
Analysis of Factors Associated with Hiccups Using the FAERS Database



Abstract
1. Introduction
2. Results
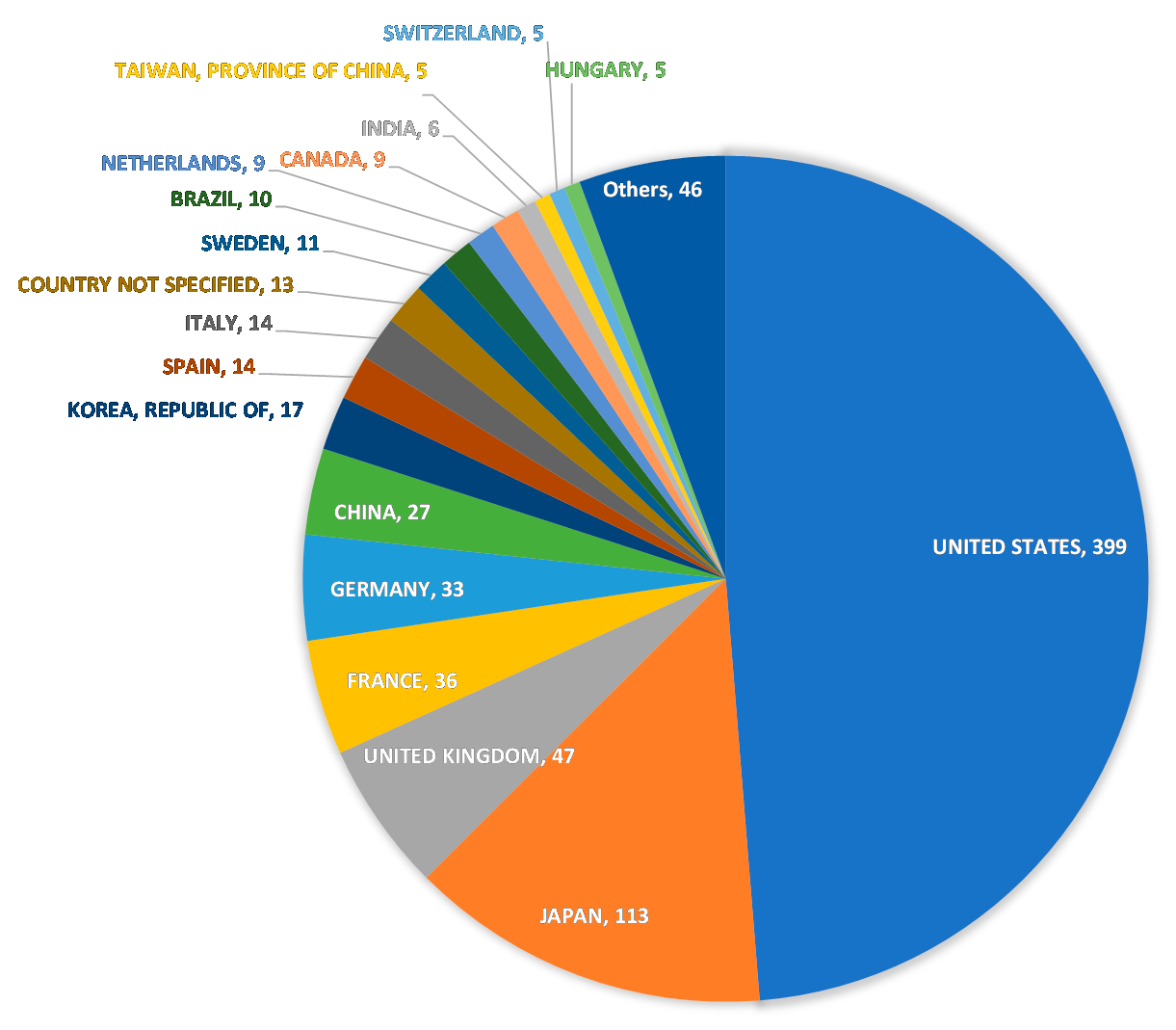
2.1. Database
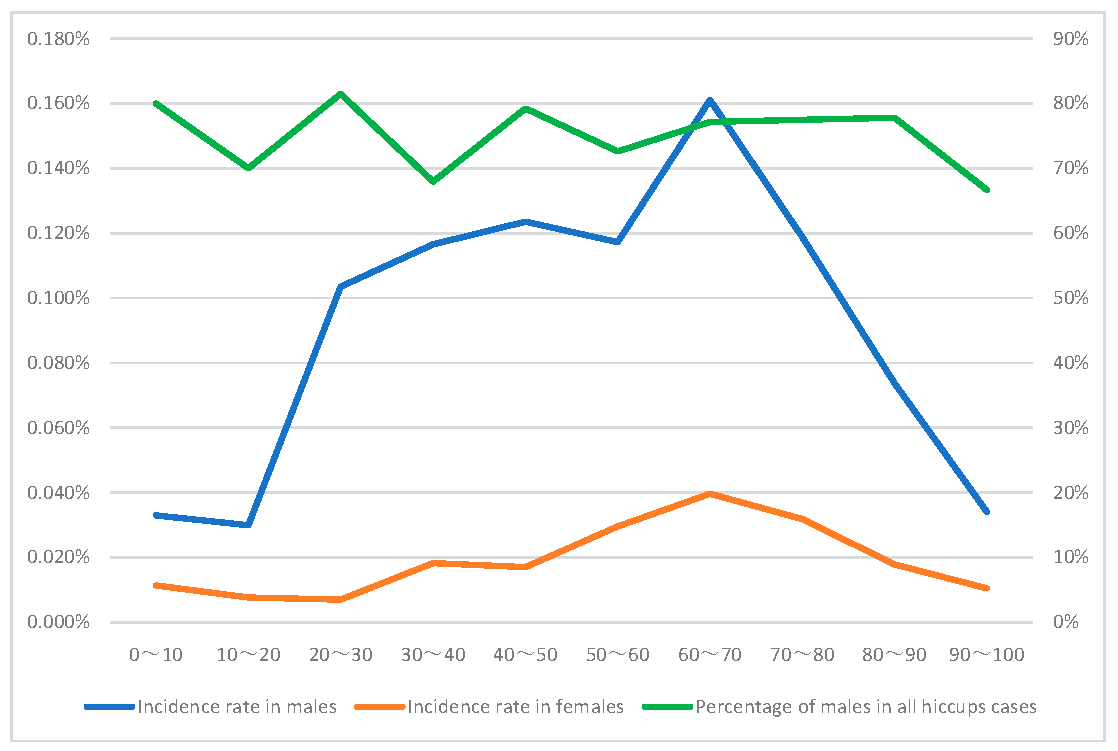
2.2. Patient Information
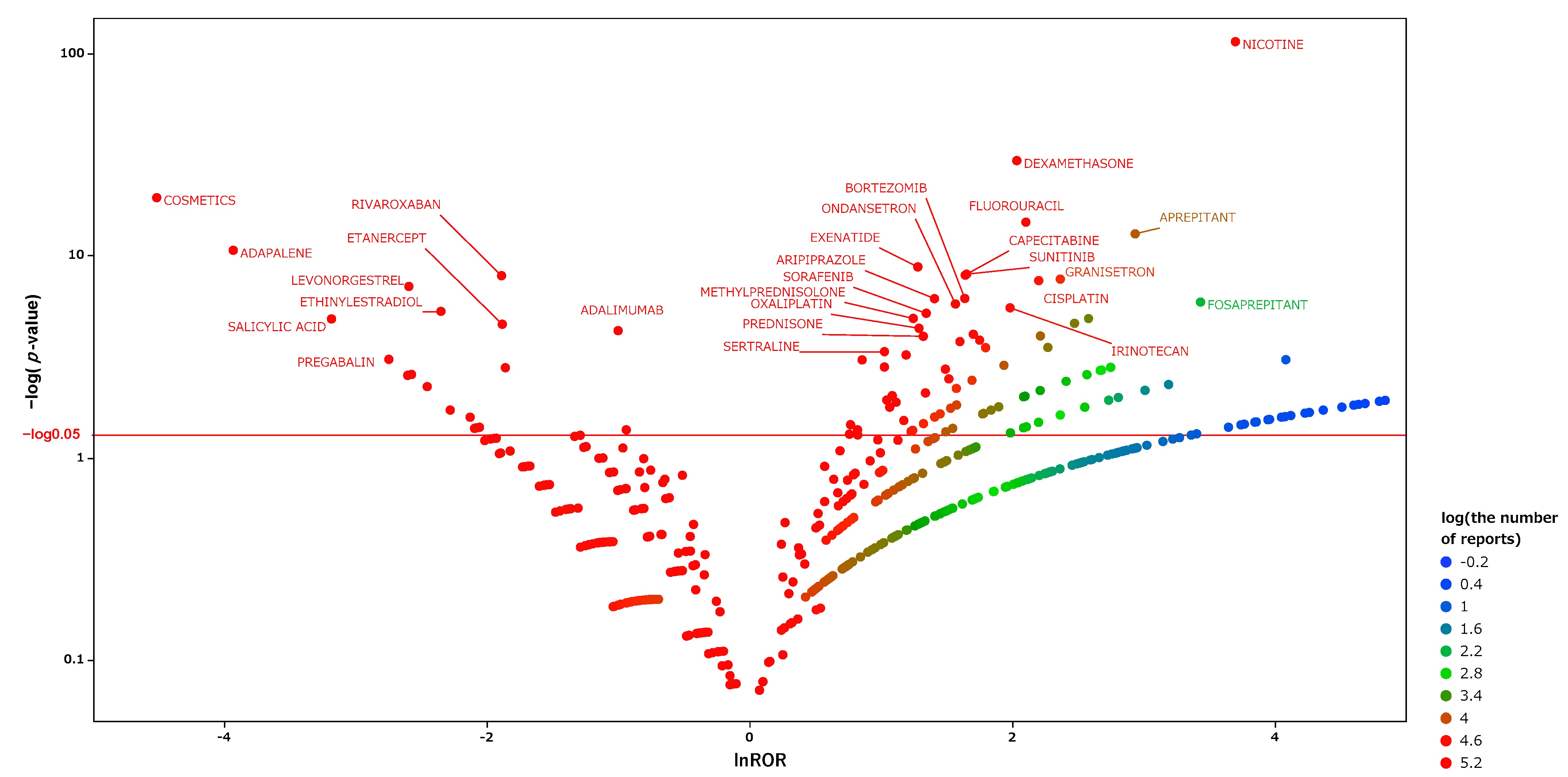
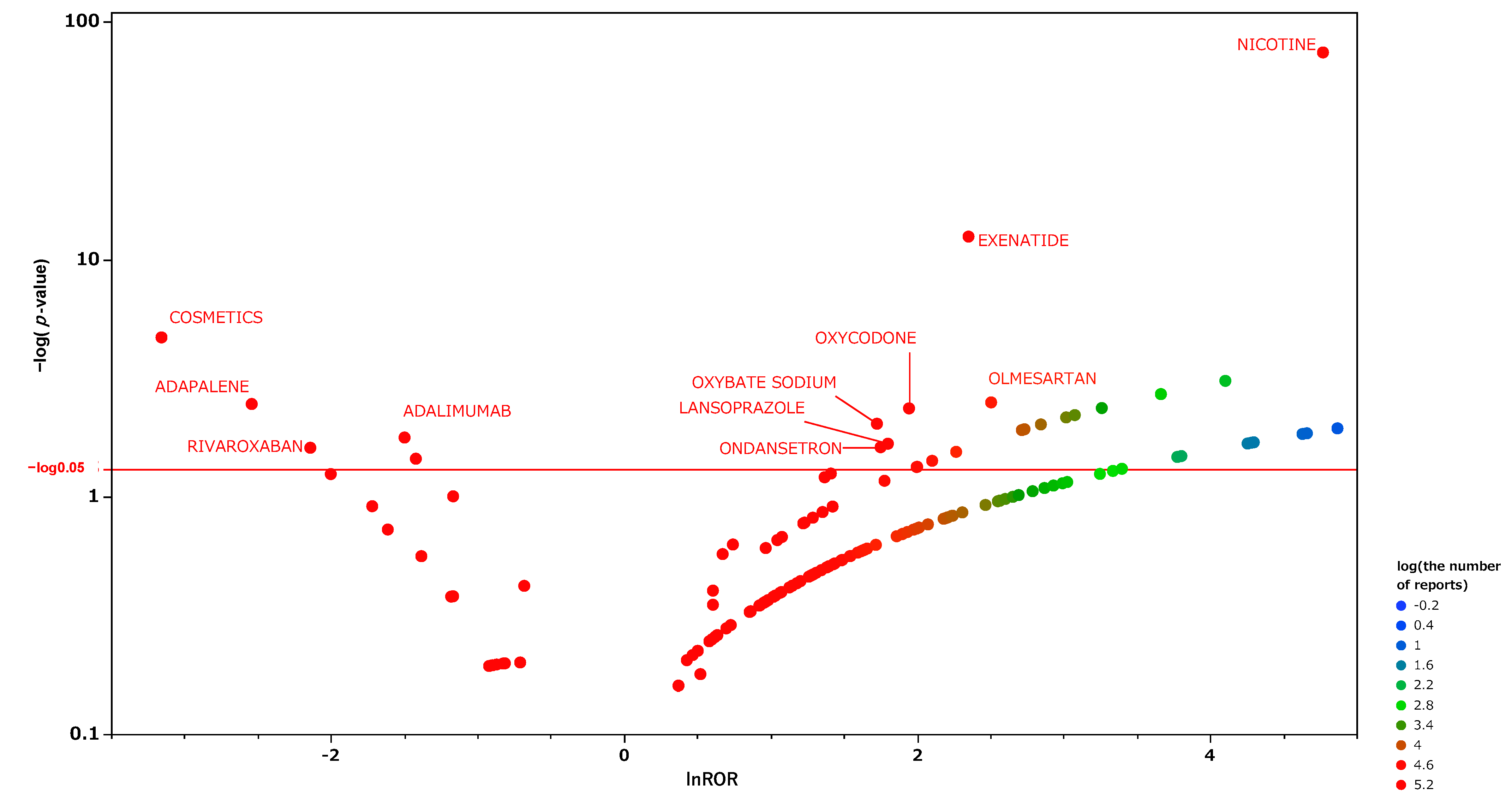
2.3. Hiccup-Inducing Medications
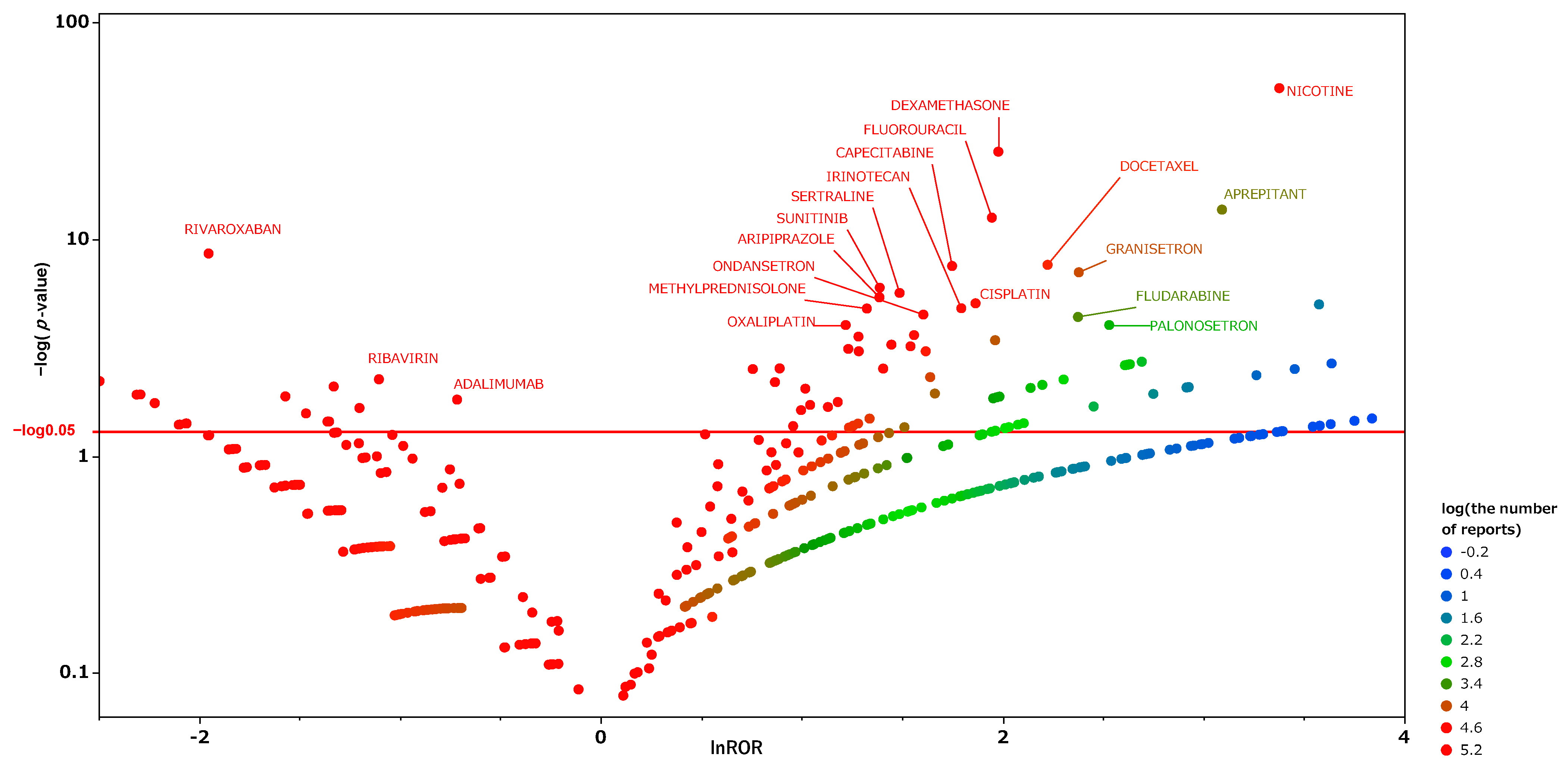
2.4. Risk Factors for Hiccups in Males
2.5. Risk Factors for Hiccups in Females
3. Discussion
4. Materials and Methods
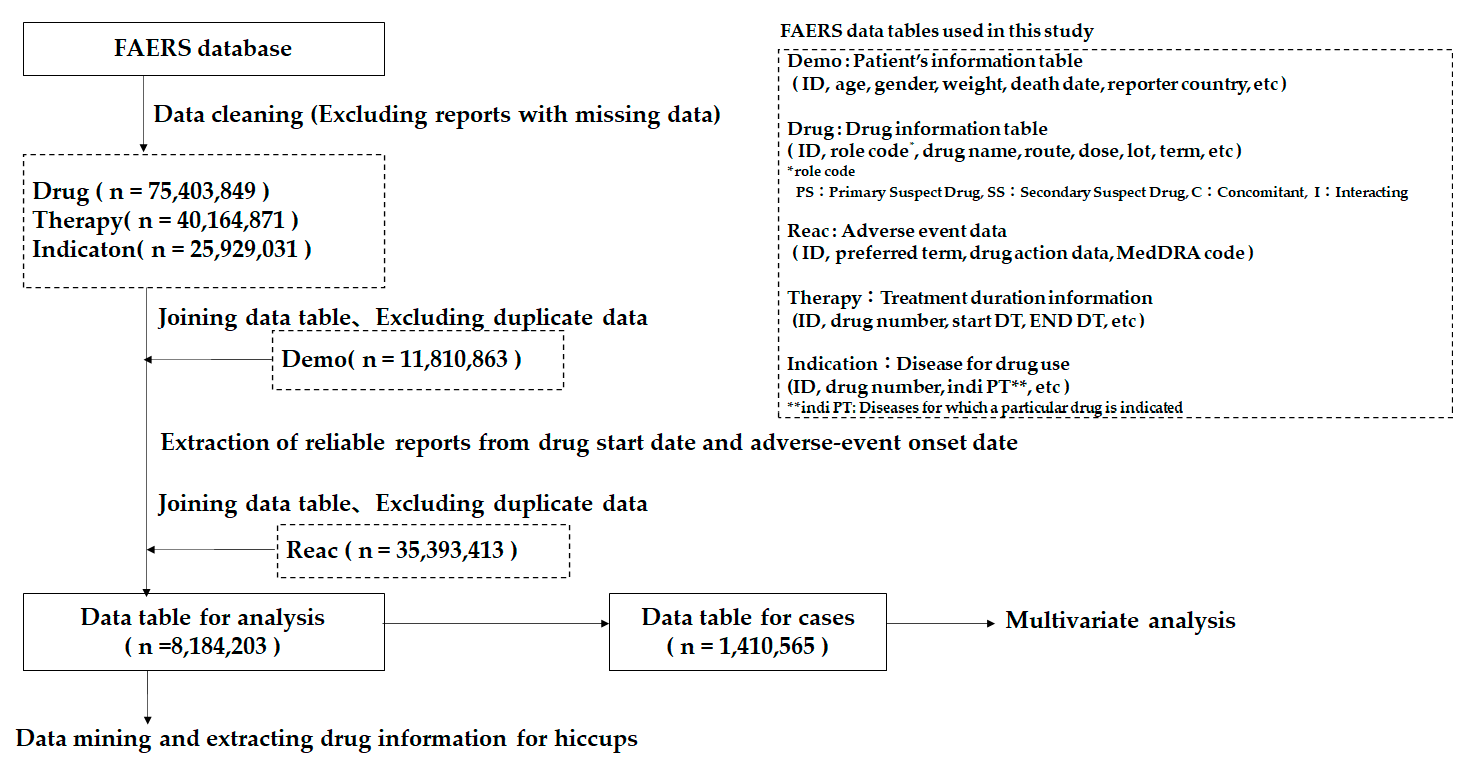
4.1. Data Source
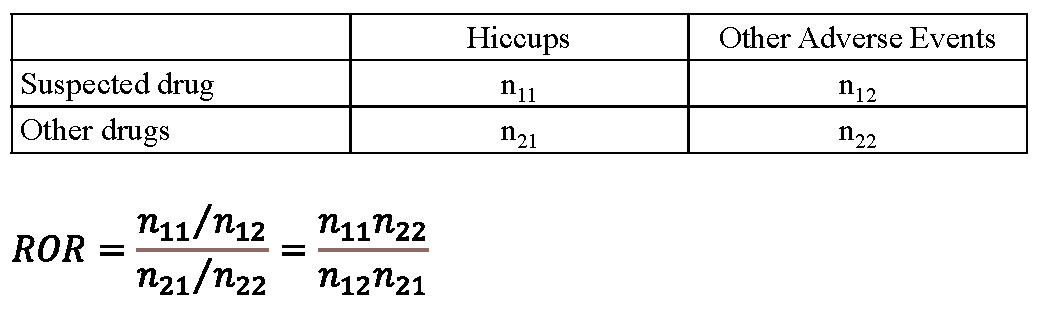
4.2. Definitions of the Terms Adverse-Event and Suspect Medicine
4.3. Production of the Data Analysis Table
4.4. Extraction of Suspect Drugs for Hiccups Using Data Mining Methods
4.5. Relationship between Patient Information and Hiccups
4.6. Multivariate Analysis
4.7. Subgroup Analysis of the Two Separate Groups of Men and Women
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Becker, D.E. Nausea, Vomiting, and Hiccups: A Review of Mechanisms and Treatment. Anesth. Prog. 2010, 57, 150–157. [Google Scholar] [CrossRef]
- Kolodzik, P.W.; Eilers, M.A. Hiccups (singultus): Review and approach to management. Ann. Emerg. Med. 1991, 20, 565–573. [Google Scholar] [CrossRef]
- Kondo, T.; Toyooka, H.; Arita, H. Hiccup reflex is mediated by pharyngeal branch of glossopharyngeal nerve in cats. Neurosci. Res. 2003, 47, 317–321. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0168010203002256 (accessed on 4 November 2021). [CrossRef]
