
Potential for Gut Peptide-Based Therapy in Postprandial Hypotension
by
 , and
, and
Malcolm J. Borg
1, 
Cong Xie
1 ,
,
Christopher K. Rayner
1,
Michael Horowitz
1,2,
Karen L. Jones
1,2 and
Tongzhi Wu
1,2,*
1
Adelaide Medical School and Centre of Research Excellence in Translating Nutritional Science to Good Health, The University of Adelaide, Adelaide 5000, Australia
2
Endocrine and Metabolic Unit, Royal Adelaide Hospital, Adelaide 5000, Australia
*
Author to whom correspondence should be addressed.
Nutrients 2021, 13(8), 2826; https://doi.org/10.3390/nu13082826
Submission received: 17 July 2021
/
Revised: 6 August 2021
/
Accepted: 14 August 2021
/
Published: 17 August 2021
(This article belongs to the Special Issue Nutrients and Cardiometabolic Health in Type 2 Diabetes)
Abstract
:Postprandial hypotension (PPH) is an important and under-recognised disorder resulting from inadequate compensatory cardiovascular responses to meal-induced splanchnic blood pooling. Current approaches to management are suboptimal. Recent studies have established that the cardiovascular response to a meal is modulated profoundly by gastrointestinal factors, including the type and caloric content of ingested meals, rate of gastric emptying, and small intestinal transit and absorption of nutrients. The small intestine represents the major site of nutrient-gut interactions and associated neurohormonal responses, including secretion of glucagon-like peptide-1, glucose-dependent insulinotropic peptide and somatostatin, which exert pleotropic actions relevant to the postprandial haemodynamic profile. This review summarises knowledge relating to the role of these gut peptides in the cardiovascular response to a meal and their potential application to the management of PPH.
1. Introduction
Postprandial hypotension (PPH) is defined as a fall in systolic blood pressure (SBP) of ≥20 mmHg, or a decrease to ≤90 mmHg if normotensive at baseline, within 2 h of a meal [1]. It is under-recognised, despite occurring frequently in the elderly (prevalence ~20–30%) and individuals with type 2 diabetes mellitus (T2D) (~40%) and chronic neurological disorders, such as Parkinson’s disease (40–100%) [1]. PPH is associated with substantially increased morbidity and mortality, and predisposes to syncope, falls, angina, transient ischaemic attacks and stroke [2]. The pathophysiology underlying PPH remains incompletely understood, but emerging evidence has revealed the fundamental role of gastrointestinal function in the regulation of cardiovascular responses to a meal [1], particularly the secretion and action of gut-derived peptides including glucagon-like peptide-1 (GLP-1) [3], glucose-dependent insulinotropic polypeptide (GIP) [4,5] and somatostatin [6]. Indeed, therapeutic strategies that modulate gastrointestinal hormone secretion or signalling have been shown to influence postprandial blood pressure substantially, although few, if any, studies have assessed whether the available therapies have a sustained effect on postprandial blood pressure or can prevent complications of PPH [1]. This review discusses the relevance of gastrointestinal function to the regulation of postprandial blood pressure, with an emphasis on the role of gut peptides in the pathophysiology and management of PPH.
2. Gastrointestinal Regulation of Postprandial Blood Pressure
The onset of PPH reflects inadequate cardiovascular compensation to meal-induced splanchnic blood pooling, which results from complex interactions between ingested nutrients and the gastrointestinal tract. There is now compelling evidence that gastrointestinal factors, including meal composition, the rate of nutrient delivery to the small intestine (i.e., gastric emptying), nutrient absorption, the specific region of the small intestine exposed to nutrients, and the consequent neurohormonal responses, are integral to the postprandial blood pressure response (Figure 1) [1].
Carbohydrate, fat and protein have all been shown to induce variable haemodynamic responses. For example, in hypertensive older individuals, oral carbohydrate, but not fat or protein, reduced mean blood pressure [10]. In “healthy” older individuals, intraduodenal administration of glucose (3 kcal/min) led to a more rapid decline in SBP when compared with intraduodenal isocaloric fat and protein [11], and the increase in superior mesenteric artery blood flow, a surrogate measure of splanchnic blood pooling, in response to intraduodenal protein was less when compared with glucose and fat [11]. In individuals with T2D, intraduodenal infusion of glucose (2 kcal/min), but not lipid, reduced diastolic blood pressure (DBP) [12]. The variable haemodynamic responses to macronutrients may reflect differences in neurohormonal profiles; for example, fat, relative to isocaloric glucose, is a more potent stimulus for secretion of the two incretin hormones, GLP-1 and GIP [12,13].
The rate of nutrient delivery into the small intestine is tightly controlled by gastric emptying, which exhibits substantial inter-individual, but much less intra-individual, variation [14]. Along with the observation that gastric emptying predicts postprandial glucose excursions [14], changes in postprandial blood pressure have also been found to be related to the rate of gastric emptying. There is now compelling evidence that gastric emptying represents a major determinant of the blood pressure response to a meal, such that the postprandial fall in SBP is greater when gastric emptying is relatively more rapid [15,16], reflecting enhanced small intestinal nutrient interaction and splanchnic blood pooling [17]. However, the relationship between gastric emptying and postprandial blood pressure does not appear to be linear; in healthy older individuals, the fall in blood pressure increased with escalating rates of intraduodenal glucose infusion between 1–2 kcal/min but did not differ between 2 and 3 kcal/min [17]. This apparent “threshold” may reflect concurrent changes in the secretion of gut-derived peptides involved in the regulation of postprandial cardiovascular function. Interventions that slow gastric emptying, either dietary (e.g., co-ingestion of dietary fibre, guar gum) or pharmacological (e.g., acarbose and GLP-1 receptor agonists), have been shown to attenuate the fall in SBP in response to a carbohydrate meal in “healthy” older individuals and those with T2D [18,19,20].
The interaction of nutrients with the small intestine results in splanchnic vasodilatation to facilitate the absorption of nutrients via the portal circulation. In parallel with this phenomenon, interventions that slow the rate of small intestinal carbohydrate absorption, such as ingestion of an alpha-glucosidase inhibitor, acarbose [21], or small intestinal infusion of a viscous polysaccharide, guar gum [22], are associated with reduced splanchnic blood pooling and attenuation of the fall in SBP in “healthy” older individuals. Variations in nutrient absorption along the small intestine affect the region of the intestine exposed to nutrients, and this may also influence postprandial haemodynamics. In a recent study, a standardised glucose infusion (2 kcal/min over 60 min) was delivered into the duodenum (13 cm post-pylorus) or ileum (190 cm post-pylorus) in individuals with T2D, and changes in blood pressure, heart rate and superior mesenteric artery flow were evaluated. Duodenal glucose exposure was shown to result in a much greater decline in SBP and rise in superior mesenteric artery flow than ileal [23], in association with more rapid glucose absorption, greater GIP release, and less GLP-1 secretion [24]. The latter observation supports the influence of gut-derived peptides in the regulation of postprandial cardiovascular function (as discussed in Section 3.1, Section 4.1 and Section 5.1).
The fall in systemic blood volume secondary to splanchnic vasodilatation is normally compensated for by a combination of enhanced cardiac output via increases in heart rate and/or stroke volume, and increased systemic vascular resistance [25]. Multiple neurohormonal mechanisms have been implicated in the cardiovascular response to a meal. Gastric distension, such as with meal ingestion, triggers a “gastrovascular reflex,” involving the stimulation of noradrenaline secretion, which enhances sympathetic nervous activity. This response is often blunted in the elderly, particularly those with PPH [2]. A number of vasoactive gut peptides have recently been implicated in the regulation of postprandial cardiovascular function, most notably GLP-1, GIP and somatostatin. Early interventional studies suggest that modulation of the secretion or signalling of these gut peptides may have a profound impact on the blood pressure response to meals, providing potential novel targets for the management of PPH (as discussed in Section 3.1, Section 4.1 and Section 5.1) [24,26]. Other gut peptides, including amylin, calcitonin-gene-related peptide, neurotensin, vasoactive-intestinal peptide, bradykinin and substance P are conceivable targets for modulating postprandial cardiovascular function, either via slowing of gastric emptying [27] or vasoactive actions [1]. However, there is a lack of evidence to support their role in postprandial cardiovascular function [1,28].
3. Glucagon-Like Peptide-1 (GLP-1)
GLP-1 is secreted by enteroendocrine L-cells which are located most densely in the ileum and colon. The secretion of GLP-1 is minimal during fasting, but is increased markedly following intestinal nutrient stimulation, particularly when the distal gut is exposed [29]. The majority of GLP-1 is inactivated prior to reaching the peripheral circulation by dipeptidyl peptidase-4 (DPP-4), an enzyme located on the surface of endothelial cells in close proximity to enteroendocrine cells [30], as well as in the liver and within the circulation [31]. Despite its rapid degradation, GLP-1 mediates considerable postprandial insulin secretion via the “incretin effect”, i.e., enhanced insulin secretion following oral or enteral glucose loads, when compared with an “isoglycaemic” intravenous glucose infusion [24]. In addition, GLP-1 slows gastric emptying and suppresses glucagon secretion [24]. Accordingly, both the DPP-4 resistant GLP-1 receptor agonists (GLP-1RAs) and DPP-4 inhibitors have been developed for glycaemic control in T2D. It is noteworthy that augmented GLP-1 secretion may also underlie the anti-diabetic effect of older anti-diabetic agents, such as metformin [32,33] and alpha-glucosidase inhibitors [34,35,36], since they delay intestinal glucose absorption and, hence, increase stimulation of the enteroendocrine L-cells in more distal gut regions (Table 1). Since its discovery in 1987 [37,38], numerous extra-glycaemic actions of GLP-1 have been appreciated, including effects on the cardiovascular system. The clinical implications of the latter remain to be explored comprehensively.
