
Treatment of Urinary Tract Infections with Canephron® in Germany: A Retrospective Database Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population and Covariables
2.3. Statistical Analyses
3. Results
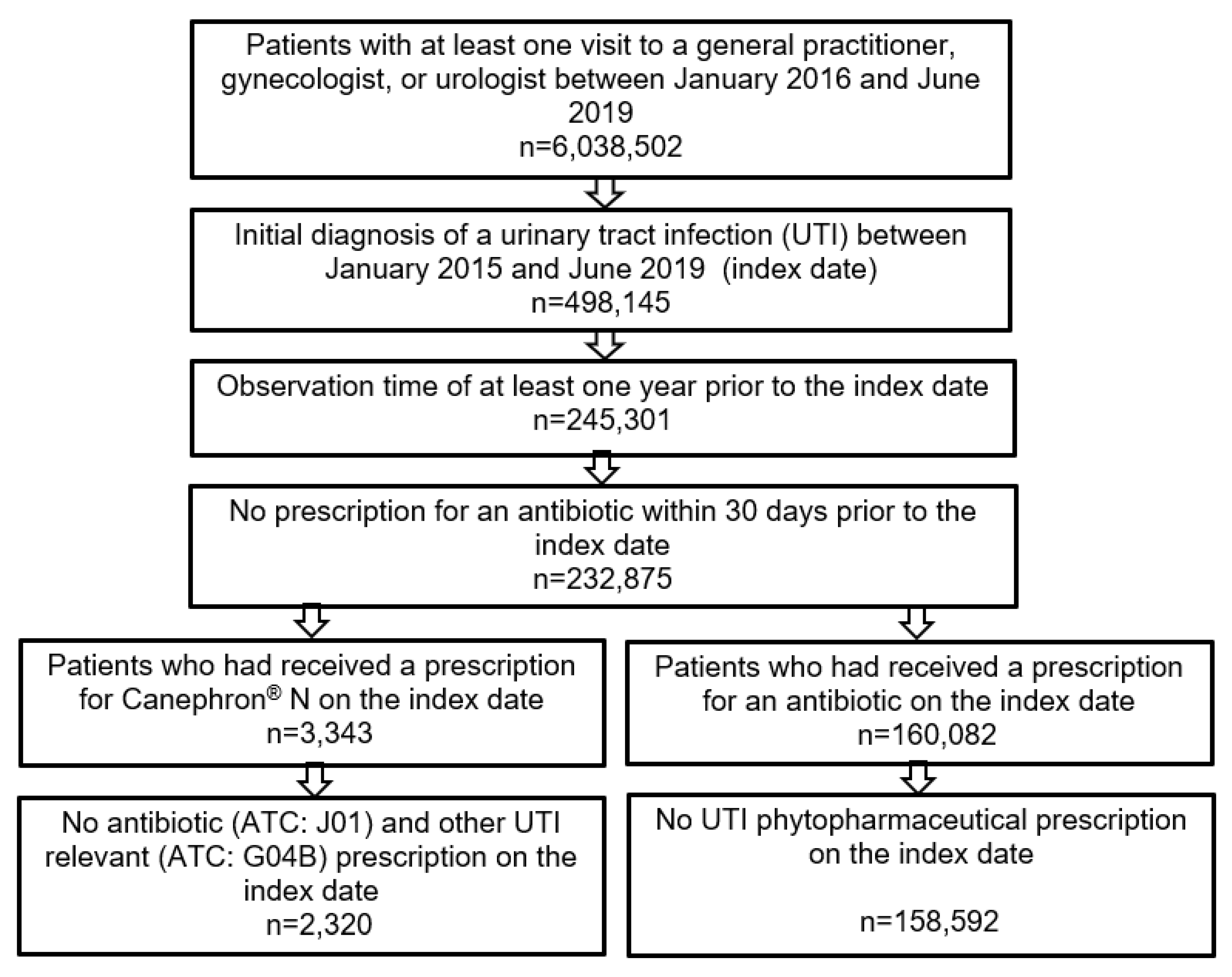
3.1. Patient Selection and Baseline Characteristics of Study Patients
3.2. Sporadic Recurrent Urinary Tract Infection
