“Smartphone Apps Are Cool, But Do They Help Me?”: A Qualitative Interview Study of Adolescents’ Perspectives on Using Smartphone Interventions to Manage Nonsuicidal Self-Injury

 , ,
, , {kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Data Collection
2.3. Data Analysis
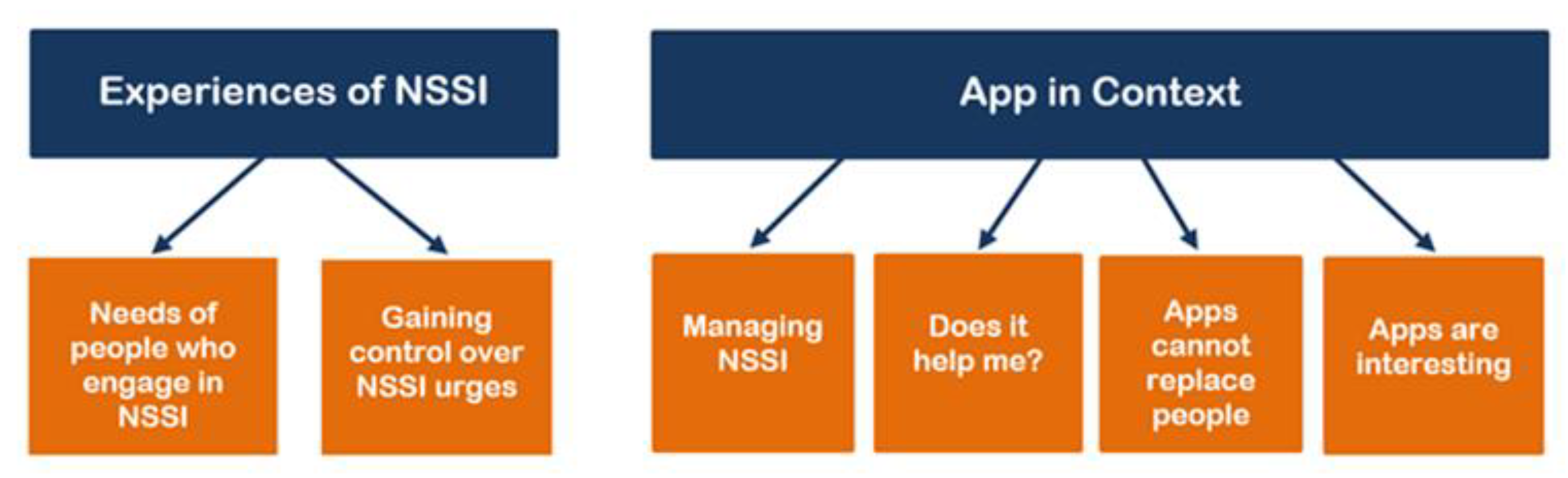
3. Results
3.1. Experiences of NSSI
3.1.1. The Needs of People Who Engage in NSSI
P14: “Ok. So, it mostly arises from the situation that triggered that, are the situations where I say: ‘Yes, you are a disappointment’, so I say it to myself, that I am a disappointment and need to be punished for that, so ‘for this mistake you need to be punished’ and I accept that. And well, that is how it is and then I did it.”
P10: “I mean obviously, like covering scars and like when people see scars like they get freaked out and they start asking questions, so that’s obviously something that I try to avoid.”
P13: “For me it simply became a part of my life/…/. It is also difficult to stop with it, as it is so much inside of my everyday life.”
I: “And what do you need, when you have the feeling you want to injure yourself?”
P5: “Simply to talk, but I have the problem for example, that I cannot say, yes, ‘Hi, I need help, I need someone to talk to.’”
3.1.2. Gaining Control over NSSI Urges
P11: “I do the opposite. I learned that in [the DBT] skills group. I do the opposite of the feeling that I have. For example, if I am sad and feel like crying, I wipe my tears and put a smile on my face.”
I: “How was that before the skills group?”
P11: “Then I would cut myself.”
P9: “I called a hotline and that did not go well/…/And then she repeated all the time that life is beautiful. And then I hang up.”
I: “Ok. And when you called, what would help you more than someone who says that life is beautiful?”
P9: “[To hear] that life can be absolutely crap.”
