
Comparative Analysis of Social Support in Online Health Communities Using a Word Co-Occurrence Network Analysis Approach


Abstract
:1. Introduction
2. Materials and Methods
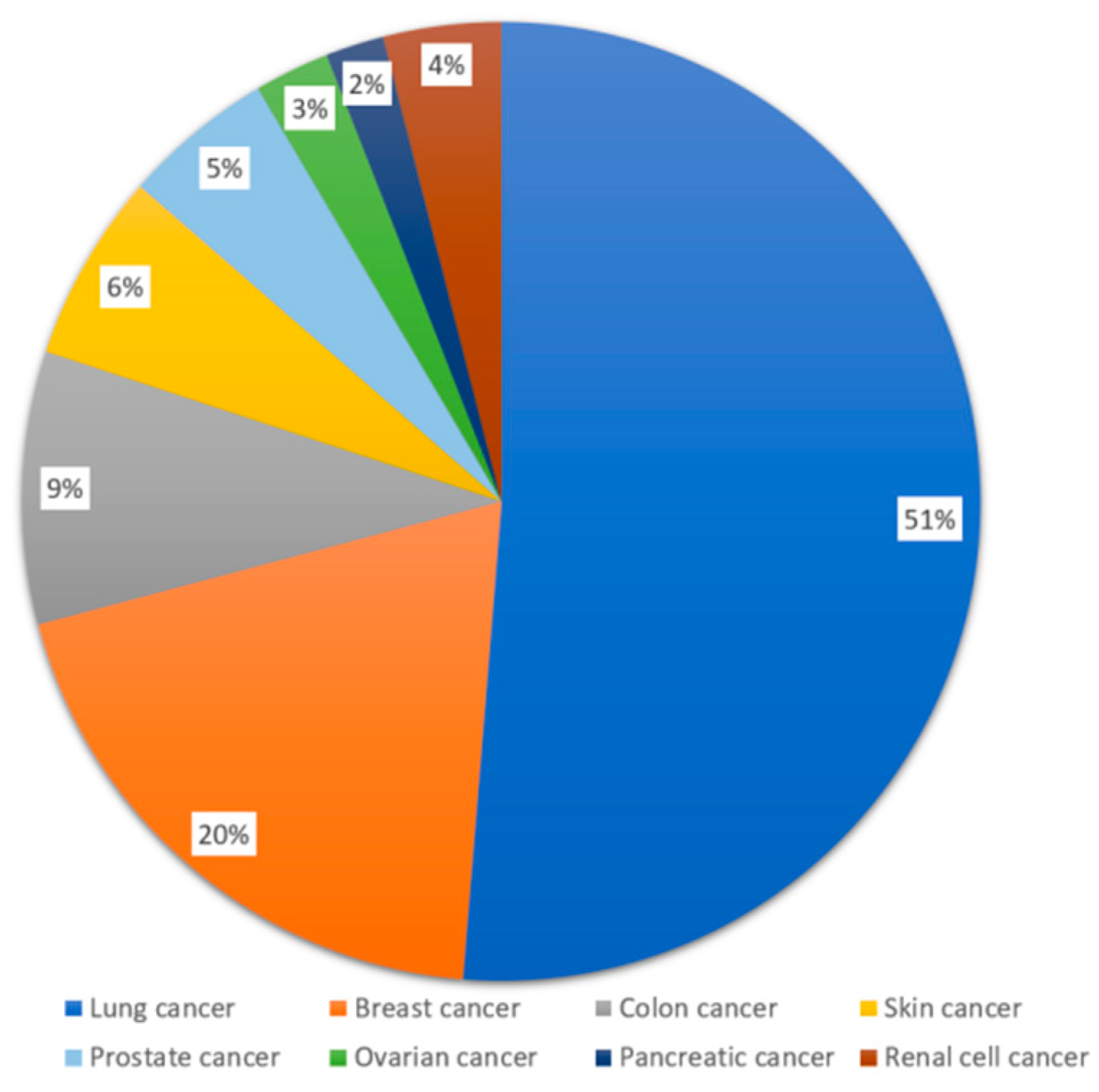
2.1. Data Source
2.2. Method and Procedures
- The Taxonomy of Social Support.
3. Results
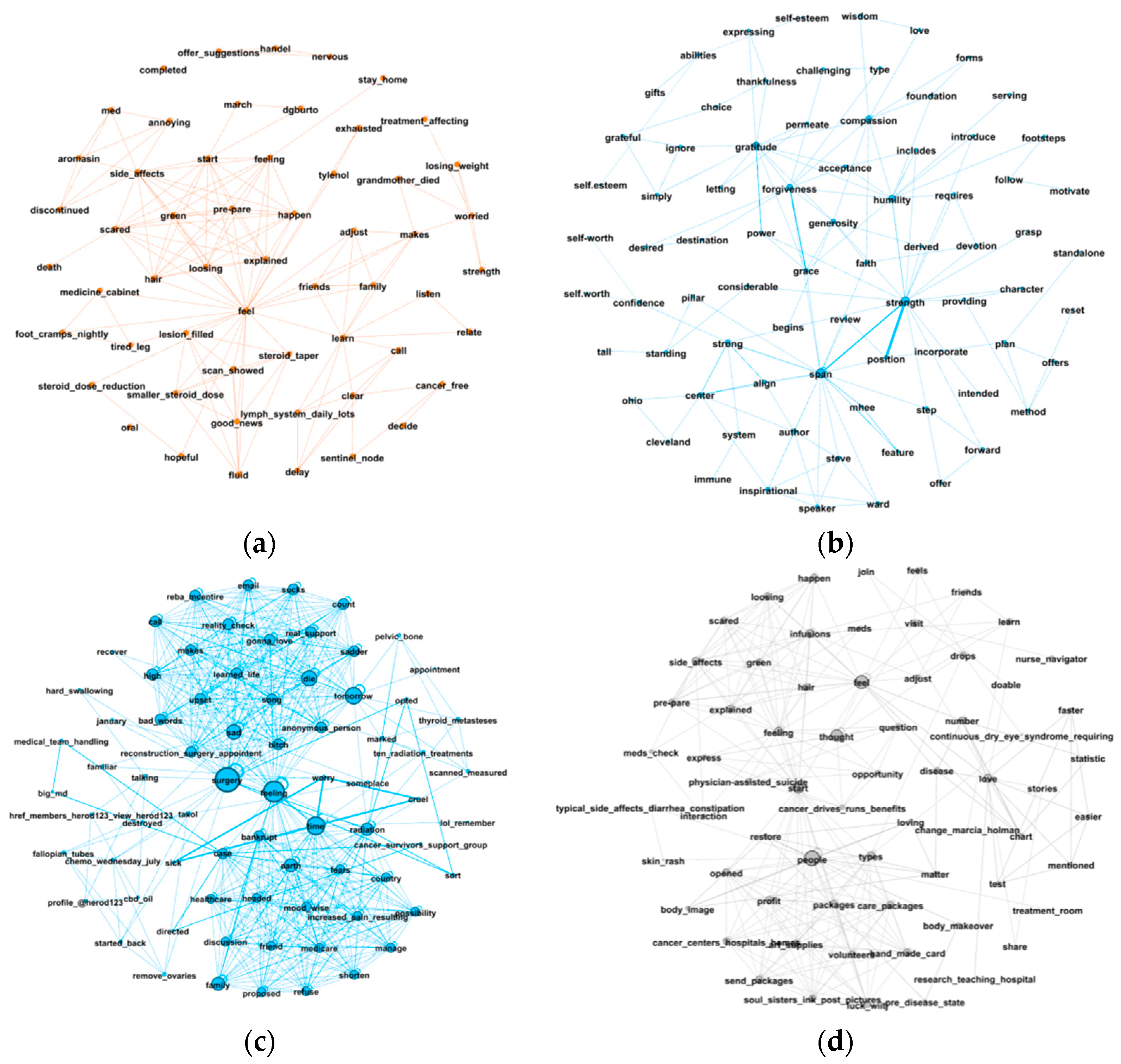
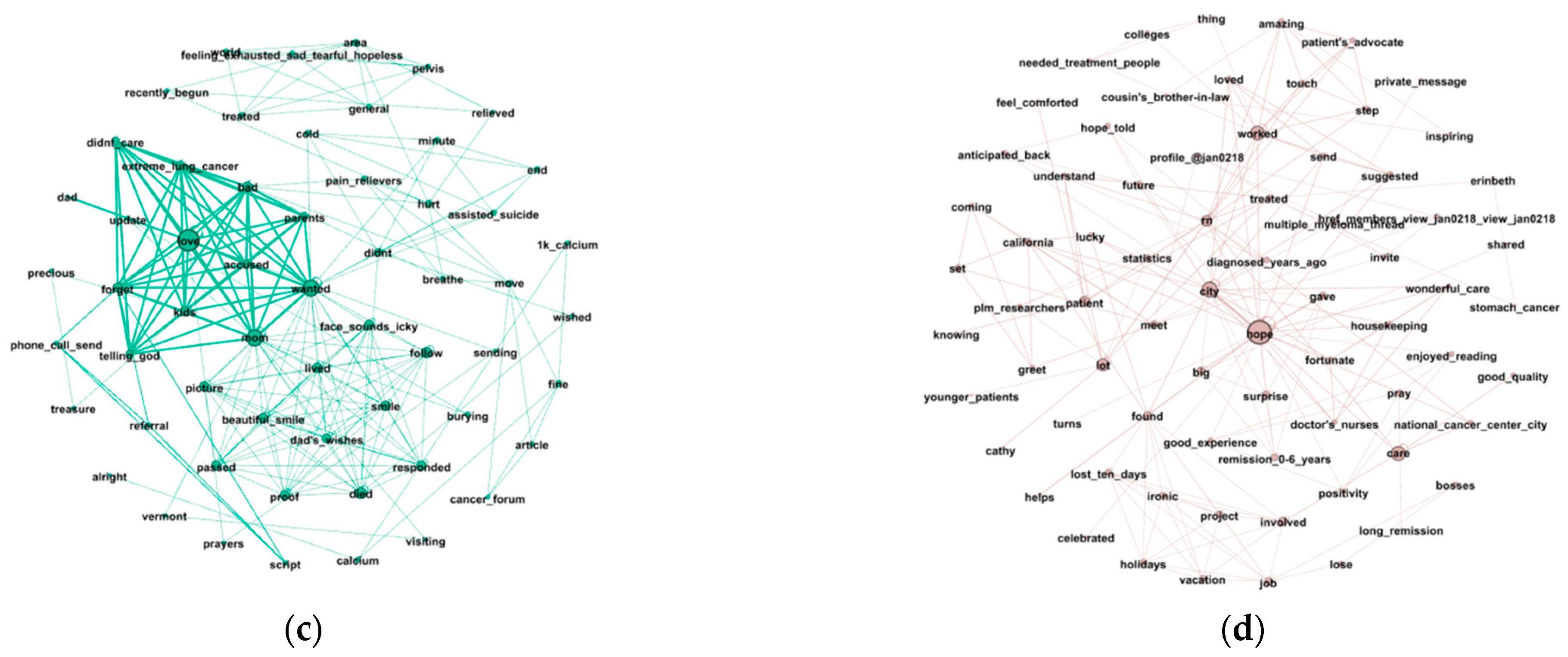
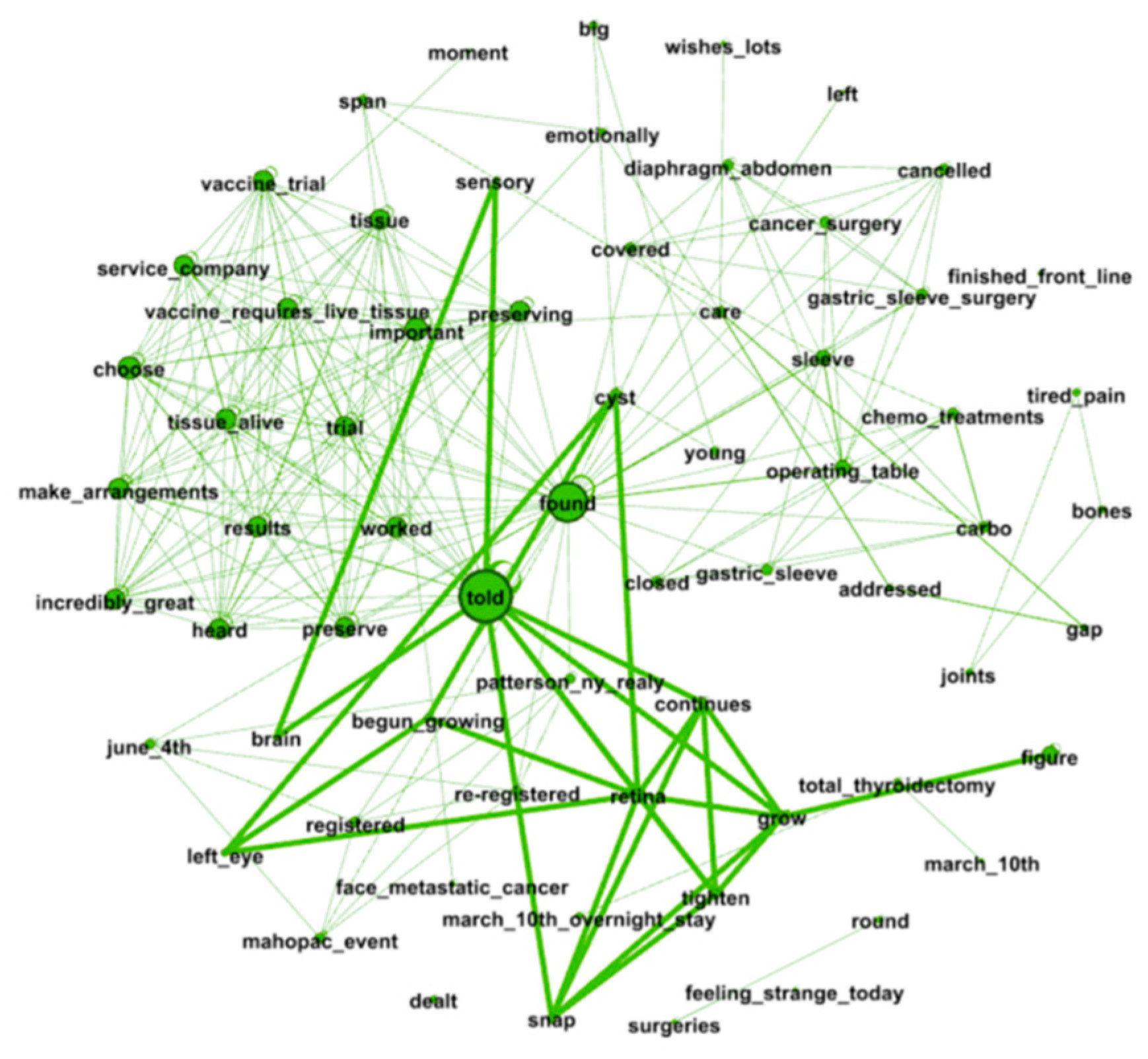
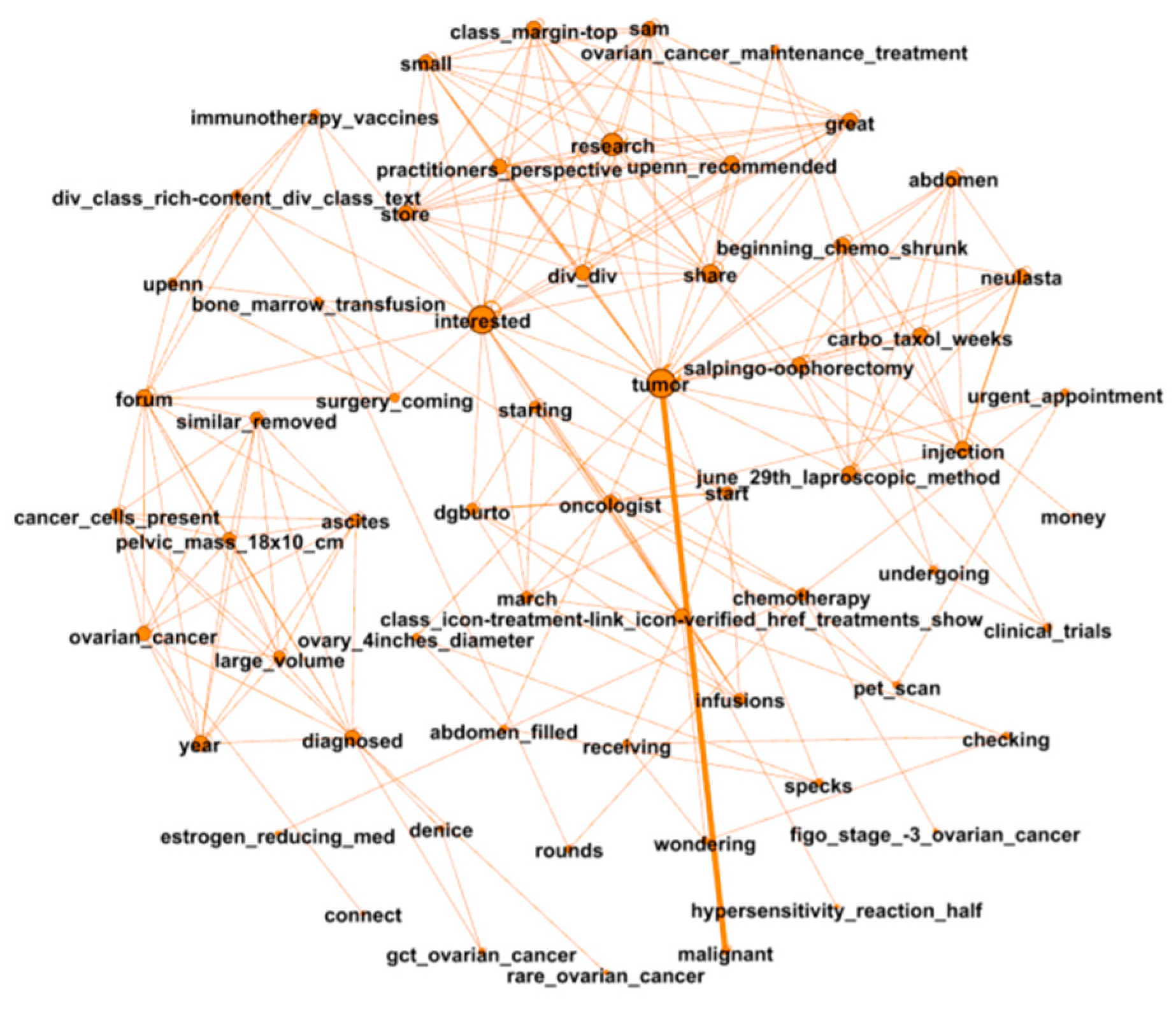
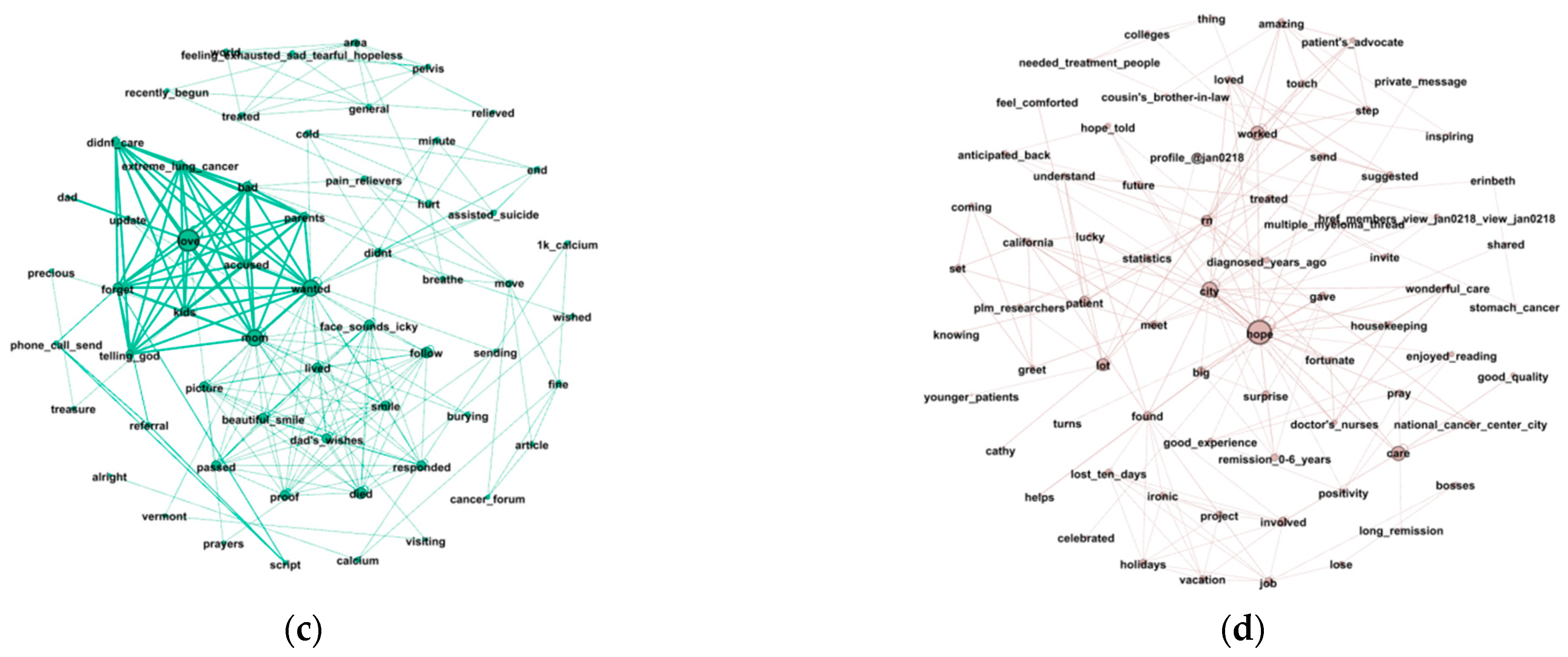
3.1. Word Co-Occurrence Network
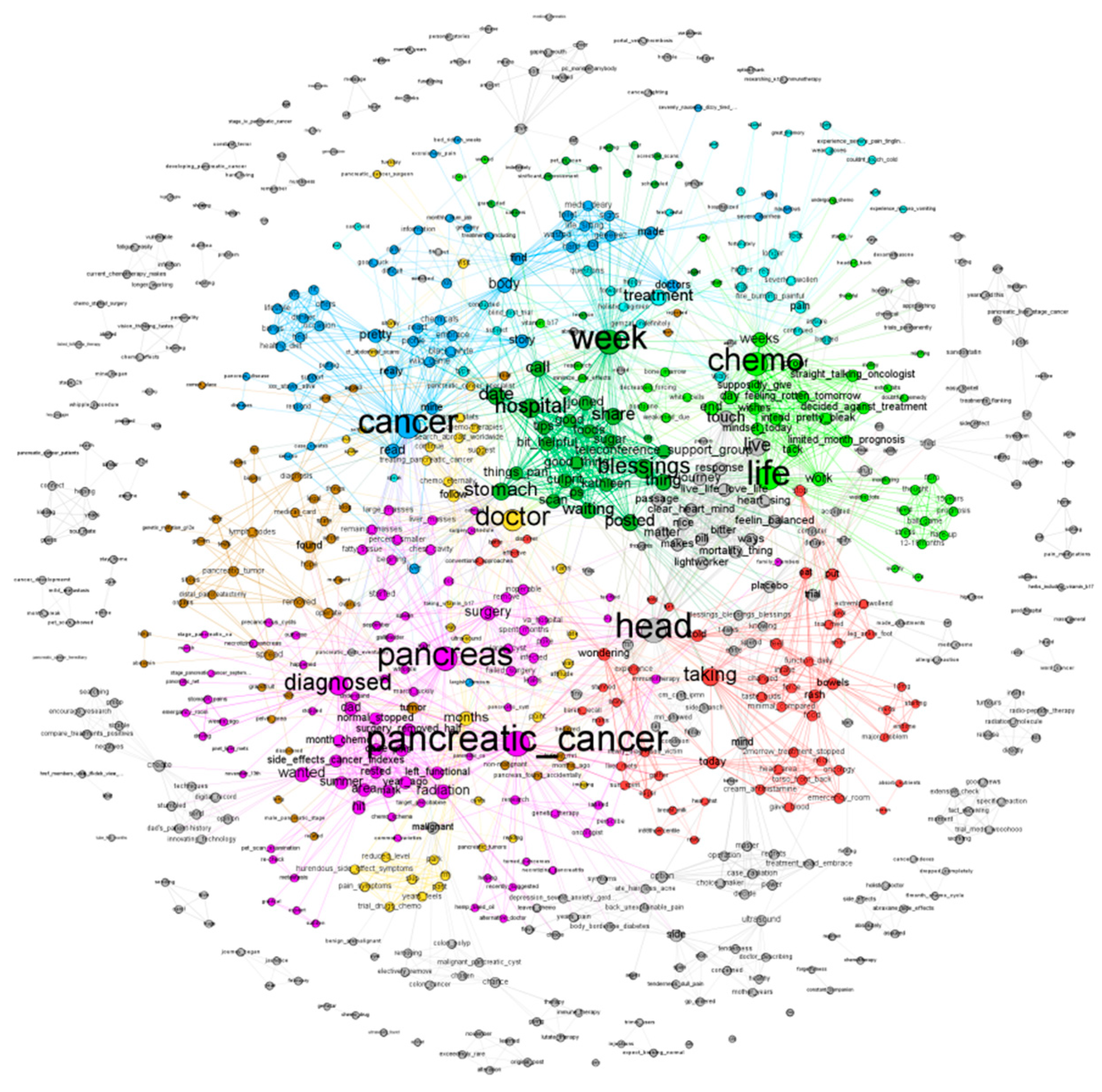
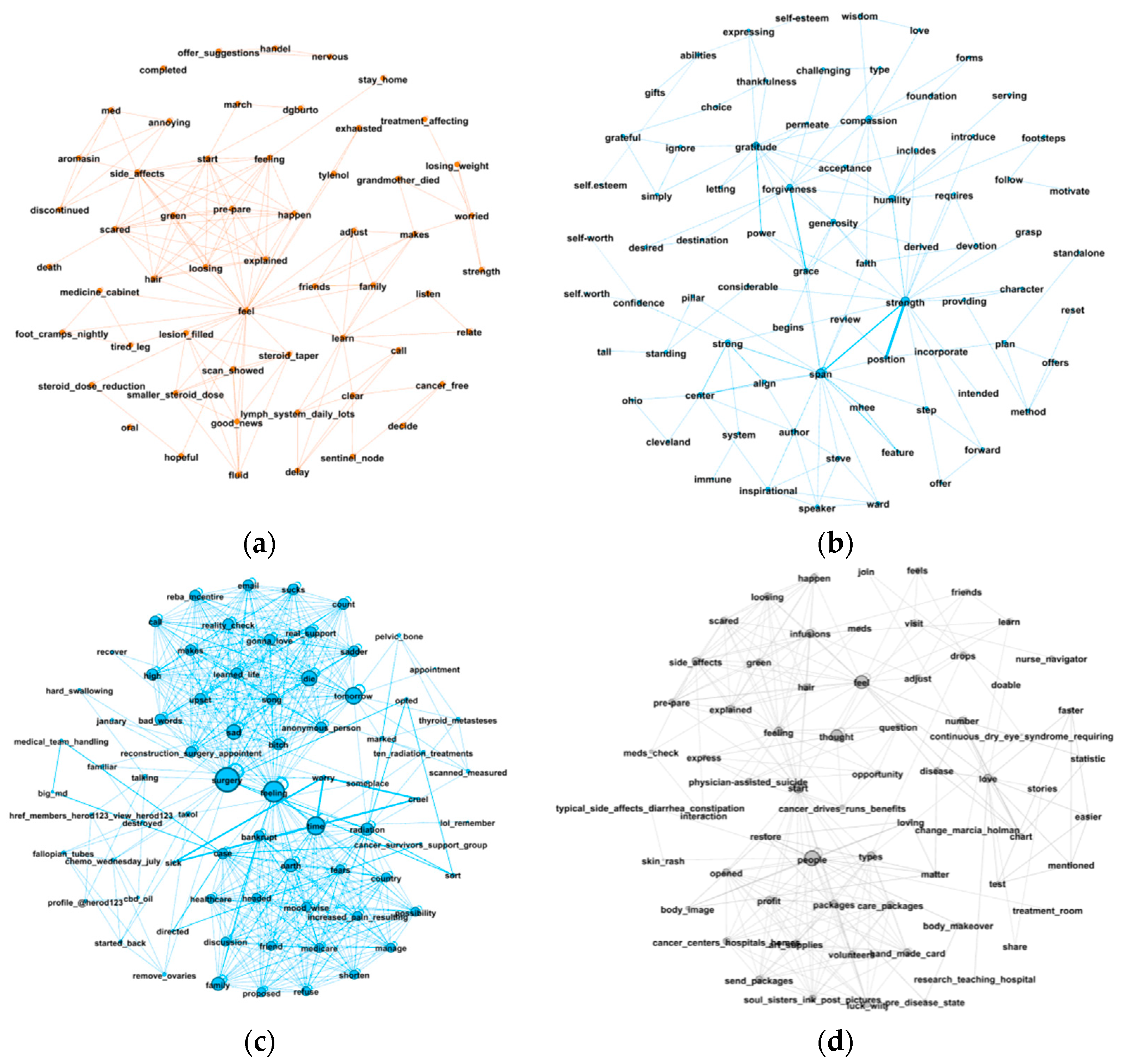
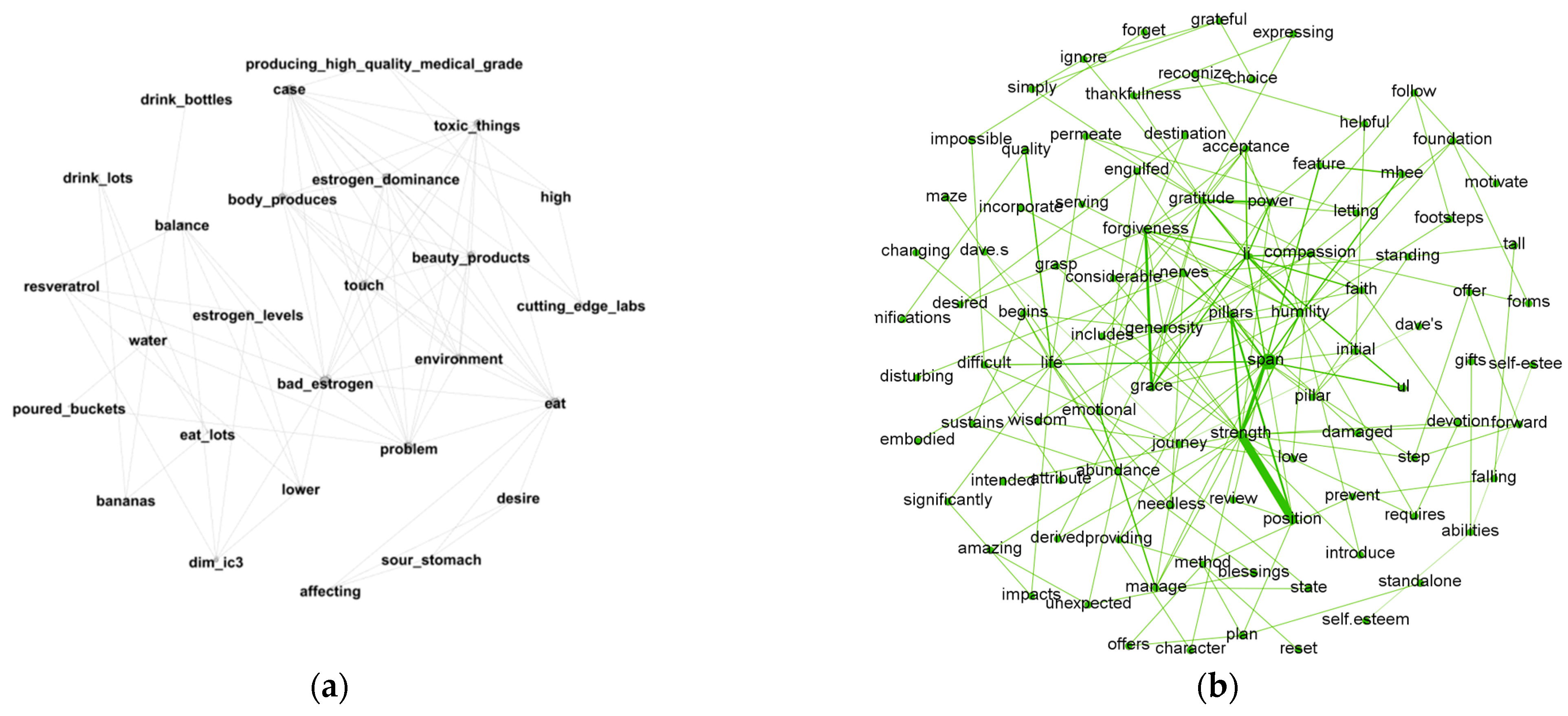
3.2. Module Detection
3.3. Social Support Quantification and Interpretation
3.3.1. Differences across Diseases in Types of Social Support
3.3.2. Differences across Diseases in Communication Preference and Language Use
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van der Eijk, M.; Faber, M.J.; Aarts, J.W.; Kremer, J.A.; Munneke, M.; Bloem, B.R. Using online health communities to deliver patient-centered care to people with chronic conditions. J. Med. Internet Res. 2013, 15, e115. [Google Scholar] [CrossRef] [PubMed]
- Goh, J.M.; Gao, G.; Agarwal, R. The creation of social value: Can an online health community reduce rural–urban health disparities? MIS Q. 2016, 40, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Merolli, M.; Gray, K.; Martin-Sanchez, F. Health outcomes and related effects of using social media in chronic disease management: A literature review and analysis of affordances. J. Biomed. Inform. 