
Willingness and SARS-CoV-2 Vaccination Coverage among Healthcare Workers in China: A Nationwide Study


 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
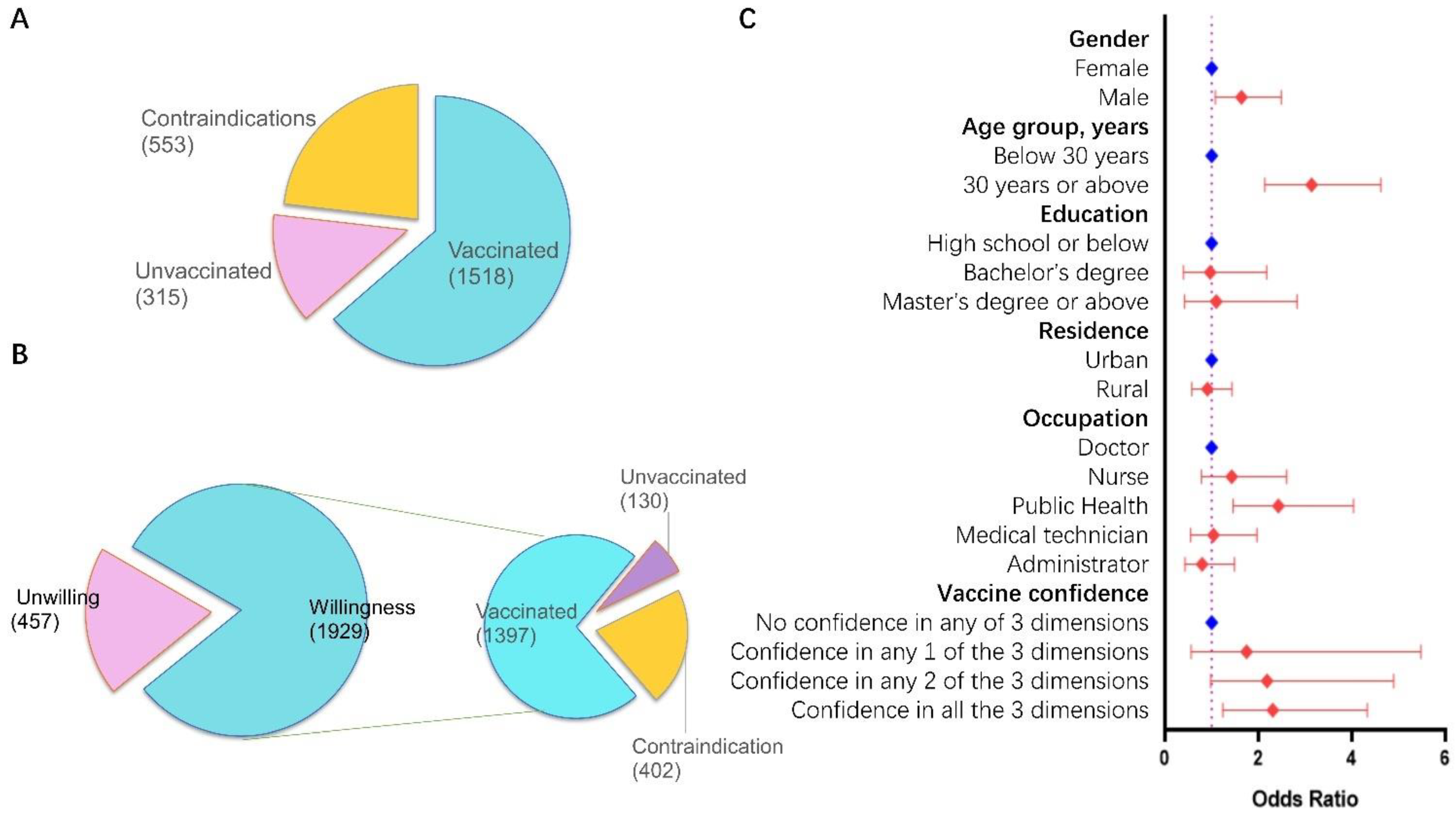
3.1. Overview of Participants’ Characters
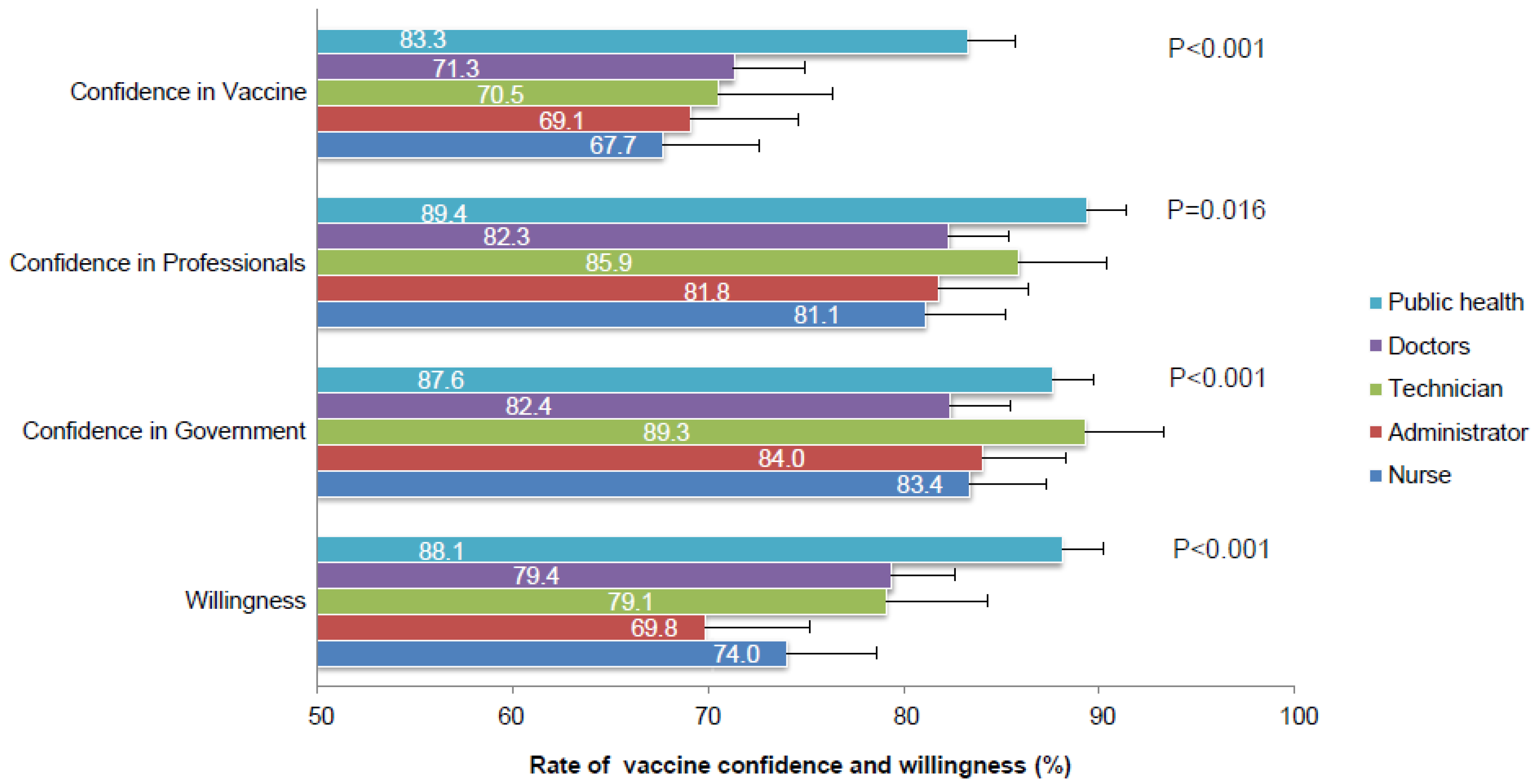
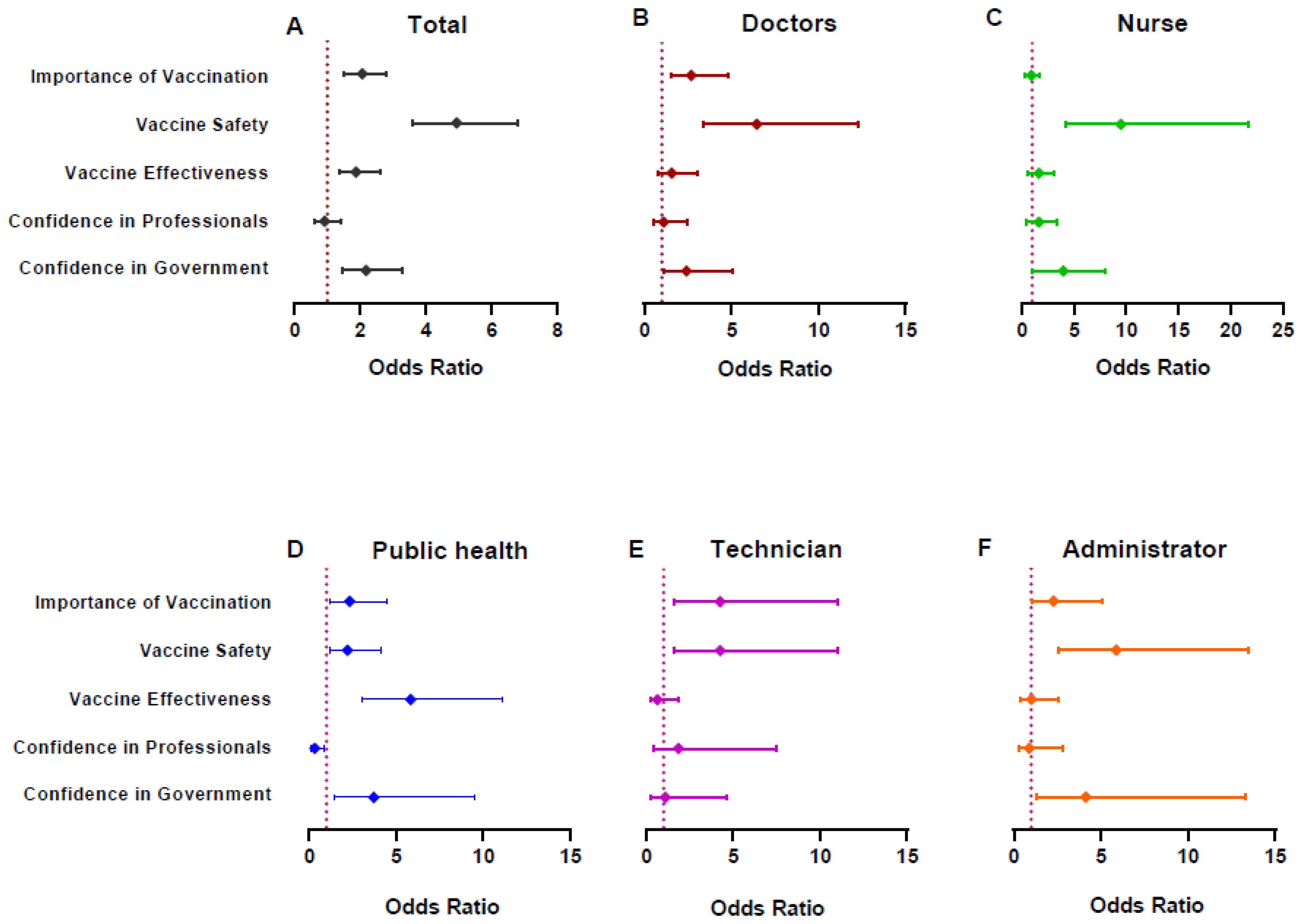
3.2. Analysis by Subgroups of HCWs
3.3. Combined Willingness & Vaccination Status Analysis
4. Discussions
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akande, O.W.; Akande, T.M. COVID-19 pandemic: A global health burden. Niger. Postgrad. Med. J. 2020, 27, 147–155. [Google Scholar] [CrossRef]
- Güner, R.; Hasanoğlu, I.; Aktaş, F. COVID-19: Prevention and control measures in community. Turk. J. Med Sci. 2020, 50, 571–577. [Google Scholar] [CrossRef]
- Sun, S.; Xie, Z.; Yu, K.; Jiang, B.; Zheng, S.; Pan, X. COVID-19 and healthcare system in China: Challenges and progression for a sustainable future. Glob. Health 2021, 17, 14. [Google Scholar] [CrossRef]
- Tse, D.M.-S.; Li, Z.; Lu, Y.; Li, Y.; Liu, Y.; Wong, W.C.W. Fighting against COVID-19: Preparedness and implications on clinical practice in primary care in Shenzhen, China. BMC Fam. Pract. 2020, 21, 271. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Wang, C.; Han, B.; Zhao, T.; Liu, H.; Liu, B.; Chen, L.; Xie, M.; Liu, J.; Zheng, H.; Zhang, S.; et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021, 39, 2833–2842. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Kukreti, S.; Lu, M.-Y.; Lin, Y.-H.; Strong, C.; Lin, C.-Y.; Ko, N.-Y.; Chen, P.-L.; Ko, W.-C. Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines 2021, 9, 246. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.; Ho, K.