I: Do you try to distract yourself from self-injuring?
P3: Often.
I: How do you do this?
P3: It depends on where I am./…/At home drawing, music, series or a book. In school, nothing works for me anyways.
3.2. App in Context
3.2.1. Managing NSSI
P9: “So, with me it is so, I cannot think clearly in the situation, to solve problems is then not even an option, it is the feeling of not being able to do anything, that leads to it.”
P14: “If there would be a button that can do it—to help immediately. That would be for me a total rescue./…/It also depends on umm the degree, how severely one is affected by self-injury. There are some, who can resist it and some who really cannot resist it./…/And that one would before it comes that far, that one would get an immediate help.”
I: “Do you have another idea, about an app?”
P2: “Well, perhaps so that you can get into contact with others, can somehow talk, because there often are unfamiliar people, with unfamiliar people it is often easier to talk compared to those that know you, those with whom you are together the whole day. Perhaps like a chat, so that a lot of people can write with each other, like a group.”
I: “Ok. And who would be the people, are these your peers or older or adults?”
P2: “Well, adults that have a clue about it, that how I…”
I: “So, professionals.”
P2: “Yes, rather professionals.”
I: “So not peers, but…”
P2: “No, not that, because that can go wrong, you never know.”
3.2.2. Does It Help Me?
P11: “What would I insert into it? That you first know when you the whole time only feel so so sad, that you know why are you sad./…/I would insert something about me inside. For example, what is my name and how I live. No clue, I do not know, but first tell a bit about myself.”
I: “Which rewards should an app have that it keeps you motivated to use it?”
P8: “Only that it helps, that is actually the only thing.”
3.2.3. Apps Cannot Replace People
P14: “So, I know many apps, I don’t know, how my app would look like, but from what I’ve seen, there are these AI, these fake chats, where one can write into and one can talk with a robot, so that one does not feel alone or something like that. It can be good for some people, but for the others, it can be quite disappointing to notice, that one does not talk with a person. So, it has a different feeling to it. One knows exactly what is human and what is not human.”
I: “How do you use the Internet to feel better?”
P15: “/…/At the moment not at all, because I prefer to talk with people who I know, to talk about it in person. Mostly I then meet my friends and talk with them.”
3.2.4. Apps Are Interesting
P10: “Yeah, I mean, your phone, definitely I mean, I guess everyone has like their music on their phone and like games or different chats or like social media, so, yeah, so I think that’s something that is like since it’s always like attached to you, you can use it to actually benefit you in that way.”
P1: “It could be like a game. So that when you… Or one should take a photo of their hand if they injured themselves or not. And you log that in. Like a photo album. Yes. Like a photo album where you take a photo of your hand every day whether you injured yourself or not. And then at the end of the month you receive an award or so. Or, I don’t know, a voucher or something like that.”
P2: “I cannot imagine it [how it would look like]. I found the idea interesting, that is why I do this [the interview]. It would be cool if there is something like that.”
P13: “Helpful, actually [referring to the interview experience]. So, I find this with the apps cool, that you think about some things and also reflect again about these strategies, if you could use them.”