2013, 46, 957–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nausheen, B.; Gidron, Y.; Peveler, R.; Moss-Morris, R. Social support and cancer progression: A systematic review. J. Psychosom. Res. 2009, 67, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Crispo, A.; Brennan, P.; Jockel, K.H.; Schaffrath-Rosario, A.; Wichmann, H.E.; Nyberg, F.; Simonato, L.; Merletti, F.; Forastiere, F.; Boffetta, P.; et al. The cumulative risk of lung cancer among current, ex-and never-smokers in European men. Br. J. Cancer 2004, 91, 1280–1286. [Google Scholar] [CrossRef] [Green Version]
- Fareed, N.; Swoboda, C.M.; Jonnalagadda, P.; Huerta, T.R. Persistent digital divide in health-related internet use among cancer survivors: Findings from the Health Information National Trends Survey, 2003–2018. J. Cancer Surviv. 2021, 15, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.J.; Lee, B. The effect of computer-mediated social support in online communities on patient empowerment and doctor-patient communication. Health Commun. 2012, 27, 30–41. [Google Scholar] [CrossRef]
- Walther, J.B.; Boyd, S. Attraction to computer-mediated social support. Commun. Technol. Soc. Audlence Adopt. Uses 2002, 153188, 2. [Google Scholar]
- Wright, K.B.; Miller, C.H. A measure of weak-tie/strong-tie support network preference. Commun. Monogr. 2010, 77, 500–517. [Google Scholar] [CrossRef]
- Wright, K.B.; Johnson, A.; Bernard, D.R.; Averbeck, J. Computer-mediated social support: Promises and pitfalls for individuals coping with health concerns. In The Routledge Handbook of Health Communication; Thompson, T.L., Parrott, R., Nussbaum, J.F., Eds.; Routledge: Abingdon, UK, 2011; pp. 349–362. [Google Scholar]
- Keating, D.M. Spirituality and support: A descriptive analysis of online social support for depression. J. Relig. Health 2013, 52, 1014–1028. [Google Scholar] [CrossRef] [PubMed]