- Oshima, T.; Sakamoto, M.; Tatsuta, H.; Arita, H. GABAergic inhibition of hiccup-like reflex induced by electrical stimulation in medulla of cats. Neurosci. Res. 1998, 30, 287–293. [Google Scholar] [CrossRef]
- Nausheen, F.; Mohsin, H.; Lakhan, S.E. Neurotransmitters in Hiccups; SpringerOpen: Berlin/Heidelberg, Germany, 2016; Volume 5. [Google Scholar]
- Lee, G.-W.; Kim, R.B.; Go, S.I.; Cho, H.S.; Lee, S.J.; Hui, D.; Bruera, E.; Kang, J.H. Gender Differences in Hiccup Patients: Analysis of Published Case Reports and Case-Control Studies. J. Pain Symptom Manag. 2016, 51, 278–283. [Google Scholar] [CrossRef]
- Silverman, M.A.; Leung, J.G.; Schak, K.M. Aripiprazole-associated hiccups: A case and closer look at the association between hiccups and antipsychotics. J. Pharm. Pract. 2014, 27, 587–590. [Google Scholar] [CrossRef]
- Hayashi, M.; Sugimura, H.; Suga, Y.; Kawahara, M.; Aimiya, K.; Miyamoto, K.-I. Study on Risk Factors for Hiccups Induced by Cisplatin-based Chemotherapy. Jpn. J. Pharm. Health Care Sci. 2009, 35, 89–95. [Google Scholar] [CrossRef][Green Version]
- Toriumi, S.; Nakazawa, K.; Shoji, M. Effect of Antiemetic Agents on Hiccups during Chemotherapy in Patients with Lung Cancer. Pharmacol. Pharm. 2018, 9, 124–133. [Google Scholar] [CrossRef]
