
The Order of Draw during Blood Collection: A Systematic Literature Review

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
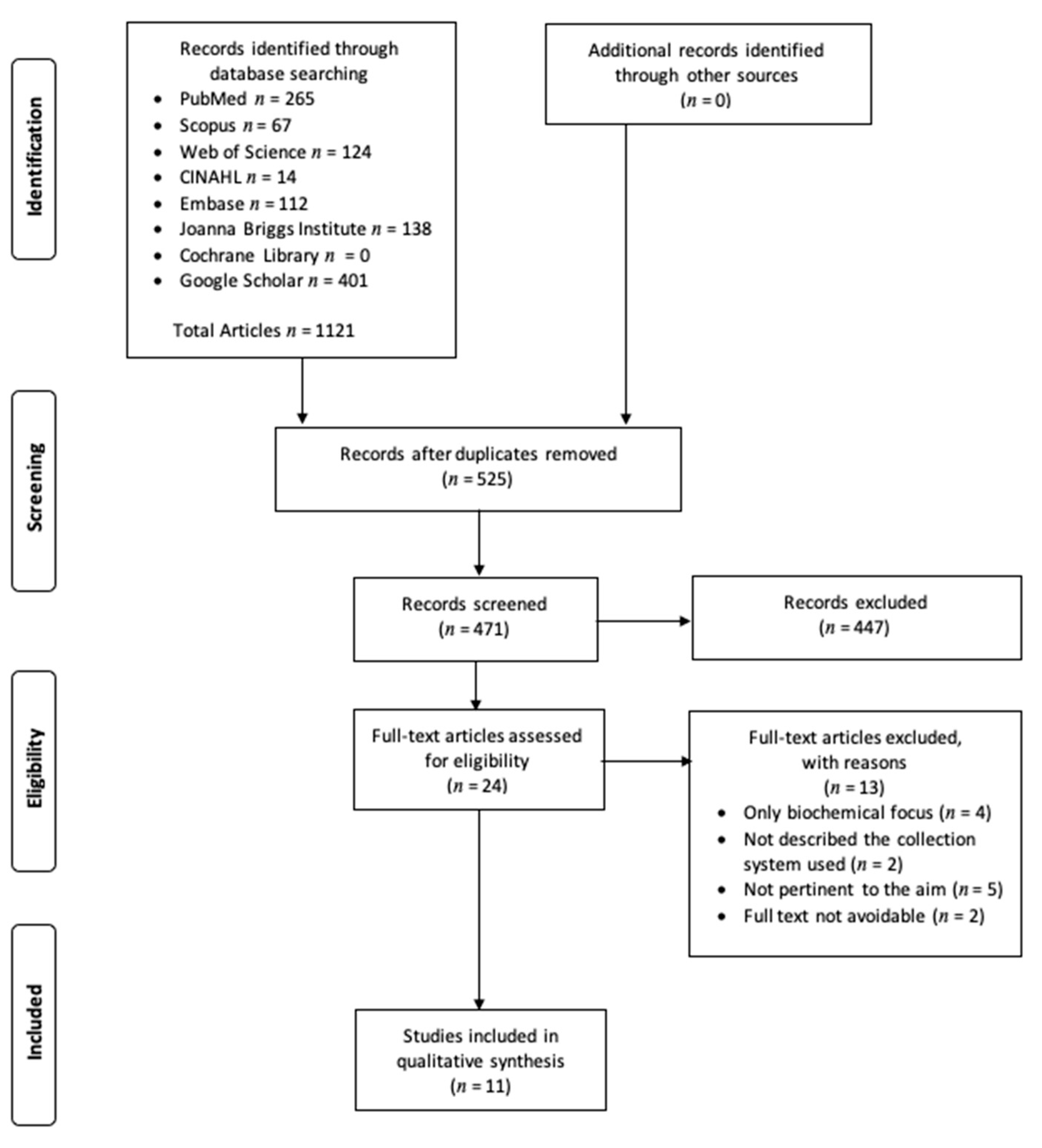
2.4. Search Outcomes
2.5. Quality Appraisal
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Efficacy of Order of Draw
3.4. Negligible Importance of the Order of Draw
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galazzi, A.; Rancati, S.; Milos, R. A survey of accidents during the clinical rotation of students in a nursing degree program. G Ital. Med. Lav. Ergon. 2014, 36, 25–31. [Google Scholar]
- Wiwanitki, V. Types and frequency of preanalytical mistakes in the first Thai ISO 9002:1994 certified clinical laboratory, a 6-month monitoring. BMC Clin. Pathol. 2002, 1, 5. [Google Scholar] [CrossRef]
- Bonini, P.; Plebani, M.; Ceriotti, F.; Rubboli, F. Errors in laboratory medicine. Clin. Chem. 2002, 48, 691–698. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy. Available online: http://whqlibdoc.who.int/publications/2010/9789241599221_eng.pdf (accessed on 28 April 2020).