- Gooden, R.J.; Winefield, H.R. Breast and prostate cancer online discussion boards: A thematic analysis of gender differences and similarities: A thematic analysis of gender differences and similarities. J. Health Psychol. 2007, 12, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Meier, A.; Lyons, E.; Frydman, G.; Forlenza, M.; Rimer, B. How cancer survivors provide support on cancer-related Internet mailing lists. J. Med. Internet Res. 2007, 9, e12. [Google Scholar] [CrossRef] [PubMed]
- Barger, S.D. Perceived emotional support and frequent social contacts are associated with greater knowledge of stroke warning signs: Evidence from two cross-sectional us population surveys. J. Health Psychol. 2012, 17, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Buis, L.R. Emotional and informational support messages in an online hospice support community. Comput. Inform. Nurs. 2008, 26, 358–367. [Google Scholar] [CrossRef]
- Rains, S.A.; Peterson, E.B.; Wright, K.B. Communicating social support in computer-mediated contexts: A meta-analytic review of content analyses examining support messages shared online among individuals coping with illness. Commun. Monogr. 2015, 82, 403–430. [Google Scholar] [CrossRef]
- Blank, T.O.; Adams-Blodnieks, M. The who and the what of usage of two cancer online communities. Comput. Hum. Behav. 2007, 23, 1249–1257. [Google Scholar] [CrossRef]
- Seale, C.; Ziebland, S.; Charteris-Black, J. Gender, cancer experience and internet use: A comparative keyword analysis of interviews and online cancer support groups. Soc. Sci. Med. 2006, 62, 2577–2590. [Google Scholar] [CrossRef]