3.1. Effects of GLP-1 on Postprandial Haemodynamics
In rodents, intravenous administration of GLP-1 was shown to increase sympathetic activation, evidenced by a thermogenic effect attenuated by adrenalectomy or pre-treatment with pharmacological antagonists of sympathetic nervous activity [40]. In humans, GLP-1RAs do not affect preprandial blood pressure acutely [41], but have been shown to reduce SBP modestly in the long-term, an effect attributed to enhanced natriuresis and weight loss [42]. Few studies however, have attempted to discriminate between the cardiovascular profiles of GLP-1 in the fasting and postprandial states [43]. Intravenous GLP-1 administration at a pharmacological dose (0.9 pmol/kg/min) attenuates the fall in SBP and DBP (~5 mmHg at 60 min) in response to a carbohydrate meal in T2D (Figure 2) and does so variably in “healthy” older individuals [3,7]. This occurs in association with slowing of gastric emptying, a reduction in superior mesenteric artery blood flow, and a variable increase in heart rate [3,7]. GLP-1 may have direct effects on cardiac pacemaker cells given that cardiac GLP-1 receptors appear to be localised to the atria, where the sinoatrial and atrioventricular nodes reside [24]. Accordingly, the release of GLP-1 from the distal gut may logically serve as a “negative feedback” mechanism to prevent an exacerbated hypotensive response to increased delivery of nutrients into the small intestine.
Paradoxically, in one study, higher plasma GLP-1 levels were associated with PPH in patients with multiple system atrophy, but it remains uncertain as to whether increased GLP-1 levels were a cause of PPH or secondary to multiple system atrophy. Notably, the individuals with PPH in this study had sympathetic failure which may have attenuated the effect of GLP-1-signalling on blood pressure [44].
3.2. Interventional Strategies Utilising GLP-1 for Postprandial Blood Pressure Control
The potential for GLP-1 to modulate postprandial cardiovascular function has rendered it an attractive target for maintaining postprandial blood pressure. Several antidiabetic agents, including GLP-1RAs, DPP-4 inhibitors, metformin and alpha-glucosidase inhibitors, have been investigated for their effects on postprandial blood pressure and GLP-1.
The short-acting GLP-1RAs, such as exenatide BD and lixisenatide, have demonstrated similar effects to administration of exogenous GLP-1 on the postprandial haemodynamic profile. In individuals with and without T2D, administration of lixisenatide (10ug, by subcutaneous injection) markedly slowed gastric emptying and attenuated the increase in superior mesenteric artery flow and fall in SBP and DBP postprandially (Figure 3) [20]. Acute administration of exenatide BD increased heart rate and attenuated the fall in SBP and DBP in response to intraduodenal glucose infusion (2 kcal/min) in patients with T2D [45]. In contrast, the effects of long-acting GLP-1RAs, such as exenatide QW and semaglutide, on postprandial haemodynamics are less well-studied. Even though sustained stimulation of the GLP-1 receptor is known to be associated with tachyphylaxis for the slowing of gastric emptying by GLP-1 [46], there is recent evidence that exenatide QW [47] and semaglutide [48] may retain some capacity to slow gastric emptying in health and T2D with prolonged use. Hence, even long-acting GLP-1RAs may have the potential to attenuate the postprandial fall in blood pressure.
The cardiovascular effects of DPP-4 inhibitors (“gliptins”) are of increasing interest [49]. There is limited information about the effects of DPP-4 inhibition on postprandial blood pressure. Reported benefits of DPP-4 inhibitors on PPH relate primarily to case studies, as well as a small cohort of overweight T2D patients receiving metformin therapy [50,51,52]. For example, in a comparative study in overweight patients with T2D, 8 weeks treatment with the DPP-4 inhibitor, linagliptin, while achieving comparable glucose-lowering to glimepiride (a sulphonylurea anti-diabetic drug which does not affect haemodynamics), was reported to attenuate the fall in blood pressure after a meal (0.7 ± 2.3 mmHg) without impacting preprandial blood pressure [50]. In contrast, when another DPP-4 inhibitor, vildagliptin, was administered acutely with an intraduodenal glucose infusion in T2D, postprandial SBP and DBP were lower when compared with placebo [53]. In T2D, sitagliptin administration did not significantly impact blood pressure after a potato meal [54]. The discrepancy in the studies of vildagliptin and sitagliptin, compared with linagliptin, may relate to differences in study design, including the study duration and method of carbohydrate administration. Perhaps the most important difference in the studies was the concomitant use in the former of metformin, a drug known to moderate cardiovascular outcomes with DPP-4 inhibitors and potentially act to augment DPP-4 inhibition to enhance plasma active GLP-1 levels [55,56].
The impact of metformin on postprandial blood pressure has only been evaluated in a small cohort of T2D patients. In this study, intraduodenal infusion of metformin 1g attenuated the fall in blood pressure after 50 g oral glucose substantially (by almost 10 mmHg 60 min after a meal) (Figure 4), an effect associated with an increase in plasma GLP-1 and slowing of gastric emptying [57]. Metformin has also been shown to slow intestinal glucose absorption and increase noradrenaline secretion [58], which may contribute to the attenuation of the fall in blood pressure after enteral glucose.
Observations on the postprandial haemodynamic effects of alpha-glucosidase inhibition have focused primarily on acarbose, with minimal study of the other drugs of this class [59]. Acarbose administration in “healthy” individuals leads to enhanced plasma GLP-1, although this is inconsistent in individuals with T2D [19,36,60]. Several small cohorts [61,62,63] and case studies [64,65,66,67] support the potential for acarbose to modulate postprandial haemodynamics. In one such case study, a 58-year-old individual with T2D, complicated by microvascular disease and severe symptomatic postprandial hypotension, received acarbose (300 mg/day), octreotide and midodrine on separate days, undergoing 24 h ambulatory blood pressure monitoring. Postprandial blood pressure, along with orthostatic dizziness and postprandial vertigo, were attenuated after acarbose, but not octreotide or midodrine [64]. The acute effect of a single oral dose of acarbose (50–100 mg) on blood pressure and heart rate after a standardised meal has been studied in cohorts of “healthy” elderly (Figure 5) [19,63], T2D with PPH [62], and subjects with pure autonomic failure [61]. In each case, the fall in postprandial blood pressure was attenuated significantly (by 15–20 mmHg SBP). Postprandial heart rate was affected by acarbose in a single study (Figure 5). The effect of sustained, relative to acute, acarbose administration on postprandial blood pressure is less well-studied, although case studies suggest it is maintained [67,68]. Slowing of gastric emptying, which may result from enhanced GLP-1 concentrations, and attenuation of postprandial splanchnic vasodilation with acarbose, are likely to contribute to its effects on postprandial haemodynamics [21,69]. Practically, the widespread use of acarbose is not limited by safety or cost, but by gastrointestinal adverse effects, including flatulence and diarrhoea, which are common but tend to subside with continued treatment, and can be minimised through stepwise dose increments and dietary modifications (consuming complex carbohydrate over simple sugars) [70,71].
These therapies, originally introduced as glucose-lowering agents, offer exciting therapeutic potential for the management of PPH, but further studies in larger cohorts of patients with and without T2D are warranted.
4. Glucose-Dependent Insulinotropic Polypeptide
GIP is the first of the two “incretin hormones” identified in the 1970s [72]. It is released from the enteroendocrine K-cells which predominate in the proximal small intestine. Like GLP-1, GIP has a short half-life in the systemic circulation due to prompt inactivation by DPP-4. Plasma GIP concentrations are low in the fasting state and increase promptly in response to nutrient stimulation [24]. As an incretin hormone, GIP has a well-established effect to stimulate postprandial insulin secretion in a glucose-dependent manner [73]. Unlike GLP-1, GIP has little effect on gastric emptying, and can augment glucagon secretion in the face of falling glycaemia. It is increasingly recognised that GIP exhibits numerous extraglycaemic functions mediated by GIP receptors identified in diverse tissues [24].
4.1. Effects of GIP on Postprandial Haemodynamics
GIP has been reported to induce splanchnic blood pooling and increase heart rate, with variable effects on blood pressure [4,5]. Pre-clinical studies have delineated the variable profile of GIP in the splanchnic, compared with systemic, circulation. Intravenous administration of GIP at supraphysiological doses consistently increased splanchnic blood flow in multiple animal studies [74,75,76]. In contrast, intravenous GIP in dogs reduced hepatic artery blood flow [76]. In humans, the postprandial rise in plasma GIP in individuals with T2D receiving sitagliptin concurrently with enteral glucose infusion was proportional to the increase in heart rate [5]. In patients with type 1 diabetes who underwent hyperglycaemic and hypoglycaemic clamps, intravenous GIP infusion was associated with an elevation in heart rate (10.1 2.6 and 16 4.7 bpm respectively), with a concurrent reduction in DBP (5.4 4.5 and 9.7 6.6 mmHg respectively), although SBP was observed to be increased during the former (5.6 3.1 mmHg), and unaffected in the latter, setting [8]. During a hyperglycaemic clamp in T2D patients, GIP infusion led to a reduction in mean arterial blood pressure (10–15 mmHg) and increase in heart rate (~8 bpm) [4]. Splanchnic blood flow was not assessed in these studies but, conceivably, the increase in heart rate represented a compensation for GIP-induced splanchnic blood pooling. Alternatively, given the presence of GIP receptors in the heart [24], GIP could have a positive chronotropic action either directly, or mediated via anti-cholinergic activity [8]. Overall, GIP has been associated with a decline in postprandial blood pressure in most settings, an effect likely mediated via splanchnic blood pooling, at times compensated for by an increase in heart rate.