- Clinical and Laboratory Standards Institute. Procedures for Collection of Diagnostic Blood Specimens by Venipuncture. Approved Standard, 6th ed.; CLSI: Wayne, PA, USA, 2007; pp. H3–A6. [Google Scholar]
- Sun, N.; Knauf, R. Cross contamination solved by technique. ASCP Summ. Rep. 1977, 14, 3. [Google Scholar]
- Calam, R.R.; Cooper, M.H. Recommended "order of draw" for collecting blood specimens into additive-containing tubes. Clin. Chem. 1982, 28, 1399. [Google Scholar] [CrossRef] [PubMed]
- Ernst, D.J.; Calam, R. NCCLS simplifies the order of draw: A brief history. MLO Med. Lab. Obs. 2004, 36, 26–27. [Google Scholar]
- Chadwick, K.; Whitehead, S.J.; Ford, C.; Gama, R. kEDTA Sample Contamination: A Reappraisal. J. Appl. Lab. Med. 2019, 3, 925–935. [Google Scholar] [CrossRef]
- Logie, J.J.; Chaloner, C. A national survey of specimen contamination in the UK. Ann. Clin. Biochem. 2019, 56, 219–227. [Google Scholar] [CrossRef]
- Davidson, D.F. Effects of contamination of blood specimens with liquid potassium-EDTA anticoagulant. Ann. Clin. Biochem. 2002, 39, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, R. Addressing “order of draw” in comparative calcium levels. MLO Med. Lab. Obs. 2001, 33, 6. [Google Scholar]
- Keppel, M.H.; Auer, S.; Lippi, G.; Von Meyer, A.; Cornes, M.; Felder, T.K.; Oberkofler, H.; Mrazek, C.; Haschke-Becher, E.; Cadamuro, J. Heparin and citrate additive carryover during blood collection. Clin. Chem. Lab. Med. 2019, 57, 1888–1896. [Google Scholar] [CrossRef]
- Sulaiman, R.A.; Cornes, M.P.; Whitehead, S.J.; Othonos, N.; Ford, C.; Gama, R. Effect of order of draw of blood samples during phlebotomy on routine biochemistry results. J. Clin. Pathol. 2011, 64, 1019–1020. [Google Scholar] [CrossRef]
- Cornes, M.P.; Davidson, F.; Darwin, L.; Gay, C.; Redpath, M.; Waldron, J.L.; Ford, C.; Gama, R. Multi-centre observational study of spurious hyperkalaemia due to EDTA contamination. Clin. Lab. 2010, 56, 597–599. [Google Scholar] [PubMed]
- Cornes, M.; Van Dongen-Lases, E.; Grankvist, K.; Ibarz, M.; Kristensen, G.; Lippi, G.; Nybo, M.; Simundic, A.M.; Working Group for Preanalytical Phase (WG-PRE), European Federation of Clinical Chemistry and Laboratory Medicine (EFLM). Order of blood draw: Opinion Paper by the European Federation for Clinical Chemistry and Laboratory Medicine (EFLM) Working Group for the Preanalytical Phase (WG-PRE). Clin. Chem. Lab. Med. 2017, 55, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 12 August 2020).
