
Evaluation of Patient No-Shows in a Tertiary Hospital: Focusing on Modes of Appointment-Making and Type of Appointment



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Data Source
2.2. Variables and Measurement
2.2.1. Dependent Variable
2.2.2. Independent Variables
Demographic Characteristics
Appointment Related Characteristics
Practice-Related Characteristics
2.3. Statistical Analysis
3. Results
3.1. Comparison of Characteristics between No-Shows and Show-Ups
3.2. Factors Associated with No-Shows
3.3. The Interaction Term
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, Y.; Hanauer, D.A. Patient no-show predictive model development using multiple data sources for an effective overbooking approach. Appl. Clin. Inform. 2014, 5, 836–860. [Google Scholar]
- Turkcan, A.; Nuti, L.; DeLaurentis, P.C.; Tian, Z.; Daggy, J.; Zhang, L.; Lawley, M.; Sands, L. No-show modeling for adult ambulatory clinics. In Handbook of Healthcare Operations Management; Denton, B.T., Ed.; Springer: New York, NY, USA, 2013; Volume 184, pp. 251–288. ISBN 978-1-4614-5884-5. [Google Scholar]
- DuMontier, C.; Rindfleisch, K.; Pruszynski, J.; Frey, J.J., 3rd. A multi-method intervention to reduce no-shows in an urban residency clinic. Fam. Med. 2013, 45, 634–641. [Google Scholar] [PubMed]
- Partin, M.R.; Burgess, D.J.; Burgess, J.F., Jr.; Gravely, A.; Haggstrom, D.; Lillie, S.E.; Nugent, S.; Powell, A.A.; Shaukat, A.; Walter, L.C.; et al. Organizational predictors of colonoscopy follow-up for positive fecal occult blood test results: An observational study. Cancer Epidemiol. Biomark. Prev. 2015, 24, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.-Y.; Gupta, D. Adaptive appointment systems with patient preferences. Manuf. Serv. Oper. Manag. 2011, 13, 373–389. [Google Scholar] [CrossRef]
- Hu, M.; Xu, X.; Li, X.; Che, T. Managing patients’ no-show behaviour to improve the sustainability of hospital appointment systems: Exploring the conscious and unconscious determinants of no-show behaviour. J. Clean Prod. 2020, 269, 122318. [Google Scholar] [CrossRef]
- Min, D.; Koo, H. No-Show Related Factors for Outpatients at a Hospital. J. Soc. e-Bus. Stu. 2017, 22, 37–49. [Google Scholar] [CrossRef][Green Version]
- Ko, Y.K. The Relationships among Waiting Time, Patient’s Satisfaction, and Revisiting Intention of Outpatients in General Hospital. J. Korean Acad. Nurs. Adm. 2010, 16, 219–228. [Google Scholar] [CrossRef][Green Version]
- Hashim, M.J.; Franks, P.; Fiscella, K. Effectiveness of telephone reminders in improving rate of appointments kept at an outpatient clinic: A randomized controlled trial. J. Am. Board Fam. Pract. 2001, 14, 193–196. [Google Scholar]
- Daggy, J.; Lawley, M.; Willis, D.; Thayer, D.; Suelzer, C.; DeLaurentis, P.C.; Turkcan, A.; Chakraborty, S.; Sands, L. Using no-show modeling to improve clinic performance. Health Inform. J. 2010, 16, 246–259. [Google Scholar] [CrossRef]
- Guzek, L.M.; Fadel, W.F.; Golomb, M.R. A Pilot Study of Reasons and Risk Factors for “No-Shows” in a Pediatric Neurology Clinic. J. Child Neurol. 2015, 30, 1295–1299. [Google Scholar] [CrossRef]
- Kwon, S.T.; Lee, Y.S.; Han, E.; Kim, T.H. Factors Associated with No-show in an Academic Medical Center. Korean Public Health Res. 2015, 41, 29–46. [Google Scholar] [CrossRef]
- Gatrad, A.R. Comparison of Asian and English non-attenders at a hospital outpatient department. Arch. Dis. Child. 1997, 77, 423–426. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Neal, R.D.; Lawlor, D.A.; Allgar, V.; Colledge, M.; Ali, S.; Hassey, A.; Portz, C.; Wilson, A. Missed appointments in general practice: Retrospective data analysis from four practices. Br. J. Gen. Pract. 2001, 51, 830–832. [Google Scholar] [PubMed]
- Weingarten, N.; Meyer, D.L.; Schneid, J.A. Failed appointments in residency practices: Who misses them and what providers are most affected? J. Am. Board Fam. Pract. 1997, 10, 407–411. [Google Scholar]
- Alaeddini, A.; Yang, K.; Reddy, C.; Yu, S. A probabilistic model for predicting the probability of no-show in hospital appointments. Health Care Manag. Sci. 2011, 14, 146–157. [Google Scholar] [CrossRef]
