
Telomere Shortening and Accelerated Aging in US Military Veterans


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Descriptive Analysis
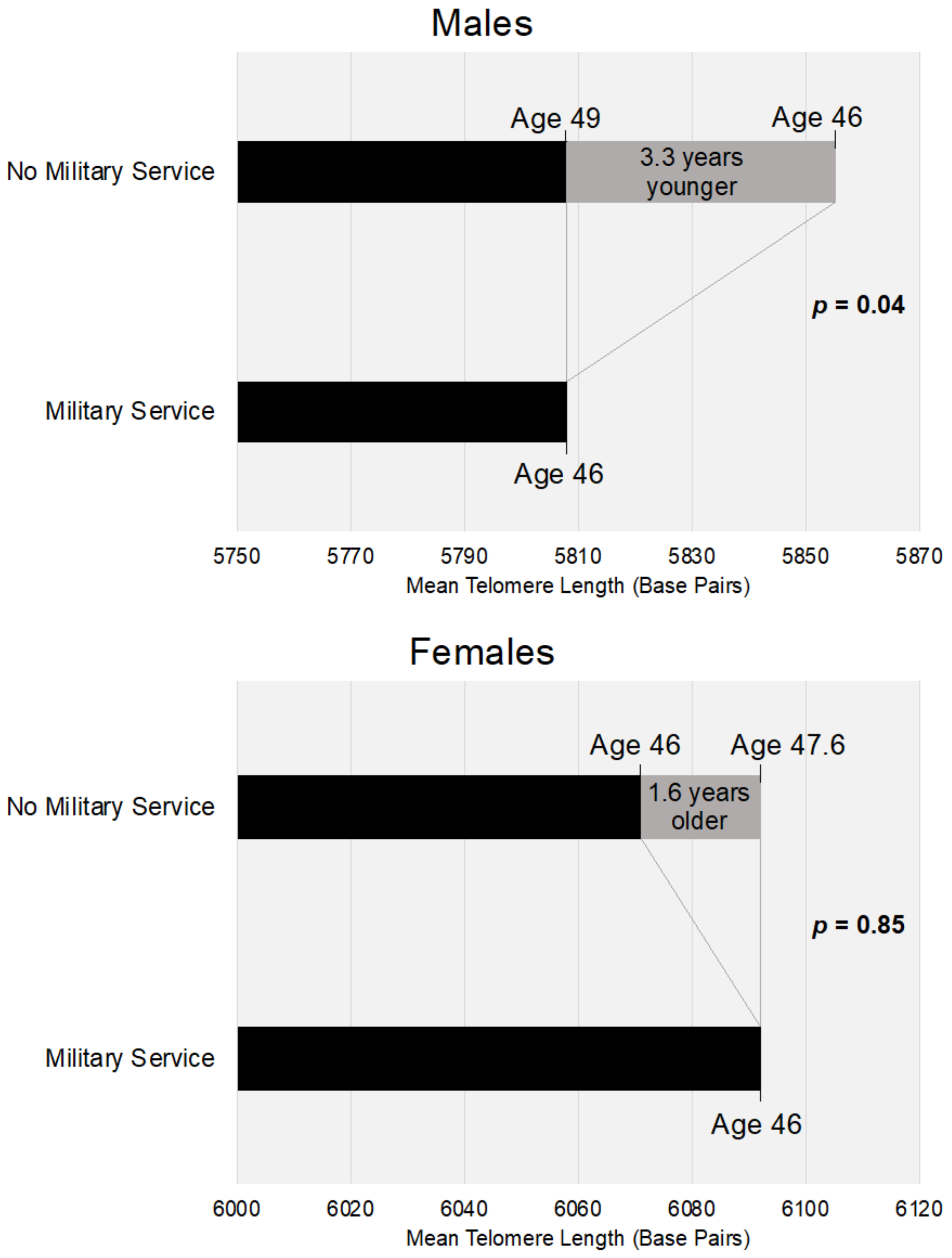
3.2. Multivariate Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclaimer
References
- Heron, M. Deaths: Leading Causes for 2017. Natl. Vital Stat. Rep. 2019, 68, 1–77. [Google Scholar]
- Boos, C.J.; De Villiers, N.; Dyball, D.; McConnell, A.; Bennett, A.N. The Relationship between Military Combat and Cardiovascular Risk: A Systematic Review and Meta-Analysis. Int. J. Vasc. Med. 2019, 2019, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Crum-Cianflone, N.F.; Bagnell, M.E.; Schaller, E.; Boyko, E.J.; Smith, B.; Maynard, C.; Ulmer, C.S.; Vernalis, M.; Smith, T.C. Impact of Combat Deployment and Posttraumatic Stress Disorder on Newly Reported Coronary Heart Disease Among US Active Duty and Reserve Forces. Circulation 2014, 129, 1813–1820. [Google Scholar] [CrossRef] [Green Version]
- Howard, J.T.; Stewart, I.J.; Kolaja, C.A.; Sosnov, J.A.; Rull, R.P.; Torres, I.; Janak, J.C.; Walker, L.E.; Trone, D.W.; Armenta, R.F. Hypertension in military veterans is associated with combat exposure and combat injury. J. Hypertens. 2020, 38, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.T.; Sosnov, J.A.; Janak, J.C.; Gundlapalli, A.V.; Pettey, W.B.; Walker, L.E.; Stewart, I.J. Associations of Initial Injury Severity and Posttraumatic Stress Disorder Diagnoses with Long-Term Hypertension Risk After Combat Injury. Hypertension 2018, 71, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Stewart, I.; Sosnov, J.; Howard, J.; Orman, J.; Fang, R.; Morrow, B.; Zonies, D.; Bollinger, M.; Tuman, C.; Freedman, B.; et al. Retrospective Analysis of Long-Term Outcomes After Combat Injury: A Hidden Cost of War. Circulation 2015, 132, 2126–2133. [Google Scholar] [CrossRef] [PubMed]
- Walker, L.E.; Poltavskiy, E.; Janak, J.C.; Beyer, C.A.; Stewart, I.J.; Howard, J.T. US Military Service and Racial/Ethnic Differences in Cardiovascular Disease: An Analysis of the 2011–2016 Behavioral Risk Factor Surveillance System. Ethn. Dis. 2019, 29, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, J.; Turner, B.; Stotts, N.; Dracup, K. Health-Related Coping Behaviors and Mental Health in Military Personnel. Mil. Med. 2017, 182, e1620–e1627. [Google Scholar] [CrossRef] [Green Version]
- Stewart, I.; Sosnov, J.; Snow, B.; Batou, A.; Howard, J.; Janak, J.; Bollinger, M.; Chung, K. Hypertension after injury among burned combat veterans: A retrospective cohort study. Burns 2016, 43, 290–296. [Google Scholar] [CrossRef]
- Cohen, B.; Marmar, C.; Neylan, T.; Schiller, N.; Sadia, A. Posttraumatic Stress Disorder and Health-Related Quality of Life in Patients with Coronary Heart Disease: Findings from the Heart and Soul Study. JAMA Psychiatry 2009, 66, 1214–1220. [Google Scholar] [CrossRef]