4.2. Interventional Strategies Utilising GIP for Postprandial Blood Pressure Control
Given that GIP enhances splanchnic blood pooling, the impact of GIP agonists and antagonists on PPH would be of interest. A dual GLP-1/GIP agonist, tirzepatide, has been developed for the treatment of T2D [77,78], while GIP antagonism, utilising a selective competitive inhibitor (GIP fragment GIP(3–30)NH2), has been examined in a pre-clinical setting for potential benefits in T2D [79]. Conceivably, GIP agonism could aggravate, and antagonism could benefit, postprandial blood pressure control. Further studies evaluating the effects of such drugs on the cardiovascular system pre- and postprandially are warranted.
5. Somatostatin
Originally named “growth-hormone release-inhibiting hormone” upon its discovery in 1973 [80], the hormone now known as somatostatin comprises two main forms—somatostatin-14 and somatostatin-28. The former is dominant in the CNS, arising from the arcuate and anterior periventricular nuclei of the hypothalamus, as well as pancreatic islet delta-cells. The latter is dominant in the gastrointestinal tract, which is the predominant source of somatostatin in humans, being secreted by D-cells throughout the length of the gastrointestinal mucosa [81,82]. The half-life of somatostatin is only 1–3 min and, as a result, it has been considered to act locally to inhibit secretion of various hormones (e.g., insulin, glucagon, secretin, growth hormone) and gastrointestinal fluids (e.g., gastric acid, bile, colonic fluid) [83]. Synthetic analogues of somatostatin with longer half-lives are utilised in clinical practice, including first-generation (octreotide and lanreotide) and second-generation (pasireotide) agents, for a variety of indications (e.g., acromegaly, neuroendocrine tumours, bleeding oesophageal varices) given the effects of somatostatin to inhibit secretion of other hormones and influence splanchnic blood flow (as discussed in Section 5.1) [82]. The relatively high cost and rates of gastrointestinal adverse effects with somatostatin analogues limit their use, although the latter tend to subside with continued use [84].
5.1. Interventional Strategies Utilising Somatostatin for Postprandial Blood Pressure Control
Increasing evidence over the past two decades supports a therapeutic role for somatostatin in postprandial hypotension. Octreotide attenuates the postprandial fall in blood pressure in normotensive and hypertensive elderly (by 7–15 mmHg SBP) [9], and autonomic failure with and without diabetes (by 15 2 mmHg SBP) [85,86]. This effect has been attributed primarily to splanchnic vasoconstriction. However, the mechanism(s) by which somatostatin, or its analogues, induce splanchnic vasoconstriction remain poorly understood. This effect is unlikely to be mediated via the autonomic nervous system given that it occurs independently of changes in plasma catecholamine concentrations, and is maintained in autonomic failure [87]. Splanchnic vasoconstriction was shown to occur concurrently with increasing forearm vascular resistance when octreotide was administered to patients with autonomic failure, such that a direct vasopressor effect of the drug appears likely [6,26], although this finding was not replicated in another study [86]. Alternatively, the underlying mechanism for splanchnic vasoconstriction could be neurohumoral. Somatostatin and its analogues inhibit the secretion of a number of gut peptides, including glucagon [88] and GIP [89], both of which are known to induce splanchnic blood pooling. However, markedly greater glucagon concentrations than those occurring following octreotide are required to induce this effect [88].
While octreotide is one of the most well-studied agents for PPH, few studies have examined the effect of sustained exposure. Ludwig et al. reported a reduction in splanchnic vasoconstriction after 48 h of octreotide use in “healthy subjects,” raising concern of tachyphylaxis [88]. However, attenuation of the fall in postprandial blood pressure was sustained with use of octreotide over a 6 month period in patients with multiple system atrophy [88,90].
6. Conclusions
PPH is an important and under-recognised clinical phenomenon associated with increased morbidity and mortality, and intrinsically linked to gastrointestinal function. Gut peptides, most notably GLP-1, GIP and somatostatin, are of particular interest as potential pharmacotherapy targets for PPH. GLP-1 receptors are the target of several existing drugs prescribed for glucose-lowering in T2D which, based on studies of small-cohorts, offer potential as therapies for PPH, extending their application beyond the management of T2D. Clinical trials involving sustained administration of these medications in large cohorts, with or without T2D, to document their effects on postprandial blood pressure, and the complications of PPH, are warranted. GIP may both contribute to the fall in postprandial blood pressure, and the haemodynamic effects of GIP receptor agonists and antagonists postprandially should also be examined. Somatostatin attenuates the fall in postprandial blood pressure, and its analogue, octreotide, has already been studied as a pharmacological therapy for PPH. Discrimination of the cardiovascular effects of gut peptides and their signalling pathways before and after meals may refine the therapeutic approach to PPH.
Author Contributions
Conceptualization, M.J.B. and T.W.; writing—original draft preparation, M.J.B.; writing—review and editing, T.W., C.K.R., M.H., K.L.J.; visualization, C.X. All authors have read and agreed to the published version of the manuscript.
Funding
The authors’ work in this area is supported by the Australia National Health and Medical Research Council (NHMRC: 1147333), Diabetes Australia (Y17G-WUTO; Y19G-WUTO; Y20G-WUTO, Y21G-WUTO) and Royal Adelaide Hospital Research Committee. C.X. is supported by a postgraduate scholarship from the China Scholarship Council. K.L.J. is supported by a University of Adelaide William T Southcott Research Fellowship. T.W. is supported by a Mid-Career Fellowship from The Hospital Research Foundation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in PubMed.
Acknowledgments
The Centre of Research Excellence (CRE) in Translating Nutritional Science to Good Health has been supported by The Hospital Research Foundation.
Conflicts of Interest
K.L.J. has received research funding from Sanofi and AstraZeneca; M.H. has participated in the advisory boards and/or symposia for Novo Nordisk, Sanofi, Novartis, Eli Lilly, Merck Sharp & Dohme, Boehringer Ingelheim and AstraZeneca and has received honoraria for this activity; C.K.R. has received research funding from Merck, Sharp & Dohme, AstraZeneca, Novartis and Sanofi; T.W. has received research funding from AstraZeneca and Novartis. M.J.B. and C.X. have no personal or financial conflict of interest to declare.