-F.; Cheung, A.; Yau, P.; Dong, D.; Wong, S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Wang, J.; Feng, Y.; Hou, Z.; Lu, Y.; Chen, H.; Ouyang, L.; Wang, N.; Fu, H.; Wang, S.; Kan, X.; et al. Willingness to receive SARS-CoV-2 vaccine among healthcare workers in public institutions of Zhejiang Province, China. Hum. Vaccin Immunother. 2021, 17, 2926–2933. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 1–8, in press. [Google Scholar] [CrossRef]
- Chang, D.; Xu, H.; Rebaza, A.; Sharma, L.; Cruz, C.S.D. Protecting health-care workers from subclinical coronavirus infection. Lancet Respir. Med. 2020, 8, e13. [Google Scholar] [CrossRef] [Green Version]
- Hanrath, A.T.; van der Loeff, I.S.; Lendrem, D.W.; Baker, K.F.; Price, D.A.; McDowall, P.; McDowall, K.; Cook, S.; Towns, P.; Schwab, U.; et al. SARS-CoV-2 Testing of 11,884 Healthcare Workers at an Acute NHS Hospital Trust in England: A Retrospective Analysis. Front. Med. 2021, 8, 636160. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Huang, Z.; Xiao, Y.; Huang, X.; Fan, X.-G. Protecting Chinese healthcare workers while combating the 2019 novel coronavirus. Infect. Control. Hosp. Epidemiol. 2020, 41, 745–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, R.; Penders, B.; Horstman, K. Addressing Vaccine Hesitancy in China: A Scoping Review of Chinese Scholarship. Vaccines 2019, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, J.V.; Picchio, C.A.; Nayagam, A.S.; Ratzan, S.; Thursz, M. Strengthening vaccine confidence during the COVID-19 pandemic: A new opportunity for global hepatitis B virus elimination. J. Hepatol. 2020, 73, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Sun, S.; Lin, D.; Operario, D. Interest in COVID-19 vaccine trials participation among young adults in China: Willingness, reasons for hesitancy, and demographic and psychosocial determinants. Prev. Med. Rep. 2021, 22, 101350. [Google Scholar] [CrossRef]
