Abstract
Policies requiring childcare settings to promote healthy eating, physical activity, and limited screentime have the potential to improve young children’s health. However, policies may have limited impact without effective implementation strategies to promote policy adoption. In this mixed-methods study, we evaluated the type, quality, and dose of implementation strategies for state-level childcare licensing regulations focused on healthy eating, physical activity, or screentime using: (1) a survey of state licensing staff and technical assistance providers (n = 89) in 32 states; (2) a structured review of each state’s childcare licensing and training websites for childcare providers; and (3) in-depth, semi-structured interviews with 31 childcare licensing administrators and technical assistance providers across 17 states. Implementation strategies for supporting childcare providers in adopting healthy eating, physical activity, and screentime regulations vary substantially by state, in quantity and structure. Childcare programs’ financial challenges, staff turnover, and lack of adequate facilities were identified as key barriers to adoption. Access to federal food programs was seen as critical to implementing nutrition regulations. Implementation resources such as training and informational materials were rarely available in multiple languages or targeted to providers serving low-income or racially/ethnically diverse families. There is a substantial need for implementation supports for ensuring policies are successfully and equitably implemented in childcare.
1. Introduction
Eating a healthy diet, engaging in frequent physical activity, limiting screentime, and maintaining a healthy body weight are crucial for the prevention of the chronic diseases that constitute the majority of the burdens of morbidity and mortality in the U.S. Forming healthy eating and physical activity habits in early childhood has emerged as a critical point of intervention, as habits may be more difficult to change later in the life course [1]. However, young children in the U.S. often have an overall poor diet, with socioeconomic disparities reflecting structural inequities in access to healthy foods already present in early childhood [2].
Early childcare programs represent an ideal setting for intervening to improve the diet, physical activity, and screentime habits of young children. In the U.S., childcare programs serve 60% of 3–5-year-olds through center-based care and another 13% through family-based daycare programs [3]. Nutrition, physical activity, and screentime practices used in childcare have been shown to have significant impacts on children’s behaviors and healthy growth [4,5]. Yet, surveys of childcare providers across several U.S. states have indicated that best practices for healthy feeding practices, physical activity opportunities, and limited screentime viewing are rarely adopted [6,7,8].
Policies have been identified as a strategy to help ensure that childcare programs use healthy nutrition, physical activity, and screentime practices in multiple countries [9,10]. In the U.S., state-level licensing regulations are the most relevant policies with the potential to help ensure that childcare providers follow standards to promote healthy eating, physical activity, and limited screentime for the children in their care [11,12,13]. For example, regulations can specify that sugary drinks cannot be served or require that minimum amounts of physical activity opportunities be provided. Because licensed childcare providers are technically required to follow the policies prescribed in these regulations as a condition for their licensure, incorporating such requirements into state licensing regulations has the potential to result in wide-scale adoption. However, requirements for healthy eating, physical activity, and screentime practices vary widely across states [14].
Despite the promise of these requirements to improve practice, existing evidence suggests that there may be a gap in translation from what is written as requirements in state regulations to actual childcare provider practices. A study of the impact of a 2012 law in California requiring childcare providers to eliminate sugary drinks and limit 100% juice found that providers reported some improvements in promoting drinking water and reducing 100% juice, but only 23% of surveyed providers were in full compliance with the law, and only 60% were even aware of it [15]. Recent quasi-experimental studies in South Carolina and Massachusetts suggested that childcare providers did not adopt the changes in practices for nutrition or physical activity that were prescribed by new state policies [16,17].
Understanding the implementation process for state childcare licensing regulations that relate to nutrition, physical activity, and screentime practices, and how that process could be strengthened, may help identify ways to ensure that policies are fully implemented and translate into the adoption of healthy practices. Proctor’s Conceptual Model for Implementation Research (CMIR) [18] suggests the importance of researching the implementation strategies that are used to facilitate the implementation of a given intervention, in this case, the state licensing regulations related to healthy eating, physical activity, and screentime (HEPAST) practices (Figure 1).
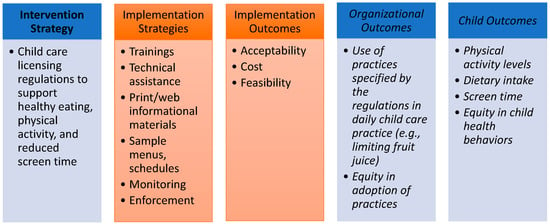
Figure 1.
Project Components Outlined by Proctor’s Conceptual Model for Implementation Research.
Comprehensive training and technical assistance are implementation strategies that have shown some promise for promoting the adoption of HEPAST regulations [4,5,19,20,21], but it is unclear how widely these are used in the U.S. Lessard et.al (2018) found that state childcare licensing staff in a sample of states that required physical activity opportunities believed that the implementation of these requirements was feasible, but that providers likely needed more support and resources for how to put these requirements into daily practice, and that state licensing agencies’ abilities to either provide that support themselves or partner with non-profit agencies to do so varied widely [22]. Even when such supports are made available, existing research suggests childcare providers are rarely able to access such opportunities, particularly in rural areas [23,24]. It is also unknown whether and how such strategies are designed and disseminated to reach childcare providers serving children of low-income households, English-language learners, and/or children from rural areas.
