
hPG80 (Circulating Progastrin), a Novel Blood-Based Biomarker for Detection of Poorly Differentiated Neuroendocrine Carcinoma and Well Differentiated Neuroendocrine Tumors


 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Control Cohorts
2.2. hPG80 Level Measurements in the Blood Samples
2.3. Statistical Analysis
3. Results
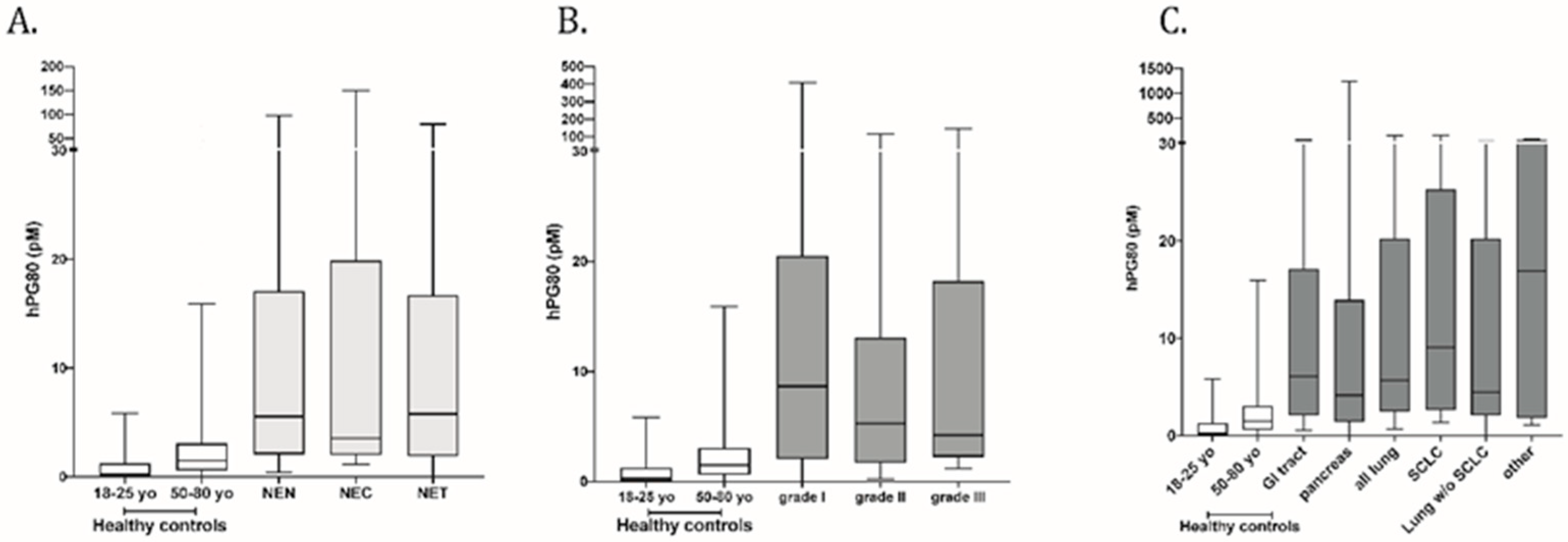
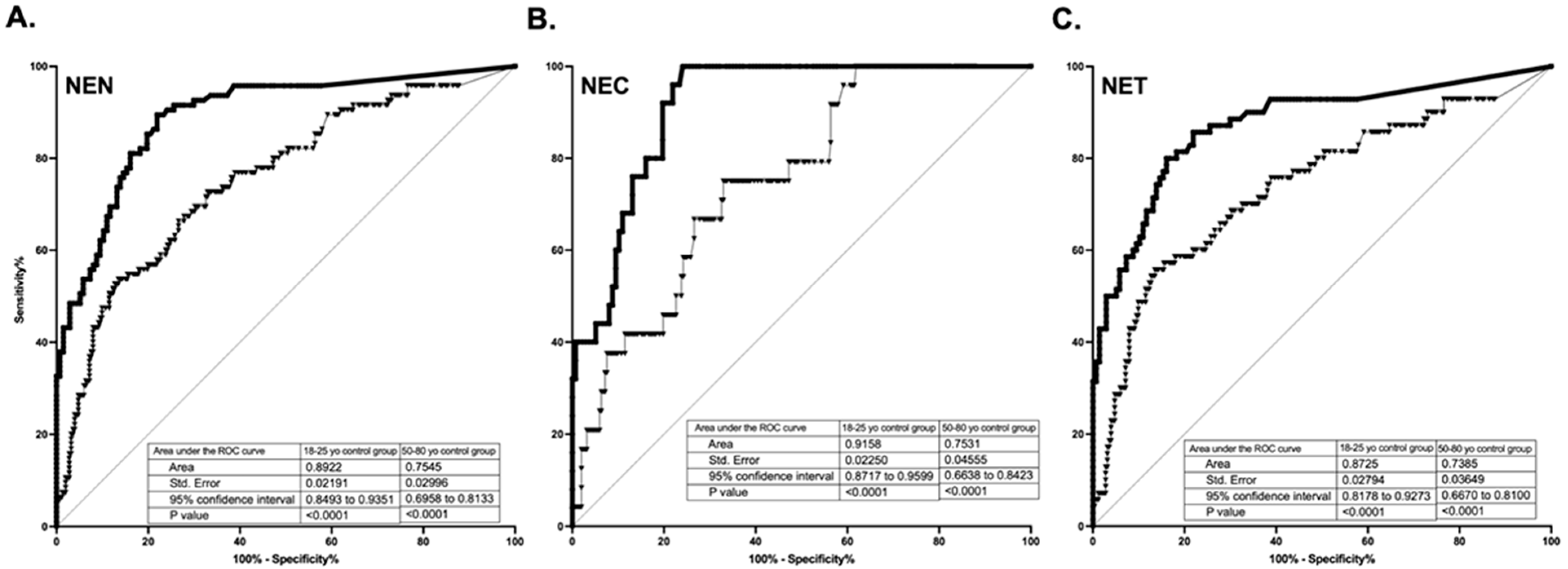
3.1. Diagnostic Performance of hPG80 in the Various Cohorts of Cancer Patients
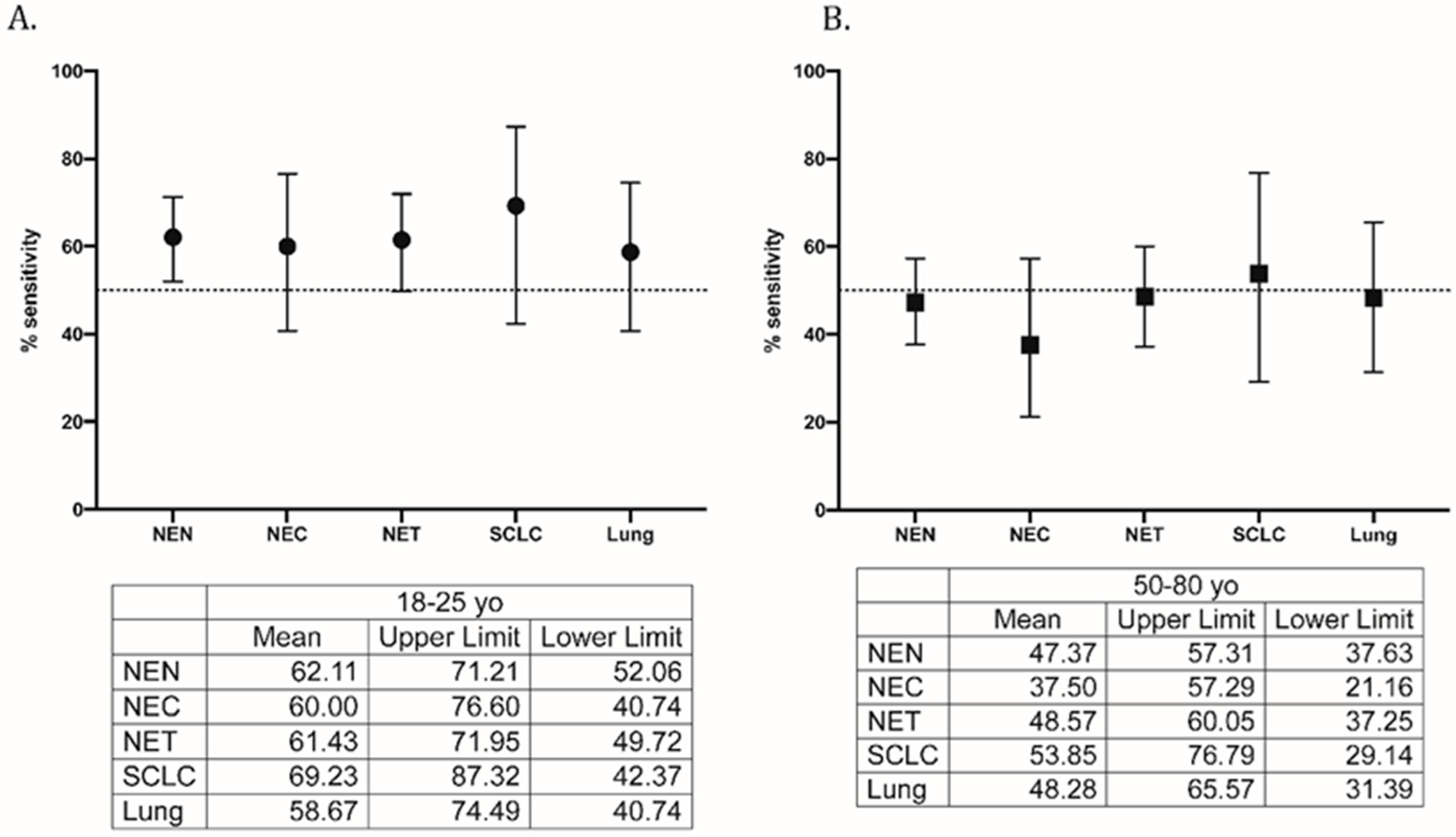
3.2. Diagnostic Performance of hPG80 in Each Sub-Cohort of Cancer Type
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chauhan, A.; Kohn, E.; Del Rivero, J. Neuroendocrine Tumors-Less Well Known, Often Misunderstood, and Rapidly Growing in Incidence. JAMA Oncol. 2020, 6, 21–22. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Oberg, K.; Modlin, I.M.; De Herder, W.; Pavel, M.; Klimstra, D.; Frilling, A.; Metz, D.C.; Heaney, A.; Kwekkeboom, D.; Strosberg, J.; et al. Consensus on biomarkers for neuroendocrine tumour disease. Lancet Oncol. 2015, 16, e435–e446. [Google Scholar] [CrossRef]
- Rehfeld, J.F.; Zhu, X.; Norrbom, C.; Bundgaard, J.R.; Johnsen, A.H.; Nielsen, J.E.; Vikesaa, J.; Stein, J.; Dey, A.; Steiner, D.F.; et al. Prohormone convertases 1/3 and 2 together orchestrate the site-specific cleavages of progastrin to release gastrin-34 and gastrin-17. Biochem. J. 2008, 415, 35–43. [Google Scholar] [CrossRef]
- Varro, A.; Voronina, S.; Dockray, G.J. Pathways of processing of the gastrin precursor in rat antral mucosa. J. Clin. Investig. 1995, 95, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Siddheshwar, R.K.; Gray, J.C.; Kelly, S.B. Plasma levels of progastrin but not amidated gastrin or glycine extended gastrin are elevated in patients with colorectal carcinoma. Gut 2001, 48, 47–52. [Google Scholar] [CrossRef]