- Udow-Phillips, M.; Lantz, P.M. Trust in Public Health Is Essential Amid the COVID-19 Pandemic. J. Hosp. Med. 2020, 15, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef]
- He, S.; Chen, S.; Kong, L.; Liu, W. Analysis of Risk Perceptions and Related Factors Concerning COVID-19 Epidemic in Chongqing, China. J. Community Health 2021, 46, 278–285. [Google Scholar] [CrossRef]
- Du, F.; Chantler, T.; Francis, M.R.; Sun, F.Y.; Zhang, X.; Han, K.; Rodewald, L.; Yu, H.; Tu, S.; Larson, H.; et al. The determinants of vaccine hesitancy in China: A cross-sectional study following the Changchun Changsheng vaccine incident. Vaccine 2020, 38, 7464–7471. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Alsuliman, M.; Ahmed, G.Y.; Rabaan, A.A.; Al-Tawfiq, J.A.; Al-Omari, A. Knowledge of infection prevention and control among healthcare workers and factors influencing compliance: A systematic review. Antimicrob. Resist. Infect. Control. 2021, 10, 86. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Di Giuseppe, G.; Pelullo, C.P.; Della, P.G.; Montemurro, M.V.; Napolitano, F.; Pavia, M.; Angelillo, I.F. Surveying willingness toward SARS-CoV-2 vaccination of healthcare workers in Italy. Expert Rev. Vaccines 2021, 20, 881–889. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’ (HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021. Published Online First: 30 June 2021. [Google Scholar] [CrossRef]