Using a mixed-methods approach, in this study, we aim to: (1) identify what implementation strategies are used to ensure that state licensing regulations related to healthy eating, physical activity, and screentime are put into practice; (2) assess the extent to which of these implementation strategies are applied in each state; (3) explore perceptions of the success of these strategies among licensing agency and non-governmental agency staff; and (4) evaluate whether states and childcare providers equitably apply implementation strategies.
2. Materials and Methods
2.1. Study Design
This cross-sectional study used a mixed-methods approach. From 2019–2020, we collected multiple modes of qualitative and quantitative data concurrently to capture the range of implementation strategies that states use to put healthy eating, physical activity, and screentime regulations into practice. We first reviewed state childcare regulations to identify each state’s healthy eating, physical activity, and screentime requirements for licensed childcare programs. We then collected quantitative data about implementation activities to support adoption of these requirements, using an online survey completed by administrators at state childcare licensing agencies and staff employed at non-governmental agencies that provide implementation support to childcare providers, such as childcare resource and referral agencies and non-profits or academic extension entities that provide training and technical assistance (hereafter referred to, as per Lessard et al. 2018 [22], as non-profit partners). We invited survey participants to additionally participate in an in-depth qualitative interview to obtain explanatory data about implementation activities. Finally, we conducted structured reviews of each state’s childcare licensing agency and non-profit partner websites. The data collection procedures used for each are summarized below. Assessment of equity was integrated across each data collection approach.
The Harvard T.H. Chan School of Public Health Institutional Review Board approved all study procedures and materials and classified the study as exempt.
2.2. Identification of the HEPAST Childcare Regulations
We first identified which childcare licensing regulations for HEPAST were present in each state as of June 2020. We used a database from a complementary study conducted by our research team that included information on whether each state (plus Washington DC) required a set of key healthy eating, physical activity, and screentime policies with evidence for positively impacting nutrition and physical activity behaviors and healthy weight development [25]. Forty-eight states had at least one of these HEPAST policies and are included in this analysis; the frequencies of each policy being present in state childcare licensing regulations are shown in Table 1.

Table 1.
Types of healthy eating, physical activity, and screentime (HEPAST) policies identified in state childcare licensing regulations in the study sample (n = 196 regulations across 48 states).
2.3. Quantitative Investigation of Implementation Strategies Provided in Each State
We utilized two quantitative measures to determine the extent to which states employed implementation strategies to support childcare providers in putting their healthy eating, physical activity, and screentime policies into practice. First, among the 48 states with relevant regulations, we surveyed state childcare licensing administrators and non-profit partners on the activities taking place in their state to support childcare providers in following the regulations. Second, we conducted a structured review of each state’s childcare licensing and non-profit partner websites to quantify what resources were available to support providers in putting HEPAST regulations into practice.
Sample and recruitment. The target population for the survey sample was state licensing agency administrators and their non-profit partners, (i.e., those actors that are responsible for developing and carrying out implementation strategies to support childcare providers’ adherence to state licensing regulations) among states with HEPAST regulations. We identified survey participants at state agencies by reviewing each state’s licensing website to identify contact information for administrators at the state or county level and cross-checked that information with the names listed on states’ applications for federal Child Care Development Funds. We then identified potential non-profit partner respondents by reviewing contact information from websites linked on the state licensing website (e.g., childcare resource and referral agencies, training institutes, local academic institutions). We further identified potential non-profit partner contacts by asking those who initially responded to the survey to recommend additional partners for us to recruit.
All identified potential participants were sent e-mail invitations to participate and were offered a $20 gift card for completing the survey. Individuals were classified as non-responders if the survey was not completed after three contact attempts.
Measure development: Survey. We developed a 20-min survey to capture the types of implementation strategies used to support healthy eating, physical activity, and screentime regulation implementation and the dose of those strategies, in addition to licensing administrators’ and non-profit partners’ perceptions of whether those strategies were equitably accessible. The survey development was guided by Proctor et al.’s taxonomy of implementation strategies [26]. The survey was pre-populated for each state with the list of applicable regulations as identified in the first stage of data collection [25]. For each of these pre-identified regulations, the surveys asked a series of questions about implementation strategies, including what types of strategies were used (training; consultations/technical assistance; print or website materials; training guides/implementation guidelines; suggested curricula/lesson plans; and suggested menus or food purchasing guides) and how providers were monitored for compliance with the regulations. Survey participants were also asked their perceptions towards how well the strategies worked in helping childcare providers adopt regulations. Participants were also asked if strategies were equitably designed and disseminated. For example, we asked survey respondents if training and materials were offered in multiple languages; if they had access to training related to promoting diversity and equity and/or cultural competence; and if they considered providing training or technical assistance on childcare regulations was a priority for English language learners, providers of low-income families, and/or providers serving predominantly families from marginalized racial/ethnic groups. Survey questions were reviewed by content experts in childcare HEPAST policy (e.g., state licensing agency staff and childcare technical assistance providers) to ensure that the listed implementation strategies reflected those currently used in the field.
Methods for Website review. We identified and reviewed 93 websites (n = 48 childcare state licensing websites and n = 45 childcare professional development websites) across the 48 states with HEPAST policies. We created a coding tool to describe the characteristics of the licensing websites and non-profit partner websites or training portals for each state. For the licensing and professional development/training portals, we indicated if training related to nutrition, physical activity, or screentime was listed on the website. For each training identified, we then collected information on the training topics, whether the training was accessible in multiple languages, and whether it was in-person or online.