- Blumenthal, D.M.; Singal, G.; Mangla, S.S.; Macklin, E.A.; Chung, D.C. Predicting Non-Adherence with Outpatient Colonoscopy Using a Novel Electronic Tool that Measures Prior Non-Adherence. J. Gen. Intern. Med. 2015, 30, 724–731. [Google Scholar] [CrossRef]
- Kopach, R.; DeLaurentis, P.C.; Lawley, M.; Muthuraman, K.; Ozsen, L.; Rardin, R.; Wan, H.; Intrevado, P.; Qu, X.; Willis, D. Effects of clinical characteristics on successful open access scheduling. Health Care Manag. Sci. 2007, 10, 111–124. [Google Scholar] [CrossRef]
- Lee, V.J.; Earnest, A.; Chen, M.I.; Krishnan, B. Predictors of failed attendances in a multi-specialty outpatient centre using electronic databases. BMC Health Serv. Res. 2005, 5, 51. [Google Scholar] [CrossRef]
- Norris, J.B.; Kumar, C.; Chand, S.; Moskowitz, H.; Shade, S.A.; Willis, D.R. An empirical investigation into factors affecting patient cancellations and no-shows at outpatient clinics. Dec. Support Syst. 2014, 57, 428–443. [Google Scholar] [CrossRef]
- Pesata, V.; Pallija, G.; Webb, A.A. A descriptive study of missed appointments: Families’ perceptions of barriers to care. J. Pediatr. Health Care 1999, 13, 178–182. [Google Scholar] [CrossRef]
- Starkenburg, R.J.; Rosner, F.; Crowley, K. Missed appointments among patients new to a general medical clinic. N. Y. State J. Med. 1988, 88, 473–475. [Google Scholar]
- Vikander, T.; Parnicky, K.; Demers, R.; Frisof, K.; Demers, P.; Chase, N. New-patient no-shows in an urban family practice center: Analysis and intervention. J. Fam. Pract. 1986, 22, 263–268. [Google Scholar]
- Graber, A.; Davidson, P.; Brown, A.; McRae, J.; Woolridge, K. Dropout and relapse during diabetes care. Diabetes Care 1992, 15, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Weinert, C.; Richardson, J. Rural residents’ use of cardiac rehabilitation programs. Public Health Nurs. 1998, 15, 288–296. [Google Scholar] [CrossRef]
- Gucciardi, E. A systematic review of attrition from diabetes education services: Strategies to improve attrition and retention research. Can. J. Diabetes 2008, 32, 53–65. [Google Scholar] [CrossRef]
- Gatrad, A.R. A completed audit to reduce hospital outpatients non-attendance rates. Arch. Dis. Child. 2000, 82, 59–61. [Google Scholar] [CrossRef]
- Sharp, D.J.; Hamilton, W. Non-attendance at general practices and outpatient clinics. BMJ 2001, 323, 1081–1082. [Google Scholar] [CrossRef] [PubMed]
- Topuz, K.; Uner, H.; Oztekin, A.; Yildirim, M.B. Predicting pediatric clinic no-shows: A decision analytic framework using elastic net and Bayesian belief network. Ann. Oper. Res. 2018, 263, 479–499. [Google Scholar] [CrossRef]
- Harvey, H.B.; Liu, C.; Ai, J.; Jaworsky, C.; Guerrier, C.E.; Flores, E.; Pianykh, O. Predicting No-Shows in Radiology Using Regression Modeling of Data Available in the Electronic Medical Record. J. Am. Coll. Radiol. 2017, 14, 1303–1309. [Google Scholar] [CrossRef]
- Hwang, A.S.; Atlas, S.J.; Cronin, P.; Ashburner, J.M.; Shah, S.J.; He, W.; Hong, C.S. Appointment “no-shows” are an independent predictor of subsequent quality of care and resource utilization outcomes. J. Gen. Intern. Med. 2015, 30, 1426–1433. [Google Scholar] [CrossRef]
- Kaplan-Lewis, E.; Percac-Lima, S. No-show to primary care appointments: Why patients do not come. J. Prim. Care Community Health 2013, 4, 251–255. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, T.H.; Kim, J. Association between missed appointment and related factors of patients with cancer in a tertiary hospital. Int. J. Health Plan. Manag. 2018. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for the Western, P. Republic of Korea Health System Review; WHO Regional Office for the Western Pacific: Manila, Philippines, 2015. [Google Scholar]
- Song, Y.J. The South Korean health care system. JMAJ 2009, 52, 206–209. [Google Scholar]
- Ministry of Health and Welfare. 2018 Welfare Services Guidelines; Ministry of Health and Welfare: Sejong, Korea, 2018; p. 37.