- Cohen, B.; Marmar, C.; Ren, L. Association of Cardiovascular Risk Factors with Mental Health Diagnoses in Iraq and Afghanistan War Veterans Using VA Health Care. JAMA 2009, 302, 489–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandweiss, D.A.; Slymen, N.J.; LeardMann, C.A.; White, M.R.; Hooper, T.I.; Gackstetter, G.D.; Smith, B.; Boyko, E.J.; Amoroso, P.J.; Smith, T.C. Preinjury Psychiatric Status, Injury Severity, and Postdeployment Posttraumatic Stress Disorder. Arch. Gen. Psychiatry 2011, 68, 496–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, D.L.; Zeber, J.E. Mental Health Outcomes Among Military Service Members After Severe Injury in Combat and TBI. Mil. Med. 2019, 185, e711–e718. [Google Scholar] [CrossRef] [Green Version]
- Vance, M.C.; Wiitala, W.L.; Sussman, J.B.; Pfeiffer, P.; Hayward, R.A. Increased Cardiovascular Disease Risk in Veterans with Mental Illness. Circ. Cardiovasc. Qual. Outcomes 2019, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sidney, S.; Quesenberry, C.P.; Jaffe, M.G.; Sorel, M.; Nguyen-Huynh, M.N.; Kushi, L.H.; Go, A.S.; Rana, J.S. Recent Trends in Cardiovascular Mortality in the United States and Public Health Goals. JAMA Cardiol. 2016, 1, 594–599. [Google Scholar] [CrossRef] [Green Version]
- Tajeu, G.S.; Safford, M.M.; Howard, G.; Howard, V.J.; Chen, L.; Long, D.L.; Tanner, R.M.; Muntner, P. Black–White Differences in Cardiovascular Disease Mortality: A Prospective US Study, 2003–2017. Am. J. Public Health 2020, 110, 696–703. [Google Scholar] [CrossRef]
- Blackburn, E.H.; Epel, E.S.; Lin, J. Human telomere biology: A contributory and interactive factor in aging, disease risks, and protection. Science 2015, 350, 1193–1198. [Google Scholar] [CrossRef] [Green Version]
- Aubert, G.; Lansdorp, P.M. Telomeres and Aging. Physiol. Rev. 2008, 88, 557–579. [Google Scholar] [CrossRef]
- Kotrschal, A.; Ilmonen, P.; Penn, D.J. Stress impacts telomere dynamics. Biol. Lett. 2007, 3, 128–130. [Google Scholar] [CrossRef]
- Epel, E.S.; Blackburn, E.H.; Lin, J.; Dhabhar, F.S.; Adler, N.E.; Morrow, J.D.; Cawthon, R.M. Accelerated telomere shortening in response to life stress. Proc. Natl. Acad. Sci. USA 2004, 101, 17312–17315. [Google Scholar] [CrossRef] [Green Version]
- Mathur, M.; Epel, E.; Kind, S.; Desai, M.; Parks, C.; Sandler, D.; Khazeni, N. Perceived stress and telomere length: A systematic review, meta-analysis, and methodologic considerations for advancing the field. Brain Behav. Immun. 2016, 54, 158–169. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, A.; Pantell, M.S.; Puterman, E.; Dhabhar, F.S.; Blackburn, E.H.; Yaffe, K.; Cawthon, R.M.; Opresko, P.L.; Hsueh, W.-C.; Satterfield, S.; et al. Cumulative Inflammatory Load Is Associated with Short Leukocyte Telomere Length in the Health, Aging and Body Composition Study. PLoS ONE 2011, 6, e19687. [Google Scholar] [CrossRef] [Green Version]
- Wolkowitz, O.M.; Mellon, S.H.; Epel, E.S.; Lin, J.; Dhabhar, F.S.; Su, Y.; Reus, V.I.; Rosser, R.; Burke, H.M.; Kupferman, E.; et al. Leukocyte Telomere Length in Major Depression: Correlations with Chronicity, Inflammation and Oxidative Stress—Preliminary Findings. PLoS ONE 2011, 6, e17837. [Google Scholar] [CrossRef] [Green Version]