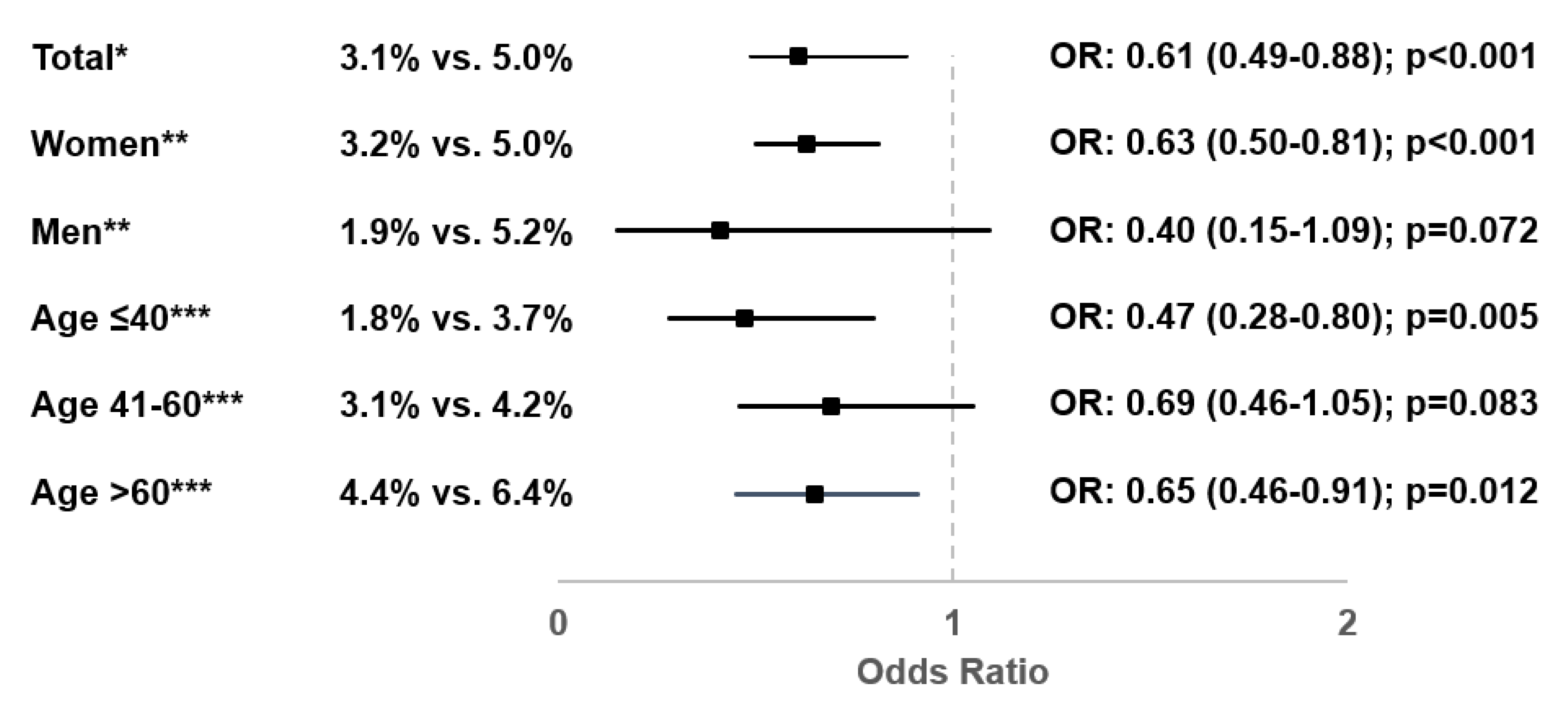
3.3. Frequent Recurrent Urinary Tract Infections
3.4. Sick Leave Associated with a Urinary Tract Infection
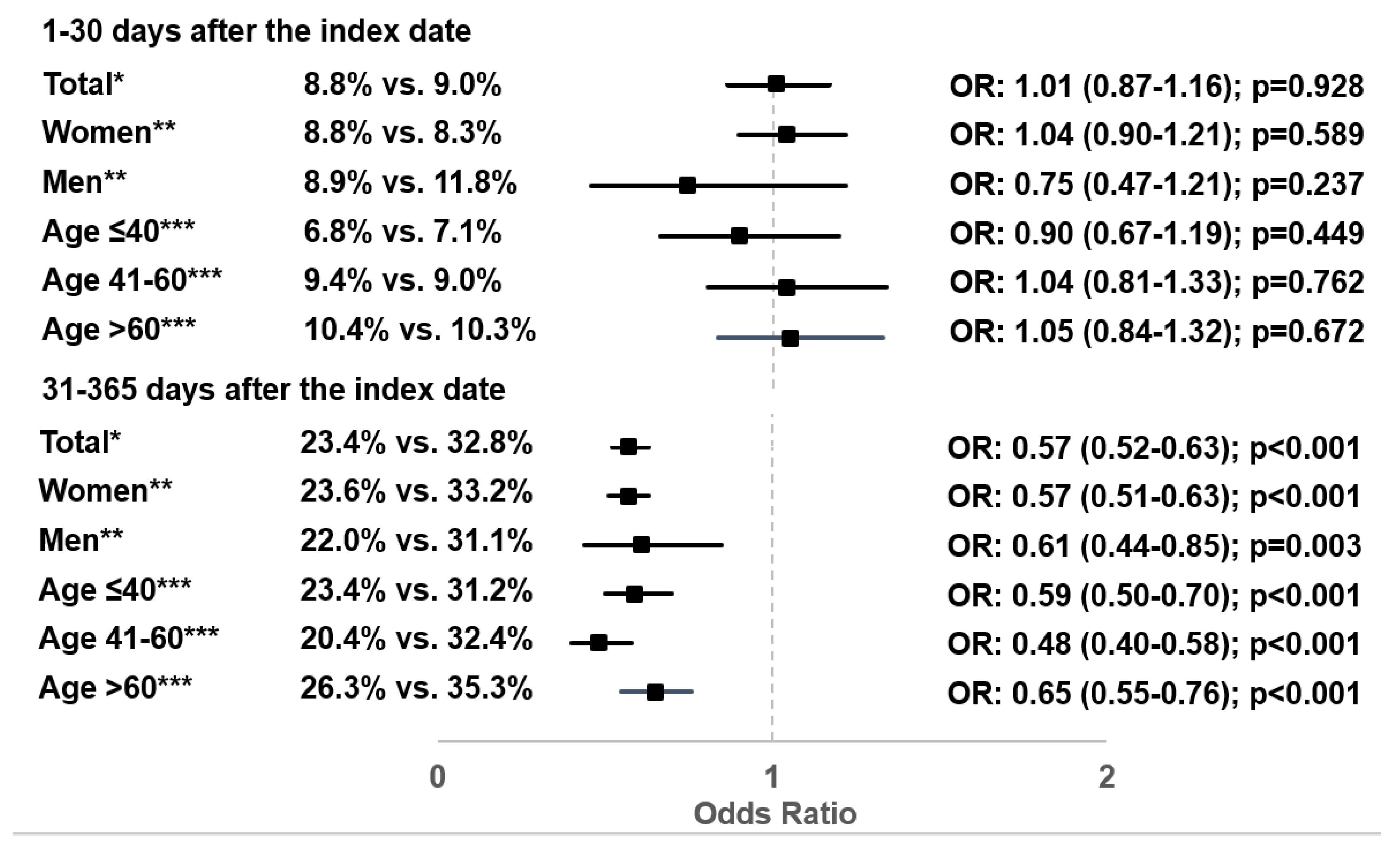
3.5. Additional Antibiotic Prescriptions after the Index Date
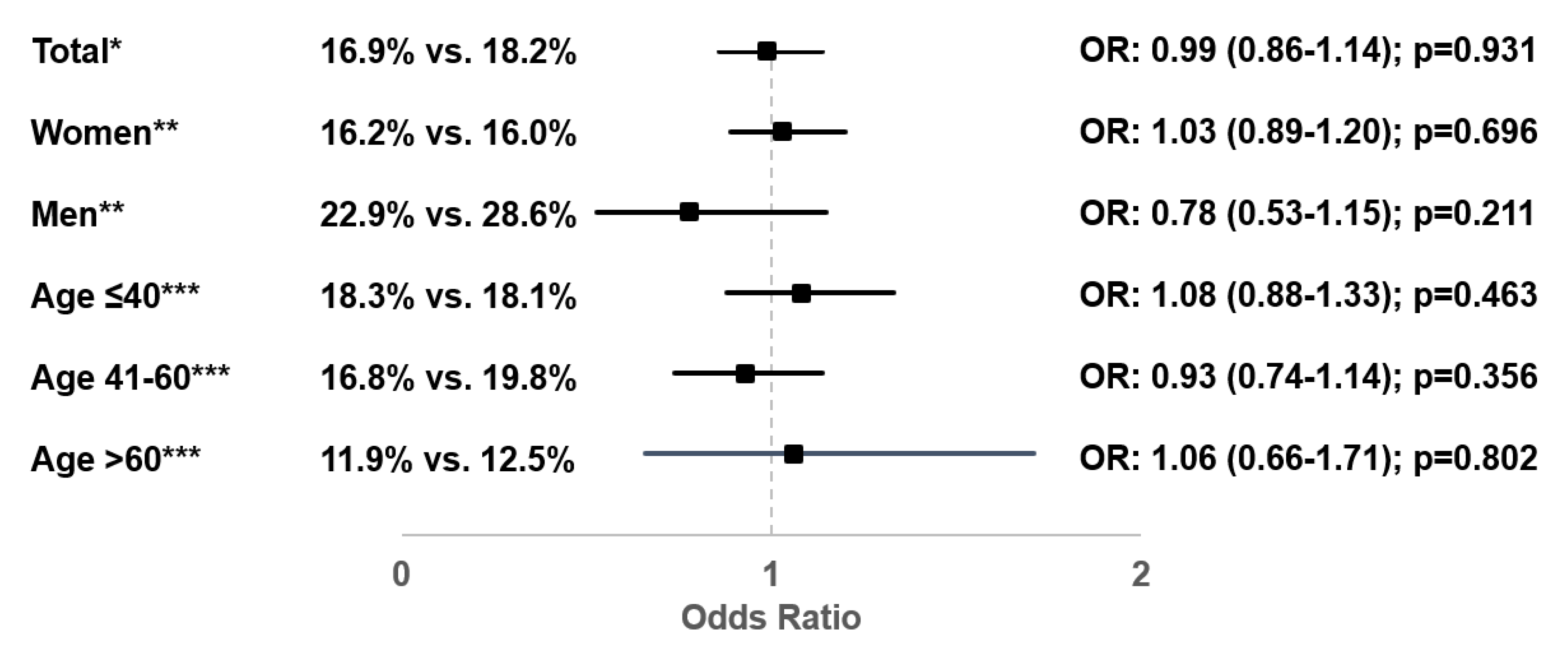
3.6. Incidence of Pyelonephritis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Schmiemann, G.; Kniehl, E.; Gebhardt, K.; Matejczyk, M.M.; Hummers, E. The Diagnosis of Urinary Tract Infection. Dtsch. Aerzteblatt Online 2010, 107, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am. J. Med. 2002, 113, 5–13. [Google Scholar] [CrossRef]
- Colgan, R.; Williams, M. Diagnosis and treatment of acute uncomplicated cystitis. Am. Fam. Physician 2011, 84, 771–776. [Google Scholar]
- Bonkat, G.; Bartoletti, R.; Bruyère, F.; Cai, T.; Geerlings, S.E.; Köves, B.; Schubert, S.; Wagenlehner, F.; Mezei, T.; Pilatz, A.; et al. European Association of Urology Guidelines on Urological Infections; EAU Guidelines Office: Arnhem, The Netherlands, 2020; ISBN 978-94-92671-07-3. Available online: https://uroweb.org/guideline/urological-infections/ (accessed on 4 January 2021).