- Horsley, B.P.; Lindauer, S.J.; Shroff, B.; Tüfekçi, E.; Abubaker, A.O.; Fowler, C.E.; Maxfield, B.J. Appointment keeping behavior of Medicaid vs non-Medicaid orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 49–53. [Google Scholar] [CrossRef]
- Iben, P.; Kanellis, M.J.; Warren, J. Appointment-keeping behavior of Medicaid-enrolled pediatric dental patients in eastern Iowa. Pediatr. Dent. 2000, 22, 325–329. [Google Scholar]
- Kim, K.H.; Han, S.T.; Kang, H.; Sohn, B. A preventive model to cancel reservation of new patients using the health information data base. JKDAS 2004, 6, 1817–1827. [Google Scholar]
- Hayhurst, C. To Retain New Patients, Give Them an Appointment Stat. Available online: https://www.athenahealth.com/knowledge-hub/financial-performance/retain-new-patients-give-them-appointment-stat (accessed on 12 November 2020).
- Rice, T. The behavioral economics of health and health care. Annu. Rev. Public Health 2013, 34, 431–447. [Google Scholar] [CrossRef] [PubMed]
- DeFife, J.A.; Conklin, C.Z.; Smith, J.M.; Poole, J. Psychotherapy appointment no-shows: Rates and reasons. Psychotherapy 2010, 47, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.; Walley, J.; Katabira, E.; Muchuro, S.; Balidawa, H.; Namagala, E.; Ikoona, E. Clinic Attendance for Medication Refills and Medication Adherence amongst an Antiretroviral Treatment Cohort in Uganda: A Prospective Study. AIDS Res. Treat. 2010, 2010, 872396. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total | Show-Ups | No-Shows | p-Value | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Demographic characteristics | |||||||
| Gender | |||||||
| Female | 667,734 | 53.3 | 628,559 | 94.1 | 39,175 | 5.9 | <0.0001 |
| Male | 584,393 | 46.7 | 546,895 | 93.6 | 37,498 | 6.4 | |
| Age | |||||||
| ≤19 | 173,825 | 13.9 | 161,291 | 92.8 | 12,534 | 7.2 | <0.0001 |
| 20–29 | 78,534 | 6.3 | 73,225 | 93.2 | 5309 | 6.8 | |
| 30–39 | 114,031 | 9.1 | 107,474 | 94.3 | 6557 | 5.8 | |
| 40–49 | 151,203 | 12.1 | 142,957 | 94.6 | 8246 | 5.5 | |
| 50–59 | 220,641 | 17.6 | 208,067 | 94.3 | 12,574 | 5.7 | |
| 60–69 | 249,549 | 19.9 | 235,529 | 94.4 | 14,020 | 5.6 | |
| ≥70 | 264,344 | 21.1 | 246,911 | 93.4 | 17,433 | 6.6 | |
| Region | |||||||
| Seoul | 721,492 | 57.6 | 674,846 | 93.5 | 46,646 | 6.5 | <0.0001 |
| Incheon·Gyeonggi area | 333,993 | 26.7 | 314,404 | 94.1 | 19,589 | 5.9 | |
