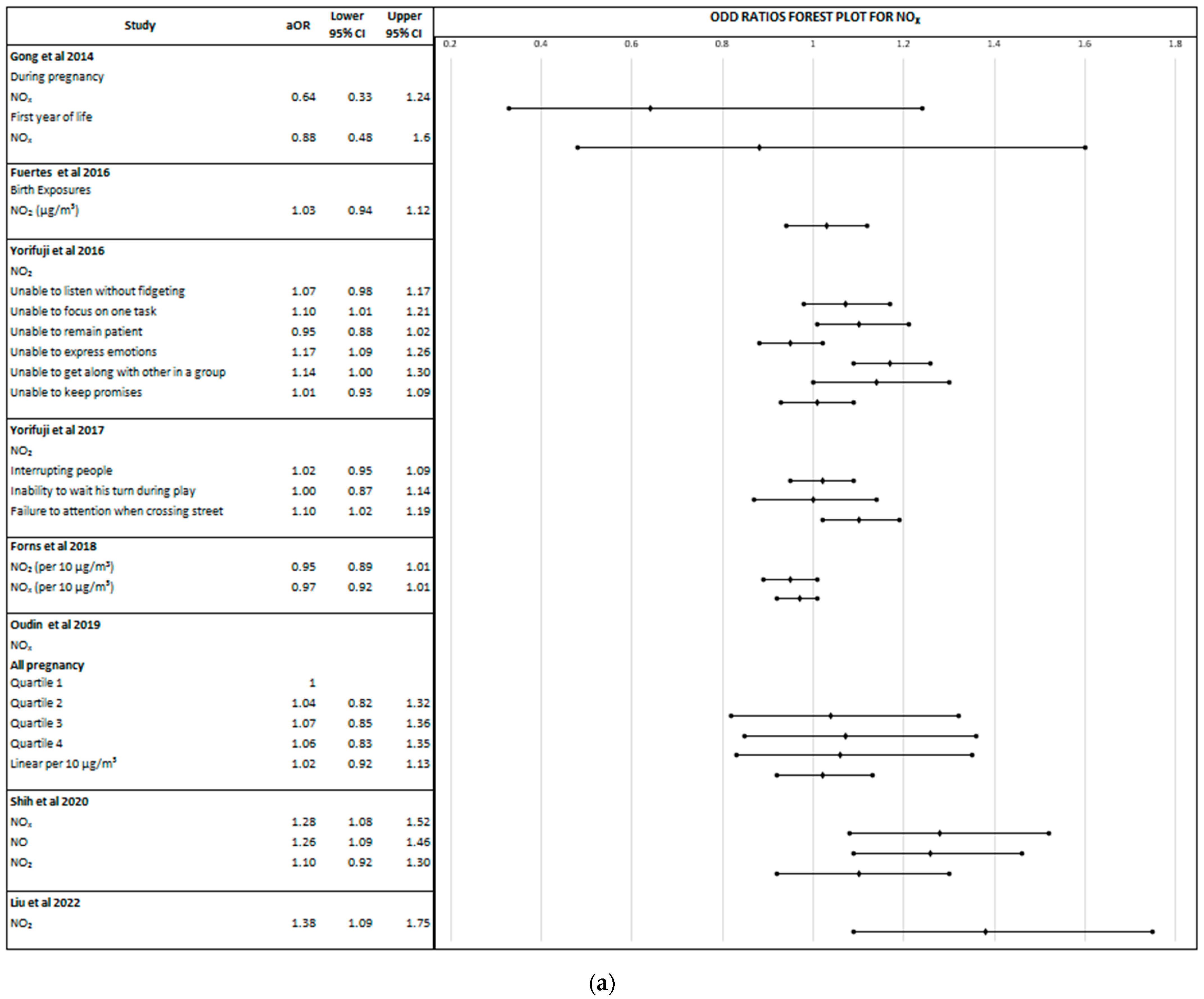
3.3.1. Nitrogen Oxides
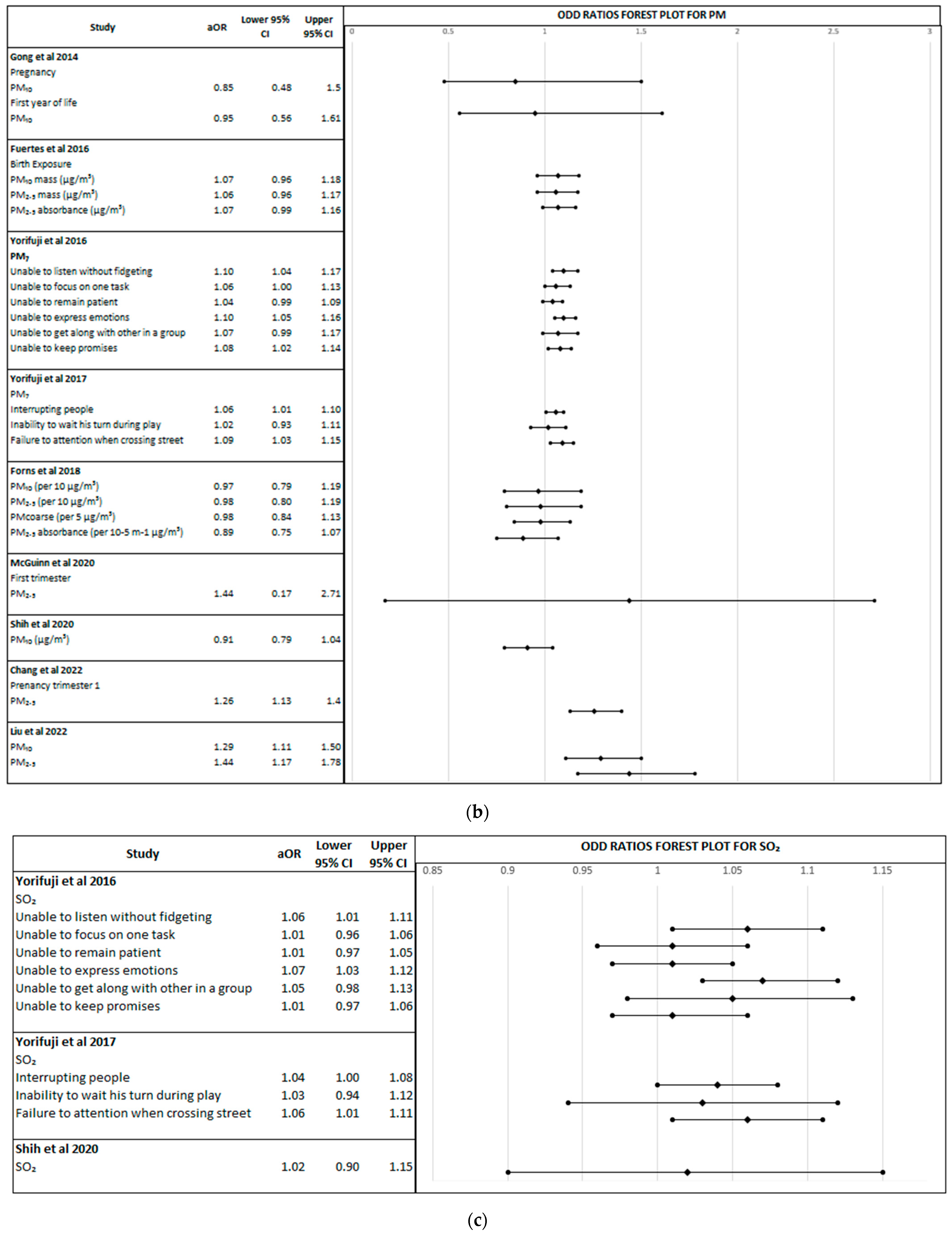
3.3.2. Particulate Matter
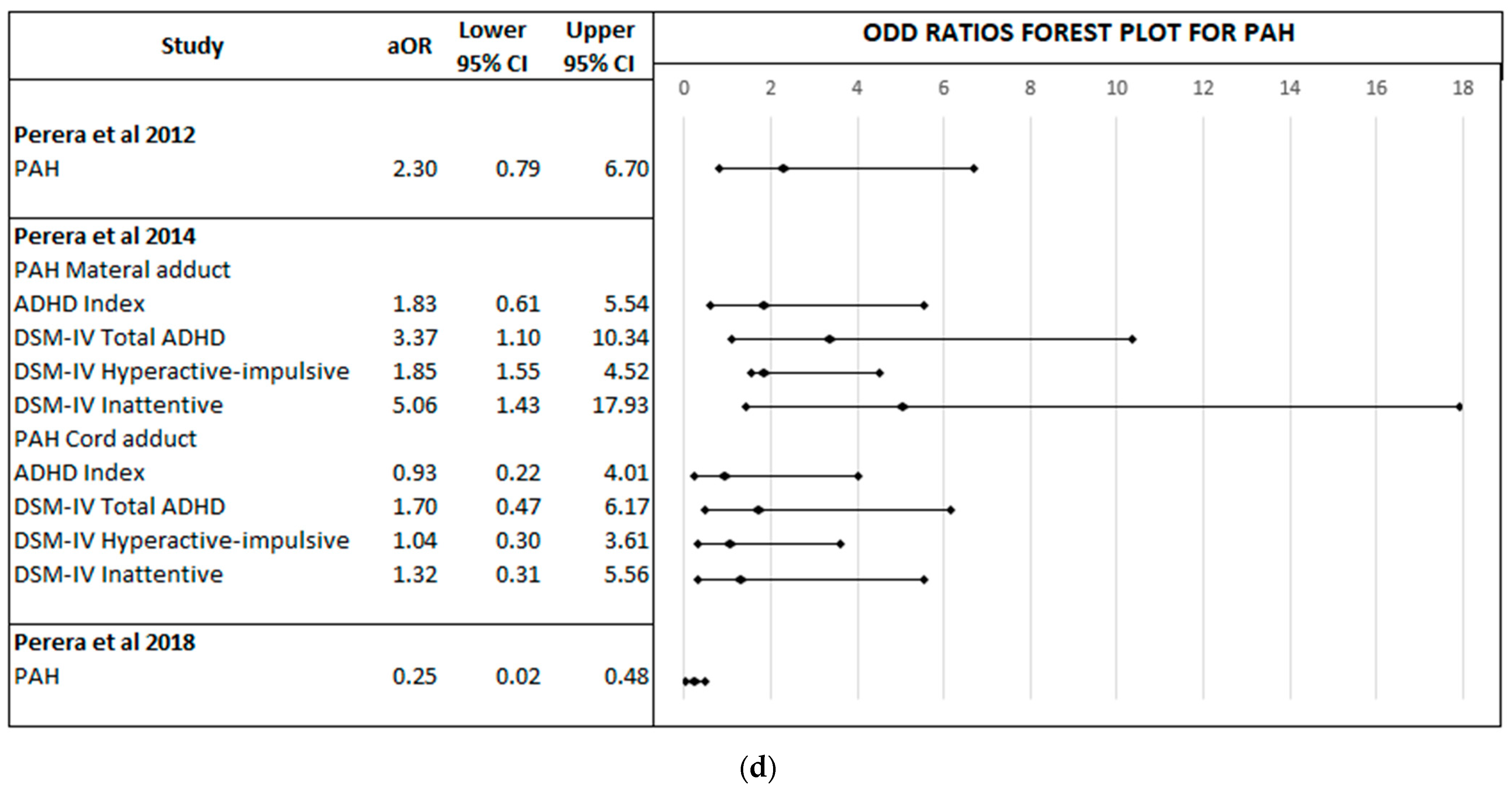
3.3.3. Polycyclic Aromatic Hydrocarbons
3.3.4. Sulphur Dioxide
3.3.5. Carbon Monoxide and Ozone
3.4. Risk Bias and Quality Assessment
4. Discussion
4.1. Selected Studies Limitations
4.2. Limitations and Strengths of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Global Air Quality Guidelines. Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021.