- Asif, U.; Whitehead, S.J.; Ford, C.; Gama, R. Preanalytical potassium EDTA sample contamination: Open versus closed phlebotomy systems. Ann. Clin. Biochem. 2019, 56, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Indevuyst, C.; Schuermans, W.; Bailleul, E.; Meeus, P. The order of draw: Much ado about nothing? Int. J. Lab. Hematol. 2015, 37, 50–55. [Google Scholar] [CrossRef]
- Cornes, M.R.; Sulaiman, R.A.; Whitehead, S.J.; Othonos, N.; Ford, C.; Gama, R. Incorrect order of draw of blood samples does not cause potassium EDTA sample contamination. Br. J. Biomed. Sci. 2012, 69, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.; Lima-Oliveira, G.; Brocco, G.; Danese, E.; Guidi, G.C.; Lippi, G. The order of draw: Myth or science? Clin. Chem. Lab. Med. 2013, 51, 2281–2285. [Google Scholar] [CrossRef]
- Cadamuro, J.; Felder, T.K.; Oberkofler, H.; Mrazek, C.; Wiedemann, H.; Haschke-Becher, E. Relevance of EDTA carryover during blood collection. Clin. Chem. Lab. Med. 2015, 53, 1271–1278. [Google Scholar] [CrossRef]
- Sharratt, C.L.; Gilbert, C.J.; Cornes, M.C.; Ford, C.; Gama, R. EDTA sample contamination is common and often undetected, putting patients at unnecessary risk of harm. Int. J. Clin. Pract. 2009, 63, 1259–1262. [Google Scholar] [CrossRef] [PubMed]
- Fukugawa, Y.; Ohnishi, H.; Ishii, T.; Tanouchi, A.; Sano, J.; Miyawaki, H.; Kishino, T.; Ohtsuka, K.; Yoshino, H.; Watanabe, T. Effect of carryover of clot activators on coagulation tests during phlebotomy. Am. J. Clin. Pathol. 2012, 137, 900–903. [Google Scholar] [CrossRef] [PubMed]
- Cornes, M.P.; Ford, C.; Gama, R. Spurious hyperkalaemia due to EDTA contamination: Common and not always easy to identify. Ann. Clin. Biochem. 2008, 45, 601–603. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Journal | Aim | Type of Study | Samples | System of Draw | Main Findings | CASP |
|---|---|---|---|---|---|---|---|
| Cornes et al. (2008) [26] | Annals of Clinical Biochemistry | Measure EDTA in hyperkalemic samples to identify EDTA contamination. | Observational | 117 inpatients and outpatients | Closed blood collection system | 28 tubes were contaminated with EDTA. At low concentration, it is common, and it can only be confidently detected by measurement of serum EDTA. The order of draw is necessary to obtain correct biochemical results. EDTA contamination was not evident in blood samples collected by trained phlebotomists. The biochemical alterations are statistically and clinically significant. | 10/12 |
| Sharratt et al. (2009) [24] | International Journal of Clinical Practice | To audit the prevalence of EDTA contamination as a cause of hyperkalemia, hypocalcemia, hypomagnesemia, and hypozincemia. | Observational | 12,895 patients | Closed blood collection system | 31 tubes were contaminated with EDTA. Factious hyperkalemia, hypocalcemia, and hypomagnesemia and hypozincemia caused by EDTA contamination is relatively common, so the order of draw has importance. The spurious results are statistically and clinically significant. | 11/12 |
| Cornes et al. (2010) [15] | Clinical Laboratory | Measured EDTA in hyperkalemic (serum potassium ≥ 6.0 mmol/L) samples to determine the prevalence of EDTA sample contamination. | Observational | 131,824 inpatients | Closed blood collection system | 37 tubes were contaminated with EDTA. Hyperkalemia due to EDTA contamination is not uncommon and may remain undetected. The order of draw avoids spurious biochemical results. The results altered by EDTA are statistically and clinically significant. | 9/12 |
| Sulaiman et al. (2011) [14] | Journal of Clinical Pathology | To investigate whether incorrect order of draw of blood samples during phlebotomy causes in vitro potassium EDTA contamination of blood samples. | Observational | 10 healthy volunteers | Closed blood collection system | 0 tubes were contaminated with EDTA. The incorrect order of draw of blood samples does not result in EDTA sample contamination. In ideal phlebotomy conditions, the order of draw has no effect on serum biochemical results. | 11/12 |
| Fukugawa et al. (2012) [25] | American Journal of Clinical Pathology | To investigate the effect of clot activators carried over from the serum in major coagulation tests during phlebotomy. | Observational and in vitro | 100 (75 healthy volunteers and 25 patients) | Closed blood collection system | Using standard phlebotomy sequence, it may be accepFIGUREto collect the coagulation after the serum tube. The order of draw has statistically but not clinically significant importance. | 10/12 |