| Other areas | 196,642 | 15.7 | 186,204 | 94.7 | 10,438 | 5.3 | |
| Types of insurance | |||||||
| National Health Insurance | 1,166,189 | 93.1 | 1,096,750 | 94.1 | 69,439 | 5.9 | <0.0001 |
| Medical Aid | 50,403 | 4.0 | 46,030 | 91.3 | 4373 | 8.7 | |
| Industrial Accident Compensation Insurance and Automobile Insurance | 10,929 | 0.9 | 10,164 | 93.0 | 765 | 7.0 | |
| International Insurance and Private Insurance | 24,606 | 2.0 | 22,510 | 91.5 | 2096 | 8.5 | |
| Appointment related characteristics | |||||||
| Modes of appointment-making | |||||||
| Walk-in | 59,187 | 4.7 | 52,922 | 89.4 | 6265 | 10.6 | <0.0001 |
| Follow-up | 1,178,836 | 94.1 | 1,109,091 | 94.1 | 69,745 | 5.9 | |
| Online/telephone | 14,104 | 1.1 | 13,441 | 95.3 | 663 | 4.7 | |
| Time of visit | |||||||
| 9:00–11:00 | 100,503 | 8.0 | 91,784 | 91.3 | 8719 | 8.7 | <0.0001 |
| <9:00 | 327,124 | 26.1 | 310,519 | 94.9 | 16,605 | 5.1 | |
| 11:00–13:00 | 269,994 | 21.6 | 253,514 | 93.9 | 16,480 | 6.1 | |
| 13:00–15:00 | 226,907 | 18.1 | 213,868 | 94.3 | 13,039 | 5.7 | |
| 15:00–17:00 | 236,243 | 18.9 | 221,798 | 93.9 | 14,445 | 6.1 | |
| ≥17:00 | 91,356 | 7.3 | 83,971 | 91.9 | 7385 | 8.1 | |
| Day of week | |||||||
| Monday | 255,286 | 20.4 | 240,098 | 94.1 | 15,188 | 5.9 | <0.0001 |
| Tuesday | 237,566 | 19.0 | 223,731 | 94.2 | 13,835 | 5.8 | |
| Wednesday | 226,738 | 18.1 | 213,466 | 94.2 | 13,272 | 5.8 | |
| Thursday | 266,325 | 21.3 | 250,448 | 94.0 | 15,877 | 6.0 | |
| Friday | 222,594 | 17.8 | 208,281 | 93.6 | 14,313 | 6.4 | |
| Weekend (Saturday and Sunday) | 43,618 | 3.5 | 39,430 | 90.4 | 4188 | 9.6 | |
| Lead time | |||||||
| Less than 8 days | 231,134 | 18.5 | 212,432 | 91.9 | 18,702 | 8.1 | <0.0001 |
| 8–14 days | 158,800 | 12.7 | 147,811 | 93.1 | 10,989 | 6.9 | |
| 15–21 days | 108,705 | 8.7 | 102,969 | 94.7 | 5736 | 5.3 | |
| 22–28 days | 74,548 | 6.0 | 70,371 | 94.4 | 4177 | 5.6 | |
| 29–56 days | 200,341 | 16.0 | 187,479 | 93.6 | 12,862 | 6.4 | |
| 57–84 days | 102,606 | 8.2 | 95,705 | 93.3 | 6901 | 6.7 | |
| More than 85 days | 375,993 | 30.0 | 358,687 | 95.4 | 17,306 | 4.6 | |
| Practice-related characteristics | |||||||
| Types of visit * | |||||||
| A | 79,990 | 6.4 | 78,914 | 98.7 | 1076 | 1.3 | <0.0001 |
| B | 1,015,836 | 81.1 | 949,339 | 93.5 | 66,497 | 6.5 | |
| C | 156,301 | 12.5 | 147,201 | 94.2 | 9100 | 5.8 | |
| Types of appointment | |||||||
| Consultation | 1,098,863 | 87.8 | 1,049,756 | 95.5 | 49,107 | 4.5 | <0.0001 |