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Sunyer, J.; Dadvand, P. Pre-natal brain development as a target for urban air pollution. Basic Clin. Pharmacol. Toxicol. 2019, 125, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Block, M.L.; Calderón-Garcidueñas, L. Air pollution: Mechanisms of neuroinflammation and CNS disease. Trends Neurosci. 2009, 32, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardenas-Iniguez, C.; Burnor, E.; Herting, M.M. Neurotoxicants, the developing brain, and mental health. Biol. Psychiatry Glob. Open Sci. 2022, 2, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.C.; Garrick, J.M. Developmental impact of air pollution on brain function. Neurochem. Int. 2019, 131, 104580. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.H.; Counsell, S.J.; McGonnell, I.M.; Thornton, C. Early life exposure to air pollution impacts neuronal and glial cell function leading to impaired neurodevelopment. BioEssays News Rev. Mol. Cell. Dev. Biol. 2021, 43, 2000288. [Google Scholar] [CrossRef]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in children and young people: Prevalence, care pathways, and service provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Sans, J.C.; Hidalgo, P.M.; Castellví, J.R.; Moreso, N.V.; Martínez, C.H. Prevalence and Epidemiological Characteristics of ADHD in Pre-School and School Age Children in the Province of Tarragona, Spain. J. Atten. Disord. 2021, 25, 1818–1833. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef]
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Blumberg, S.J.; Kogan, M.D.; Boyle, C.A. Prevalence and Trends of Developmental Disabilities among Children in the United States: 2009–2017. Pediatrics 2019, 144. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Quintero, J.; Ramos-Quiroga, J.A.; Sebastián, J.S.; Montañés, F.; Fernández-Jaén, A.; Martínez-Raga, J.; Giral, M.G.; Graell, M.; Mardomingo, M.J.; Soutullo, C.; et al. Health care and societal costs of the management of children and adolescents with attention-deficit/hyperactivity disorder in Spain: A descriptive analysis. BMC Psychiatry 2018, 18, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciberras, E.; Streatfeild, J.; Ceccato, T.; Pezzullo, L.; Scott, J.G.; Middeldorp, C.M.; Hutchins, P.; Paterson, R.; Bellgrove, M.A.; Coghill, D. Social and Economic Costs of Attention-Deficit/Hyperactivity Disorder Across the Lifespan. J. Atten. Disord. 2022, 26, 72–87. [Google Scholar] [CrossRef]
- Sciberras, E.; Mulraney, M.; Silva, D.; Coghill, D. Prenatal Risk Factors and the Etiology of ADHD-Review of Existing Evidence. Curr. Psychiatry Rep. 2017, 19, 1. [Google Scholar] [CrossRef]
- Montagna, A.; Karolis, V.; Batalle, D.; Counsell, S.; Rutherford, M.; Arulkumaran, S.; Happe, F.; Edwards, D.; Nosarti, C. ADHD symptoms and their neurodevelopmental correlates in children born very preterm. PLoS ONE 2020, 15, e0224343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Kim, J.Y.; Lee, J.; Jeong, G.H.; Lee, E.; Lee, S.; Lee, K.H.; Kronbichler, A.; Stubbs, B.; Solmi, M.; et al. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: An umbrella review. Lancet Psychiatry 2020, 7, 955–970. [Google Scholar] [CrossRef] [PubMed]
- Roigé-Castellví, J.; Murphy, M.M.; Voltas, N.; Solé-Navais, P.; Cavallé-Busquets, P.; Fernández-Ballart, J.; Ballesteros, M.; Canals-Sans, J. A Prospective Study of Maternal Exposure to Smoking during Pregnancy and Behavioral Development in the Child. J. Child Fam. Stud. 2021, 30, 2204–2214. [Google Scholar] [CrossRef]
- Aghaei, M.; Janjani, H.; Yousefian, F.; Jamal, A.; Yunesian, M. Association between ambient gaseous and particulate air pollutants and attention deficit hyperactivity disorder (ADHD) in children; a systematic review. Environ. Res. 2019, 173, 135–156. [Google Scholar] [CrossRef] [PubMed]
- Myhre, O.; Låg, M.; Villanger, G.D.; Oftedal, B.; Øvrevik, J.; Holme, J.A.; Aase, H.; Paulsen, R.E.; Bal-Price, A.; Dirven, H. Early life exposure to air pollution particulate matter (PM) as risk factor for attention deficit/hyperactivity disorder (ADHD): Need for novel strategies for mechanisms and causalities. Toxicol. Appl. Pharmacol. 2018, 354, 196–214. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, M.; Holst, G.J.; Hansen, B.; Geels, C.; Kalkbrenner, A.; Schendel, D.; Brandt, J.; Pedersen, C.B.; Dalsgaard, S. Exposure to air pollution in early childhood and the association with Attention-Deficit Hyperactivity Disorder. Environ. Res. 2019, 183, 108930. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Sohn, J.H.; Cho, S.J.; Seo, H.Y.; Hwang, I.U.; Hong, Y.-C.; Kim, K.-N. Association between short-term air pollution exposure and attention-deficit/hyperactivity disorder-related hospital admissions among adolescents: A nationwide time-series study. Environ. Pollut. 2020, 266 Pt 1, 115369. [Google Scholar] [CrossRef]
- Mortamais, M.; Pujol, J.; Martínez-Vilavella, G.; Fenoll, R.; Reynes, C.; Sabatier, R.; Rivas, I.; Forns, J.; Vilor-Tejedor, N.; Alemany, S.; et al. Effects of prenatal exposure to particulate matter air pollution on corpus callosum and behavioral problems in children. Environ. Res. 2019, 178, 108734. [Google Scholar] [CrossRef] [PubMed]
- Rivas, I.; Basagaña, X.; Cirach, M.; López-Vicente, M.; Suades-González, E.; Garcia-Esteban, R.; Álvarez-Pedrerol, M.; Dadvand, P.; Sunyer, J. Association between Early Life Exposure to Air Pollution and Working Memory and Attention. Environ. Health Perspect. 2019, 127, 057002. [Google Scholar] [CrossRef] [Green Version]