- D’Mello, M.J.; Ross, S.A.; Briel, M.; Anand, S.S.; Gerstein, H.; Paré, G. Association Between Shortened Leukocyte Telomere Length and Cardiometabolic Outcomes. Circ. Cardiovasc. Genet. 2015, 8, 82–90. [Google Scholar] [CrossRef]
- Haycock, P.C.; E Heydon, E.; Kaptoge, S.; Butterworth, A.S.; Thompson, A.; Willeit, P. Leucocyte telomere length and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2014, 349, g4227. [Google Scholar] [CrossRef] [Green Version]
- Hunt, S.; Chen, W.; Gardner, J.; Kimura, M.; Srinivasan, S.; Eckfeldt, J.; Berenson, G.; Aviv, A. Leukocyte telomeres are longer in African Americans than in whites: The national heart, lung, and blood institute family heart study and the bogalusa heart study. Aging Cell 2008, 7, 451–458. [Google Scholar] [CrossRef]
- Elbers, C.C.; Garcia, M.E.; Kimura, M.; Cummings, S.R.; Nalls, M.A.; Newman, A.B.; Park, V.; Sanders, J.L.; Tranah, G.J.; Tishkoff, S.A.; et al. Comparison Between Southern Blots and qPCR Analysis of Leukocyte Telomere Length in the Health ABC Study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 69, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.E.; Hunt, S.C.; Stone, R.C.; Horvath, K.; Herbig, U.; Ranciaro, A.; Hirbo, J.; Beggs, W.; Reiner, A.P.; Wilson, J.G.; et al. Shorter telomere length in Europeans than in Africans due to polygenetic adaptation. Hum. Mol. Genet. 2016, 25, 2324–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuda, K.; Bardeguez, A.; Gardner, J.P.; Rodriguez, P.; Ganesh, V.; Kimura, M.; Skurnick, J.; Awad, G.; Aviv, A. Telomere Length in the Newborn. Pediatr. Res. 2002, 52, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Watkins, L.E.; Harpaz-Rotem, I.; Sippel, L.M.; Krystal, J.H.; Southwick, S.M.; Pietrzak, R.H. Hostility and telomere shortening among U.S. military veterans: Results from the National Health and Resilience in Veterans Study. Psychoneuroendocrinology 2016, 74, 251–257. [Google Scholar] [CrossRef]
- Jergović, M.; Tomičević, M.; Vidović, A.; Bendelja, K.; Savić, A.; Vojvoda, V.; Rac, D.; Lovrić-Čavar, D.; Rabatić, S.; Jovanovic, T.; et al. Telomere shortening and immune activity in war veterans with posttraumatic stress disorder. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2014, 54, 275–283. [Google Scholar] [CrossRef]
- Kang, J.I.; Mueller, S.G.; Wu, G.W.; Lin, J.; Ng, P.; Yehuda, R.; Flory, J.D.; Abu-Amara, D.; Reus, V.I.; Gautam, A.; et al. Effect of Combat Exposure and Posttraumatic Stress Disorder on Telomere Length and Amygdala Volume. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2020, 5, 678–687. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, X.-Z.; Russell, D.W.; Benedek, D.M.; Fullerton, C.S.; Naifeh, J.A.; Li, X.; Chen, Z.; Wu, H.; Ng, T.H.H.; et al. Association between leukocyte telomere length and hostility in US army service members. Neurosci. Lett. 2019, 706, 24–29. [Google Scholar] [CrossRef]