- Lee, G.-W.; Oh, S.Y.; Kang, M.H.; Kang, J.H.; Park, S.H.; Hwang, I.G.; Yi, S.Y.; Choi, Y.J.; Ji, J.H.; Lee, H.Y.; et al. Treatment of Dexamethasone-Induced Hiccup in Chemotherapy Patients by Methylprednisolone Rotation. Oncologist 2013, 18, 1229–1234. [Google Scholar] [CrossRef]
- Hosoya, R.; Uesawa, Y.; Ishii-Nozawa, R.; Kagaya, H. Analysis of factors associated with hiccups based on the Japanese Adverse Drug Event Report database. PLoS ONE 2017, 12, e0172057. [Google Scholar] [CrossRef]
- Hosoya, R.; Tanaka, I.; Nozawa, R.I.; Amino, T.; Kamata, T.; Hino, S.; Kagaya, H.; Uesawa, Y. Demographic and clinical risk factors of hiccups. J. Pharm. Pharmacol. Sci. Res. 2018, 3, 167. [Google Scholar] [CrossRef]
- Hosoya, R.; Tanaka, I.; Ishii-Nozawa, R.; Amino, T.; Kamata, T.; Hino, S.; Kagaya, H.; Uesawa, Y. Risk Factors for Cancer Chemotherapy-Induced Hiccups (CIH). Pharmacol. Pharm. 2018, 9, 331–343. [Google Scholar] [CrossRef]
- FDA FAERS. Available online: https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard (accessed on 4 November 2021).
- Petroianu, G.A.; Lorke, D.E. The Role of Serotonin in Singultus: A Review. Front. Neurosci. 2020, 14, 629. [Google Scholar] [CrossRef]
- Horii, K.; Ehara, Y.; Shiina, T.; Naitou, K.; Nakamori, H.; Horii, Y.; Shimaoka, H.; Saito, S.; Shimizu, Y. Sexually dimorphic response of colorectal motility to noxious stimuli in the colorectum in rats. J. Physiol. 2021, 599, 1421–1437. [Google Scholar] [CrossRef]