- Peterson, B.S.; Rauh, V.A.; Bansal, R.; Hao, X.; Toth, Z.; Nati, G.; Walsh, K.; Miller, R.L.; Arias, F.; Semanek, D.; et al. Effects of Prenatal Exposure to Air Pollutants (Polycyclic Aromatic Hydrocarbons) on the Development of Brain White Matter, Cognition, and Behavior in Later Childhood. JAMA Psychiatry 2015, 72, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Seeni, I.; Ha, S.; Nobles, C.; Liu, D.; Sherman, S.; Mendola, P. Air pollution exposure during pregnancy: Maternal asthma and neonatal respiratory outcomes. Ann. Epidemiol. 2018, 28, 612–618.e4. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Ren, Z.; Liu, Y.; Qiu, Y.; Yang, H.; Zhou, Y.; Wang, X.; Jiao, K.; Liao, J.; Ma, L. The Association between Preterm Birth and Ambient Air Pollution Exposure in Shiyan, China, 2015–2017. Int. J. Environ. Res. Public Health 2021, 18, 4326. [Google Scholar] [CrossRef] [PubMed]
- Daneshparvar, M.; Mostafavi, S.-A.; Jeddi, M.Z.; Yunesian, M.; Mesdaghinia, A.; Mahvi, A.H.; Akhondzadeh, S. The Role of Lead Exposure on Attention-Deficit/ Hyperactivity Disorder in Children: A Systematic Review. Iran. J. Psychiatry 2016, 11, 1–14. [Google Scholar]
- Skogheim, T.S.; Weyde, K.V.F.; Engel, S.M.; Aase, H.; Surén, P.; Øie, M.G.; Biele, G.; Reichborn-Kjennerud, T.; Caspersen, I.H.; Hornig, M.; et al. Metal and essential element concentrations during pregnancy and associations with autism spectrum disorder and attention-deficit/hyperactivity disorder in children. Environ. Int. 2021, 152, 106468. [Google Scholar] [CrossRef] [PubMed]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; de Matteis, S.; Jung, S.-H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A.; et al. Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air Pollution and Organ Systems. Chest 2019, 155, 417–426. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Air Pollution, the Invisible Killer; World Health Organization: Geneva, Switzerland, 2018. Available online: http://www.who.int/health-topics/air-pollution (accessed on 19 June 2022).
- Hjortebjerg, D.; Andersen, A.-M.N.; Christensen, J.S.; Ketzel, M.; Raaschou-Nielsen, O.; Sunyer, J.; Julvez, J.; Forns, J.; Sørensen, M. Exposure to Road Traffic Noise and Behavioral Problems in 7-Year-Old Children: A Cohort Study. Environ. Health Perspect. 2016, 124, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donzelli, G.; Llopis-Gonzalez, A.; Llopis-Morales, A.; Cioni, L.; Morales-Suárez-Varela, M. Particulate matter exposure and attention-deficit/hyperactivity disorder in children: A systematic review of epidemiological studies. Int. J. Environ. Res. Public Health 2020, 17, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Wang, C.; Zhang, X.; Song, H.; Li, Y. Association between exposure to air pollutants and attention-deficit hyperactivity disorder (ADHD) in children: A systematic review and meta-analysis. Int. J. Environ. Health Res. 2022, 32, 207–219. [Google Scholar] [CrossRef]
- Volk, H.E.; Perera, F.; Braun, J.M.; Kingsley, S.L.; Gray, K.; Buckley, J.; Clougherty, J.E.; Croen, L.A.; Eskenazi, B.; Herting, M.; et al. Prenatal air pollution exposure and neurodevelopment: A review and blueprint for a harmonized approach within ECHO. In Environmental Research; Academic Press Inc.: Cambridge, MA, USA, 2021; Volume 196. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Conell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 26 July 2022).
- World Health Organization. Regional Office for Europe. In Risk of Bias Assessment Instrument for Systematic Reviews Informing WHO Global Air Quality Guidelines; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2020. Available online: https://apps.who.int/iris/handle/10665/341717 (accessed on 19 June 2022).
- Hansson, S.L.; Svanstrom Rojvall, A.; Rastam, M.; Gillberg, C.; Gillberg, C.; Anckarsater, H. Psychiatric telephone interview with parents for screening of childhood autism—Tics, attention-deficit hyperactivity disorder and other comorbidities (A-TAC): Preliminary reliability and validity. Br. J. Psychiatry 2005, 187, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) (Manual Diagnóstico y Estadístico de Los Trastornos Mentales DSM-IV), 4th ed.; Masson: Barcelona, Spain, 2002. [Google Scholar]
- Dupaul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale—IV: Checklists, Norms, and Clinical Interpretation; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Conners, C.K. Conners’ Rating Scales–Revised: User’s Manual; Multi-Health Systems, Incorporated: Toronto, ON, Canada, 1997. [Google Scholar]
- Conners, C.; Erhardt, D.; Sparrow, E. Conners’ Adult ADHD Rating Scales: Technical Manual; Multi-Health Systems: New York, NY, USA, 1999. [Google Scholar]
- Achenbach, T.M. Manual for ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Itani, T. Standardization of the Japanese version of the child behavior checklist/4-18. Psychiatr. Neurol. Pediatr. Jpn. 2001, 41, 243–252. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. BASC-2 Behavior Assessment System for Children 2; Pearson: Bloomington, MN, USA, 2004. [Google Scholar]
- The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993.
- WHO. International Classification of Diseases: Basic Tabulation List with Alphabetic Index, 9th ed.; World Health Organization: Geneva, Switzerland, 1978.