References
- Trahair, L.G.; Horowitz, M.; Jones, K.L. Postprandial hypotension: A systematic review. J. Am. Med. Dir. Assoc. 2014, 15, 394–409. [Google Scholar] [CrossRef]
- Aronow Wilbert, S.; Ahn, C. Association of postprandial hypotension with incidence of falls, syncope, coronary events, stroke, and total mortality at 29-month follow-up in 499 older nursing home residents. J. Am. Geriatr. Soc. 1997, 45, 1051–1053. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Horowitz, M.; Hausken, T.; Feinle-Bisset, C.; Rayner, C.K.; Jones, K.L. Effects of exogenous glucagon-like peptide-1 on the blood pressure, heart rate, mesenteric blood flow, and glycemic responses to intraduodenal glucose in healthy older subjects. J. Clin. Endocrinol. Metab. 2014, 99, 2628–2634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wice, B.M.; Reeds, D.N.; Tran, H.D.; Crimmins, D.L.; Patterson, B.W.; Dunai, J.; Wallendorf, M.J.; Ladenson, J.H.; Villareal, D.T.; Polonsky, K.S. Xenin-25 amplifies GIP-mediated insulin secretion in humans with normal and impaired glucose tolerance but not type 2 diabetes. Diabetes 2012, 61, 1793–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Trahair, L.G.; Bound, M.J.; Deacon, C.F.; Horowitz, M.; Rayner, C.K.; Jones, K.L. Effects of sitagliptin on blood pressure and heart rate in response to intraduodenal glucose infusion in patients with Type 2 diabetes: A potential role for glucose-dependent insulinotropic polypeptide? Diabet. Med. 2015, 32, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Hoeldtke, R.D.; Dworkin, G.E.; Gaspar, S.R.; Israel, B.C.; Boden, G. Effect of the somatostatin analogue SMS-201-995 on the adrenergic response to glucose ingestion in patients with postprandial hypotension. Am. J. Med. 1989, 86, 673–677. [Google Scholar] [CrossRef]
- Trahair, L.G.; Horowitz, M.; Stevens, J.E.; Feinle-Bisset, C.; Standfield, S.; Piscitelli, D.; Rayner, C.K.; Deane, A.M.; Jones, K.L. Effects of exogenous glucagon-like peptide-1 on blood pressure, heart rate, gastric emptying, mesenteric blood flow and glycaemic responses to oral glucose in older individuals with normal glucose tolerance or type 2 diabetes. Diabetologia 2015, 58, 1769–1778. [Google Scholar] [CrossRef] [Green Version]
- Heimbürger, S.M.; Bergmann, N.C.; Augustin, R.; Gasbjerg, L.S.; Christensen, M.B.; Knop, F.K. Glucose-dependent insulinotropic polypeptide (GIP) and cardiovascular disease. Peptides 2020, 125, 170174. [Google Scholar] [CrossRef]
- Jansen, R.W.; Peeters, T.L.; Lenders, J.W.; van Lier, H.J.; v’t Laar, A.; Hoefnagels, W.H. Somatostatin analog octreotide (SMS 201-995) prevents the decrease in blood pressure after oral glucose loading in the elderly. J. Clin. Endocrinol. Metab. 1989, 68, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.W.; Peeters, T.L.; Van Lier, H.J.; Hoefnagels, W.H. The effect of oral glucose, protein, fat and water loading on blood pressure and the gastrointestinal peptides VIP and somatostatin in hypertensive elderly subjects. Eur. J. Clin. Investig. 1990, 20, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore, D.; Hausken, T.; Meyer, J.H.; Chapman, I.M.; Horowitz, M.; Jones, K.L. Effects of intraduodenal glucose, fat, and protein on blood pressure, heart rate, and splanchnic blood flow in healthy older subjects. Am. J. Clin. Nutr. 2008, 87, 156–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, C.; Wang, X.; Jones, K.L.; Horowitz, M.; Sun, Z.; Little, T.J.; Rayner, C.K.; Wu, T. Comparative Effects of Intraduodenal Glucose and Fat Infusion on Blood Pressure and Heart Rate in Type 2 Diabetes. Front. Nutr. 2020, 7, 582314. [Google Scholar] [CrossRef]
- Wu, T.; Rayner, C.K.; Watson, L.E.; Jones, K.L.; Horowitz, M.; Little, T.J. Comparative effects of intraduodenal fat and glucose on the gut-incretin axis in healthy males. Peptides 2017, 95, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Rayner, C.K.; Horowitz, M. Inter-regulation of gastric emptying and incretin hormone secretion: Implications for postprandial glycemic control. Biomark. Med. 2016, 10, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Horowitz, M.; Jones, K.L. Postprandial Hypotension Is Associated With More Rapid Gastric Emptying in Healthy Older Individuals. J. Am. Med. Dir. Assoc. 2015, 16, 521–523. [Google Scholar] [CrossRef]
- Jones, K.L.; Tonkin, A.; Horowitz, M.; Wishart, J.M.; Carney, B.I.; Guha, S.; Green, L. Rate of gastric emptying is a determinant of postprandial hypotension in non-insulin-dependent diabetes mellitus. Clin. Sci. 1998, 94, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Vanis, L.; Gentilcore, D.; Rayner, C.K.; Wishart, J.M.; Horowitz, M.; Feinle-Bisset, C.; Jones, K.L. Effects of small intestinal glucose load on blood pressure, splanchnic blood flow, glycemia, and GLP-1 release in healthy older subjects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 300, 1524–1531. [Google Scholar] [CrossRef]
- Russo, A.; Stevens, J.E.; Wilson, T.; Wells, F.; Tonkin, A.; Horowitz, M.; Jones, K.L. Guar attenuates fall in postprandial blood pressure and slows gastric emptying of oral glucose in type 2 diabetes. Dig. Dis. Sci. 2003, 48, 1221–1229. [Google Scholar] [CrossRef]
- Gentilcore, D.; Bryant, B.; Wishart, J.M.; Morris, H.A.; Horowitz, M.; Jones, K.L. Acarbose attenuates the hypotensive response to sucrose and slows gastric emptying in the elderly. Am. J. Med. 2005, 118, 1289. [Google Scholar] [CrossRef]
- Jones, K.L.; Rigda, R.S.; Buttfield, M.D.M.; Hatzinikolas, S.; Pham, H.T.; Marathe, C.S.; Wu, T.; Lange, K.; Trahair, L.G.; Rayner, C.K.; et al. Effects of lixisenatide on postprandial blood pressure, gastric emptying and glycaemia in healthy people and people with type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore, D.; Horowitz, M.; Jones, K.L. Acarbose and postprandial hypotension. Hypertension 2007, 50, 159–160. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, D.; Feinle-Bisset, C.; Chong, C.; Cameron, A.; Tonkin, A.; Wishart, J.; Horowitz, M.; Jones, K.L. Intraduodenal guar attenuates the fall in blood pressure induced by glucose in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 940–946. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Jones, K.L.; Horowitz, M.; Rayner, C.K.; Wu, T. Effects of Proximal and Distal Enteral Glucose Infusion on Cardiovascular Response in Health and Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2020, 105, 2877–2884. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Rayner, C.K.; Horowitz, M. Incretins. Handb. Exp. Pharm. 2016, 233, 137–171. [Google Scholar] [CrossRef]
- Jansen, R.W.; Lipsitz, L.A. Postprandial hypotension: Epidemiology, pathophysiology, and clinical management. Ann. Intern. Med. 1995, 122, 286–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeldtke, R.D.; Davis, K.M.; Joseph, J.; Gonzales, R.; Panidis, I.P.; Friedman, A.C. Hemodynamic effects of octreotide in patients with autonomic neuropathy. Circulation 1991, 84, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolffenbuttel, B.H.; Graal, M.B. New treatments for patients with type 2 diabetes mellitus. Postgrad. Med. J. 1996, 72, 657–662. [Google Scholar] [CrossRef]
- Hoogwerf, B.J.; Doshi, K.B.; Diab, D. Pramlintide, the synthetic analogue of amylin: Physiology, pathophysiology, and effects on glycemic control, body weight, and selected biomarkers of vascular risk. Vasc Health Risk Manag. 2008, 4, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Rayner, C.K.; Jones, K.; Horowitz, M. Dietary effects on incretin hormone secretion. Vitam. Horm. 2010, 84, 81–110. [Google Scholar] [CrossRef]
- Hansen, L.; Deacon, C.F.; Orskov, C.; Holst, J.J. Glucagon-like peptide-1-(7-36)amide is transformed to glucagon-like peptide-1-(9-36)amide by dipeptidyl peptidase IV in the capillaries supplying the L cells of the porcine intestine. Endocrinology 1999, 140, 5356–5363. [Google Scholar] [CrossRef]
- Holst, J.J. The physiology of glucagon-like peptide 1. Physiol. Rev. 2007, 87, 1409–1439. [Google Scholar] [CrossRef] [PubMed]