- Baumann, A.; Weicker, T.; Alb, I.; Audibert, G. Baclofen for the treatment of hiccup related to brainstem compression. Ann. Fr. d’Anesthésie Réanim. 2014, 33, e27–e28. [Google Scholar] [CrossRef] [PubMed]
- Yamada, J.; Okabe, A.; Toyoda, H.; Kilb, W.; Luhmann, H.J.; Fukuda, A. Cl− uptake promoting depolarizing GABA actions in immature rat neocortical neurones is mediated by NKCC1. J. Physiol. 2004, 557, 829–841. [Google Scholar] [CrossRef]
- Einarson, T.R.; Einarson, A. Hiccups following nicotine gum use. Ann. Pharmacother. 1997, 31, 1263–1264. [Google Scholar] [CrossRef] [PubMed]
- Balfour, D. The effects of nicotine on brain neurotransmitter systems. Pharmacol. Ther. 1982, 16, 269–282. [Google Scholar] [CrossRef]
- Goodman, F. Effects of nicotine on distribution and release of 14C-norepinephrine and 14C-dopamine in rat brain striatum and hypothalamus slices. Neuropharmacology 1974, 13, 1025–1032. [Google Scholar] [CrossRef]
- Jeon, Y.S.; Kearney, A.M.; Baker, P.G. Management of hiccups in palliative care patients. BMJ Support. Palliat. Care 2017, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Stewart, B.L.; Redeker, A.G. EMESIS AND HICCOUGH—Treatment with Chlorpromazine. Calif. Med. 1954, 81, 203–205. [Google Scholar]
- Yonemura, K.; Miyanaga, K. Profiles of Affinity of Antipsychotic Drug for Neurotransmitter Receptors and Their Clinical Inplication. Kitakanto Med. J. 1998, 48, 87–102. [Google Scholar] [CrossRef][Green Version]