- Perera, F.P.; Tang, D.; Wang, S.; Vishnevetsky, J.; Zhang, B.; Diaz, D.; Camann, D.; Rauh, V. Prenatal polycyclic aromatic hydrocarbon (PAH) exposure and child behavior at age 6–7 years. Environ. Health Perspect. 2012, 120, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Gong, T.; Almqvist, C.; Bölte, S.; Lichtenstein, P.; Anckarsäter, H.; Lind, T.; Lundholm, C.; Pershagen, G. Exposure to air pollution from traffic and neurodevelopmental disorders in Swedish twins. Twin Res. Hum. Genet. Off. J. Int. Soc. Twin Stud. 2014, 17, 553–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, F.P.; Chang, H.W.; Tang, D.; Roen, E.L.; Herbstman, J.; Margolis, A.; Huang, T.J.; Miller, R.L.; Wang, S.; Rauh, V. Early-life exposure to polycyclic aromatic hydrocarbons and ADHD behavior problems. PLoS ONE 2014, 9, e111670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuertes, E.; Standl, M.; Forns, J.; Berdel, D.; Garcia-Aymerich, J.; Markevych, I.; Schulte-Koerne, G.; Sugiri, D.; Schikowski, T.; Tiesler, C.M.T.; et al. Traffic-related air pollution and hyperactivity/inattention, dyslexia and dyscalculia in adolescents of the German GINIplus and LISAplus birth cohorts. Environ. Int. 2016, 97, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Kashima, S.; Diez, M.H.; Kado, Y.; Sanada, S.; Doi, H. Prenatal Exposure to Traffic-related Air Pollution and Child Behavioral Development Milestone Delays in Japan. Epidemiology 2016, 27, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Kashima, S.; Diez, M.H.; Kado, Y.; Sanada, S.; Doi, H. Prenatal exposure to outdoor air pollution and child behavioral problems at school age in Japan. Environ. Int. 2017, 99, 192–198. [Google Scholar] [CrossRef]
- Forns, J.; Sunyer, J.; Garcia-Esteban, R.; Porta, D.; Ghassabian, A.; Giorgis-Allemand, L.; Gong, T.; Gehring, U.; Sørensen, M.; Standl, M.; et al. Air Pollution Exposure During Pregnancy and Symptoms of Attention Deficit and Hyperactivity Disorder in Children in Europe. Epidemiology 2018, 29, 618–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, F.P.; Wheelock, K.; Wang, Y.; Tang, D.; Margolis, A.E.; Badia, G.; Cowell, W.; Miller, R.L.; Rauh, V.; Wang, S.; et al. Combined effects of prenatal exposure to polycyclic aromatic hydrocarbons and material hardship on child ADHD behavior problems. Environ. Res. 2018, 160, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Oudin, A.; Frondelius, K.; Haglund, N.; Källén, K.; Forsberg, B.; Gustafsson, P.; Malmqvist, E. Prenatal exposure to air pollution as a potential risk factor for autism and ADHD. Environ. Int. 2019, 133 Pt A, 105149. [Google Scholar] [CrossRef]
- Pagliaccio, D.; Herbstman, J.B.; Perera, F.; Tang, D.; Goldsmith, J.; Peterson, B.S.; Rauh, V.; Margolis, A.E. Prenatal exposure to polycyclic aromatic hydrocarbons modifies the effects of early life stress on attention and Thought Problems in late childhood. J. Child Psychol. Psychiatry 2020, 61, 1253–1265. [Google Scholar] [CrossRef] [PubMed]
- McGuinn, L.A.; Bellinger, D.C.; Colicino, E.; Coull, B.A.; Just, A.C.; Kloog, I.; Osorio-Valencia, E.; Schnaas, L.; Wright, R.J.; Téllez-Rojo, M.M.; et al. Prenatal PM2.5 exposure and behavioral development in children from Mexico City. Neurotoxicology 2020, 81, 109–115. [Google Scholar] [PubMed]
- Shih, P.; Huang, C.-C.; Pan, S.-C.; Chiang, T.-L.; Guo, Y.L. Hyperactivity disorder in children related to traffic-based air pollution during pregnancy. Environ. Res. 2020, 188, 109588. [Google Scholar] [CrossRef]
- Peterson, B.S.; Bansal, R.; Sawardekar, S.; Nati, C.; Elgabalawy, E.R.; Hoepner, L.A.; Garcia, W.; Hao, X.; Margolis, A.; Perera, F.; et al. Prenatal exposure to air pollution is associated with altered brain structure, function, and metabolism in childhood. J. Child Psychol. Psychiatry 2022, 63, 1316–1331. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.C.; Chen, W.T.; Su, S.H.; Jung, C.R.; Hwang, B.F. PM2. 5 exposure and incident attention-deficit/hyperactivity disorder during the prenatal and postnatal periods: A birth cohort study. Environ. Res. 2022, 214, 113769. [Google Scholar] [CrossRef]
- Liu, B.; Fang, X.; Strodl, E.; He, G.; Ruan, Z.; Wang, X.; Liu, L.; Chen, W. Fetal Exposure to Air Pollution in Late Pregnancy Significantly Increases ADHD-Risk Behavior in Early Childhood. Int. J. Environ. Res. Public Health 2022, 19, 10482. [Google Scholar] [CrossRef]
- European Environmental Agency. Unequal Exposure and Unequal Impacts: Social Vulnerability to Air Pollution, Noise and Extreme Temperatures in Europe; Publications Office of the European Union: Copenhagen, Denmark, 2019. [Google Scholar] [CrossRef]
- Russell, A.E.; Ford, T.; Russell, G. Socioeconomic Associations with ADHD: Findings from a Mediation Analysis. PLoS ONE 2015, 10, e0128248. [Google Scholar] [CrossRef]
- Ma, Q.; Wang, T.; Liu, C.; He, H.; Wang, Z.; Wang, W.; Liang, Y. SO2 initiates the efficient conversion of NO2 to HONO on MgO surface. Environ. Sci. Technol. 2017, 51, 3767–3775. [Google Scholar] [CrossRef] [PubMed]
- Klepac, P.; Locatelli, I.; Korošec, S.; Künzli, N.; Kukec, A. Ambient air pollution and pregnancy outcomes: A comprehensive review and identification of environmental public health challenges. Environ. Res. 2018, 167, 144–159. [Google Scholar] [CrossRef] [PubMed]
- Muoth, C.; Aengenheister, L.; Kucki, M.; Wick, P.; Buerki-Thurnherr, T. Nanoparticle transport across the placental barrier: Pushing the field forward! Nanomedicine 2016, 11, 941–957. [Google Scholar] [CrossRef]
- Banaschewski, T.; Becker, K.; Döpfner, M.; Holtmann, M.; Rösler, M.; Romanos, M. Attention-deficit/hyperactivity disorder: A current overview. Dtsch. Ärzteblatt Int. 2017, 114, 149. [Google Scholar]
- Williams, J.; Taylor, E. The evolution of hyperactivity, impulsivity and cognitive diversity. J. R. Soc. Interface 2006, 3, 399–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kian, N.; Samieefar, N.; Rezaei, N. Prenatal risk factors and genetic causes of ADHD in children. World J. Pediatr. WJP 2022, 18, 308–319. [Google Scholar] [CrossRef]