- Kohli, M.; Tan, W.; Vire, B.; Liaud, P.; Blairvacq, M.; Berthier, F.; Rouison, D.; Garnier, G.; Payen, L.; Cousin, T.; et al. Prognostic Value of Plasma hPG80 (Circulating Progastrin) in Metastatic Renal Cell Carcinoma. Cancers 2021, 13, 375. [Google Scholar] [CrossRef] [PubMed]
- You, B.; Mercier, F.; Assenat, E.; Langlois-Jacques, C.; Glehen, O.; Soule, J.; Payen, L.; Kepenekian, V.; Dupuy, M.; Belouin, F.; et al. The oncogenic and druggable hPG80 (Progastrin) is overexpressed in multiple cancers and detected in the blood of patients. EBioMedicine 2019, 51, 102574. [Google Scholar] [CrossRef] [PubMed]
- Prieur, A.; Cappellini, M.; Habif, G.; Lefranc, M.P.; Mazard, T.; Morency, E.; Pascussi, J.M.; Flaceliere, M.; Cahuzac, N.; Vire, B.; et al. Targeting the Wnt Pathway and Cancer Stem Cells with Anti-progastrin Humanized Antibodies as a Potential Treatment for K-RAS-Mutated Colorectal Cancer. Clin. Cancer Res. 2017, 23, 5267–5280. [Google Scholar] [CrossRef]
- Kim, J.T.; Li, J.; Jang, E.R.; Gulhati, P.; Rychahou, P.G.; Napier, D.L.; Wang, C.; Weiss, H.L.; Lee, E.Y.; Anthony, L.; et al. Deregulation of Wnt/beta-catenin signaling through genetic or epigenetic alterations in human neuroendocrine tumors. Carcinogenesis 2013, 34, 953–961. [Google Scholar] [CrossRef]
- Giraud, J.; Failla, L.M.; Pascussi, J.M.; Lagerqvist, E.L.; Ollier, J.; Finetti, P.; Bertucci, F.; Ya, C.; Gasmi, I.; Bourgaux, J.F.; et al. Autocrine Secretion of Progastrin Promotes the Survival and Self-Renewal of Colon Cancer Stem-like Cells. Cancer Res. 2016, 76, 3618–3628. [Google Scholar] [CrossRef] [PubMed]