2.4. Quantitative Analysis
We calculated frequencies for participants’ reports on the survey questions. To quantify the dose of implementation strategies employed to support each HEPAST policy, we summed the number of types of implementation supports the participants reported for each policy, stratified by whether they were reported by licensing and non-licensing agencies. If there were multiple respondents for a single agency with conflicting responses, we used the highest number reported per agency for the calculation.
2.5. Qualitative Investigation of the Perspectives on Policy Implementation
To better understand state licensing agency and non-profit partner perspectives on implementation strategies for HEPAST childcare licensing regulations, we conducted semi-structured interviews with a sub-sample of survey respondents. We invited individuals who completed at least 75% of the survey to participate in an interview (n = 96).
Measure development. We developed a 60-min semi-structured interview protocol guided by CMIR [18]. Interview questions focused first on participants’ perceptions of the appropriateness and feasibility of the HEPAST regulations and how successfully childcare providers were able to adopt the regulations; we focused on the cost, feasibility, and acceptability of the regulations themselves first given that these are also key predictors of implementation [18]. We also asked about the participants’ home states’ specific implementation strategies for HEPAST regulations, including: why specific implementation strategies were chosen; who offers the strategies (e.g., who delivers training, who provides technical assistance, who offers implementation guidance); how strategies may differ from those used for other regulatory requirements; and what implementation supports would be needed to support fuller adoption of the HEPAST regulations in childcare providers’ daily practice. We also asked participants about their perceptions of whether implementation supports were distributed equitably according to childcare program types (i.e., centers versus family childcare homes); providers’ income; location/region (including urban versus rural locations); language; and/or culture.
Content experts reviewed the interview guide. Because the interviews were conducted after the start of the COVID-19 pandemic, interviewees were asked to speak about their experiences “in normal times” (i.e., before the pandemic began).
Qualitative Analysis: We conducted interviews over Zoom or by phone and transcribed the audio-recordings verbatim. We used a framework analysis approach [27] grounded in Proctor’s model [18] to analyze the qualitative data. Four research assistants (W.J., M.K.P., K.T., and J.D.) double-coded 20% (n = 6) of the interview transcriptions. The research team reviewed coding discrepancies to identify codes that needed further refinement and clarification. With this revised codebook, coders recoded the initial interviews and double-coded the remaining 25 interviews. The research team met weekly during the coding process to discuss processes and ensure coding was consistent across all research assistants. Researchers used NVivo software to organize and sort coded data. When coding was complete, three team members (W.J., R.M., E.K.) reviewed the results and identified themes that emerged within and across codes for licensing and non-profit partner interviews. The entire research team met to review the identified themes that emerged across codes and finalize key themes.
2.6. Integrative Analysis
A critical step in mixed-methods studies is to interpret the qualitative and quantitative data across modalities, rather than simply analyzing modalities in isolation [28]. To integrate the qualitative and quantitative findings, we developed a table with rows for each of the key themes identified in the interviews, organized by the domains of the Proctor framework assessed in this study: implementation strategies and implementation outcomes. We created columns for each data source: quantitative surveys and website reviews; and qualitative interviews. We then entered what was known for each theme from each data source into the appropriate table cell. With the data thus organized, we reviewed the table across data sources to identify where themes were aligned and where themes differed. We present the data below organized by the Proctor framework and discuss the results across each mode of data collection for each theme.
3. Results
3.1. Sample Characteristics
Among the 48 states with HEPAST policies, 157 licensing administrators and staff were contacted to participate in the survey. In total, 47 responded to the survey from 32 states. Of the 218 training and technical assistance providers approached for the survey, 41 responded from 22 states. Across the 39 states represented by the licensing agency respondents, the states had a mean of 5.0 (SD: 2.4) regulations related to HEPAST, with 2.5 (SD: 0.9) related to nutrition, 1.7 (SD: 1.0) related to physical activity, and 1.7 (SD: 0.7) related to screentime per state (Table 1). Most survey respondents (83%) identified as white, and the mean respondent age was 51.3 (SD: 10.2). Most respondents had a college (44%) or master’s degree (47%) (Table 2). Among the 96 survey respondents who were invited, 12 licensing agency administrators and 19 non-profit partners across 17 states agreed to participate.
Table 2.
Demographics of the survey respondents 1.
3.2. Implementation Strategies Utilized
Overall, survey respondents at non-profit partners reported providing higher levels of implementation support and addressing implementation of more regulations than licensing agencies. On average, via the survey, non-profit partners reported providing 4.4 (SD: 2.1) implementation supports for each HEPAST regulation in their state while licensing staff reported providing 3.3 supports (SD: 1.9) (Table 3). Non-profit partners frequently reported providing technical assistance (for 87% of regulations) and training (90% of regulations). Meanwhile, licensing staff were most likely to cite monitoring for compliance during in-person licensing visits as an implementation strategy for HEPAST regulations (97% of regulations) in addition to providing brief technical assistance. In terms of how licensing agency staff monitored for compliance with HEPAST regulations, survey respondents reported that reviews of menus or schedules (84%) and observations of mealtimes and physical activity times (91%) were conducted for most HEPAST regulations. In the event of finding noncompliance with an HEPAST regulation, licensing survey respondents reported that a conversation with the provider was the most common consequence; written warnings or citations rarely occurred (Table 3).
Table 3.
Number and types of strategies in place for supporting implementation of HEPAST childcare licensing regulations reported by licensing staff and non-profit partners.