| Cornes et al. (2012) [21] | British Journal of Biomedical Science | To investigate whether reversed order of draw of blood causes in vitro potassium EDTA contamination. | Observational | 11 healthy volunteers | Closed blood collection system | 0 tubes were contaminated with EDTA. Reversed order of draw of blood samples does not cause potassium EDTA sample contamination, irrespective of the type of closed blood collection system used. The draw was collected by the same experienced phlebotomist. | 10/12 |
| Salvagno et al. (2013) [22] | Clinical Chemistry and Laboratory Medicine | To establish whether or not following a specific order of draw is still reasonable or analytically and clinically justified. | Observational | 115 (57 outpatients and 58 healthy volunteers) | Closed blood collection system | 0 tubes were contaminated with EDTA. The order of draw has a negligible importance even when the internal needle of the holder gets in contact with the blood/additive mixture. It should be no longer considered a quality criterion in the evaluation of the performance of phlebotomists. | 11/12 |
| Indevuyst et al. (2015) [20] | International Journal of Laboratory Hematology | To evaluate the effect of the order of draw on the PT/INR and aPTT. | Observational | 193 patients | Closed blood collection system | The order of draw has no significant influence on PT/INR but biases the aPTT without clinical consequence. The venipunctures were performed by experienced phlebotomists. The order of draw for modern vacuum tube collection systems is indeed “much ado about nothing.” | 10/12 |
| Cadamuro et al. (2015) [23] | Clinical Chemistry and Laboratory Medicine | To investigate the principle of EDTA carryover during venipuncture using the closed vacuum system and EDTA contamination in vitro by simulating specimen collection. | Observational and in vitro | 10 healthy volunteers | Open bloodcollection system | 0 tubes were contaminated with EDTA. The carryover during blood collection using a closed system is highly unlikely and, even if it occurs, the volume needed to alter the test results is huge. The order of draw, adhering to the current recommendations in blood collection, could not be followed. | 10/12 |
| Keppel et al. (2019) [13] | Clinical Chemistry and Laboratory Medicine | To assess effects of potential carryover of citrate and heparin additives during a standard phlebotomy procedure. | In vitro | 10 tubes | Closed blood collection system | Sample contamination with additives from other tubes can occur only if guidelines on blood collection are not strictly followed or an open blood-sampling system is used. The effect of order of draw using closed blood collection system seems to be negligible. | 11/12 |
| Asif et al. (2019) [19] | Annals of Clinical Biochemistry | To identify the causes of EDTA contaminated samples in routine clinical practice. | Observational | 96 patients | Open blood collection system | EDTA sample contamination is a trait of the open phlebotomy system. The guidelines should emphasize the use of closed blood collection systems and underline the need to follow the order of draw only when using open phlebotomy methods. | 11/12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazzano, G.; Galazzi, A.; Giusti, G.D.; Panigada, M.; Laquintana, D. The Order of Draw during Blood Collection: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 1568. https://doi.org/10.3390/ijerph18041568
Bazzano G, Galazzi A, Giusti GD, Panigada M, Laquintana D. The Order of Draw during Blood Collection: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1568. https://doi.org/10.3390/ijerph18041568
Chicago/Turabian StyleBazzano, Giacomo, Alessandro Galazzi, Gian Domenico Giusti, Mauro Panigada, and Dario Laquintana. 2021. "The Order of Draw during Blood Collection: A Systematic Literature Review" International Journal of Environmental Research and Public Health 18, no. 4: 1568. https://doi.org/10.3390/ijerph18041568
APA StyleBazzano, G., Galazzi, A., Giusti, G. D., Panigada, M., & Laquintana, D. (2021). The Order of Draw during Blood Collection: A Systematic Literature Review. International Journal of Environmental Research and Public Health, 18(4), 1568. https://doi.org/10.3390/ijerph18041568