- Hollande, F.; Lee, D.J.; Choquet, A.; Roche, S.; Baldwin, G.S. Adherens junctions and tight junctions are regulated via different pathways by progastrin in epithelial cells. J. Cell Sci. 2003, 116, 1187–1197. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pannequin, J.; Delaunay, N.; Buchert, M.; Surrel, F.; Bourgaux, J.F.; Ryan, J.; Boireau, S.; Coelho, J.; Pélegrin, A.; Singh, P.; et al. β-Catenin/Tcf-4 Inhibition after Progastrin Targeting Reduces Growth and Drives Differentiation of Intestinal Tumors. Gastroenterology 2007, 133, 1554–1568. [Google Scholar] [CrossRef]
- Singh, P.; Owlia, A.; Varro, A.; Dai, B.; Rajaraman, S.; Wood, T. Gastrin gene expression is required for the proliferation and tumorigenicity of human colon cancer cells. Cancer Res. 1996, 56, 4111–4115. [Google Scholar]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46, S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.; Flaceliere, M.; Saywell, V.; Soule, J.; Blanc, E.; Belouin, F.; Ortiz, E.; Canterel-Thouennon, L.; Poupeau, S.; Tigrett, S.; et al. A novel method to detect hPG80 (human circulating progastrin) in the blood. Anal. Methods 2021, 13, 4468–4477. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; de Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef] [PubMed]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef]
- Herrera-Martinez, A.D.; Hofland, L.J.; Galvez Moreno, M.A.; Castano, J.P.; de Herder, W.W.; Feelders, R.A. Neuroendocrine neoplasms: Current and potential diagnostic, predictive and prognostic markers. Endocr. Relat. Cancer 2019, 26, R157–R179. [Google Scholar] [CrossRef]
- Ahmed, M. Gastrointestinal neuroendocrine tumors in 2020. World J. Gastrointest. Oncol. 2020, 12, 791–807. [Google Scholar] [CrossRef]