Training was less commonly provided by licensing staff, who reported providing training support to 58% of providers; more training was offered for physical activity regulations (69%) than nutrition (56%) or screentime (44%) (Table 3). This pattern was also seen in our review of state websites, which found that only 19% of state licensing websites provided training opportunities related to HEPAST regulations for childcare providers. In contrast, 67% of non-profit partner websites provided training opportunities.
Implementation guidelines, or written documents that help explain the meaning of childcare licensing regulations and specific activities or objectives that can be met to meet compliance, were less commonly used. Licensing staff reported that their agency provided implementation guidelines to help outline practices that would meet the standards for 50% of the regulations; non-profit partners reported providing guidelines to help meet 67% of the regulations (Table 3). Sample menus or schedules, which have been cited by providers as being especially helpful [29], were provided for only 30% of regulations by licensing agency respondents, and 51% of regulations by non-profit partners (Table 3).
While the survey and website results provided information on the overall availability of different implementation supports, the interviews helped elucidate what the different strategies looked like in practice (Table 4). Overall, states varied substantially in how their implementation supports were operationalized. A key theme from the qualitative interviews was that the term “technical assistance” is viewed very broadly by licensing agencies and can have multiple meanings. The term was used by interviewees in reference to simply providing resources on their website; a quick phone call or e-mail in response to a provider’s question; or apply to more intensive coaching over several visits or sessions. How technical assistance provided, and by whom, was also described differently across states. Many state childcare licensing agencies have dedicated employees (oftentimes licensing specialists) to answer via calls, texts, or emails with questions from providers. Other states fully contract technical assistance support to resource and referral agencies to field providers’ questions. Licensing staff in particular described technical assistance as something that was often provided reactively in response to rule violations seen during monitoring visits, rather than proactively provided.
Table 4.
Integration of quantitative and qualitative data describing state implementation strategies for healthy eating, physical activity, and/or screentime regulations.
Licensing staff were more likely to see their key role in the implementation process as being monitors for compliance with the regulations. Several licensing interviewees additionally described monitoring visits as an opportunity to offer more implementation support, as it was an opportunity to interact with providers in person. Licensing interviewees said they write citations or reports in response to a HEPAST regulation violation and assign licensing specialists to help providers to come up with a plan to correct the violation and move into compliance within a specific timeframe.
Participants mostly reported supportive and non-punitive responses to licensing violations related to HEPAST. One participant mentioned rules violations being posted to their state childcare website, but none used monetary fines as a method of enforcement. One sentiment shared was that some providers were hesitant to ask licensing agencies for clarification or support in fears they will get in trouble, and therefore turn to non-profit partners for assistance instead. One licensing agency respondent noted that HEPAST regulations are more difficult to regulate: “When the licensor is there, it’s just a quick snapshot of what’s happening. And so it’s kind of hard to know if they’re [the childcare programs] really following those rules”.
3.3. Implementation Outcomes (Cost, Feasibility, Fidelity, Acceptability, Equity, Sustainability)
Cost. The theme of cost as a barrier to fulfilling HEPAST regulations, particularly related to nutrition, was consistent across interviews with both licensing and non-profit partners. One participant said, “I think sometimes it’s hard for providers to provide healthy choices for children because I know it does cost a lot more”. Another participant noted, “Teaching nutrition is just…some of it actually is monetary, is money. To have fresh vegetables and fresh fruit…it is more expensive than not”. Smaller childcare centers, family childcare home providers, and providers serving a higher proportion of low-income children struggled more than larger childcare centers. One participant said, “[Smaller providers’] monthly bills take most of the income that the center is earning. They have a harder time (if it’s anything that’s going to be a cost involved in some standards) meeting those, just because maybe their finances are more limited than a larger [program]--you know one that’s a corporation type facility where it’s maybe a bigger organization, where they have a little more free money”.
The time cost involved in preparing and serving healthier foods was also highlighted as a way in which many providers struggle to meet healthier eating policies. Additionally, participants described how a lack of funding for physical activity equipment (e.g., playground equipment, fences) can make it difficult for some providers to fully implement regulations related to physical activity.
Feasibility. Licensing interview participants generally reported they felt the HEPAST regulations were feasible for providers to implement. However, non-profit partner participants reported that they felt many of their state’s HEPAST regulations were not feasible for some providers. Non-profit partners described high staff turnover in childcare programs as a key hurdle that makes implementation of HEPAST regulations less feasible. Non-profit partners also mentioned that accessing the implementation supports themselves was not always feasible for providers. Lack of reliable internet access and availability to attend day-time training made it difficult for providers (especially home providers) to attend offered training. Participants also raised several logistical challenges that providers face in adhering to physical activity regulations specifically, such as when weather conditions preclude outdoor play and/or programs do not have access to indoor physical activity facilities. Access to facilities such as playgrounds and fences, particularly in family childcare homes, makes it difficult for programs to meet physical activity program requirements.
Fidelity. State licensing participants overall reported that they felt childcare providers comply with HEPAST regulations, though they acknowledged that their visits are a snapshot in time. Interview participants did not feel that physical activity and screentime regulations were followed to the same degree as nutrition regulations. Extreme weather was cited as a reason that physical activity regulations in particular may be difficult to follow. One interviewee also commented on how home providers have a more difficult time following physical activity regulations due to the cost of equipment.