- Gerschlager, W.; Bloem, B.R. Hiccups associated with levodopa in Parkinson’s disease. Mov. Disord. 2009, 24, 621–622. [Google Scholar] [CrossRef] [PubMed]
- Kani, A.S.; Ocek, T.; Aksoy-Poyraz, C.; Turan, S.; Duran, A. Aripiprazole-Induced Acute Hiccups: A Case Report. J. Neuropsychiatry Clin. Neurosci. 2015, 27, 60. [Google Scholar] [CrossRef] [PubMed]
- Hori, H.; Nakamura, J. Hiccups Associated With Switching From Olanzapine to Aripiprazole in a Patient with Paranoid Schizophrenia. Clin. Neuropharmacol. 2014, 37, 88–89. [Google Scholar] [CrossRef]
- Ray, P.; Haq, M.Z.U.; Nizamie, S.H. Aripiprazole-induced hiccups: A case report. Gen. Hosp. Psychiatry 2009, 31, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Alefishat, E.; Aloum, L.; Baltatu, O.C.; Petroianu, G.A. The action of aripiprazole and brexpiprazole at the receptor level in singultus. J. Integr. Neurosci. 2021, 20, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Bilgiç, A. Possible Sertraline-Induced Hiccups in a Boy with Obsessive-Compulsive Disorder and Attention-Deficit/Hyperactivity Disorder. Clin. Neuropharmacol. 2019, 42, 17–18. [Google Scholar] [CrossRef]
- Vaidya, V. Sertraline in the Treatment of Hiccups. J. Psychosom. Res. 2000, 41, 353–355. [Google Scholar] [CrossRef]