- Modlin, I.M.; Gustafsson, B.I.; Moss, S.F.; Pavel, M.; Tsolakis, A.V.; Kidd, M. Chromogranin A—Biological function and clinical utility in neuro endocrine tumor disease. Ann. Surg. Oncol. 2010, 17, 2427–2443. [Google Scholar] [CrossRef] [PubMed]
- Walenkamp, A.; Crespo, G.; Fierro Maya, F.; Fossmark, R.; Igaz, P.; Rinke, A.; Tamagno, G.; Vitale, G.; Oberg, K.; Meyer, T. Hallmarks of gastrointestinal neuroendocrine tumours: Implications for treatment. Endocr. Relat. Cancer 2014, 21, R445–R460. [Google Scholar] [CrossRef] [PubMed]
- Malczewska, A.; Kos-Kudla, B.; Kidd, M.; Drozdov, I.; Bodei, L.; Matar, S.; Oberg, K.; Modlin, I.M. The clinical applications of a multigene liquid biopsy (NETest) in neuroendocrine tumors. Adv. Med. Sci. 2020, 65, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.Y.; Gong, Y.F.; Zhuang, H.K.; Zhou, Z.X.; Huang, S.Z.; Zou, Y.P.; Huang, B.W.; Sun, Z.H.; Zhang, C.Z.; Tang, Y.Q.; et al. Pancreatic neuroendocrine tumors: A review of serum biomarkers, staging, and management. World J. Gastroenterol. 2020, 26, 2305–2322. [Google Scholar] [CrossRef] [PubMed]
- Nusse, R.; Clevers, H. Wnt/beta-Catenin Signaling, Disease, and Emerging Therapeutic Modalities. Cell 2017, 169, 985–999. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Cao, Y.; Li, F.; Su, Y.; Li, Y.; Peng, Y.; Cheng, Y.; Zhang, C.; Wang, W.; Ning, G. Targeting beta-catenin signaling for therapeutic intervention in MEN1-deficient pancreatic neuroendocrine tumours. Nat. Commun. 2014, 5, 5809. [Google Scholar] [CrossRef]
- Cao, Y.; Zhou, W.; Li, L.; Wang, J.; Gao, Z.; Jiang, Y.; Jiang, X.; Shan, A.; Bailey, M.H.; Huang, K.L.; et al. Pan-cancer analysis of somatic mutations across 21 neuroendocrine tumor types. Cell Res. 2018, 28, 601–604. [Google Scholar] [CrossRef]
- Koh, T.J.; Chen, D. Gastrin as a growth factor in the gastrointestinal tract. Regul. Pept. 2000, 93, 37–44. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| NEN | NEC | NET | Control Cohorts | |||