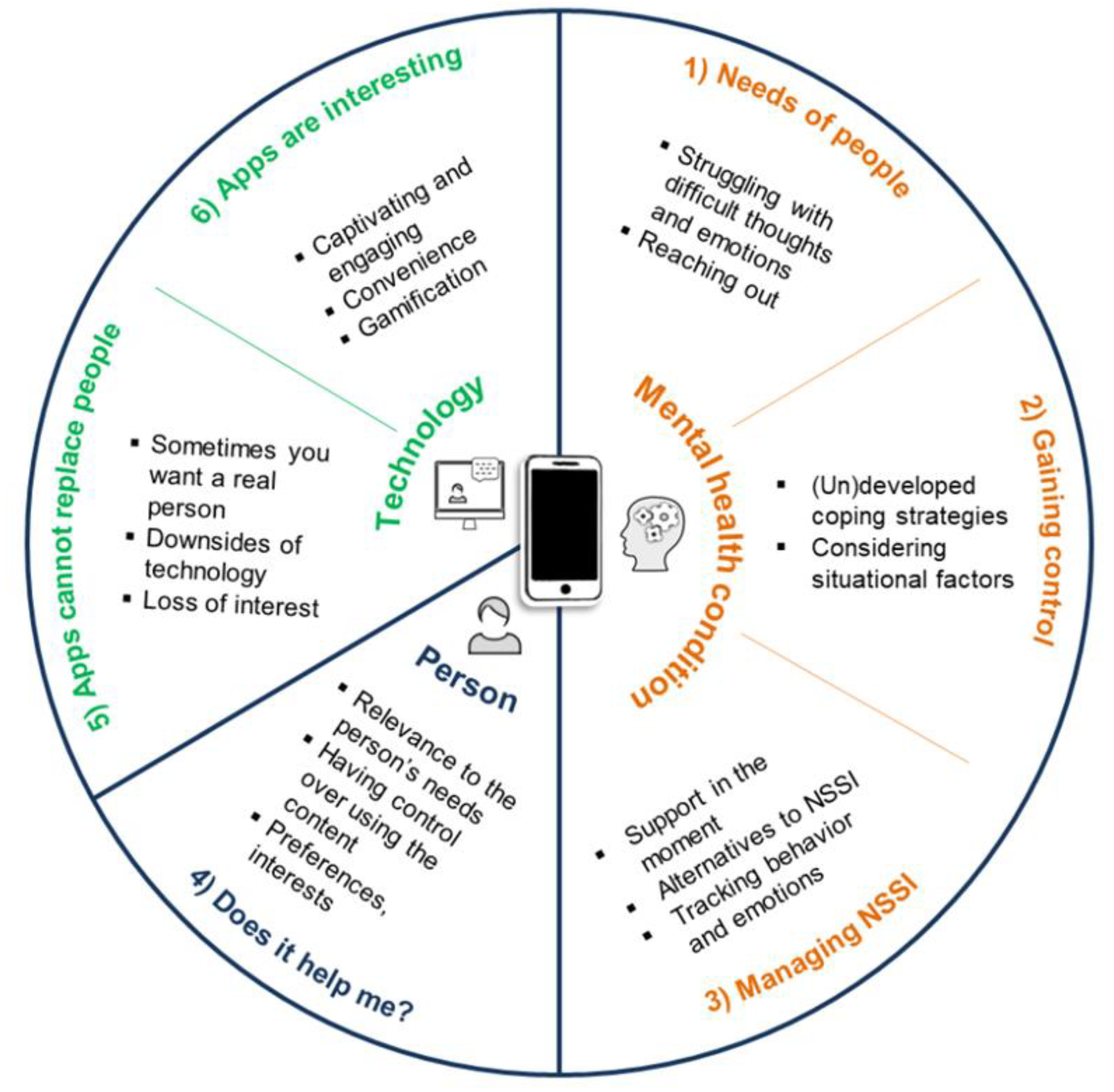
3.3. Framework for Designing Digital Mental Health Interventions Derived from the Context of NSSI
4. Discussion
4.1. General Discussion
4.2. Design Implications for Digital Interventions
4.2.1. Context I: Mental Health Condition
4.2.2. Context II: Person
4.2.3. Context III: Technology
4.3. Strengths, Limitations and Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Society for the Study of Self-Injury. What Is Self-Injury? May 2018. Available online: https://itriples.org/about-self-injury/what-is-self-injury (accessed on 10 March 2021).