- Bahne, E.; Hansen, M.; Bronden, A.; Sonne, D.P.; Vilsboll, T.; Knop, F.K. Involvement of glucagon-like peptide-1 in the glucose-lowering effect of metformin. Diabetes Obes. Metab. 2016, 18, 955–961. [Google Scholar] [CrossRef]
- Wu, T.; Thazhath, S.S.; Bound, M.J.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Mechanism of increase in plasma intact GLP-1 by metformin in type 2 diabetes: Stimulation of GLP-1 secretion or reduction in plasma DPP-4 activity? Diabetes Res. Clin. Pr. 2014, 106, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Moritoh, Y.; Takeuchi, K.; Hazama, M. Chronic administration of voglibose, an alpha-glucosidase inhibitor, increases active glucagon-like peptide-1 levels by increasing its secretion and decreasing dipeptidyl peptidase-4 activity in ob/ob mice. J. Pharm. Exp. Ther. 2009, 329, 669–676. [Google Scholar] [CrossRef]
- Lee, A.; Patrick, P.; Wishart, J.; Horowitz, M.; Morley, J.E. The effects of miglitol on glucagon-like peptide-1 secretion and appetite sensations in obese type 2 diabetics. Diabetes Obes. Metab. 2002, 4, 329–335. [Google Scholar] [CrossRef]
- Dalsgaard, N.B.; Gasbjerg, L.S.; Hansen, L.S.; Hansen, N.L.; Stensen, S.; Hartmann, B.; Rehfeld, J.F.; Holst, J.J.; Vilsbøll, T.; Knop, F.K. The role of GLP-1 in the postprandial effects of acarbose in type 2 diabetes. Eur. J. Endocrinol. 2021, 184, 387–398. [Google Scholar] [CrossRef]
- Drucker, D.J.; Philippe, J.; Mojsov, S.; Chick, W.L.; Habener, J.F. Glucagon-like peptide I stimulates insulin gene expression and increases cyclic AMP levels in a rat islet cell line. Proc. Natl. Acad. Sci. USA 1987, 84, 3434–3438. [Google Scholar] [CrossRef] [Green Version]
- Kreymann, B.; Williams, G.; Ghatei, M.A.; Bloom, S.R. Glucagon-like peptide-1 7-36: A physiological incretin in man. Lancet 1987, 2, 1300–1304. [Google Scholar] [CrossRef]
- Bahne, E.; Sun, E.W.L.; Young, R.L.; Hansen, M.; Sonne, D.P.; Hansen, J.S.; Rohde, U.; Liou, A.P.; Jackson, M.L.; de Fontgalland, D.; et al. Metformin-induced glucagon-like peptide-1 secretion contributes to the actions of metformin in type 2 diabetes. JCI Insight 2018, 3, e93936. [Google Scholar] [CrossRef] [Green Version]
- Osaka, T.; Endo, M.; Yamakawa, M.; Inoue, S. Energy expenditure by intravenous administration of glucagon-like peptide-1 mediated by the lower brainstem and sympathoadrenal system. Peptides 2005, 26, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.E.; Charkoudian, N.; Andrews, C.N.; Camilleri, M.; Sletten, D.; Zinsmeister, A.R.; Low, P.A. Effects of glucagon-like peptide-1, yohimbine, and nitrergic modulation on sympathetic and parasympathetic activity in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, 874–880. [Google Scholar] [CrossRef] [Green Version]
- Seufert, J.; Gallwitz, B. The extra-pancreatic effects of GLP-1 receptor agonists: A focus on the cardiovascular, gastrointestinal and central nervous systems. Diabetes Obes. Metab. 2014, 16, 673–688. [Google Scholar] [CrossRef] [Green Version]
- Maringwa, J.; Sardu, M.L.; Hang, Y.; Czerniak, R.; Vishnubhotla, M.; Vakilynejad, M.; Pfister, M. Characterizing Effects of Antidiabetic Drugs on Heart Rate, Systolic and Diastolic Blood Pressure. Clin. Pharm. Ther. 2020, 109, 1583–1592. [Google Scholar] [CrossRef]
- Fukushima, T.; Asahina, M.; Fujinuma, Y.; Yamanaka, Y.; Katagiri, A.; Mori, M.; Kuwabara, S. Role of intestinal peptides and the autonomic nervous system in postprandial hypotension in patients with multiple system atrophy. J. Neurol. 2013, 260, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Thazhath, S.S.; Marathe, C.S.; Wu, T.; Chang, J.; Khoo, J.; Kuo, P.; Checklin, H.L.; Bound, M.J.; Rigda, R.S.; Horowitz, M.; et al. Acute effects of the glucagon-like peptide-1 receptor agonist, exenatide, on blood pressure and heart rate responses to intraduodenal glucose infusion in type 2 diabetes. Diab. Vasc. Dis. Res. 2017, 14, 59–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nauck, M.A.; Kemmeries, G.; Holst, J.J.; Meier, J.J. Rapid tachyphylaxis of the glucagon-like peptide 1-induced deceleration of gastric emptying in humans. Diabetes 2011, 60, 1561–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.L.; Huynh, L.Q.; Hatzinikolas, S.; Rigda, R.S.; Phillips, L.K.; Pham, H.T.; Marathe, C.S.; Wu, T.; Malbert, C.H.; Stevens, J.E.; et al. Exenatide once weekly slows gastric emptying of solids and liquids in healthy, overweight people at steady-state concentrations. Diabetes Obes. Metab. 2020, 22, 788–797. [Google Scholar] [CrossRef]
- Hjerpsted, J.B.; Flint, A.; Brooks, A.; Axelsen, M.B.; Kvist, T.; Blundell, J. Semaglutide improves postprandial glucose and lipid metabolism, and delays first-hour gastric emptying in subjects with obesity. Diabetes Obes. Metab. 2018, 20, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avogaro, A.; Fadini, G.P. The pleiotropic cardiovascular effects of dipeptidyl peptidase-4 inhibitors. Br. J. Clin. Pharmacol. 2018, 84, 1686–1695. [Google Scholar] [CrossRef] [Green Version]
- Kraaijenhof, J.; Muskiet, M.H.A.; Tonneijck, L.; Ouwens, D.M.; Kramer, M.H.H.; van Raalte, D.H.; Smits, M.M. Effects of dipeptidyl peptidase-4 inhibitor linagliptin versus sulphonylurea glimepiride on systemic haemodynamics in overweight patients with type 2 diabetes: A secondary analysis of an 8-week, randomized, controlled, double-blind trial. Diabetes Obes. Metab. 2020, 22, 1847–1856. [Google Scholar] [CrossRef]
- Yonenaga, A.; Ota, H.; Honda, M.; Koshiyama, D.; Yagi, T.; Hanaoka, Y.; Yamamoto, H.; Yamaguchi, Y.; Iijima, K.; Akishita, M.; et al. Marked improvement of elderly postprandial hypotension by dipeptidyl peptidase IV inhibitor. Geriatr. Gerontol. Int. 2013, 13, 227–229. [Google Scholar] [CrossRef]
- Saito, Y.; Ishikawa, J.; Harada, K. Postprandial and Orthostatic Hypotension Treated by Sitagliptin in a Patient with Dementia with Lewy Bodies. Am. J. Case Rep. 2016, 17, 887–893. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Trahair, L.G.; Little, T.J.; Bound, M.J.; Zhang, X.; Wu, H.; Sun, Z.; Horowitz, M.; Rayner, C.K.; Jones, K.L. Effects of vildagliptin and metformin on blood pressure and heart rate responses to small intestinal glucose in type 2 diabetes. Diabetes Care 2017, 40, 702–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.E.; Buttfield, M.; Wu, T.; Hatzinikolas, S.; Pham, H.; Lange, K.; Rayner, C.K.; Horowitz, M.; Jones, K.L. Effects of sitagliptin on gastric emptying of, and the glycaemic and blood pressure responses to, a carbohydrate meal in type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Crowley, M.J.; Williams, J.W., Jr.; Kosinski, A.S.; D’Alessio, D.A.; Buse, J.B. Metformin Use May Moderate the Effect of DPP-4 Inhibitors on Cardiovascular Outcomes. Diabetes Care 2017, 40, 1787–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardarli, I.; Arndt, E.; Deacon, C.F.; Holst, J.J.; Nauck, M.A. Effects of sitagliptin and metformin treatment on incretin hormone and insulin secretory responses to oral and “isoglycemic” intravenous glucose. Diabetes 2014, 63, 663–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, M.J.; Jones, K.L.; Sun, Z.; Horowitz, M.; Rayner, C.K.; Wu, T. Metformin attenuates the postprandial fall in blood pressure in type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 1251–1254. [Google Scholar] [CrossRef]
- Borg, M.J.; Rayner, C.K.; Jones, K.L.; Horowitz, M.; Xie, C.; Wu, T. Gastrointestinal Mechanisms Underlying the Cardiovascular Effect of Metformin. Pharmaceuticals 2020, 13, 410. [Google Scholar] [CrossRef]
- Maruta, T.; Komai, K.; Takamori, M.; Yamada, M. Voglibose inhibits postprandial hypotension in neurologic disorders and elderly people. Neurology 2006, 66, 1432–1434. [Google Scholar] [CrossRef]
- Hücking, K.; Kostic, Z.; Pox, C.; Ritzel, R.; Holst, J.J.; Schmiegel, W.; Nauck, M.A. alpha-Glucosidase inhibition (acarbose) fails to enhance secretion of glucagon-like peptide 1 (7-36 amide) and to delay gastric emptying in Type 2 diabetic patients. Diabet. Med. 2005, 22, 470–476. [Google Scholar] [CrossRef]