| Examination | 15,831 | 1.3 | 11,059 | 69.9 | 4772 | 30.1 | |
| Treatment and surgery | 137,433 | 11.0 | 114,639 | 83.4 | 22,794 | 16.6 | |
| Department | |||||||
| Internal medicine | 437,833 | 35.0 | 413,638 | 94.5 | 24,195 | 5.5 | <0.0001 |
| Surgery department | 200,870 | 16.0 | 188,408 | 93.8 | 12,462 | 6.2 | |
| OBGYN | 64,137 | 5.1 | 61,235 | 95.5 | 2902 | 4.5 | |
| Pediatrics | 117,329 | 9.4 | 110,659 | 94.3 | 6670 | 5.7 | |
| Ophthalmology | 61,496 | 4.9 | 58,192 | 94.6 | 3304 | 5.4 | |
| Otolaryngology | 40,031 | 3.2 | 37,329 | 93.3 | 2702 | 6.7 | |
| Dermatology | 35,508 | 2.8 | 32,918 | 92.7 | 2590 | 7.3 | |
| Urology | 50,391 | 4.0 | 47,252 | 93.8 | 3139 | 6.2 | |
| Neuropsychiatry | 33,436 | 2.7 | 31,927 | 95.5 | 1509 | 4.5 | |
| Others | 211,096 | 16.9 | 193,896 | 91.9 | 17,200 | 8.1 | |
| Doctor’s position | |||||||
| Professional position | 1,142,108 | 91.2 | 1,072,506 | 93.9 | 69,602 | 6.1 | <0.0001 |
| Training position | 82,800 | 6.6 | 77,488 | 93.6 | 5312 | 6.4 | |
| Fellow position | 27,219 | 2.2 | 25,460 | 93.5 | 1759 | 6.5 | |
| Major diagnosis | |||||||
| A00-B99 | 12,821 | 1.0 | 11,866 | 92.6 | 955 | 7.4 | <0.0001 |
| C00-D48 | 159,483 | 12.7 | 146,806 | 92.1 | 12,677 | 7.9 | |
| D50-D89 | 38,148 | 3.0 | 35,573 | 93.3 | 2575 | 6.7 | |
| E00-E90 | 48,549 | 3.9 | 45,619 | 94.0 | 2930 | 6.0 | |
| F00-F99 | 26,763 | 2.1 | 25,757 | 96.2 | 1006 | 3.8 | |
| G00-G99 | 56,838 | 4.5 | 50,395 | 88.7 | 6443 | 11.3 | |
| H00-H59 | 41,301 | 3.3 | 38,061 | 92.2 | 3240 | 7.8 | |
| I00-I99 | 81,548 | 6.5 | 76,575 | 93.9 | 4973 | 6.1 | |
| J00-J99 | 24,509 | 2.0 | 22,515 | 91.9 | 1994 | 8.1 | |
| K00-K93 | 34,537 | 2.8 | 31,887 | 92.3 | 2650 | 7.7 | |
| L00-L99 | 19,304 | 1.5 | 18,148 | 94.0 | 1156 | 6.0 | |
| M00-M99 | 54,041 | 4.3 | 49,662 | 91.9 | 4379 | 8.1 | |
| N00-N99 | 46,461 | 3.7 | 41,779 | 89.9 | 4682 | 10.1 | |
| O00-P96 | 7025 | 0.6 | 6339 | 90.2 | 686 | 9.8 | |
| Q00-Q99 | 17,635 | 1.4 | 16,263 | 92.2 | 1372 | 7.8 | |
| R00-R99 | 56,723 | 4.5 | 51,220 | 90.3 | 5503 | 9.7 | |
| S00-T98 | 19,544 | 1.6 | 17,546 | 89.8 | 1998 | 10.2 | |
| U00-Z99 | 47,544 | 3.8 | 44,906 | 94.5 | 2638 | 5.5 | |
| No diagnosis | 459,353 | 36.7 | 444,537 | 96.8 | 14,816 | 3.2 | |
| Variables | Model 1 | Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Demographic characteristics | ||||||||
| Gender | ||||||||
| Female | ref | |||||||