- Muehlenkamp, J.J.; Claes, L.; Havertape, L.; Plener, P.L. International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Child Adolesc. Psychiatry Ment. Health 2012, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Cipriano, A.; Cella, S.; Cotrufo, P. Nonsuicidal self-injury: A systematic review. Front. Psychol. 2017, 8, 1946. [Google Scholar] [CrossRef] [PubMed]
- Hamza, C.A.; Stewart, S.L.; Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: A review of the literature and an integrated model. Clin. Psychol. Rev. 2012, 32, 482–495. [Google Scholar] [CrossRef]
- Taylor, P.J.; Jomar, K.; Dhingra, K.; Forrester, R.; Shahmalak, U.; Dickson, J.M. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. J. Affect. Disord. 2018, 227, 759–769. [Google Scholar] [CrossRef]
- Fortune, S.; Sinclair, J.; Hawton, K. Help-seeking before and after episodes of self-harm: A descriptive study in school pupils in England. BMC Public Health 2008, 8, 369. [Google Scholar] [CrossRef]
- Hawton, K.; Saunders, K.E.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Rowe, S.L.; French, R.S.; Henderson, C.; Ougrin, D.; Slade, M.; Moran, P. Help-seeking behaviour and adolescent self-harm: A systematic review. Aust. N. Z. J. Psychiatry 2014, 48, 1083–1095. [Google Scholar] [CrossRef] [PubMed]
- Nicol, G.E.; Karp, J.F.; Reiersen, A.M.; Zorumski, C.F.; Lenze, E.J. “What were you before the war?” Repurposing psychiatry during the COVID-19 pandemic. J. Clin. Psychiatry 2020, 81. [Google Scholar] [CrossRef]
- Dyson, M.P.; Hartling, L.; Shulhan, J.; Chisholm, A.; Milne, A.; Sundar, P.; Scott, S.D.; Newton, A.S. A systematic review of social media use to discuss and view deliberate self-harm acts. PLoS ONE 2016, 11, e0155813. [Google Scholar] [CrossRef]
- Lewis, S.P.; Seko, Y. A double-edged sword: A review of benefits and risks of online nonsuicidal self-injury activities. J. Clin. Psychol. 2015, 72, 249–262. [Google Scholar] [CrossRef]
- Lumsden, J. (Ed.) Handbook of Research on User Interface Design and Evaluation for Mobile Technology; IGI Global: Hershey, PA, USA, 2008; pp. 635–656. [Google Scholar] [CrossRef]
- Odgers, C. Smartphones are bad for some teens, not all. Nat. Cell Biol. 2018, 554, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.M.; Lewis, S.P. Mobile apps for self-injury: A content analysis. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 333–337. [Google Scholar] [CrossRef]
- Hooley, J.M.; Fox, K.R.; Wang, S.B.; Kwashie, A.N.D. Novel online daily diary interventions for nonsuicidal self-injury: A randomized controlled trial. BMC Psychiatry 2018, 18, 264. [Google Scholar] [CrossRef]
- Franklin, J.C.; Fox, K.R.; Franklin, C.R.; Kleiman, E.M.; Ribeiro, J.D.; Jaroszewski, A.C.; Hooley, J.M.; Nock, M.K. A brief mobile app reduces nonsuicidal and suicidal self-injury: Evidence from three randomized controlled trials. J. Consult. Clin. Psychol. 2016, 84, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Leigh, S.; Flatt, S. App-based psychological interventions: Friend or foe? Évid. Based Ment. Health 2015, 18, 97–99. [Google Scholar] [CrossRef] [PubMed]
- APA. App Evaluation Model. 2020. Available online: https://www.psychiatry.org/psychiatrists/practice/mental-health-apps/app-evaluation-model (accessed on 10 March 2021).
- Witt, K.; Spittal, M.J.; Carter, G.; Pirkis, J.; Hetrick, S.; Currier, D.; Robinson, J.; Milner, A. Effectiveness of online and mobile telephone applications (‘apps’) for the self-management of suicidal ideation and self-harm: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 297. [Google Scholar] [CrossRef]
- Arshad, U.; Ain, F.U.; Gauntlett, J.; Husain, N.; Chaudhry, N.; Taylor, P.J. A systematic review of the evidence supporting mobile- and internet-based psychological interventions for self-harm. Suicide Life-Threat. Behav. 2019, 50, 151–179. [Google Scholar] [CrossRef] [PubMed]