- Shibao, C.; Gamboa, A.; Diedrich, A.; Dossett, C.; Choi, L.; Farley, G.; Biaggioni, I. Acarbose, an alpha-glucosidase inhibitor, attenuates postprandial hypotension in autonomic failure. Hypertension 2007, 50, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Madden, K.M.; Harris, D.E.; Meneilly, G.S. Attenuation of Postprandial Hypotension with Acarbose in Older Adults with Type 2 Diabetes Mellitus. J. Am. Geriatr. Soc. 2015, 63, 1484–1486. [Google Scholar] [CrossRef]
- Pham, H.; Trahair, L.; Phillips, L.; Rayner, C.; Horowitz, M.; Jones, K. A randomized, crossover study of the acute effects of acarbose and gastric distension, alone and combined, on postprandial blood pressure in healthy older adults. BMC Geriatr. 2019, 19, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, E.; Goda, K.; Nagata, K.; Kitaoka, H.; Ohsawa, N.; Hanafusa, T. Acarbose improved severe postprandial hypotension in a patient with diabetes mellitus. J. Diabetes Complicat. 2001, 15, 158–161. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, H.S.; Lee, T.Y.; Jang, E.; Kang, M.H.; Cho, D.K. A case of postprandial hypotension in the intensive care unit treated with acarbose. Korean Circ. J. 2011, 41, 629–631. [Google Scholar] [CrossRef] [Green Version]
- Farrehi, C.; Pazzi, C.; Stillman, M. A case of postprandial hypotension in an individual with cervical spinal cord injury: Treatment with acarbose. Spinal Cord Ser. Cases 2019, 5, 75. [Google Scholar] [CrossRef]
- Maule, S.; Tredici, M.; Dematteis, A.; Matteoda, C.; Chiandussi, L. Postprandial hypotension treated with acarbose in a patient with type 1 diabetes mellitus. Clin. Auton Res. 2004, 14, 405–407. [Google Scholar] [CrossRef]
- Yamamoto, N.; Sasaki, E.; Arishima, T.; Ito, M.; Tanaka, H.; Terasaki, J.; Imagawa, A.; Hanafusa, T. Combination therapy for postprandial and orthostatic hypotension in an elderly patient with type 2 diabetes mellitus. J. Am. Geriatr. Soc. 2006, 54, 727–728. [Google Scholar] [CrossRef]
- Gentilcore, D.; Vanis, L.; Wishart, J.M.; Rayner, C.K.; Horowitz, M.; Jones, K.L. The alpha (α)-glucosidase inhibitor, acarbose, attenuates the blood pressure and splanchnic blood flow responses to intraduodenal sucrose in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Hanefeld, M. Cardiovascular benefits and safety profile of acarbose therapy in prediabetes and established type 2 diabetes. Cardiovasc. Diabetol. 2007, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Pishdad, P.; Pishdad, R.; Pishdad, G.R.; Panahi, Y. A Time to revisit the two oldest prandial anti-diabetes agents: Acarbose and repaglinide. Endocrine 2020, 70, 307–313. [Google Scholar] [CrossRef]
- Brown, J.C.; Dryburgh, J.R.; Ross, S.A.; Dupré, J. Identification and actions of gastric inhibitory polypeptide. Recent Prog. Horm. Res. 1975, 31, 487–532. [Google Scholar] [CrossRef] [PubMed]
- Creutzfeldt, W. The incretin concept today. Diabetologia 1979, 16, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fara, J.W.; Salazar, A.M. Gastric inhibitory polypeptide increases mesenteric blood flow. Proc. Soc. Exp. Biol. Med. 1978, 158, 446–448. [Google Scholar] [CrossRef] [PubMed]
- Svensson, A.M.; Efendic, S.; Ostenson, C.G.; Jansson, L. Gastric inhibitory polypeptide and splanchnic blood perfusion: Augmentation of the islet blood flow increase in hyperglycemic rats. Peptides 1997, 18, 1055–1059. [Google Scholar] [CrossRef]
- Kogire, M.; Inoue, K.; Sumi, S.; Doi, R.; Takaori, K.; Yun, M.; Fujii, N.; Yajima, H.; Tobe, T. Effects of synthetic human gastric inhibitory polypeptide on splanchnic circulation in dogs. Gastroenterology 1988, 95, 1636–1640. [Google Scholar] [CrossRef]
- Frias, J.P.; Nauck, M.A.; Van, J.; Benson, C.; Bray, R.; Cui, X.; Milicevic, Z.; Urva, S.; Haupt, A.; Robins, D.A. Efficacy and tolerability of tirzepatide, a dual glucose-dependent insulinotropic peptide and glucagon-like peptide-1 receptor agonist in patients with type 2 diabetes: A 12-week, randomized, double-blind, placebo-controlled study to evaluate different dose-escalation regimens. Diabetes Obes. Metab. 2020, 22, 938–946. [Google Scholar] [CrossRef]
- Min, T.; Bain, S.C. The Role of Tirzepatide, Dual GIP and GLP-1 Receptor Agonist, in the Management of Type 2 Diabetes: The SURPASS Clinical Trials. Diabetes Ther. 2021, 12, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Gasbjerg, L.S.; Gabe, M.B.N.; Hartmann, B.; Christensen, M.B.; Knop, F.K.; Holst, J.J.; Rosenkilde, M.M. Glucose-dependent insulinotropic polypeptide (GIP) receptor antagonists as anti-diabetic agents. Peptides 2018, 100, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Brazeau, P.; Vale, W.; Burgus, R.; Ling, N.; Butcher, M.; Rivier, J.; Guillemin, R. Hypothalamic polypeptide that inhibits the secretion of immunoreactive pituitary growth hormone. Science 1973, 179, 77–79. [Google Scholar] [CrossRef]
- Rorsman, P.; Huising, M.O. The somatostatin-secreting pancreatic δ-cell in health and disease. Nat. Rev. Endocrinol. 2018, 14, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Porras, M.; Cárdenas-Salas, J.; Álvarez-Escolá, C. Somatostatin Analogs in Clinical Practice: A Review. Int. J. Mol. Sci. 2020, 21, 1682. [Google Scholar] [CrossRef] [Green Version]
- O’Toole, T.J.; Sharma, S. Physiology, Somatostatin. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Lamberts, S.W.; van der Lely, A.J.; de Herder, W.W.; Hofland, L.J. Octreotide. N. Engl. J. Med. 1996, 334, 246–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.; Smith, G.; Bleasdale-Barr, K.; Pavitt, D.V.; Mathias, C.J. Effects of the peptide release inhibitor, octreotide, on daytime hypotension and on nocturnal hypertension in primary autonomic failure. J. Hypertens. 1995, 13, 1664–1669. [Google Scholar] [PubMed]
- Raimbach, S.J.; Cortelli, P.; Kooner, J.S.; Bannister, R.; Bloom, S.R.; Mathias, C.J. Prevention of glucose-induced hypotension by the somatostatin analogue octreotide (SMS 201-995) in chronic autonomic failure: Haemodynamic and hormonal changes. Clin. Sci. 1989, 77, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.; Mathias, C.J. The effects of the somatostatin analogue, octreotide, on postural hypotension, before and after food ingestion, in primary autonomic failure. Clin. Auton. Res. 1991, 1, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.; Terai, S.; Brüning, A.; Stange, E.F. Long-term haemodynamic effects of octreotide on postprandial splanchnic hyperemia in humans: A placebo-controlled echo-doppler study. Aliment. Pharm. Ther. 1999, 13, 1119–1129. [Google Scholar] [CrossRef]
- Pederson, R.A.; Dryburgh, J.R.; Brown, J.C. The effect of somatostatin on release and insulinotropic action of gastric inhibitory polypeptide. Can. J. Physiol. Pharm. 1975, 53, 1200–1205. [Google Scholar] [CrossRef]
- Eschlböck, S.; Wenning, G.; Fanciulli, A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J. Neural. Transm. 2017, 124, 1567–1605. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Proposed model by which the gut modulates the postprandial haemodynamic response. The composition of the meal ingested, rate of small intestinal nutrient exposure and subsequent absorption of nutrients, region of small intestine exposed to nutrients and neurohormonal responses all affect postprandial haemodynamics, with the potential to influence the blood pressure response to a meal. Gut peptides, notably GLP-1 [7], GIP [8] and somatostatin [9], may have profound effects on postprandial haemodynamic responses.
Figure 1.
Proposed model by which the gut modulates the postprandial haemodynamic response. The composition of the meal ingested, rate of small intestinal nutrient exposure and subsequent absorption of nutrients, region of small intestine exposed to nutrients and neurohormonal responses all affect postprandial haemodynamics, with the potential to influence the blood pressure response to a meal. Gut peptides, notably GLP-1 [7], GIP [8] and somatostatin [9], may have profound effects on postprandial haemodynamic responses.
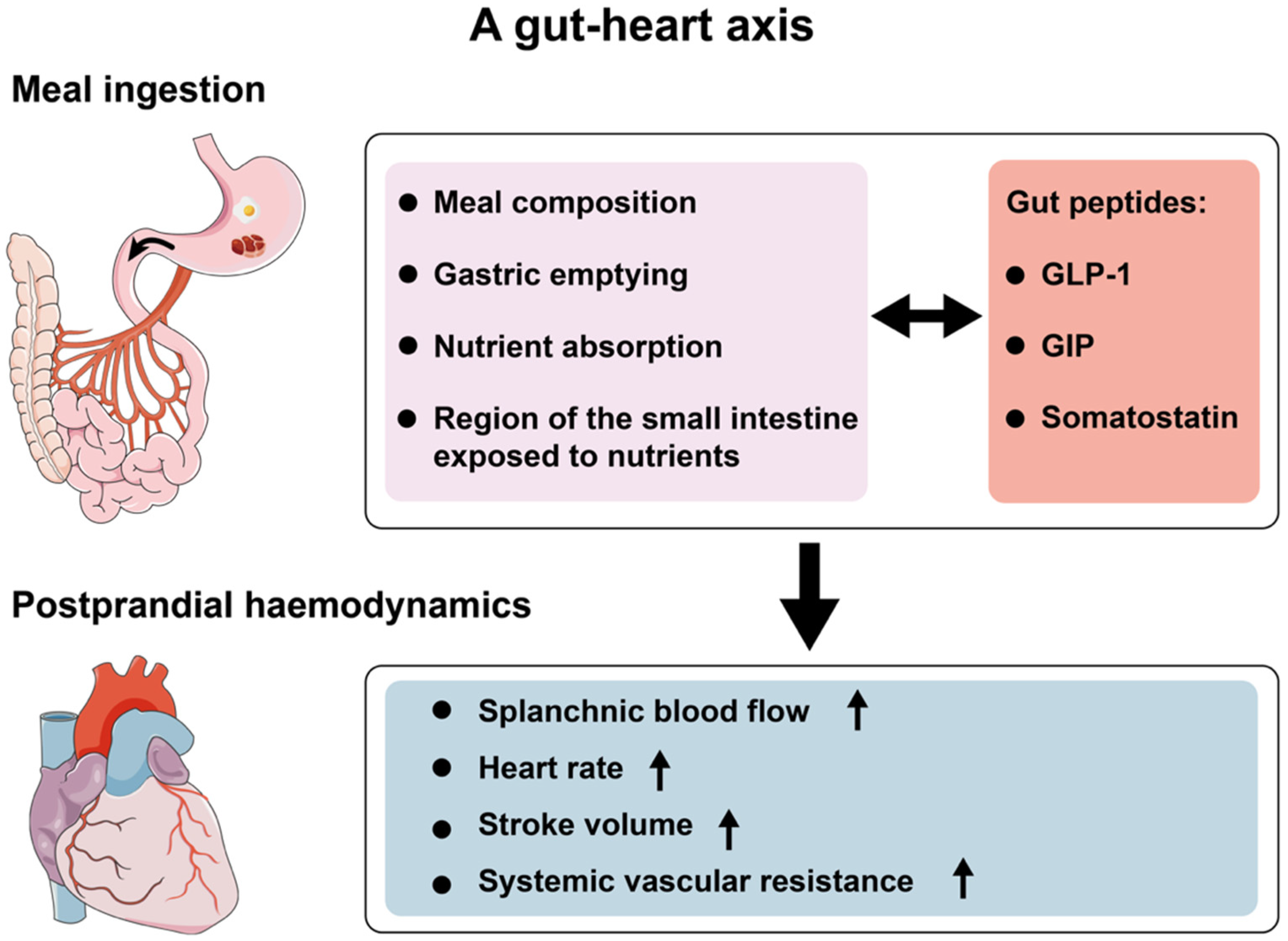
Figure 2.