- Braun, M.; Klingelhöfer, D.; Oremek, G.M.; Quarcoo, D.; Groneberg, D.A. Influence of second-hand smoke and prenatal tobacco smoke exposure on biomarkers, genetics and physiological processes in children—An overview in research insights of the last few years. Int. J. Environ. Res. Public Health 2020, 17, 3212. [Google Scholar] [CrossRef]
- Mahlberg, N.; James, M.E.; Bulten, R.; Rodriguez, C.; Kwan, M.; Cairney, J. Investigating the association between exposure to second hand smoke in utero and developmental coordination disorder. Front. Pediatr. 2019, 7, 438. [Google Scholar] [CrossRef] [Green Version]
- Schraufnagel, D.E. The health effects of ultrafine particles. Exp. Mol. Med. 2020, 52, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Dimasuay, K.G.; Boeuf, P.; Powell, T.L.; Jansson, T. Placental Responses to Changes in the Maternal Environment Determine Fetal Growth. Front. Physiol. 2016, 7, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Ha, S.U.; Basnet, R. A Review of Epidemiological Research on Adverse Neurological Effects of Exposure to Ambient Air Pollution. Front. Public Health 2016, 4, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.J.; Cho, J.; Hong, Y.C.; Lee, D.W.; Moon, S.; Park, S.J.; Lee, K.S.; Shin, C.H.; Lee, Y.A.; Kim, B.N.; et al. DNA methylation is associated with prenatal exposure to sulfur dioxide and childhood attention-deficit hyperactivity disorder symptoms. Sci. Rep. 2023, 13, 3501. [Google Scholar] [CrossRef]
- Herting, M.M.; Younan, D.; Campbell, C.E.; Chen, J.C. Outdoor air pollution and brain structure and function from across childhood to young adulthood: A methodological review of brain MRI studies. Front. Public Health 2019, 7, 332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S. Air pollution and neurological development in children. Dev. Med. Child Neurol. 2021, 63, 374–381. [Google Scholar] [CrossRef]
- De Cock, M.; Maas, Y.G.; Van De Bor, M. Does perinatal exposure to endocrine disruptors induce autism spectrum and attention deficit hyperactivity disorders? Review. Acta Paediatr. 2012, 101, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Rivollier, F.; Krebs, M.O.; Kebir, O. Perinatal Exposure to Environmental Endocrine Disruptors in the Emergence of Neurodevelopmental Psychiatric Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1318. [Google Scholar] [CrossRef] [Green Version]
- Meng, Z.; Liu, Y. Cell morphological ultrastructural changes in various organs from mice exposed by inhalation to sulfur dioxide. Inhal. Toxicol. 2007, 19, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Dix-Cooper, L.; Eskenazi, B.; Romero, C.; Balmes, J.; Smith, K.R. Neurodevelopmental performance among school age children in rural Guatemala is associated with prenatal and postnatal exposure to carbon monoxide, a marker for exposure to woodsmoke. Neurotoxicology 2012, 33, 246–254. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year/Location/Design | Participants | Exposure Time | Exposure Measurement and Method | Pollutants | ADHD Symptoms and Diagnosis | Covariates | Results |
|---|---|---|---|---|---|---|---|
| Perera et al. (2012) USA Cohort [51] | 253 children aged 6–7 years | Pregnancy | PAH measured by personal air monitoring of the mothers during pregnancy and DNA adducts specific to benzo[a]pyrene (BaP), a representative PAH, in maternal and cord blood. | PAH | Tool: CBCL/6–18. Method: The questionnaire was completed by mothers under the guidance of research workers trained in neurodevelopmental testing. | Child: sex, prenatal ETS. Mother: gestational age, maternal IQ, maternal education, ethnicity, prenatal demoralization, and age at assessment Family/environment: heating season and home caretaking environment (HOME inventory). | High prenatal PAH exposure was positively associated with symptoms in the CBCL syndromic scales of anxious/depressed and attention problems. |
| Gong et al. (2014) Sweden Cohort [52] | 3426 twins’ parents. Children aged 9 or 12 years | Pregnancy, child’s first year | Air pollution concentrations at residential address during pregnancy of the mother and child‘s first year of life by dispersion model to obtain historical emission database on NOx and PM (PM10). | NOx and PM (PM10) | Tool: children neurodevelopment outcomes measures with A-TAC. Method: a telephone interview was conducted with parents. | Child: gender. Mother: gestational age, birth weight, maternal age at birth and maternal smoking during pregnancy. Family/environment: parity, neighbourhood deprivation index at child’s birth, and socio-economic data (maternal marital status, parental education, family income, and family size). | No clear association was found between air pollutants (NOx and PM10) and during pregnancy and in the first of child’s life and ADHD. |
| Perera et al. (2014) USA Cohort [53] | 233, children aged 9 years | Pregnancy | Prenatal PAH exposure estimated by levels of PAH-DNA adducts in maternal and cord blood collected at delivery. | PAH | Tool: CBCL/6–18 and CPRS–Revised: long version. Method: questionnaires were answered by mothers under the guidance of trained research worker. | Child: gender, child ethnicity, and prenatal ETS. Mother: gestational age, maternal intelligence, maternal education, maternal demoralization score, and maternal ADHD. Family/environment: heating season and home caretaking environment (HOME inventory). | High maternal adducts were positivity associated with the DSM-oriented attention deficit/hyperactivity problems scale on the CBCL, albeit not significant. |
| Fuertes et al. (2016) Germany Cohort [54] | 4745 children aged 10 and 15 years | At birth/pregnancy | NO2, PM10 mass and absorbance assigned at child’s birth, 10- and 15 years home address using land-use regression model. | NO2 and PM (PM10, PM2.5 mass and absorbance | Tool: SDQ parent and self-reported versions. Method: the questionnaire was parent-informed at age of 10 years and self-informed at age of 15 years. | Child: sex. Mother: exact age at follow-up, parental education, maternal age at birth, smoking during pregnancy, second-hand smoke exposure, time spent in front of the screen, time spent outside, and single parent status. Family/environment: parental psychopathology. | Hyperactivity/inattention symptoms at 10 and 15 years were associated with PM2.5 mass and absorbance estimated. |