- Kabamba, N.M.; Kabamba, N.L.; Ngoie, M.G.; Banza, N.D.; Mbidi, M.J.; Luhata, L.C.; Lora, M.B.; Cikomola, M.B.A.; Mukamba, M.E. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V.; Fradelos, E.C.; Daniil, Z.; Rachiotis, G.; Gourgoulianis, K.I. Assessment of Knowledge, Attitudes, and Practices towards New Coronavirus (SARS-CoV-2) of Health Care Professionals in Greece before the Outbreak Period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A. Willingness of health care workers of various nationalities to accept H1N1 (2009) pandemic influenza A vaccination. Ann. Saudi Med. 2012, 32, 64–67. [Google Scholar] [CrossRef]
- Kaboli, F.; Astrakianakis, G.; Li, G.; Guzman, J.; Naus, M.; Donovan, T. Influenza Vaccination and Intention to Receive the Pandemic H1N1 Influenza Vaccine among Healthcare Workers of British Columbia, Canada: A Cross-Sectional Study. Infect. Control. Hosp. Epidemiol. 2010, 31, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Torun, S.D.; Torun, F.; Catak, B. Healthcare workers as parents: Attitudes toward vaccinating their children against pandemic influenza A/H1N1. BMC Public Health 2010, 10, 596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Randolph, H.E.; Barreiro, L.B. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Trucchi, C.; Restivo, V.; Amicizia, D.; Fortunato, F.; Manca, A.; Martinelli, D.; Montecucco, A.; Piazza, M.F.; Prato, R.; Tisa, V.; et al. Italian Health Care Workers’ Knowledge, Attitudes, and Practices Regarding Human Papillomavirus Infection and Prevention. Int. J. Environ. Res. Public Health 2020, 17, 5278. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Grech, V.; Gauci, C.; Agius, S. Withdrawn: Vaccine hesitancy among Maltese Healthcare workers toward influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020, 105213. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Di Martino, G.; Di Giovanni, P.; Di Girolamo, A.; Scampoli, P.; Cedrone, F.; D’Addezio, M.; Meo, F.; Romano, F.; Di Sciascio, M.B.; Staniscia, T. Knowledge and Attitude towards Vaccination among Healthcare Workers: A Multicenter Cross-Sectional Study in a Southern Italian Region. Vaccines 2020, 8, 248. [Google Scholar] [CrossRef] [PubMed]
- Formeister, E.J.; Chien, W.; Agrawal, Y.; Carey, J.P.; Stewart, C.M.; Sun, D.Q. Preliminary Analysis of Association Between COVID-19 Vaccination and Sudden Hearing Loss Using US Centers for Disease Control and Prevention Vaccine Adverse Events Reporting System Data. JAMA Otolaryngol. Neck Surg. 2021, 147, 674. [Google Scholar] [CrossRef] [PubMed]
- Palgi, Y.; Bergman, Y.S.; Ben-David, B.; Bodner, E. No psychological vaccination: Vaccine hesitancy is associated with negative psychiatric outcomes among Israelis who received COVID-19 vaccination. J. Affect. Disord. 2021, 287, 352–353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total n (%) | Doctor n (%) | Nurse n (%) | Public Health n (%) | Technician n (%) | Administrator n (%) | p |
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Male | 884 (37.0) | 274 (45.4) | 27 (7.7) | 395 (42.7) | 81 (34.6) | 107 (38.9) | <0.001 |
| Female | 1502 (63.0) | 329 (54.6) | 323 (92.3) | 529 (57.3) | 153 (65.4) | 168 (61.1) | |
| Age group, years | |||||||
| below 30 | 621 (26.0) | 144 (23.9) | 129 (36.9) | 197 (21.3) | 77 (32.9) | 74 (26.9) | <0.001 |
| 30 to 39 | 790 (33.1) | 209 (34.7) | 130 (37.1) | 272 (29.4) | 84 (35.9) | 95 (34.5) | |