Acceptability. Licensing participants mostly felt that a majority of childcare providers find the HEPAST regulations acceptable. When an HEPAST regulation is first introduced, participants felt that there could be pushback from providers, but messaging and raising awareness helped establish buy-in. However, non-profit partners had a different perspective. They reported that while childcare providers may follow HEPAST regulations during licensing visits, they may not actually find them acceptable due to a lack of understanding of why the regulations are in place. Several also reported that they felt regulations were difficult for providers to follow, especially regulations related to physical activity and screentime. One respondent said, “Ok, [our state] has strong childcare regulations. Could they be stronger? Sure. But I think that what we tried to do was to balance, to have an effective balance between the needs of providers and the needs of children. So I think they’re just right. Goldilocks”. Meanwhile, another noted, “Screentime and physical activity, I feel like are very low priorities in a lot of programs. And those are [practices] that are just hard to regulate”.
Several respondents from both licensing agencies and non-profit partners expressed that ensuring healthy eating policies were followed was much more effective when carried out via CACFP, suggesting that this federal food program may be a more appropriate intervention mechanism for ensuring healthy eating than childcare licensing regulations. One respondent stated, “So, I mentioned if they’re on the food program [CACFP] there’s definitely more regulation. And so I think that’s good. I think the healthy eating definitely has the most regulation because if they don’t meet those requirements, they won’t get reimbursed for the food. They have separate inspections, they have separate training for that”.
In both the quantitative survey and qualitative interviews, participants were asked their perspective on whether HEPAST regulations were a priority compared to other regulations. On the quantitative survey, respondents ranked 77% of HEPAST regulations as being “about the same priority as any other rule” for implementation support while 13% of regulations were ranked as being “not a priority” or a “minimal priority”. For the qualitative interviews, several interviewees noted that while they felt HEPAST regulations were appropriate, they also felt that ensuring their implementation was often not highly prioritized. Others noted that HEPAST regulations maintained the same priority as other regulations. Both licensing staff and non-profit partners noted that training to support HEPAST regulations are less often mandatory compared to training on topics related to preventing child health emergencies, such as choking or sudden infant death syndrome (SIDS).
Equity. Concerns about equitable implementation, with regards to provider language, rurality, technological capability, culture, and whether a program was a center versus a family childcare home, emerged in both quantitative and qualitative data. With regard to language, licensing survey respondents reported that fewer than 50% of training and technical assistance opportunities were offered in multiple languages; meanwhile, the website review found only 5% of HEPAST-related training, across both state licensing and non-profit partner websites, were available in a language other than English. Some interview participants reported that they had Spanish-speaking staff to translate materials and provide some training and technical assistance support, yet only one participant mentioned any translation services available to providers in a language other than English or Spanish. Based on location, participants reported that rural childcare providers were harder to reach to provide support, and that they have a more difficult time attending training compared to providers located in more urban areas. Participants also noted that the COVID-19 pandemic, because it resulted in many agencies defaulting to online training, illuminated additional equity challenges with respect to technology. Interview participants mentioned that many childcare providers do not have equipment to adapt to online resources and training and are also unfamiliar with technology. With regard to culture and race/ethnicity, ensuring equity by race/ethnicity and culture did not emerge as a priority topic from the surveys and website reviews. For example, in the website review, we found that 13% of states had any sort of training related to cultural competence in nutrition for this age group. Non-profit partners appeared to be considering racial/ethnic and cultural equity more than licensing staff. For example, no licensing staff mentioned differences in implementation by the race/ethnicity of providers or children served, or issues related to these constructs, but non-profit partners did have these issues on their radar; in contrast, licensing staff appeared to be more mindful of needing to provide targeted support for providers serving families with low incomes. In the survey, 69% of non-profit partners reported prioritizing providers serving primarily racial/ethnic minority families, and 74% prioritized providers serving families with low incomes while for licensing staff, those percentages were 20% and 40%, respectively. One non-profit partner said, “But whenever we talk about cultural diversity and just talking about food, for example, it always comes down to like the taco, you know -- and that kind of reeks of tokenism in a sense, you know, and being able to say, ‘hey, we checked off, you know, something that’s Hispanic Latino, excuse me, a Latin American type of food staple’. But I don’t really think it goes in the depth of like what can providers in their respective communities do to make their foods acceptable under these standards”. Finally, many licensing participants reported equity issues between centers and family childcare home providers. Participants noted that family childcare home providers cannot attend training during work hours and usually need to travel further to attend training.
Sustainability. Interviewees were split in terms of how sustainable their implementation efforts were. Some felt as though they did not need to constantly retrain providers on nutrition, physical activity, or screentime regulations, and that only brief refreshers would be necessary. Others felt as though they constantly needed to retrain providers. Staff turnover came up frequently as a reason why providers needed to be retrained. Interview participants also mentioned how family childcare home providers needed to be retrained much less often than center providers, as there is much less turnover in homes.
Apart from the challenge of addressing staff turnover, participants considered how to make training and knowledge transfer to childcare providers more sustainable and durable. Several participants reported that training using hands-on learning techniques and in-person training seemed to produce more lasting results than lecture-based or web-based training. Combining training with long-term coaching, support, and technical assistance was considered the most sustainable way to ensure that the best practices for regulation implementation were adopted. One non-licensing participant said, “I do not think a one and done training gives them what they need. I think if you want anything to be meaningful and impactful, you have to attach some kind of coaching with it”.