| Yorifuji et al. (2016) Japan Cohort [55] | 33,911 children at 2.5 and 5.5 age | Pregnancy | Air pollutants measuring throughout stations in Japan database managed by the National Institute for Environmental Studies in Japan during pregnancy of mothers. | SPM, NO2 and SO2 | Tool: national survey including three ADHD questions related to attention, self-regulation, and socially appropriate behaviours at the age of 5.5 years. Methods: items were completed by parents using “yes” or “no” categories. | Child: sex, birth month. Mother: maternal age, maternal education, and maternal smoking habit. Family/environment: parental income at the birth year of the child, type of residential area, per capita taxable income, population density of each municipality, and parity. | Air pollution exposure, in particular SPM, NO2 and SO2, during gestation were positively associated with risk for behavioural problems related to attention and delinquent or aggressive behaviour. |
| Yorifuji et al. (2017) Japan Cohort [56] | 33,911 children at 8 years | Pregnancy | Measured at all general monitoring stations throughout Japan database managed by the National Institute for Environmental Studies in Japan during pregnancy of mothers. | SPM, NO2 and SO2 | Tool: CBCL/4–18, Japanese edition and three questions related to attention problems: (1) Does your child interrupt people? (2) Can your child wait his/her turn during play? (3) Can your child pay attention to the surrounding area when crossing the street? Method: parent-informed questionnaire at child’s 8 years of age. | Child: sex, birth month. Mother: maternal age, maternal education, and maternal smoking habit. Family/environment: parental income at the birth year of the child, type of residential area, per capita taxable income, population density of each municipality, and parity. | Positive association between prenatal traffic-related air pollution exposure, in particular suspended PM, and behavioural developmental delays related to attention, self-regulation and socially appropriate behaviour was found at age 5.5 years. Additionally, observed decreased in self-inhibitory control and poor impulsive control; behaviours associated with ADHD. |
| Forns et al. (2018) European countries (Denmark, Netherlands, Germany, Italy, Spain, Sweden, and France) Cohort [57] | 29,127 children aged 3-10 years | Pregnancy | Air pollutant concentrations measured at participants’ home addresses at birth and during pregnancy, using land-use regression model. | NO2 and PM (PM10, PM2.5, PMcoarse and absorbance | Tool: A-TAC, CBCL/1 ½–5, SDQ parent version and ADHD-DSM-IV list. Method: the questionnaires were completed by parents (A-TAC, CBCL 1 ½–5, SDQ) and by teachers (ADHD-DSM-IV scale). | Child: age, sex, and season of birth. Mother: level of education, age at delivery, country of birth, prenatal smoking, mother’s height, pre-pregnancy weight, body mass index. Family/environment: type of living area. | No association was found with air pollution during pregnancy and ADHD symptoms in children. |
| Perera et al. (2018) USA Cohort [58] | 351 children aged 9 years | Pregnancy | PAH exposure, PAH-DNA adducts were measured in maternal blood at delivery. | PAH | Tool: CBCL/6–18, CPRS—Revised: long version. Method: reported by mothers and under the guidance of trained research worker. | Child: sex, child anxiety and depression symptoms at 9 years old, ethnicity, and nonverbal intelligence (TONI-2). Mother: ethnicity, prenatal ETS, maternal education, gestational age, age at assessment, and maternal ADHD. Family/environment: heating season and home caretaking environment (HOME inventory). | Children with high prenatal PAH exposure (adducts) developed more ADHD symptoms than those with low prenatal PAH exposure. |
| Oudin et al. (2019) Sweden Cohort [59] | >48,000 children | Pregnancy born between 1998–2006 | Concentration of NOx obtained from local sources, such as traffic using Gaussian dispersion model for NOx (AERMOD). | NOx | Tool: None Method: Information about children with ADHD was extracted from public databases. ADHD diagnosis criteria: ICD-10. | Child: sex Mother: parental birth country, potential perinatal and maternal risk factors (maternal smoking, maternal age) Family/environment: socio-economic status (maternal education, family income), distance from psychiatric unit. | No associations were found between prenatal NOx exposure and the risk of developing ADHD. |
| Pagliaccio et al. (2020) USA Cohort [60] | 319 children | 3rd trimester of Pregnancy born between 1998–2006 | Personal air monitoring collected an external measure of exposure to PAH and maternal PAH-DNA adducts were also collected from a smaller subset. | PAH | Tool: CBCL/1½–5 and CBCL/6–18 years, CPRS-Revised, ADHD rating scale IV Method: Questionnaires were completed by parents under guidance of a trained research staff. | Child: sex Mother: gestational age, ethnicity, maternal IQ, maternal years of education. Family/environment: presence of a smoker in the home, quality of the proximal caretaking environment at age 3, and change of residence by age 5. | Children with higher prenatal PAH exposure showed significant association between postnatal ELS and CBCL attention and thought problems T-scores. |
| McGuinn et al. (2020) Mexico Cohort [61] | 539 mother–child pairs | Pregnancy (2nd trimester) | 1 km based satellite-based estimation model. | PM2.5 | Tool: BASC-2 Method: questionnaires were completed by parents. | Child: sex, age. Mother: maternal age at enrolment, years of education, depressive symptoms during pregnancy, and maternal IQ. Family/environment: SES, home caretaking environment (HOME inventory), and season of conception. | An association between prenatal first trimester PM2.5 exposure and increases in the scores of several behavioural subscales, including attention problems and hyperactivity, was observed. |