- Kranz, J.; Schmidt, S.; Lebert, C.; Schneidewind, L.; Mandraka, F.; Kunze, M.; Helbig, S.; Vahlensieck, W.; Naber, K.; Schmiemann, G.; et al. The 2017 Update of the German Clinical Guideline on Epidemiology, Diagnostics, Therapy, Prevention, and Management of Uncomplicated Urinary Tract Infections in Adult Patients. Part II: Therapy and Prevention. Urol. Int. 2018, 100, 271–278. [Google Scholar] [CrossRef]
- Christiaens, T.C.M.; De Meyere, M.; Verschraegen, G.; Peersman, W.; Heytens, S.; De Maeseneer, J.M. Randomised controlled trial of nitrofurantoin versus placebo in the treatment of uncomplicated urinary tract infection in adult women. Br. J. Gen. Pract. 2002, 52, 729–734. [Google Scholar] [PubMed]
- Gágyor, I.; Bleidorn, J.; Kochen, M.M.; Schmiemann, G.; Wegscheider, K.; Hummers-Pradier, E. Ibuprofen versus fosfomycin for uncomplicated urinary tract infection in women: Randomised controlled trial. BMJ 2015, 351, h6544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleidorn, J.; Hummers-Pradier, E.; Schmiemann, G.; Wiese, B.; Gágyor, I. Recurrent urinary tract infections and complications after symptomatic versus antibiotic treatment: Follow-up of a randomised controlled trial. Ger. Med. Sci. 2016, 14. [Google Scholar] [CrossRef]
- Kronenberg, A.; Bütikofer, L.; Odutayo, A.; Mühlemann, K.; Da Costa, B.R.; Battaglia, M.; Meli, D.N.; Frey, P.; Limacher, A.; Reichenbach, S.; et al. Symptomatic treatment of uncomplicated lower urinary tract infections in the ambulatory setting: Randomised, double blind trial. BMJ 2017, 359, j4784. [Google Scholar] [CrossRef] [Green Version]
- Stange, R.; Schneider, B.; Albrecht, U.; Mueller, V.; Schnitker, J.; Michalsen, A. Results of a randomized, prospective, double-dummy, double-blind trial to compare efficacy and safety of a herbal combination containing Tropaeoli majoris herba and Armoraciae rusticanae radix with co-trimoxazole in patients with acute and uncomplicated cystitis. Res. Rep. Urol. 2017, 9, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Wawrysiuk, S.; Naber, K.; Rechberger, T.; Miotla, P. Prevention and treatment of uncomplicated lower urinary tract infections in the era of increasing antimicrobial resistance—non-antibiotic approaches: A systemic review. Arch. Gynecol. Obstet. 2019, 300, 821–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naber, K.G. Efficacy and safety of the phytotherapeutic drug Canephron® N in prevention and treatment of urogenital and gestational disease: Review of clinical experience in Eastern Europe and Central Asia. Res. Rep. Urol. 2013, 5, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Brenneis, C.; Künstle, G.; Haunschild, J. Spasmolytic activity of Canephron N on the contractility of rat and human isolated urinary bladder. In Proceedings of the 13th Congress of the International Society for Ethnopharmacology, Graz, Austria, 2–6 September 2012. [Google Scholar]
- Haloui, M.; Louedec, L.; Michel, J.-B.; Lyoussi, B. Experimental diuretic effects of Rosmarinus officinalis and Centaurium erythraea. J. Ethnopharmacol. 2000, 71, 465–472. [Google Scholar] [CrossRef]