4. Discussion
State-level childcare licensing regulations have been identified as a key policy lever for helping to create healthy nutrition, physical activity, and screentime environments for young children [12,13]. This has led to efforts to codify stronger and more comprehensive regulations in many states. While developing stronger written regulations is an important first step, it is not guaranteed that regulations will be implemented and adopted into practice. In this comprehensive, mixed-methods study, we triangulated several quantitative and qualitative data sources to evaluate the extent to which states support childcare providers in implementing licensing regulations related to healthy eating, physical activity, and screentime. Our results suggest that implementation supports vary extensively across states and, altogether, that childcare providers may not be receiving the supports they need to fully adopt state-level nutrition, physical activity, and screentime regulations. The incorporation of requirements for healthy eating, physical activity, and screentime best practices in childcare licensing regulations is an important first step for a policy-level intervention to promote healthy weight in childcare settings, but it is not the only step. More comprehensive and robust consideration of how to support childcare licensing and technical assistance providers who are charged with ensuring implementation of these policies is needed.
Monitoring for compliance was typically the most commonly used implementation strategy by state licensing agencies, with training of varying lengths, frequencies, and effectiveness also commonly used. Technical assistance was reported as a frequent strategy by both licensing staff and non-profit partners, but the meaning of it varied substantially—from a brief phone call to a more robust coaching strategy. Evidence suggests that more intensive and comprehensive programs may be needed to effectively support providers in changing behaviors for HEPAST policy adherence. For example, the Active Early intervention, which provided between 30 and 60 h of in-person technical assistance along with training and microgrants to support program changes in order to help providers meet the policy goal of providing 120 min of physical activity opportunities each day, resulted in significant improvements in provider practices and in children’s time spent in moderate-to-vigorous physical activity [20]. The Nutrition and Physical Activity Self-Assessment for Child Care (NAP SACC) and its more recent iteration, Go NAP SACC, are additional examples of a more intensive intervention that has been found to improve provider practices, guiding providers through a self-assessment process, goal setting, training, and technical assistance [4,19]. The Nemours Early Care and Education Learning Collaboratives (ECELC), similarly, are a series of five in-person learning collaborative workshops that support providers in helping one another learn best practices to promote healthy eating, physical activity, and reduced screentime in their programs [30]. These programs show enormous promise, and NAP SACC and ECELC in particular have been disseminated across several states, but the number of states participating in meaningful and impactful technical assistance programs such as these could be further expanded. Moreover, while these programs would certainly be resource-intensive, they may be a better investment of resources than the status quo of providing low-dose support.
At the same time, given the concerns participants in this study (particularly non-profit partners) raised regarding inequities along dimensions of income, race/ethnicity, language, rurality, and technological capacity, there should be careful consideration of how to structure implementation strategies, including the types of programs described above, so that they can be equitably accessed. Strategies that support high-quality care do not necessarily have to only be accessible only to better-resourced childcare programs—Head Start, for example, provides high-quality care and focuses specifically on families living in poverty—but prioritizing equitable access in the rollout of the strategies is necessary for ensuring that existing inequities do not widen.
Cost and staff turnover were consistently reported as barriers to implementation among survey and interview respondents. Improved practices were more difficult to maintain when staff were constantly churning, making it necessary to continually restart implementation assistance. These findings point to larger, structural problems in how childcare is funded and supported in the U.S. Despite being vital to millions of families, childcare programs are not universally funded in the same way that kindergarten-12th-grade education is in the U.S. With little public investment in childcare [31], and poverty-level wages for the childcare workforce [32], childcare providers are often struggling with a range of operational issues, and may have limited capacity both to focus on healthy eating, physical activity, or screentime policies at all and to sustain any changes. Efforts to improve healthy eating, physical activity, and screentime in childcare settings may need to consider partnering with those working to improve childcare funding in the U.S. as a necessary pre-condition to effect more intensive changes.
Strengths of this study include using a mixed-methods approach to best understand state-level variation in HEPAST regulations and the types of implementation strategies available to childcare providers. Triangulation of the survey results, website reviews, and interviews of licensing and non-profit partners allowed for a comprehensive analysis to describe state-level implementation strategies. This study also had several limitations. Because we were limited in scope to collecting the perspectives of state-level licensing staff and non-profit partners, we were unable to investigate how many providers the implementation strategies reached or how effective the implementation strategies were at supporting actual changes in provider practices. Without current data on reach and effectiveness for providers, we were also unable to directly assess potential inequities in access to supportive implementation strategies. An additional limitation is that while we were able to collect perspectives from licensing staff and non-profit partners across a diverse group of states, we still did not have full coverage in our sample. It is possible that our results may have been different had our response rate been higher.
5. Conclusions
This study suggests that more robust implementation supports are needed to promote effective implementation of healthy eating, physical activity, and screentime regulations for childcare settings. Licensing agencies and non-profit partners who support childcare providers in adopting practices that meet regulatory standards may need to provide more intensive coaching and training to help providers meet standards related to healthy eating, physical activity, and screentime, which in turn may require more funding support. Efforts to improve policy implementation should carefully consider potential inequities in access to implementation supports.