| Male | 1.05 | 1.03 | 1.08 | <.0001 | 1.05 | 1.03 | 1.08 | <0.0001 |
| Age | ||||||||
| ≤19 | ref | |||||||
| 20–29 | 1.05 | 0.99 | 1.11 | 0.1055 | 0.98 | 0.93 | 1.04 | 0.5295 |
| 30–39 | 0.91 | 0.86 | 0.97 | 0.0021 | 0.84 | 0.80 | 0.90 | <0.0001 |
| 40–49 | 0.81 | 0.76 | 0.85 | <.0001 | 0.74 | 0.70 | 0.79 | <0.0001 |
| 50–59 | 0.80 | 0.76 | 0.84 | <.0001 | 0.73 | 0.69 | 0.77 | <0.0001 |
| 60–69 | 0.78 | 0.74 | 0.82 | <.0001 | 0.71 | 0.67 | 0.75 | <0.0001 |
| ≥70 | 0.92 | 0.87 | 0.97 | 0.0026 | 0.84 | 0.79 | 0.89 | <0.0001 |
| Region | ||||||||
| Seoul | ref | |||||||
| Incheon·Gyeonggi area | 0.97 | 0.94 | 0.99 | 0.0136 | 0.97 | 0.94 | 1.00 | 0.0359 |
| Other areas | 0.97 | 0.94 | 1.00 | 0.0701 | 0.98 | 0.95 | 1.01 | 0.1947 |
| Types of insurance | ||||||||
| National Health Insurance | ref | |||||||
| Medical Aid | 1.29 | 1.21 | 1.37 | <.0001 | 1.29 | 1.21 | 1.37 | <0.0001 |
| Industrial Accident Compensation Insurance and Automobile Insurance | 0.96 | 0.82 | 1.13 | 0.6450 | 0.95 | 0.82 | 1.11 | 0.5459 |
| International Insurance and Private Insurance | 1.45 | 1.35 | 1.55 | <.0001 | 1.35 | 1.26 | 1.45 | <0.0001 |
| Appointment related characteristics | ||||||||
| Time of visit | ||||||||
| 9:00–11:00 | ref | |||||||
| <9:00 | 1.00 | 0.95 | 1.06 | 0.9182 | 0.98 | 0.93 | 1.04 | 0.5394 |
| 11:00–13:00 | 1.16 | 1.12 | 1.20 | <.0001 | 1.15 | 1.12 | 1.19 | <0.0001 |
| 13:00–15:00 | 1.10 | 1.06 | 1.14 | <.0001 | 1.09 | 1.05 | 1.13 | <0.0001 |
| 15:00–17:00 | 1.18 | 1.14 | 1.22 | <.0001 | 1.17 | 1.13 | 1.21 | <0.0001 |
| ≥17:00 | 1.33 | 1.27 | 1.39 | <.0001 | 1.31 | 1.25 | 1.37 | <0.0001 |
| Day of week | ||||||||
| Monday | ref | |||||||
| Tuesday | 0.96 | 0.92 | 0.99 | 0.0121 | 0.96 | 0.93 | 0.99 | 0.0236 |
| Wednesday | 0.97 | 0.94 | 1.01 | 0.1394 | 0.97 | 0.94 | 1.01 | 0.1742 |
| Thursday | 0.98 | 0.95 | 1.02 | 0.3351 | 0.99 | 0.95 | 1.02 | 0.4626 |
| Friday | 1.03 | 0.99 | 1.07 | 0.0963 | 1.03 | 1.00 | 1.07 | 0.0773 |
| Weekend (Saturday and Sunday) | 1.43 | 1.35 | 1.53 | <.0001 | 1.45 | 1.36 | 1.54 | <0.0001 |
| Lead time | ||||||||
| Less than 8 days | ref | |||||||
| 8–14 days | 0.88 | 0.85 | 0.92 | <.0001 | 0.88 | 0.85 | 0.92 | <0.0001 |
| 15–21 days | 0.81 | 0.78 | 0.85 | <.0001 | 0.80 | 0.77 | 0.84 | <0.0001 |
| 22–28 days | 0.88 | 0.84 | 0.93 | <.0001 | 0.88 | 0.83 | 0.92 | <0.0001 |
| 29–56 days | 1.04 | 1.00 | 1.09 | 0.0445 | 1.04 | 1.00 | 1.09 | 0.0470 |