| Shih et al. (2020) Taiwan Cohort [62] | 16,376 mother–infant pairs. Children aged 8 years | Pregnancy | Air pollution data retrieved from fixed-site stations using nondispersive infrared spectroscopy for NO, NO2, NOx, CO, SO2; beta-ray attenuation for PM. | NO, NO2, NOx, SO2, PM (PM10 or less) | Tool: none Method: data extracted from Taiwan National Birth Registry from 2005. ADHD diagnosis criteria: not specified. Parents were asked for previous clinical diagnosis. | Child: sex, birth in summer (June–August). Mother: maternal age, delivery method. Family/environment: urban or rural residence, annual household income. | The occurrence of hyperactivity was significantly related to prenatal nitrogen oxide (NOx), but not to particulate matter 10 μm or less in diameter or SO2. Further analysis to separate effects by nitrogen dioxide (NO2) and/or nitric oxide (NO) showed that only NO was significantly related to hyperactivity. |
| Peterson et al. (2022) USA Cohort [63] | 332 children aged 6–14 years | third trimester of pregnancy. | PM2.5 exposure measured for each day of pregnancy using spatiotemporal exposure models at home addresses; PAH exposure measured using personal air monitoring of the mothers over a 48 h period in the third trimester of pregnancy that collected vapours and particles ≥2.5 μg in diameter on a quartz microfiber filter. | PM2.5, PAH | Tool: ADHD severity Rating Scale. Method: children completed a detailed neuropsychological assessment at the time of MRI scanning, and mothers reported child’s social and emotional functioning. | Child: sex, child handedness. Mother: maternal ethnicity and maternal education. Family/environment: material hardship and quality of home environment. | Prenatal exposure to PAH and PM2.5 were found not significantly associated with any of the behavioural outcomes, ADHD severity or anxiety severity. |
| Chang et al. (2022) China Cohort [64] | 425,736 children aged 5 years | Pregnancy | 1 km based satellite-based estimation model. | PM2.5 | Tool: none Method: data extracted from Taiwan National Birth Registry from 2004–2011. ADHD diagnosis criteria: ICD-9-CM. | Child: sex, birth weight, preterm birth, iron deficiency anaemia, asthma, atopic eczema, allergic rhinitis. Mother: maternal age at delivery, anaemia, heart disease, chronic diabetes, gestational diabetes mellitus, polyhydramnios and oligohydramnios, chronic hypertension, gestational hypertension, preeclampsia, maternal smoke, and drug use. Family/environment: SES. | The hazard ratio (HR) of ADHD was significantly associated with a 10 μg/m3 increase in PM2.5 during the first trimester and increased at PM2.5 over 16 μg/m3. |
| Liu et al. (2022) China Cohort [65] | 26,052 children aged 3 years | Pregnancy | Air pollutants measured using land-use random forest (LURF) model collected from 57 monitoring stations. | SO2, NO2, CO, O3, PM2.5, PM10 | Tool: CPRS-48 Method: questionnaires were completed by parents. | Child: sex, age, average daily sleep duration, feeding pattern, and birth weight. Mother: maternal age at birth, delivery way, parity, maternal passive smoking or alcohol consumption during pregnancy, multivitamins, folic acid or calcium supplementation during pregnancy, and gestational diseases. Family/environment: paternal education and age at birth, family income, parent–child interactive activities, number of persons in house, prenatal household air pollution conditions (fumes from cooking, ETS, home renovation, mosquito coils, and burning of incense indoors), ETS, and monthly mean ambient temperature during first three years of age. | An association was found between air pollutants NO2, PM10, PM2.5 and hyperactivity. Moreover, the risk of hyperactivity significantly increased with 10 μg/m3 exposure from 7th month of pregnancy to 4th month after birth and peak was noticed at 9th month of pregnancy. However, no significant relation observed for air pollutants CO, O3, and SO2 and child hyperactivity. |
| Paper | Study Design | Selection (Max 4 Stars) | Comparability (Max 2 Stars) | Outcome (Max 3 Stars) | Total Score |
|---|---|---|---|---|---|
| [51] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [52] | Cohort | ★ ★ ★ | ★ ★ | ★ ★ | 7/9 |
| [53] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [54] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ ★ | 8/9 |
| [55] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [56] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [57] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ ★ | 8/9 |
| [58] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [59] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ ★ ★ | 9/9 |
| [60] | Cohort | ★ ★ ★ ★ | ★ ★ | ★ | 7/9 |
| [61] | Cohort | ★ ★ ★ | ★ ★ | ★ | 6/9 |
| [62] | Cohort | ★ ★ ★ ★ | ★★ | ★ ★★ | 9/9 |
| [63] | Cohort | ★ ★ ★ ★ | ★ | ★ ★ | 7/9 |
| [64] | Cohort | ★ ★ ★ ★ | ★★ | ★ ★★ | 9/9 |
| [65] | Cohort | ★ ★ ★ ★ | ★★ | ★ | 7/9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaur, S.; Morales-Hidalgo, P.; Arija, V.; Canals, J. Prenatal Exposure to Air Pollutants and Attentional Deficit Hyperactivity Disorder Development in Children: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 5443. https://doi.org/10.3390/ijerph20085443
Kaur S, Morales-Hidalgo P, Arija V, Canals J. Prenatal Exposure to Air Pollutants and Attentional Deficit Hyperactivity Disorder Development in Children: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(8):5443. https://doi.org/10.3390/ijerph20085443
Chicago/Turabian StyleKaur, Sharanpreet, Paula Morales-Hidalgo, Victoria Arija, and Josefa Canals. 2023. "Prenatal Exposure to Air Pollutants and Attentional Deficit Hyperactivity Disorder Development in Children: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 8: 5443. https://doi.org/10.3390/ijerph20085443