- Nausch, B.; Künstle, G.; Mönch, B.; Koeberle, A.; Werz, O.; Haunschild, J. Canephron® N alleviates pain in experimental cystitis and inhibits reactive oxygen/nitrogen species as well as microsomal prostaglandin E2 synthase-1. Der Urol. 2015, 54, 28. [Google Scholar]
- Künstle, G.; Brenneis, C.; Haunschild, J. 671 Efficacy of Canephron® N against bacterial adhesion, inflammation and bladder hyperactivity. Eur. Urol. Suppl. 2013, 12, e671. [Google Scholar] [CrossRef]
- Nausch, B.; Pace, S.; Pein, H.; Koeberle, A.; Rossi, A.; Künstle, G.; Werz, O. The standardized herbal combination BNO 2103 contained in Canephron® N alleviates inflammatory pain in experimental cystitis and prostatitis. Phytomedicine 2019, 60, 152987. [Google Scholar] [CrossRef]
- Davidov, M.I.; Bunova, N.E. Comparative assessment of Canephron® N and ciprofloxacin as monotherapy of acute uncom-plicated cystitis in women. Urologiia 2018, 4, 24–32. [Google Scholar] [CrossRef]
- Davidov, M.I.; Voitko, D.A.; Bunova, N.E. Treatment of acute uncomplicated cystitis in women with antibiotic allergy or intol-erance. Urologiia 2019, 5, 64–71. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Abramov-Sommariva, D.; Höller, M.; Steindl, H.; Naber, K.G. Non-Antibiotic Herbal Therapy (BNO 1045) versus Antibiotic Therapy (Fosfomycin Trometamol) for the Treatment of Acute Lower Uncomplicated Urinary Tract Infections in Women: A Double-Blind, Parallel-Group, Randomized, Multicentre, Non-Inferiority Phase III Trial. Urol. Int. 2018, 101, 327–336. [Google Scholar] [CrossRef]
- Haynes, B. Can it work? Does it work? Is it worth it? The testing of healthcare interventions is evolving. BMJ 1999, 319, 652–653. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.-J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding al-gorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Amdii, R.E.; Al-Shukri, S.K.; Kuzmin, I.V.; Sorokin, N.V.; Chaplitskiy, E.A.; Skvortsov, M.V.; Alekseev, A.S.; Okunchaev, A.S.; Turbin, A.A.; Timaeva, G.R.; et al. Use of Canephron N in treatment of acute uncomplicated cystitis in women. Urologicheskie Vedomosti 2016, 6, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Sabadash, M.; Shulyak, A. Canephron® N in the treatment of recurrent cystitis in women of child-bearing Age: A randomised controlled study. Clin. Phytoscience 2017, 3, 9. [Google Scholar] [CrossRef]
- Serov, V.N.; Baranov, I.I.; Protopopova, N.V.; Tkachenko, L.V.; Kukarskaya, I.I. Evaluation of experience with a combination phy-totherapeutic drug in pregnant women (a multicen-ter retrospective observational study). Obstet. Gynecol. 2013, 9, 105–112. [Google Scholar]
- Dudar, I.O.; Loboda, O.M.; Krot, V.F.; Khimich, V.I.; Kryzhanivska, V.M.; Bryzhachenko, T.P. A 12-month comparative study of Canephron® N administration in the treatment of pa-tients with the urinary tract infection. Zdorovie Muzhchiny 2010, 3, 85–90. [Google Scholar]
- Ordzhonikidze, N.V.; Yemelyanova, A.I.; Petrova, S.B. Complication pre-vention and treatment in pregnants and puerperants with urinary tract diseases. Obstet. Gynaecol. 2009, 6, 41–45. [Google Scholar]