- Owens, M.J.; Knight, D.L.; Nemeroff, C.B. Second-generation SSRIs: Human monoamine transporter binding profile of escitalopram and R-fluoxetine. Biol. Psychiatry 2001, 50, 345–350. [Google Scholar] [CrossRef]
- Vardy, J.; Chiew, K.; Galica, J.; Pond, G.R.; Tannock, I.F. Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br. J. Cancer 2006, 94, 1011–1015. [Google Scholar] [CrossRef]
- Chu, C.-C.; Hsing, C.-H.; Shieh, J.-P.; Chien, C.-C.; Ho, C.-M.; Wang, J.-J. The cellular mechanisms of the antiemetic action of dexamethasone and related glucocorticoids against vomiting. Eur. J. Pharmacol. 2014, 722, 48–54. [Google Scholar] [CrossRef]
- Kondo, T. Three cases of drug-induced hiccup: Causative drugs and mechanisms–The relationship with GABA receptor action. J. Jpn. Assoc. Acute Med. 2019, 30, 115–135. [Google Scholar]
- Popoli, M.; Yan, Z.; Mcewen, B.S.; Sanacora, G. The Stressed Synapse: The Impact of Stress and Glucocorticoids on Glutamate Transmission. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3645314/ (accessed on 4 November 2021).
- Liaw, C.-C.; Wang, C.-H.; Chang, H.-K.; Wang, H.-M.; Huang, J.-S.; Lin, Y.-C.; Chen, J.-S. Cisplatin-Related Hiccups: Male Predominance, Induction by Dexamethasone, and Protection against Nausea and Vomiting. J. Pain Symptom Manag. 2005, 30, 359–366. [Google Scholar] [CrossRef]
- Grunberg, S.M.; Hesketh, P.J. Control of chemotherapy-induced emesis. N. Engl. J. Med. 1993, 329, 1008–1012. [Google Scholar]