| 57–84 days | 1.05 | 1.00 | 1.10 | 0.0447 | 1.05 | 1.00 | 1.11 | 0.0411 |
| More than 85 days | 0.98 | 0.94 | 1.02 | 0.2422 | 0.96 | 0.92 | 1.00 | 0.0358 |
| Practice-related characteristics | ||||||||
| Types of visit * | ||||||||
| A | ref | |||||||
| B | 1.01 | 0.98 | 1.04 | 0.4891 | 0.95 | 0.93 | 0.98 | 0.0019 |
| C | 0.30 | 0.28 | 0.32 | <.0001 | 0.29 | 0.27 | 0.32 | <0.0001 |
| Department | ||||||||
| Internal medicine | ref | |||||||
| Surgery department | 1.46 | 1.42 | 1.51 | <.0001 | 1.39 | 1.35 | 1.44 | <0.0001 |
| OBGYN | 0.99 | 0.93 | 1.04 | 0.6083 | 0.94 | 0.89 | 0.99 | 0.0312 |
| Pediatrics | 1.14 | 1.07 | 1.21 | <.0001 | 1.02 | 0.96 | 1.08 | 0.5791 |
| Ophthalmology | 1.21 | 1.14 | 1.29 | <.0001 | 1.15 | 1.09 | 1.23 | <0.0001 |
| Otolaryngology | 1.40 | 1.32 | 1.48 | <.0001 | 1.35 | 1.28 | 1.43 | <0.0001 |
| Dermatology | 2.21 | 2.08 | 2.36 | <.0001 | 2.15 | 2.01 | 2.29 | <0.0001 |
| Urology | 1.30 | 1.23 | 1.37 | <.0001 | 1.27 | 1.20 | 1.34 | <0.0001 |
| Neuropsychiatry | 1.59 | 1.45 | 1.74 | <.0001 | 1.58 | 1.44 | 1.73 | <0.0001 |
| Others | 0.67 | 0.64 | 0.71 | <.0001 | 0.71 | 0.68 | 0.74 | <0.0001 |
| Doctor’s position | ||||||||
| Professional position | ref | |||||||
| Training position | 1.24 | 1.19 | 1.29 | <.0001 | 1.26 | 1.21 | 1.31 | <0.0001 |
| Fellow position | 1.16 | 1.09 | 1.24 | <.0001 | 1.18 | 1.11 | 1.26 | <0.0001 |
| Major diagnosis | ||||||||
| C00-D48 | ref | |||||||
| A00-B99 | 0.96 | 0.89 | 1.03 | 0.2576 | 0.94 | 0.87 | 1.01 | 0.0912 |
| D50- D89 | 0.95 | 0.91 | 1.00 | 0.0405 | 0.95 | 0.90 | 0.99 | 0.026 |
| E00-E90 | 0.91 | 0.86 | 0.95 | 0.0001 | 0.88 | 0.84 | 0.93 | <0.0001 |
| F00-F99 | 0.40 | 0.36 | 0.45 | <.0001 | 0.39 | 0.35 | 0.43 | <0.0001 |
| G00-G99 | 1.15 | 1.10 | 1.21 | <.0001 | 1.13 | 1.08 | 1.18 | <0.0001 |
| H00-H59 | 1.14 | 1.08 | 1.21 | <.0001 | 1.13 | 1.07 | 1.19 | <0.0001 |
| I00-I99 | 0.92 | 0.88 | 0.96 | 0.0002 | 0.89 | 0.86 | 0.93 | <0.0001 |
| J00-J99 | 1.11 | 1.05 | 1.18 | 0.0002 | 1.08 | 1.02 | 1.15 | 0.0057 |
| K00-K93 | 1.12 | 1.06 | 1.18 | <.0001 | 1.11 | 1.05 | 1.17 | <0.0001 |
| L00-L99 | 0.39 | 0.36 | 0.43 | <.0001 | 0.39 | 0.35 | 0.43 | <0.0001 |
| M00-M99 | 0.93 | 0.88 | 0.98 | 0.0044 | 0.91 | 0.86 | 0.96 | 0.0002 |
| N00-N99 | 1.07 | 1.02 | 1.13 | 0.0037 | 1.06 | 1.01 | 1.11 | 0.0263 |
| O00-P96 | 1.11 | 1.01 | 1.22 | 0.0370 | 1.06 | 0.96 | 1.16 | 0.2732 |