Author Contributions
Conceptualization, E.L.K., N.F. and A.L.C.; methodology, E.L.K., R.M.L., A.L.C. and Z.D.B.; formal analysis E.L.K., M.K.P., R.S.M., W.J., K.T. and J.D.; investigation, E.L.K., R.S.M., N.F. and A.L.C.; resources, E.L.K. and N.F.; writing—original draft preparation, E.L.K. and R.S.M.; writing—review and editing, E.L.K., R.S.M., W.J., K.T., J.D., M.K.P., Z.D.B., A.L.C., R.M.L. and N.F.; supervision, E.L.K.; funding acquisition, E.L.K., N.F. and A.L.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Healthy Eating Research, a national program of the Robert Wood Johnson Foundation (Grants #72062 and #76298). E.L.K. was supported by a National Institute of Diabetes and Digestive and Kidney Diseases Career Development Award (K01DK125278). M.K.P. was supported by a T32 training grant from the National Institutes of Health (NIH) (DK 007703-22); A.L.C. and E.L.K. were supported in part by funding from the Centers for Disease Control and Prevention (U48-DP006376).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Harvard T.H. Chan School of Public Health.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to privacy protection.
Acknowledgments
We would like to thank Misty Pearson for her review of the study materials and the Healthy Eating Research/Nutrition and Obesity Policy Research and Evaluation Network Early Care and Education Working Group for feedback on the study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1–s56. [Google Scholar] [PubMed]
- Welker, E.B.; Jacquier, E.F.; Catellier, D.J.; Anater, A.S.; Story, M.T. Room for Improvement Remains in Food Consumption Patterns of Young Children Aged 2–4 Years. J. Nutr. 2018, 148, 1536–1546S. [Google Scholar] [CrossRef] [PubMed]
- Snyder, T.D.; de Brey, C.; Dillow, S.A. Digest of Education Statistics 2016 (NCES 2017-094); National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education: Washington, DC, USA, 2018.
- Alkon, A.; Crowley, A.A.; Neelon, S.E.B.; Hill, S.; Pan, Y.; Viet, N.; Rose, R.; Savage, E.; Forestieri, N.; Shipman, L.; et al. Nutrition and Physical Activity Randomized Control Trial in Child Care Centers Improves Knowledge, Policies, and Children’s Body Mass Index. BMC Public Health 2014, 14, 215. [Google Scholar] [CrossRef]
- Stookey, J.D.; Evans, J.; Chan, C.; Tao-Lew, L.; Arana, T.; Arthur, S. Healthy Apple Program to Support Child Care Centers to Alter Nutrition and Physical Activity Practices and Improve Child Weight: A Cluster Randomized Trial. BMC Public Health 2017, 17, 965. [Google Scholar] [CrossRef]
- Loth, K.; Shanafelt, A.; Davey, C.; Anfinson, A.; Zauner, M.; Looby, A.A.; Frost, N.; Nanney, M.S. Provider Adherence to Nutrition and Physical Activity Best Practices Within Early Care and Education Settings in Minnesota, Helping to Reduce Early Childhood Health Disparities. Health Educ. Behav. 2019, 46, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Nanney, M.S.; LaRowe, T.L.; Davey, C.; Frost, N.; Arcan, C.; O’Meara, J. Obesity Prevention in Early Child Care Settings: A Bistate (Minnesota and Wisconsin) Assessment of Best Practices, Implementation Difficulty and Barriers. Health Educ. Behav. 2017, 44, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Tovar, A.; Risica, P.; Mena, N.; Lawson, E.; Ankoma, A.; Gans, K.M. An Assessment of Nutrition Practices and Attitudes in Family Child-Care Homes: Implications for Policy Implementation. Prev. Chronic Dis. 2015, 12, 88. [Google Scholar] [CrossRef][Green Version]
- Vercammen, K.A.; Frelier, J.M.; Poole, M.K.; Kenney, E.L. Obesity Prevention in Early Care and Education: A Comparison of Licensing Regulations Across Canadian Provinces and Territories. J. Public Health 2020, 42, 362–373. [Google Scholar] [CrossRef]
- Lucas, P.J.; Patterson, E.; Sacks, G.; Billich, N.; Evans, C.E. Preschool and School Meal Policies: An Overview of What We Know about Regulation, Implementation and Impact on Diet in the UK, Sweden, and Australia. Nutrients 2017, 9, 736. [Google Scholar] [CrossRef]
- National Resource Center for Health and Safety in Child Care and Education, University of Colorado Denver. Achieving a State of Healthy Weight: A National Assessment of Obesity Prevention Terminology in Child. Care Regulations 2010; National Resource Center for Health and Safety in Child Care and Early Education: Aurora, CO, USA, 2011. [Google Scholar]
- Kaphingst, K.M.; Story, M. Child Care as an Untapped Setting for Obesity Prevention: State Child Care Licensing Regulations Related to Nutrition, Physical Activity and Media Use for Preschool-Aged Children in the United States. Prev. Chronic Dis. 2009, 6, 11. [Google Scholar]
- Reynolds, M.A.; Cotwright, C.J.; Polhamus, B.; Gertel-Rosenberg, A.; Chang, D. Obesity Prevention in the Early Care and Education Setting: Successful Initiatives across a Spectrum of Opportunities. J. Law. Med. Ethics 2013, 41, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Fox, T.; Corbett, A.; Duffey, K. Early Care and Education Policies and Programs to Support Healthy Eating and Physical Activity: Best Practices and Changes over Time. Research Review: 2010–2016; Healthy Eating Research: Durham, NC, USA, 2017; pp. 2010–2016. Available online: https://healthyeatingresearch.org/wp-content/uploads/2018/01/her_ece_011718-1.pdf (accessed on 18 July 2022).