- ATGAM Info. 2018. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=e19acee5-ff33-45a5-bbbf-801756bc59b4 (accessed on 3 October 2021).
- Klibanov, O.M.; Gale, S.E.; Santevecchi, B. Ombitasvir/Paritaprevir/Ritonavir and Dasabuvir Tablets for Hepatitis C Virus Genotype 1 Infection. Ann. Pharmacother. 2015, 49, 566–581. [Google Scholar] [CrossRef] [PubMed]
- Yabe, D.; Seino, Y. Defining the role of GLP-1 receptor agonists for individualized treatment of Type 2 diabetes. Expert Rev. Endocrinol. Metab. 2014, 9, 659–670. [Google Scholar] [CrossRef]
- Busardò, F.P.; Kyriakou, C.; Napoletano, S.; Marinelli, E.; Zaami, S. Clinical Applications of Sodium Oxybate (GHB): From Narcolepsy to Alcohol Withdrawal Syndrome. Available online: https://www.europeanreview.org/article/9952 (accessed on 4 November 2021).
- Maeda, R. JADER from Pharmacovigilance Point of View. Jpn. J. Pharmacoepidemiol. Ekigaku 2014, 19, 51–56. [Google Scholar] [CrossRef]
- Avillach, P.; Salvo, F.; Thiessard, F.; Miremont-Salamé, G.; Fourrier-Reglat, A.; Haramburu, F.; Bégaud, B.; Moore, N.; Pariente, A.; on behalf of l’Association des Centres Régionaux de Pharmacovigilance. Pilot evaluation of an automated method to decrease false-positive signals induced by co-prescriptions in spontaneous reporting databases. Pharmacoepidemiol. Drug Saf. 2014, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- MedDRA. Available online: https://www.meddra.org/26 (accessed on 4 November 2021).