| Q00-Q99 | 0.92 | 0.86 | 0.98 | 0.0115 | 0.92 | 0.87 | 0.98 | 0.0143 |
| R00-R99 | 1.23 | 1.18 | 1.28 | <.0001 | 1.20 | 1.15 | 1.24 | <0.0001 |
| S00-T98 | 1.06 | 0.99 | 1.13 | 0.1003 | 1.04 | 0.97 | 1.11 | 0.2939 |
| U00-Z99 | 0.88 | 0.85 | 0.92 | <.0001 | 0.88 | 0.84 | 0.92 | <0.0001 |
| No diagnosis | 0.44 | 0.43 | 0.46 | <.0001 | 0.42 | 0.41 | 0.43 | <0.0001 |
| Modes of appointment-making | ||||||||
| Walk-in | ref | ref | ||||||
| Follow-up | 0.86 | 0.82 | 0.91 | <.0001 | 1.36 | 1.24 | 1.49 | <0.0001 |
| Online/telephone | 1.11 | 0.99 | 1.24 | 0.0619 | 1.36 | 1.18 | 1.57 | <0.0001 |
| Types of appointment | ||||||||
| Consultation | ref | ref | ||||||
| Examination | 9.09 | 8.66 | 9.54 | <.0001 | 0.77 | 0.53 | 1.11 | 0.1610 |
| Treatment and surgery | 4.51 | 4.31 | 4.72 | <.0001 | 9.38 | 8.47 | 10.39 | <0.0001 |
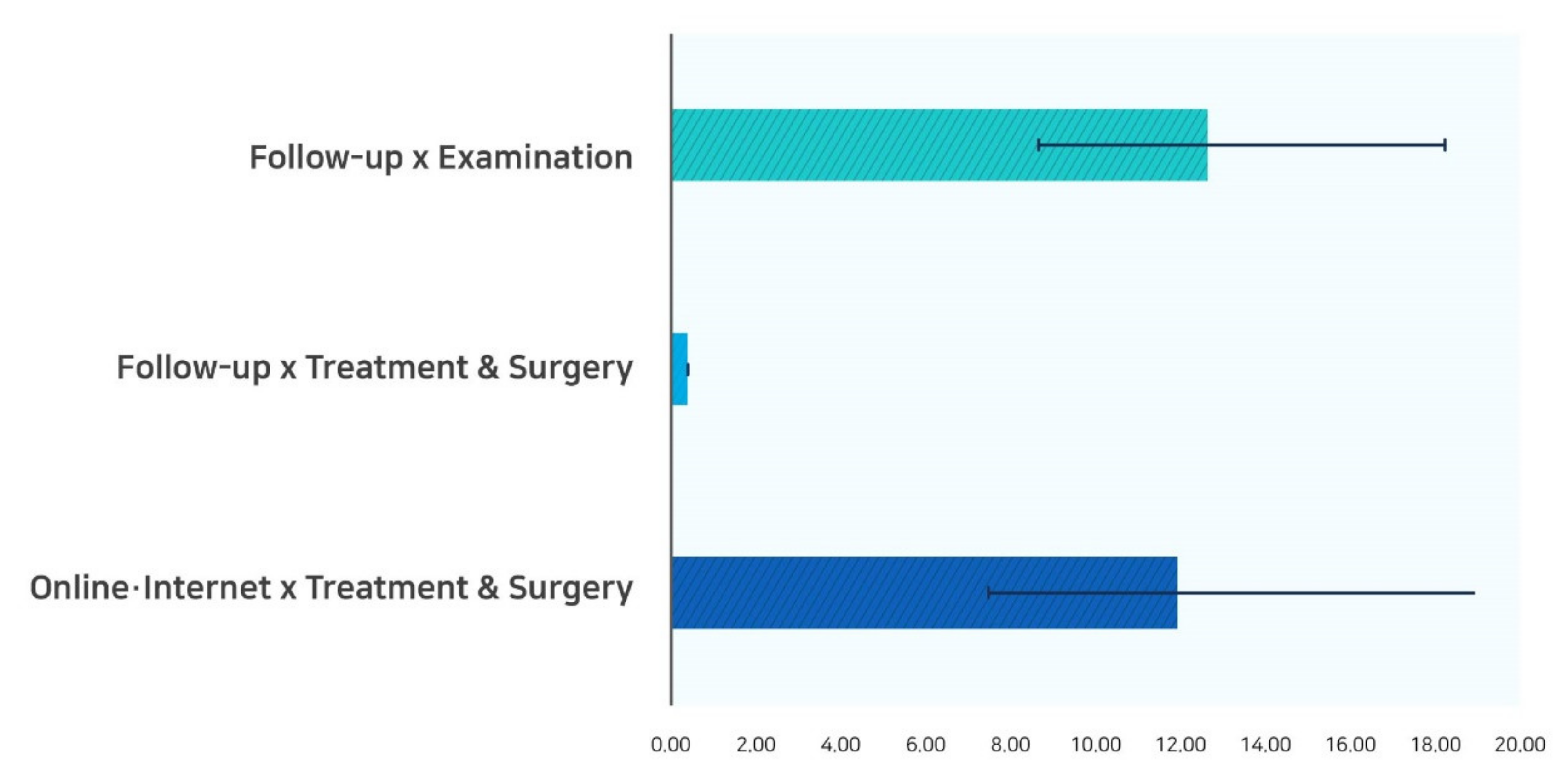
| Modes of appointment-making × Types of appointment | ||||||||
| Follow-up × Examination | 12.59 | 8.67 | 18.27 | <0.0001 | ||||
| Follow-up × Treatment and Surgery | 0.39 | 0.35 | 0.44 | <0.0001 | ||||
| Online/telephone × Treatment and Surgery | 11.89 | 7.45 | 18.99 | <0.0001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suk, M.Y.; Kim, B.; Lee, S.G.; You, C.H.; Hyun Kim, T. Evaluation of Patient No-Shows in a Tertiary Hospital: Focusing on Modes of Appointment-Making and Type of Appointment. Int. J. Environ. Res. Public Health 2021, 18, 3288. https://doi.org/10.3390/ijerph18063288
Suk MY, Kim B, Lee SG, You CH, Hyun Kim T. Evaluation of Patient No-Shows in a Tertiary Hospital: Focusing on Modes of Appointment-Making and Type of Appointment. International Journal of Environmental Research and Public Health. 2021; 18(6):3288. https://doi.org/10.3390/ijerph18063288
Chicago/Turabian StyleSuk, Mi Young, Bomgyeol Kim, Sang Gyu Lee, Chang Hoon You, and Tae Hyun Kim. 2021. "Evaluation of Patient No-Shows in a Tertiary Hospital: Focusing on Modes of Appointment-Making and Type of Appointment" International Journal of Environmental Research and Public Health 18, no. 6: 3288. https://doi.org/10.3390/ijerph18063288
APA StyleSuk, M. Y., Kim, B., Lee, S. G., You, C. H., & Hyun Kim, T. (2021). Evaluation of Patient No-Shows in a Tertiary Hospital: Focusing on Modes of Appointment-Making and Type of Appointment. International Journal of Environmental Research and Public Health, 18(6), 3288. https://doi.org/10.3390/ijerph18063288