Effect of intravenous GLP-1 (0.9 pmol/kg/min; open symbols) vs saline (filled symbols) on SBP and DBP before and after 75 g oral glucose in “healthy” older (n = 14; (a,c)) and T2D (n = 10; (b,d)) subjects. Data are mean values ± standard error of the mean. Intravenous GLP-1 increased DBP in “healthy” older subjects (p < 0.001), and SBP and DBP in T2D subjects (p < 0.05 for both), postprandially [7].
Figure 2.
Effect of intravenous GLP-1 (0.9 pmol/kg/min; open symbols) vs saline (filled symbols) on SBP and DBP before and after 75 g oral glucose in “healthy” older (n = 14; (a,c)) and T2D (n = 10; (b,d)) subjects. Data are mean values ± standard error of the mean. Intravenous GLP-1 increased DBP in “healthy” older subjects (p < 0.001), and SBP and DBP in T2D subjects (p < 0.05 for both), postprandially [7].
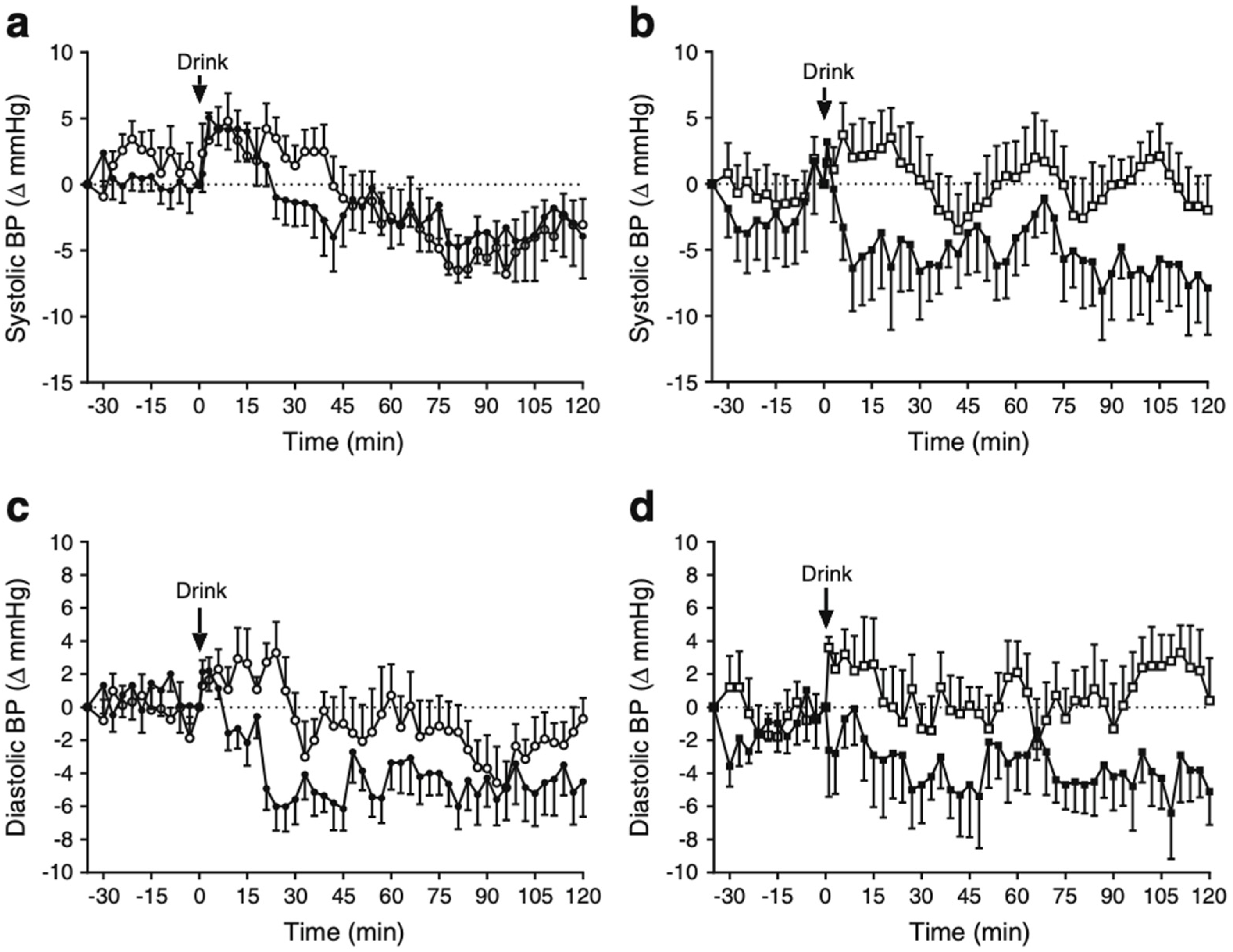
Figure 3.
Effects of lixisenatide (10 μg subcutaneously), compared with placebo, on SBP (A,B) and DBP (C,D) immediately before and after a 75 g glucose drink, in individuals with (B,D) and without T2D (A,C). Data are mean values ± standard error of the mean. Lixisenatide attenuated the fall in SBP and DBP in both groups [20].
Figure 3.
Effects of lixisenatide (10 μg subcutaneously), compared with placebo, on SBP (A,B) and DBP (C,D) immediately before and after a 75 g glucose drink, in individuals with (B,D) and without T2D (A,C). Data are mean values ± standard error of the mean. Lixisenatide attenuated the fall in SBP and DBP in both groups [20].
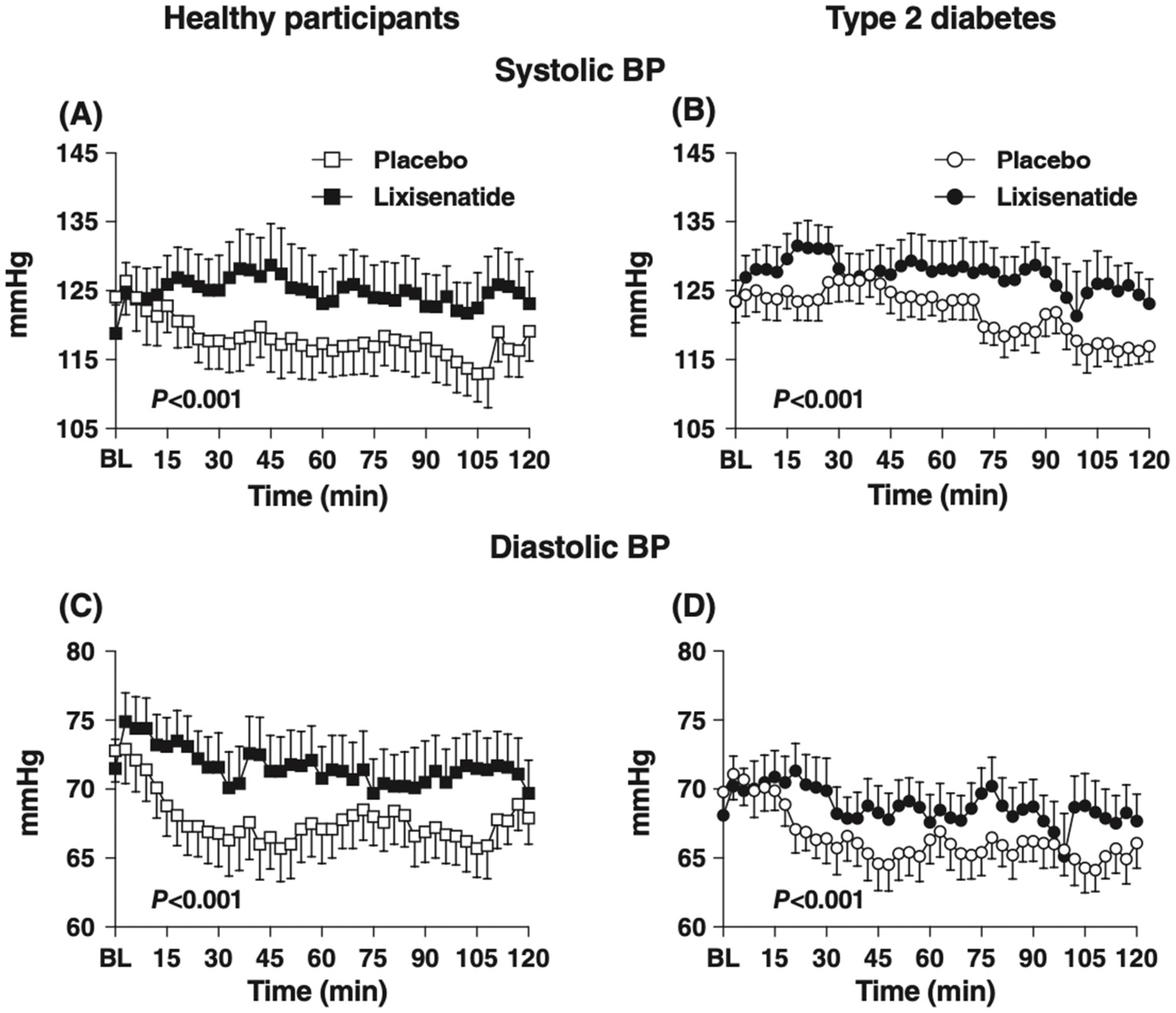
Figure 4.