- Cawthon, R.M. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002, 30, e47–e52. [Google Scholar] [CrossRef]
- Needham, B.L.; Roux, A.V.D.; Bird, C.E.; Bradley, R.; Fitzpatrick, A.L.; Jacobs, D.R.; Ouyang, P.; Seeman, T.E.; Thurston, R.C.; Vaidya, D.; et al. A Test of Biological and Behavioral Explanations for Gender Differences in Telomere Length: The Multi-Ethnic Study of Atherosclerosis. Biodemogr. Soc. Biol. 2014, 60, 156–173. [Google Scholar] [CrossRef] [Green Version]
- National Center for Health Statistics National Health and Nutrition Examination Survey, 1999–2000 Data Documentation, Code-book, and Frequencies: Analytic Notes; Hyattsville, MD. 2015. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/1999-2000/TELO_A.htm#Analytic_Notes (accessed on 25 October 2020).
- Wilson, L.C. The Prevalence of Military Sexual Trauma: A Meta-Analysis. Trauma Violence Abus. 2018, 19, 584–597. [Google Scholar] [CrossRef]
- Hawksworth, J.S.; Stojadinovic, A.; Gage, F.A.; Tadaki, D.K.; Perdue, P.W.; Forsberg, J.; Davis, T.A.; Dunne, J.R.; Denobile, J.W.; Brown, T.S.; et al. Inflammatory Biomarkers in Combat Wound Healing. Ann. Surg. 2009, 250, 1002–1007. [Google Scholar] [CrossRef]
- Devoto, C.; Arcurio, L.; Fetta, J.; Ley, M.; Rodney, T.; Kanefsky, R.; Gill, J. Inflammation Relates to Chronic Behavioral and Neurological Symptoms in Military Personnel with Traumatic Brain Injuries. Cell Transplant. 2017, 26, 1169–1177. [Google Scholar] [CrossRef]
- Jackowska, M.; Hamer, M.; Carvalho, L.A.; Erusalimsky, J.D.; Butcher, L.; Steptoe, A. Short Sleep Duration Is Associated with Shorter Telomere Length in Healthy Men: Findings from the Whitehall II Cohort Study. PLoS ONE 2012, 7, e47292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lung, F.-W.; Ku, C.-S.; Kao, W.-T. Telomere length may be associated with hypertension. J. Hum. Hypertens. 2007, 22, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.G.; Ives, S.J.; Walker, A.E.; Cawthon, R.M.; Andtbacka, R.H.; Noyes, D.; Lesniewski, L.A.; Richardson, R.S.; Donato, A.J. Role of arterial telomere dysfunction in hypertension. J. Hypertens. 2014, 32, 1293–1299. [Google Scholar] [CrossRef] [Green Version]
- White, R.F.; Steele, L.; O’Callaghan, J.P.; Sullivan, K.; Binns, J.H.; Golomb, B.A.; Bloom, F.E.; Bunker, J.A.; Crawford, F.; Graves, J.C.; et al. Recent research on Gulf War illness and other health problems in veterans of the 1991 Gulf War: Effects of toxicant exposures during deployment. Cortex 2016, 74, 449–475. [Google Scholar] [CrossRef] [Green Version]
- Richards, E.E. Responses to Occupational and Environmental Exposures in the U.S. Military—World War II to the Present. Mil. Med. 2011, 176, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rode, L.; Bojesen, S.; Weischer, M.; Vestbo, J.; Nordestgaard, B. Short telomere length, lung function and chronic obstructive pulmonary disease in 46,396 individuals. Thorax 2013, 68, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanei, B.; Reza, J.Z.; Momtaz, M.; Azimi, M.; Sakhvidi, M.J.Z. Occupational exposure to particulate matters and telomere length. Environ. Sci. Pollut. Res. 2018, 25, 36298–36305. [Google Scholar] [CrossRef] [PubMed]