- Bjureberg, J.; Sahlin, H.; Hedman-Lagerlöf, E.; Gratz, K.L.; Tull, M.T.; Jokinen, J.; Hellner, C.; Ljótsson, B. Extending research on Emotion Regulation Individual Therapy for Adolescents (ERITA) with nonsuicidal self-injury disorder: Open pilot trial and mediation analysis of a novel online version. BMC Psychiatry 2018, 18, 326. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.L.; Hughes, C.D.; Thomas, M.C. The DBT Coach mobile application as an adjunct to treatment for suicidal and self-injuring individuals with borderline personality disorder: A preliminary evaluation and challenges to client utilization. Psychol. Serv. 2016, 13, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Stallard, P.; Porter, J.; Grist, R. A smartphone app (BlueIce) for young people who self-harm: Open phase 1 pre-post trial. JMIR mHealth uHealth 2018, 6, e32. [Google Scholar] [CrossRef]
- Yeager, C.M.; Benight, C.C. If we build it, will they come? Issues of engagement with digital health interventions for trauma recovery. mHealth 2018, 4, 37. [Google Scholar] [CrossRef]
- Mohr, D.C.; Lyon, A.R.; Lattie, E.G.; Reddy, M.; Schueller, S.M. Accelerating digital mental health research from early design and creation to successful implementation and sustainment. J. Med. Internet Res. 2017, 19, e153. [Google Scholar] [CrossRef] [PubMed]
- Doherty, G.; Coyle, D.; Sharry, J. Engagement with online mental health interventions. In Proceedings of the 2012 ACM Annual Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; pp. 1421–1430. [Google Scholar] [CrossRef]
- Hetrick, S.E.; Robinson, J.; Burge, E.; Blandon, R.; Mobilio, B.; Rice, S.M.; Simmons, M.B.; Alvarez-Jimenez, M.; Goodrich, S.; Davey, C.G. Youth codesign of a mobile phone app to facilitate self-monitoring and management of mood symptoms in young people with major depression, suicidal ideation, and self-harm. JMIR Ment. Health 2018, 5, e9. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Nicholas, J.; E Larsen, M.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Évid. Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Kenny, R.; Dooley, B.A.; Fitzgerald, A. Developing mental health mobile apps: Exploring adolescents’ perspectives. Health Inform. J. 2014, 22, 265–275. [Google Scholar] [CrossRef]
- Fleming, T.; Merry, S.; Stasiak, K.; Hopkins, S.; Patolo, T.; Ruru, S.; Latu, M.; Shepherd, M.; Christie, G.; Goodyear-Smith, F. The importance of user segmentation for designing digital therapy for adolescent mental health: Findings from scoping processes. JMIR Ment. Health 2019, 6, e12656. [Google Scholar] [CrossRef]
- Thabrew, H.; Fleming, T.; Hetrick, S.; Merry, S. Co-design of eHealth interventions with children and young people. Front. Psychiatry 2018, 9, 481. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013; p. 5. [Google Scholar]
- Gulliksen, J.; Göransson, B.; Boivie, I.; Blomkvist, S.; Persson, J.; Cajander, Å. Key principles for user-centred systems design. Behav. Inf. Technol. 2003, 22, 397–409. [Google Scholar] [CrossRef]
- Lima, R.S.; Gonçalves, M.F.C. Pesquisa qualitativa de sucesso: Um guia prático para iniciantes. Rev. de Enferm. UFPE Line 2019, 13. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; SAGE: London, UK, 2006; ISBN 9780857029140. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, E.; Sayal, K.; Townsend, E. Functional coping dynamics and experiential avoidance in a community sample with no self-injury vs. non-suicidal self-injury only vs. those with both non-suicidal self-injury and suicidal behaviour. Int. J. Environ. Res. Public Health 2017, 14, 575. [Google Scholar] [CrossRef]
- Grist, R.; Porter, J.; Stallard, P. Acceptability, use, and safety of a mobile phone app (BlueIce) for young people who self-harm: Qualitative study of service users’ experience. JMIR Ment. Health 2018, 5, e16. [Google Scholar] [CrossRef]
- Hawton, K.; Witt, K.G.; Salisbury, T.L.T.; Arensman, E.; Gunnell, D.; Townsend, E.; Van Heeringen, K.; Hazell, P. Interventions for self-harm in children and adolescents. Cochrane Database Syst. Rev. 2015, 12, CD012013. [Google Scholar] [CrossRef]
- Kruzan, K.P.; Whitlock, J. Prevention of nonsuicidal self-injury. In Nonsuicidal Self-Injury: Advances in Research and Practice; Washburn, J.J., Ed.; Routledge: New York, NY, USA; London, UK, 2019; pp. 215–239. [Google Scholar] [CrossRef]