- Ritchie, L.D.; Sharma, S.; Gildengorin, G.; Yoshida, S.; Braff-Guajardo, E.; Crawford, P. Policy Improves what Beverages are Served to Young Children in Child Care. J. Acad. Nutr. Diet. 2015, 115, 724–730. [Google Scholar] [CrossRef]
- Benjamin Neelon, S.E.; Finkelstein, J.; Neelon, B.; Gillman, M.W. Evaluation of a Physical Activity Regulation for Child Care in Massachusetts. Child. Obes. 2017, 13, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Benjamin Neelon, S.E.; Mayhew, M.; O’Neill, J.R.; Neelon, B.; Li, F.; Pate, R.R. Comparative Evaluation of a South Carolina Policy to Improve Nutrition in Child Care. J. Acad. Nutr. Diet. 2016, 116, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.K.; Landsverk, J.; Aarons, G.; Chambers, D.; Glisson, C.; Mittman, B. Implementation Research in Mental Health Services: An Emerging Science with Conceptual, Methodological and Training Challenges. Adm. Policy Ment. Health 2009, 36, 24–34. [Google Scholar] [CrossRef]
- Ward, D.S.; Benjamin, S.E.; Ammerman, A.S.; Ball, S.C.; Neelon, B.H.; Bangdiwala, S.I. Nutrition and Physical Activity in Child Care: Results from an Environmental Intervention. Am. J. Prev. Med. 2008, 35, 352–356. [Google Scholar] [CrossRef]
- LaRowe, T.L.; Tomayko, E.J.; Meinen, A.M.; Hoiting, J.; Saxler, C.; Cullen, B. Active Early: One-Year Policy Intervention to Increase Physical Activity among Early Care and Education Programs in Wisconsin. BMC Public Health 2016, 16, 607. [Google Scholar] [CrossRef]
- Wolfenden, L.; Jones, J.; Williams, C.M.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to Improve the Implementation of Healthy Eating, Physical Activity and Obesity Prevention Policies, Practices or Programmes within Childcare Services. Cochrane Database Syst. Rev. 2020, 2, CD011779. [Google Scholar] [CrossRef]
- Lessard, L.; Speirs, K.E.; Slesinger, N. Implementation Strategies Used by States to Support Physical Activity Licensing Standards for Toddlers in Early Care and Education Settings: An Exploratory Qualitative Study. Child. Obes. 2018, 14, 386–392. [Google Scholar] [CrossRef]
- Foster, J.S.; Contreras, D.; Gold, A.; Keim, A.; Oscarson, R.; Peters, P.; Procter, S.; Remig, V.; Smathers, C.; Mobley, A.R. Evaluation of Nutrition and Physical Activity Policies and Practices in Child Care Centers within Rural Communities. Child. Obes. 2015, 11, 506–512. [Google Scholar] [CrossRef]
- Sigman-Grant, M.; Christiansen, E.; Fernandez, G.; Fletcher, J.; Johnson, S.L.; Branen, L.; Price, B.A. Child Care Provider Training and a Supportive Feeding Environment in Child Care Settings in 4 States, 2003. Prev. Chronic Dis. 2011, 8, A113. [Google Scholar]
- Kenney, E.L.; Mozaffarian, R.S.; Frost, N.; Ayers Looby, A.; Cradock, A.L. Opportunities to Promote Healthy Weight Through Child Care Licensing Regulations: Trends in the United States, 2016–2020. J. Acad. Nutr. Diet. 2021, 121, 1763–1774. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation Strategies: Recommendations for Specifying and Reporting. Implement Sci. 2013, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework Method for the Analysis of Qualitative Data in Multi-Disciplinary Health Research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Castro, F.G.; Kellison, J.G.; Boyd, S.J.; Kopak, A. A Methodology for Conducting Integrative Mixed Methods Research and Data Analyses. J. Mix. Methods Res. 2010, 4, 342–360. [Google Scholar] [CrossRef]
- Seward, K.; Finch, M.; Yoong, S.L.; Wyse, R.; Jones, J.; Grady, A.; Wiggers, J.; Nathan, N.; Conte, K.; Wolfenden, L. Factors that Influence the Implementation of Dietary Guidelines Regarding Food Provision in Centre Based Childcare Services: A Systematic Review. Prev. Med. 2017, 105, 197–205. [Google Scholar] [CrossRef]
- Smith, T.M.; Blaser, C.; Geno-Rasmussen, C.; Shuell, J.; Plumlee, C.; Gargano, T.; Yaroch, A.L. Improving Nutrition and Physical Activity Policies and Practices in Early Care and Education in Three States, 2014–2016. Prev. Chronic Dis. 2017, 14, E73. [Google Scholar] [CrossRef]
- Isaacs, J.B.; Lou, C.; Hahn, H.; Lauderback, E.; Quakenbush, C. Public Spending on Infants and Toddlers in Six Charts: A Kids’ Share Brief; Urban Institute: Washington, DC, USA, 2019; Available online: https://www.urban.org/sites/default/files/publication/100198/public_spending_on_infants_and_toddlers.pdf (accessed on 18 July 2022).
- Otten, J.J.; Bradford, V.A.; Stover, B.; Hill, H.D.; Osborne, C.; Getts, K.; Seixas, N. The Culture of Health in Early Care and Education: Workers’ Wages, Health and Job Characteristics. Health Aff. 2019, 38, 709–720. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).