- Blank, T.O.; Schmidt, S.D.; Vangsness, S.A.; Monteiro, A.K.; Santagata, P.V. Differences among breast and prostate cancer online support groups. Comput. Hum. Behav. 2010, 26, 1400–1404. [Google Scholar] [CrossRef]
- Liu, X.; Sun, M.; Li, J. Research on gender differences in online health communities. Int. J. Med. Inform. 2018, 111, 172–181. [Google Scholar] [CrossRef]
- Brandenbarg, D.; Maass, S.W.; Geerse, O.P.; Stegmann, M.E.; Handberg, C.; Schroevers, M.J.; Duijts, S.F. A systematic review on the prevalence of symptoms of depression, anxiety and distress in long-term cancer survivors: Implications for primary care. Eur. J. Cancer Care 2019, 28, e13086. [Google Scholar] [CrossRef]
- Coursaris, C.K.; Liu, M. An analysis of social support exchanges in online HIV/AIDS self-help groups. Comput. Hum. Behav. 2009, 25, 911–918. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, K.; Street, N. Analyzing and predicting user participations in online health communities: A social support perspective. J. Med. Internet Res. 2017, 19, e130. [Google Scholar] [CrossRef]
- Wu, J.; Hou, S.; Jin, M. Social support and user roles in a Chinese online health community: A LDA based text mining study. In Proceedings of the International Conference on Smart Health, Hong Kong, China, 26–27 June 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 169–176. [Google Scholar]
- Wicks, P.; Massagli, M.; Frost, J.; Brownstein, C.; Okun, S.; Vaughan, T.; Bradley, R.; Heywood, J. Sharing health data for better outcomes on PatientsLikeMe. J. Med. Internet Res. 2010, 12, e19. [Google Scholar] [CrossRef] [Green Version]