|---|---|---|---|---|---|---|
| 18–25 Years Old | 50–80 Years Old | |||||
| N (%) | N (%) | N (%) | N (%) | N (%) | ||
| n = 95 | n = 25 | n = 70 | n = 137 | n = 252 | ||
| Age (years) | Median (range) | 61 (37–86) | 61 (37–78) | 62 (37–86) | 21 (18–25) | 55 (50–80) |
| Gender | Male | 38 (40%) | 10 (40%) | 28 (40%) | 79 (57.7%) | 99 (39.3%) |
| Female | 57 (60%) | 15 (60%) | 42 (60%) | 58 (42.3%) | 153 (60.7%) | |
| hPG80 | Median (IQR), pM | 5.54 (0.00–1241) | 3.54 (1.13–154.1) | 5.8 (0.00–1241) | <LoD | <LoQ |
| Mean (SD) pM | 28.24 (128.8) | 20.7 (39.96) | 30.55 (148.5) | <LoD | 3.82 (0.55) | |
| Stage | I to III | 14 (14.8%) | 2 (8%) | 12 (17.2%) | NA | |
| IV | 80 (84.2%) | 23 (92%) | 57 (81.4%) | |||
| Unknown | 1 (1.0%) | 0 (0%) | 1 (1.4%) | |||
| Grade | 1 | 33 | 0 | 33 | ||
| (34.7%) | (0%) | (47.2%) | ||||
| 2 | 28 | 0 | 28 | |||
| (29.5%) | (0%) | (40%) | ||||
| 3 | 30 | 25 | 5 | |||
| (31.6%) | (100%) | (7.1%) | ||||
| Unknown | 4 | 0 | 4 | |||
| (4.2%) | (0%) | (5.7%) | ||||
| Primary Site | GI tract | 46 | 4 | 42 | ||
| (48.4%) | (16%) | (60%) | ||||
| Pancreas | 15 | 2 | 13 | |||
| (15.8%) | (8%) | (18.6%) | ||||
| SCLC | 13 | 13 | 0 | |||
| (13.7%) | (52%) | (0%) | ||||
| Lung w/o SCLC | 17 | 4 | 13 | |||
| (17.9%) | (16%) | (18.6%) | ||||
| Other | 4 | 2 | 2 | |||
| (4.2%) | (8%) | (2.8%) | ||||
| GRADE | ||||||||
|---|---|---|---|---|---|---|---|---|
| Grade I | Grade II | Grade III | ||||||
| hPG80 | Median (range), pM | 8.66 (0.00–1241) | 5.3 (0.00–142.1) | 4.22 (1.13–154.1) | ||||
| Mean (SD), pM | 48.71 (214.4) | 16.37 (32.1) | 19.18 (36.77) | |||||
| PRIMARY SITE | ||||||||
| GI Tract | Pancreas | SCLC | Lung not SCLC | Other | ||||