- Kurosaki, K.; Wu, R.; Uesawa, Y. A Toxicity Prediction Tool for Potential Agonist/Antagonist Activities in Molecular Initiating Events Based on Chemical Structures. Int. J. Mol. Sci. 2020, 21, 7853. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| a. All data table | ||||
| Number of cases | Hiccups (N = 843) | Non-hiccups (N = 1,409,722) | p-Value | |
| Gender (M/F) | 1,348,038 | 622/193 | 544,997/803,041 | <0.001 |
| age_YR | 1,202,581 | 59.28 ± 0.76 | 54.63 ± 0.04 | <0.001 |
| wt_KG | 541,174 | 74.37 ± 1.36 | 73.12 ± 0.01 | 0.3561 |
| b. Male data table | ||||
| Number of cases | Hiccups (N = 622) | Non-hiccups (N = 544,997) | p-Value | |
| age_YR | 483,580 | 59.35 ± 0.86 | 57.59 ± 0.03 | 0.0391 |
| wt_KG | 231,008 | 75.81 ± 1.58 | 78.51 ± 0.06 | 0.0882 |
| c. Female data table | ||||
| Number of cases | Hiccups (N = 193) | Non-hiccups (N = 803,041) | p-Value | |
| age_YR | 709,459 | 59.02 ± 1.59 | 52.61 ± 0.02 | <0.001 |
| wt_KG | 307,508 | 69.72 ± 2.88 | 69.08 ± 0.05 | 0.8229 |
| Odds Ratio | CI (95%) | |
|---|---|---|
| NICOTINE | 93.38 * | 69.92–124.72 |
| FLUOROURACIL | 8.22 * | 4.38–15.43 |
| SUNITINIB | 8.19 * | 4.67–14.38 |
| ARIPIPRAZOLE | 8.14 * | 3.99–16.60 |
| EXENATIDE | 7.52 * | 3.51–16.11 |
| ANTITHYMOCYTE IMMUNOGLOBULIN | 6.89 * | 2.75–17.24 |
| SERTRALINE | 6.32 * | 3.11–12.84 |
| CAPECITABINE | 6.01 * | 3.36–10.76 |
| Gender (male: 1, female: 0) | 5.19 * | 4.06–6.63 |
| GEMCITABINE | 4.34 * | 1.98–9.48 |
| GRANISETRON | 4.01 * | 1.89–8.51 |
| DEXAMETHASONE | 3.48 * | 2.09–5.79 |
| BORTEZOMIB | 3.47 * | 1.62–7.46 |
| SORAFENIB | 3.20 * | 1.50–6.81 |
| CISPLATIN | 2.62 * | 1.17–5.87 |
| METHYLPREDNISOLONE | 2.30 * | 1.06–5.01 |
| PREDNISONE | 2.02 | 0.75–5.48 |
| BEVACIZUMAB | 1.76 | 0.85–3.64 |
| IRINOTECAN | 1.70 | 0.74–3.87 |
| ONDANSETRON | 1.69 | 0.72–4.00 |
| age_YR | 1.01 * | 1.003–1.014 |
| wt_KG | 0.99 * | 0.989–0.998 |
| OXALIPLATIN | 0.91 | 0.43–1.93 |
| LENALIDOMIDE | 0.51 | 0.18–1.42 |
| FOLINIC ACID | 0.38 | 0.11–1.31 |
| Odds Ratio | CI (95%) | |
|---|---|---|
| NICOTINE | 61.73 * | 42.16–90.38 |
| ARIPIPRAZOLE | 9.26 * | 4.52–19.01 |
| FLUOROURACIL | 8.90 * | 4.65–17.05 |
| SERTRALINE | 8.65 * | 4.24–17.64 |
| ANTITHYMOCYTE IMMUNOGLOBULIN | 8.57 * | 3.54–20.77 |
| SUNITINIB | 8.33 * | 4.63–14.99 |
| CAPECITABINE | 6.97 * | 3.79–12.80 |
| GEMCITABINE | 5.12 * | 2.32–11.30 |
| DEXAMETHASONE | 4.47 * | 2.83–7.06 |
| METHYLPREDNISOLONE | 2.79 * | 1.30–5.98 |
| BORTEZOMIB | 2.59 * | 1.15–5.83 |
| CISPLATIN | 2.51 * | 1.09–5.75 |
| PREDNISONE | 2.31 | 0.86–6.25 |
| age_YR | 2.23 * | 1.09–4.56 |
| DOCETAXEL | 1.88 | 0.44–8.09 |
| IRINOTECAN | 1.86 | 0.80–4.31 |
| BEVACIZUMAB | 1.71 | 0.79–3.69 |
| ONDANSETRON | 1.67 | 0.70–4.00 |
| OXALIPLATIN | 0.97 | 0.45–2.06 |
| FOLINIC ACID | 0.43 | 0.12–1.48 |
| wt_KG | 0.10 * | 0.02–0.59 |
| Odds Ratio | CI (95%) | |
|---|---|---|
| NICOTINE | 192.16 * | 120.75–305.79 |
| DASABUVIR | 23.65 * | 5.73–97.67 |
| EXENATIDE | 11.38 * | 3.46–37.44 |
| SODIUM OXYBATE | 11.17 * | 1.53–81.85 |
| age_YR | 1.01 * | 1.001–1.026 |
| wt_KG | 1.00 | 0.988–1.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosoya, R.; Ishii-Nozawa, R.; Kurosaki, K.; Uesawa, Y. Analysis of Factors Associated with Hiccups Using the FAERS Database. Pharmaceuticals 2022, 15, 27. https://doi.org/10.3390/ph15010027
Hosoya R, Ishii-Nozawa R, Kurosaki K, Uesawa Y. Analysis of Factors Associated with Hiccups Using the FAERS Database. Pharmaceuticals. 2022; 15(1):27. https://doi.org/10.3390/ph15010027
Chicago/Turabian StyleHosoya, Ryuichiro, Reiko Ishii-Nozawa, Kota Kurosaki, and Yoshihiro Uesawa. 2022. "Analysis of Factors Associated with Hiccups Using the FAERS Database" Pharmaceuticals 15, no. 1: 27. https://doi.org/10.3390/ph15010027
APA StyleHosoya, R., Ishii-Nozawa, R., Kurosaki, K., & Uesawa, Y. (2022). Analysis of Factors Associated with Hiccups Using the FAERS Database. Pharmaceuticals, 15(1), 27. https://doi.org/10.3390/ph15010027