- Eaneff, S.; Wang, V.; Hanger, M.; Levy, M.; Mealy, M.A.; Brandt, A.U.; Eek, D.; Ratchford, J.N.; Nyberg, F.; Goodall, J.; et al. Patient perspectives on neuromyelitis optica spectrum disorders: Data from the PatientsLikeMe online community. Mult. Scler. Relat. Disord. 2017, 17, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Lustria, M.L.A.; Burnett, G.; Cortese, J.; Kazmer, M.; Frost, J.; Kim, J.H.; Ma, J. PatientsLikeMe: ALS patients sharing experiences and personal health information online. Proc. Am. Soc. Inf. Sci. Technol. 2009, 46, 1–5. [Google Scholar] [CrossRef]
- Wang, X.; Zuo, Z.; Zhao, K.; Street, N. Predicting User Participation and Detecting User Role Diffusion in Online Health Communities. In Proceedings of the IEEE 2015 International Conference on Healthcare Informatics, Dallas, TX, USA, 21–23 October 2015; p. 483. [Google Scholar]
- Xing, W.; Goggins, S.; Introne, J. Quantifying the effect of informational support on membership retention in online communities through large-scale data analytics. Comput. Hum. Behav. 2018, 86, 227–234. [Google Scholar] [CrossRef]
- Watts, D.J.; Strogatz, S.H. Collective dynamics of ‘small-world’ networks. Nature 1998, 393, 440–442. [Google Scholar] [CrossRef]
- Barabási, A.L.; Albert, R. Emergence of scaling in random networks. Science 1999, 286, 509–512. [Google Scholar] [CrossRef] [Green Version]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. 2008, 10, P10008. [Google Scholar] [CrossRef] [Green Version]
- Lambiotte, R.; Delvenne, J.C.; Barahona, M. Laplacian dynamics and multiscale modular structure in networks. IEEE Trans. Netw. Sci. Eng. 2014, 1, 76–90. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, C.; Coyne, J.C.; Lazarus, R.S. The health-related functions of social support. J. Behav. Med. 1981, 4, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Cutrona, C.E.; Suhr, J.A. Controllability of stressful events and satisfaction with spouse support behaviors. Commun. Res. 1992, 19, 154–174. [Google Scholar] [CrossRef]
- Bambina, A. Online Social Support: The Interplay of Social Networks and Computer-Mediated Communication; Cambria Press: Youngstown, NY, USA, 2007; pp. 27–54. [Google Scholar]
- Mo, P.K.; Malik, S.H.; Coulson, N.S. Gender differences in computer-mediated communication: A systematic literature review of online health-related support groups. Patient Educ. Couns. 2009, 75, 16–24. [Google Scholar] [CrossRef]
- Alwhaibi, M.; Sambamoorthi, U.; Madhavan, S.; Bias, T.; Kelly, K.; Walkup, J. Cancer type and risk of newly diagnosed depression among elderly medicare beneficiaries with incident breast, colorectal, and prostate cancers. J. Natl. Compr. Cancer Netw. 2017, 15, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Petrič, G.; Atanasova, S.; Kamin, T. Impact of Social Processes in Online Health Communities on Patient Empowerment in Relationship With the Physician: Emergence of Functional and Dysfunctional Empowerment. J. Med. Internet Res. 2017, 19, e74. [Google Scholar] [CrossRef]
- Audrain-Pontevia, A.F.; Menvielle, L. Do online health communities enhance patient-physician relationship? An assessment of the impact of social support and patient empowerment. Health Serv. Manag. Res. 2018, 31, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Moorhead, S.A.; Hazlett, D.E.; Harrison, L.; Carroll, J.K.; Irwin, A.; Hoving, C. A new dimension of health care: Systematic review of the uses, benefits, and limitations of social media for health communication. J. Med. Internet Res. 2013, 15, e85. [Google Scholar] [CrossRef] [Green Version]