| hPG80 | Median (range), pM | 6.06 (0.00–142.1) | 4.14 (0.00–1241) | 9.09 (1.35–124.1) | 4.51 (0.00–34.85) | 16.89 (1.13–86.87) | ||
| Mean (SD), pM | 13.88 (24.02) | 88.9 (318.9) | 30.36 (52.78) | 11.37 (11.35) | 30.45 (39.78) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chauhan, A.; Prieur, A.; Kolesar, J.; Arnold, S.; Payen, L.; Mahi, Y.; Vire, B.; Sands, M.; Evers, B.M.; Joubert, D.; et al. hPG80 (Circulating Progastrin), a Novel Blood-Based Biomarker for Detection of Poorly Differentiated Neuroendocrine Carcinoma and Well Differentiated Neuroendocrine Tumors. Cancers 2022, 14, 863. https://doi.org/10.3390/cancers14040863
Chauhan A, Prieur A, Kolesar J, Arnold S, Payen L, Mahi Y, Vire B, Sands M, Evers BM, Joubert D, et al. hPG80 (Circulating Progastrin), a Novel Blood-Based Biomarker for Detection of Poorly Differentiated Neuroendocrine Carcinoma and Well Differentiated Neuroendocrine Tumors. Cancers. 2022; 14(4):863. https://doi.org/10.3390/cancers14040863
Chicago/Turabian StyleChauhan, Aman, Alexandre Prieur, Jill Kolesar, Susanne Arnold, Léa Payen, Younes Mahi, Berengere Vire, Madison Sands, B. Mark Evers, Dominique Joubert, and et al. 2022. "hPG80 (Circulating Progastrin), a Novel Blood-Based Biomarker for Detection of Poorly Differentiated Neuroendocrine Carcinoma and Well Differentiated Neuroendocrine Tumors" Cancers 14, no. 4: 863. https://doi.org/10.3390/cancers14040863
APA StyleChauhan, A., Prieur, A., Kolesar, J., Arnold, S., Payen, L., Mahi, Y., Vire, B., Sands, M., Evers, B. M., Joubert, D., & Anthony, L. (2022). hPG80 (Circulating Progastrin), a Novel Blood-Based Biomarker for Detection of Poorly Differentiated Neuroendocrine Carcinoma and Well Differentiated Neuroendocrine Tumors. Cancers, 14(4), 863. https://doi.org/10.3390/cancers14040863