- Hollis, C.; Falconer, C.J.; Martin, J.L.; Whittington, C.; Stockton, S.; Glazebrook, C.; Davies, E.B. Annual research review: Digital health interventions for children and young people with mental health problems—A systematic and meta-review. J. Child Psychol. Psychiatry 2017, 58, 474–503. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.; Wilkes, C.; Rowan, K.; Toledo, A.; Paradiso, A.; Czerwinski, M.; Linehan, M.M. Pocket skills: A conversational mobile web app to support dialectical behavioral therapy. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 21–26 April 2018. [Google Scholar]
- Rodríguez-Blanco, L.; Carballo-Belloso, J.J.; Baca-García, E. Use of Ecological Momentary Assessment (EMA) in Non-Suicidal Self-Injury (NSSI): A systematic review. Psychiatry Res. 2018, 263, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, P.; Bohus, M.; Ebner-Priemer, U.W. Ecological momentary assessment in borderline personality disorder: A review of recent findings and methodological challenges. J. Pers. Disord. 2014, 28, 555–576. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Neff, K. Self-Compassion: An alternative conceptualization of a healthy attitude toward oneself. Self Identit 2003, 2, 85–101. [Google Scholar] [CrossRef]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Wilks, C.R.; Yin, Q.; Zuromski, K.L. User experience affects dropout from internet-delivered dialectical behavior therapy. Telemed. e-Health 2019, 26, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Doherty, G.; Coyle, D.; Matthews, M. Design and evaluation guidelines for mental health technologies. Interact. Comput. 2010, 22, 243–252. [Google Scholar] [CrossRef]
- Bresin, K.; Schoenleber, M. Gender differences in the prevalence of nonsuicidal self-injury: A meta-analysis. Clin. Psychol. Rev. 2015, 38, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.; Vandereycken, W.; Vertommen, H. Self-injury in female versus male psychiatric patients: A comparison of characteristics, psychopathology and aggression regulation. Pers. Individ. Differ. 2007, 42, 611–621. [Google Scholar] [CrossRef]
- Smail-Crevier, R.; Powers, G.; Noel, C.; Wang, J. Health-Related Internet Usage and Design Feature Preference for E-Mental Health Programs Among Men and Women. J. Med. Internet Res. 2019, 21, e11224. [Google Scholar] [CrossRef] [PubMed]
- Stawarz, K.; Preist, C.; Tallon, D.; Wiles, N.; Coyle, D. User Experience of Cognitive Behavioral Therapy Apps for Depression: An Analysis of App Functionality and User Reviews. J. Med. Internet Res. 2018, 20, e10120. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čuš, A.; Edbrooke-Childs, J.; Ohmann, S.; Plener, P.L.; Akkaya-Kalayci, T. “Smartphone Apps Are Cool, But Do They Help Me?”: A Qualitative Interview Study of Adolescents’ Perspectives on Using Smartphone Interventions to Manage Nonsuicidal Self-Injury. Int. J. Environ. Res. Public Health 2021, 18, 3289. https://doi.org/10.3390/ijerph18063289
Čuš A, Edbrooke-Childs J, Ohmann S, Plener PL, Akkaya-Kalayci T. “Smartphone Apps Are Cool, But Do They Help Me?”: A Qualitative Interview Study of Adolescents’ Perspectives on Using Smartphone Interventions to Manage Nonsuicidal Self-Injury. International Journal of Environmental Research and Public Health. 2021; 18(6):3289. https://doi.org/10.3390/ijerph18063289
Chicago/Turabian StyleČuš, Anja, Julian Edbrooke-Childs, Susanne Ohmann, Paul L. Plener, and Türkan Akkaya-Kalayci. 2021. "“Smartphone Apps Are Cool, But Do They Help Me?”: A Qualitative Interview Study of Adolescents’ Perspectives on Using Smartphone Interventions to Manage Nonsuicidal Self-Injury" International Journal of Environmental Research and Public Health 18, no. 6: 3289. https://doi.org/10.3390/ijerph18063289
APA StyleČuš, A., Edbrooke-Childs, J., Ohmann, S., Plener, P. L., & Akkaya-Kalayci, T. (2021). “Smartphone Apps Are Cool, But Do They Help Me?”: A Qualitative Interview Study of Adolescents’ Perspectives on Using Smartphone Interventions to Manage Nonsuicidal Self-Injury. International Journal of Environmental Research and Public Health, 18(6), 3289. https://doi.org/10.3390/ijerph18063289