- Pirraglia, P.A.; Kravitz, R.L. Social media: New opportunities, new ethical concerns. J. Gen. Intern. Med. 2013, 28, 165–166. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Type | Sentences | Words | Co-Occurrence Pairs | |||
|---|---|---|---|---|---|---|
| Lung cancer | 15,690 | 12,830 | 196,620 | 3.167/2.764 | 0.789/0.001 | 2.416 |
| Breast cancer | 3222 | 4059 | 48,559 | 3.481/2.617 | 0.821/0.003 | 2.930 |
| Colon cancer | 2746 | 3524 | 57,430 | 3.188/2.344 | 0.826/0.005 | 3.017 |
| Basal cell skin cancer | 1295 | 1462 | 12,124 | 3.901/2.595 | 0.831/0.006 | 3.453 |
| Prostate cancer | 751 | 2005 | 28,475 | 3.409/2.272 | 0.867/0.007 | 3.056 |
| Ovarian cancer | 585 | 936 | 10,842 | 3.592/2.177 | 0.884/0.012 | 4.802 |
| Pancreatic cancer | 315 | 729 | 6749 | 3.595/2.258 | 0.861/0.013 | 3.939 |
| Renal cell cancer | 848 | 1196 | 9692 | 4.054/2.544 | 0.858/0.007 | 3.414 |
| Module ID | % of Edges | Silhouette | Selected Keywords |
|---|---|---|---|
| 1 | 11.35% | 0.503 | pancreatic cancer; diagnosed; side effects; surgery; left functional |
| 2 | 7.90% | 0.546 | chemo; life; oncologist; monitoring; weeks |
| 3 | 6.32% | 0.615 | cancer; healthy diet; drinker; fatty tissue; chest cavity |
| 4 | 6.08% | 0.771 | doctors; medical cars; scans; sign; pain symptoms |
| 5 | 4.39% | 0.791 | treatment; pain; happy; awful; painful |
| Cancer Type | Modularity | CC | Silhouette | Number of Modules |
|---|---|---|---|---|
| Lung cancer | 0.414 | 0.855 | 0.426 | 28 |
| Breast cancer | 0.646 | 0.842 | 0.433 | 29 |
| Colon cancer | 0.576 | 0.840 | 0.506 | 27 |