- Perepanova, T.S.; Khazan, P.L. Phytopreparation Canephron® N in the treatment and prophylaxis of urinary tract infections. Vrachebnoye Soslovie 2005, 5, 44–46. [Google Scholar]
- Ivanov, D.; Abramov-Sommariva, D.; Moritz, K.; Eskötter, H.; Kostinenko, T.; Martynyuk, L.; Kolesnik, N.; Naber, K.G. An open label, non-controlled, multicentre, interventional trial to investigate the safety and efficacy of Canephron® N in the management of uncomplicated urinary tract infections (uUTIs). Clin. Phytoscience 2015, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Naber, K.G.; Kogan, M.; Wagenlehner, F.M.E.; Siener, R.; Gessner, A. How the microbiome is influenced by the therapy of urological diseases: Standard versus alternative approaches. Clin. Phytoscience 2017, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Cai, T.; Verze, P.; Palmieri, A.; Gacci, M.; Lanzafame, P.; Malossini, G.; Nesi, G.; Bonkat, G.; Wagenlehner, F.M.; Mirone, V.; et al. Is Preoperative Assessment and Treatment of Asymptomatic Bacteriuria Necessary for Reducing the Risk of Postoperative Symptomatic Urinary Tract Infections After Urologic Surgical Procedures? Urology 2017, 99, 100–105. [Google Scholar] [CrossRef]
- Wullt, B.; Svanborg, C. Deliberate Establishment of Asymptomatic Bacteriuria—A Novel Strategy to Prevent Recurrent UTI. Pathogens 2016, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.; Konrad, M.; Adarkwah, C.C.; Kostev, K. Reduced antibiotic use after initial treatment of acute respiratory infections with phytopharmaceuticals- a retrospective cohort study. Postgrad. Med. 2020, 132, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with Canephron® Prescription | Patients with Antibiotic Prescription | p-Value |
|---|---|---|---|
| N | 2320 | 158,592 | |
| Age (mean, SD) | 51.3 (19.9) | 55.0 (20.8) | <0.001 |
| ≤40 years (%) | 33.2 | 29.5 | <0.001 |
| 41–60 years (%) | 32.3 | 28.6 | |
| >60 years (%) | 34.5 | 41.9 | |
| Sex: female (%) | 81.2 | 90.8 | <0.001 |
| CCI (mean, SD) | 1.6 (2.3) | 1.7 (2.4) | 0.019 |
| Private health insurance coverage (%) | 11.3 | 7.6 | <0.001 |
| Therapy by general practitioners | 90.0 | 80.7 | <0.001 |
| Therapy by gynecologists | 7.1 | 14.1 | |
| Therapy by urologists | 2.9 | 5.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höller, M.; Steindl, H.; Abramov-Sommariva, D.; Wagenlehner, F.; Naber, K.G.; Kostev, K. Treatment of Urinary Tract Infections with Canephron® in Germany: A Retrospective Database Analysis. Antibiotics 2021, 10, 685. https://doi.org/10.3390/antibiotics10060685
Höller M, Steindl H, Abramov-Sommariva D, Wagenlehner F, Naber KG, Kostev K. Treatment of Urinary Tract Infections with Canephron® in Germany: A Retrospective Database Analysis. Antibiotics. 2021; 10(6):685. https://doi.org/10.3390/antibiotics10060685
Chicago/Turabian StyleHöller, Martina, Hubert Steindl, Dimitri Abramov-Sommariva, Florian Wagenlehner, Kurt G. Naber, and Karel Kostev. 2021. "Treatment of Urinary Tract Infections with Canephron® in Germany: A Retrospective Database Analysis" Antibiotics 10, no. 6: 685. https://doi.org/10.3390/antibiotics10060685