Effect of intraduodenal infusion of metformin 1g, compared with placebo, on the SBP response to 50g oral glucose in T2D. Data are mean values ± standard error of the mean. Metformin attenuated the fall in SBP postprandially [57].
Figure 4.
Effect of intraduodenal infusion of metformin 1g, compared with placebo, on the SBP response to 50g oral glucose in T2D. Data are mean values ± standard error of the mean. Metformin attenuated the fall in SBP postprandially [57].
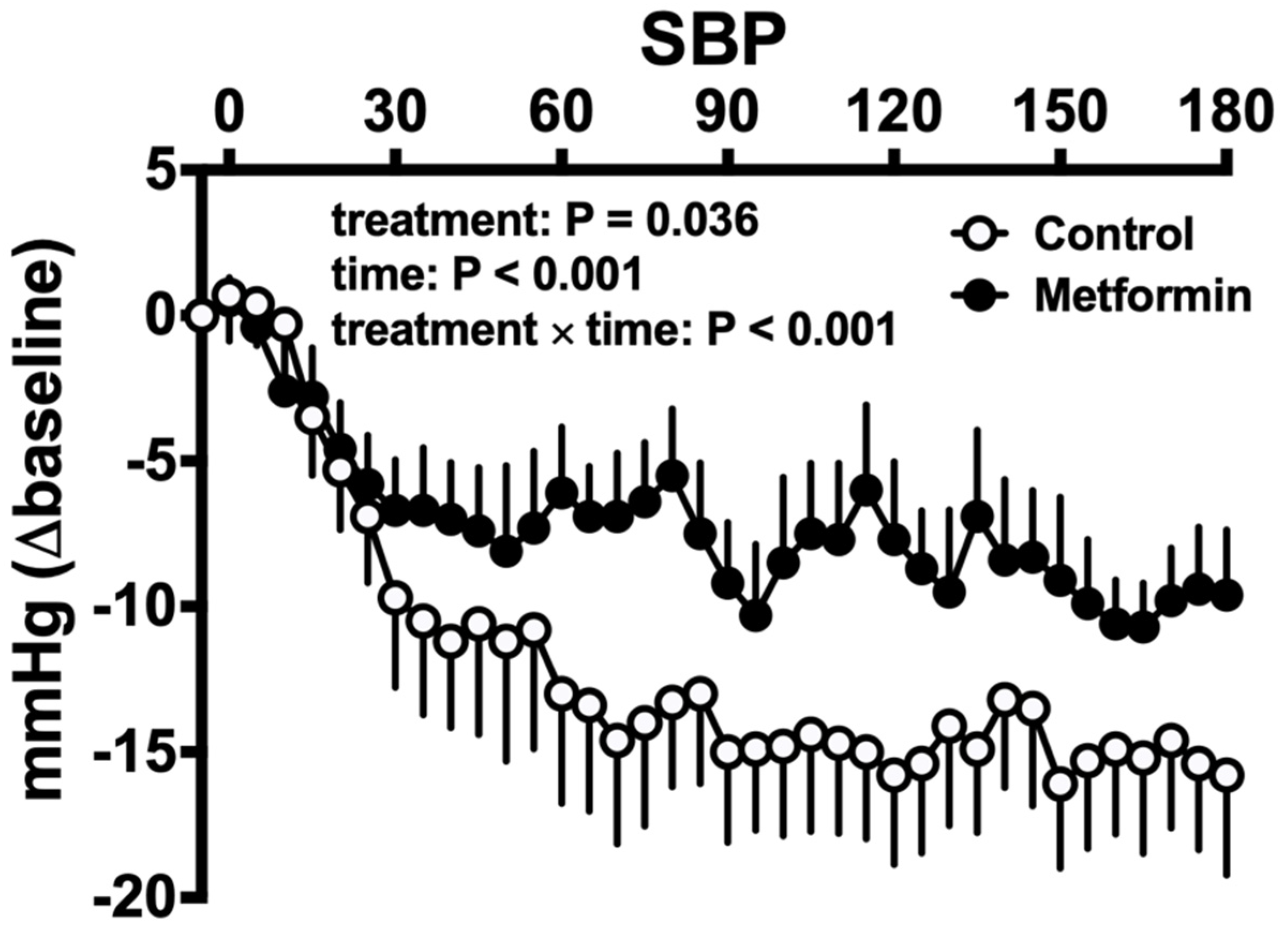
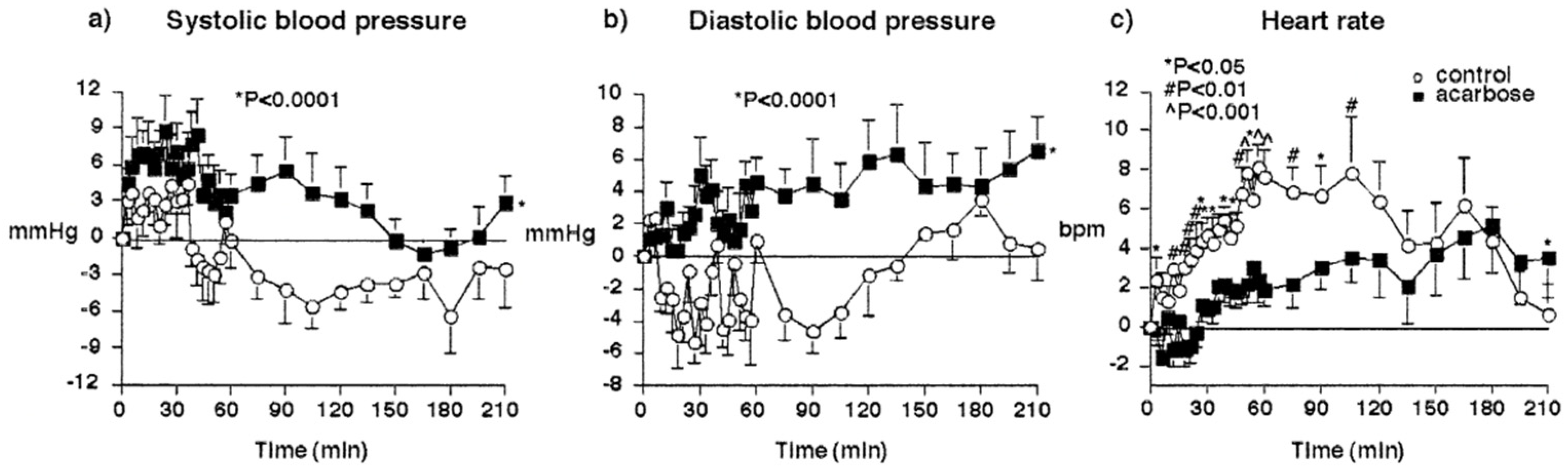
Figure 5.
Effect of 100 mg acarbose (black squares) vs. placebo (open circles) on the SBP (a), DBP (b) and heart rate (c) responses to 100 g sucrose in “healthy” older subjects. Data are mean values with 95% confidence intervals. Acarbose increased SBP and DBP, and reduced heart rate postprandially [19].
Figure 5.
Effect of 100 mg acarbose (black squares) vs. placebo (open circles) on the SBP (a), DBP (b) and heart rate (c) responses to 100 g sucrose in “healthy” older subjects. Data are mean values with 95% confidence intervals. Acarbose increased SBP and DBP, and reduced heart rate postprandially [19].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Pharmacotherapies with GLP-1 based actions and the mechanisms of their effects [24,33,34,35,36,39].
| Drug Class | Example Drugs | GLP-1 Associated Effect(s) |
|---|---|---|
| Biguanide | Metformin | secretion (directly/indirectly) DPP-4 activity (modest) |
| Alpha-glucosidase inhibitor | Acarbose Miglitol Voglibose | secretion DPP-4 activity (voglibose) |
| Short-acting GLP-1RA | Exenatide BD Lixisenatide | Activation of GLP-1 receptors |
| Long-acting GLP-1RA | Dulaglutide Exenatide QW Liraglutide Semaglutide | Activation of GLP-1 receptors |
| DPP-4 inhibitor | Alogliptin Linagliptin Sitagliptin Saxagliptin Vildagliptin | intact GLP-1 plasma half-life |
: increase; : decrease; GLP: glucagon-like peptide; DPP: dipeptidyl peptidase.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Borg, M.J.; Xie, C.; Rayner, C.K.; Horowitz, M.; Jones, K.L.; Wu, T. Potential for Gut Peptide-Based Therapy in Postprandial Hypotension. Nutrients 2021, 13, 2826. https://doi.org/10.3390/nu13082826
AMA Style
Borg MJ, Xie C, Rayner CK, Horowitz M, Jones KL, Wu T. Potential for Gut Peptide-Based Therapy in Postprandial Hypotension. Nutrients. 2021; 13(8):2826. https://doi.org/10.3390/nu13082826
Chicago/Turabian StyleBorg, Malcolm J., Cong Xie, Christopher K. Rayner, Michael Horowitz, Karen L. Jones, and Tongzhi Wu. 2021. "Potential for Gut Peptide-Based Therapy in Postprandial Hypotension" Nutrients 13, no. 8: 2826. https://doi.org/10.3390/nu13082826
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.