| 40 to 49 | 627 (26.3) | 170 (28.2) | 67 (19.1) | 278 (30.1) | 44 (18.8) | 68 (24.7) | |
| 50 or above | 348 (14.6) | 80 (13.2) | 24 (6.9) | 177 (19.2) | 29 (12.4) | 38 (13.8) | |
| Education | |||||||
| Below bachelor | 160 (6.7) | 29 (4.8) | 28 (8.0) | 63 (6.8) | 13 (5.6) | 27 (9.8) | <0.001 |
| Bachelor | 1684 (70.6) | 380 (63.0) | 321 (91.7) | 646 (69.9) | 157 (67.1) | 180 (65.5) | |
| Master or above | 542 (22.7) | 194 (32.2) | 1 (0.3) | 215 (23.3) | 64 (27.4) | 68 (24.7) | |
| Residence | |||||||
| Urban | 1820 (76.3) | 431 (71.5) | 219 (62.6) | 767 (83.0) | 177 (75.6) | 226 (82.2) | <0.001 |
| Rural | 566 (23.7) | 172 (28.5) | 131 (37.4) | 157 (17.0) | 57 (24.4) | 49 (17.8) | |
| Total | 2386 (100) | 603 (25.3) | 350 (14.7) | 924 (38.7) | 234 (9.8) | 275 (11.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Wang, Y.; Han, B.; Zhao, T.-S.; Liu, B.; Liu, H.; Chen, L.; Xie, M.; Zheng, H.; Zhang, S.; et al. Willingness and SARS-CoV-2 Vaccination Coverage among Healthcare Workers in China: A Nationwide Study. Vaccines 2021, 9, 993. https://doi.org/10.3390/vaccines9090993
Wang C, Wang Y, Han B, Zhao T-S, Liu B, Liu H, Chen L, Xie M, Zheng H, Zhang S, et al. Willingness and SARS-CoV-2 Vaccination Coverage among Healthcare Workers in China: A Nationwide Study. Vaccines. 2021; 9(9):993. https://doi.org/10.3390/vaccines9090993
Chicago/Turabian StyleWang, Chao, Yu Wang, Bingfeng Han, Tian-Shuo Zhao, Bei Liu, Hanyu Liu, Linyi Chen, Mingzhu Xie, Hui Zheng, Sihui Zhang, and et al. 2021. "Willingness and SARS-CoV-2 Vaccination Coverage among Healthcare Workers in China: A Nationwide Study" Vaccines 9, no. 9: 993. https://doi.org/10.3390/vaccines9090993