| Basal cell skin cancer | 0.751 | 0.857 | 0.575 | 29 |
| Prostate cancer | 0.685 | 0.898 | 0.802 | 28 |
| Ovarian cancer | 0.786 | 0.903 | 0.593 | 27 |
| Pancreatic cancer | 0.769 | 0.890 | 0.649 | 25 |
| Renal cell cancer | 0.797 | 0.877 | 0.503 | 26 |
| Cancer Type | Information Support | Emotional Support | Companionship |
|---|---|---|---|
| Lung cancer | 54.94% | 13.32% | 31.74% |
| Breast cancer | 40.68% | 40.45% | 18.87% |
| Colon cancer | 58.81% | 8.99% | 32.20% |
| Basal cell skin cancer | 42.02% | 24.19% | 33.79% |
| Prostate cancer | 41.15% | 36.73% | 22.12% |
| Ovarian cancer | 37.22% | 36.43% | 26.35% |
| Pancreatic cancer | 54.34% | 13.13% | 32.53% |
| Renal cell cancer | 47.92% | 23.61% | 28.47% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Zou, X.; Chen, J.; Ma, S. Comparative Analysis of Social Support in Online Health Communities Using a Word Co-Occurrence Network Analysis Approach. Entropy 2022, 24, 174. https://doi.org/10.3390/e24020174
Liu M, Zou X, Chen J, Ma S. Comparative Analysis of Social Support in Online Health Communities Using a Word Co-Occurrence Network Analysis Approach. Entropy. 2022; 24(2):174. https://doi.org/10.3390/e24020174
Chicago/Turabian StyleLiu, Mengque, Xia Zou, Jiyin Chen, and Shuangge Ma. 2022. "Comparative Analysis of Social Support in Online Health Communities Using a Word Co-Occurrence Network Analysis Approach" Entropy 24, no. 2: 174. https://doi.org/10.3390/e24020174
APA StyleLiu, M., Zou, X., Chen, J., & Ma, S. (2022). Comparative Analysis of Social Support in Online Health Communities Using a Word Co-Occurrence Network Analysis Approach. Entropy, 24(2), 174. https://doi.org/10.3390/e24020174