- Senthilkumar, P.; Klingelhutz, A.; Jacobus, J.; Lehmler, H.; Robertson, L.; Ludewig, G. Airborne polychlorinated biphenyls (PCBs) reduce telomerase activity and shorten telomere length in immortal human skin keratinocytes (HaCat). Toxicol. Lett. 2011, 204, 64–70. [Google Scholar] [CrossRef] [Green Version]
- De Felice, B.; Nappi, C.; Zizolfi, B.; Guida, M.; Sardo, A.D.S.; Bifulco, G.; Guida, M. Telomere shortening in women resident close to waste landfill sites. Gene 2012, 500, 101–106. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Litz, B.T.; Weathers, F.W. Social anxiety, depression, and PTSD in Vietnam veterans. J. Anxiety Disord. 2003, 17, 573–582. [Google Scholar] [CrossRef]
- Stellman, J.M.; Stellman, S.D. Agent Orange During the Vietnam War: The Lingering Issue of Its Civilian and Military Health Impact. Am. J. Public Health 2018, 108, 726–728. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.-W.; Hong, J.-S.; Ohrr, H.; Yi, J.-J. Agent Orange exposure and disease prevalence in Korean Vietnam veterans: The Korean veterans health study. Environ. Res. 2014, 133, 56–65. [Google Scholar] [CrossRef]
- Wolf, E.J.; Logue, M.W.; Hayes, J.P.; Sadeh, N.; Schichman, S.A.; Stone, A.; Salat, D.H.; Milberg, W.P.; McGlinchey, R.E.; Miller, M.W. Accelerated DNA methylation age: Associations with PTSD and neural integrity. Psychoneuroendocrinology 2016, 63, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, E.J.; Morrison, F.G. Traumatic Stress and Accelerated Cellular Aging: From Epigenetics to Cardiometabolic Disease. Curr. Psychiatry Rep. 2017, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total Sample | Prior Military Service | No Prior Military Service | p Value * |
|---|---|---|---|---|
| Telomere length base pairs, mean (SE) | 5821.7 (35.4) | 5630.0 (30.0) | 5855.8 (37.6) | <0.001 |
| Age in years, mean (SE) | 46.1 (0.4) | 55.8 (0.6) | 44.4 (0.4) | <0.001 |
| Male Sex, percent (SE) | 48.6 (0.5) | 94.4 (0.8) | 40.5 (0.7) | <0.001 |
| Race/Ethnicity, percent (SE) | <0.001 | |||
| Non-Hispanic White | 72.9 (1.8) | 84.8 (1.5) | 70.8 (2.0) | |
| Non-Hispanic Black | 9.3 (1.1) | 8.2 (0.9) | 9.5 (1.1) | |
| Mexican American | 7.0 (0.9) | 2.2 (0.4) | 7.8 (1.0) | |
| Other Hispanic | 6.8 (1.6) | 3.3 (1.1) | 7.4 (1.8) | |
| Other | 4.0 (0.6) | 1.4 (0.4) | 4.5 (0.7) | |
| Education, percent (SE) | <0.001 | |||
| Less than High School | 21.4 (0.9) | 14.7 (1.2) | 22.6 (0.9) | |
| High School Graduate or Equivalent | 26.0 (1.0) | 28.3 (2.1) | 25.6 (1.0) | |
| Some College | 28.4 (0.9) | 28.6 (1.9) | 28.3 (1.0) | |
| College Degree or More | 24.1 (1.6) | 28.3 (2.1) | 23.4 (1.6) | |
| Missing | 0.1 (0.0) | 0.0 (0.0) | 0.1 (0.1) | |
| Marital Status | <0.001 | |||
| Never Married | 15.7 (0.8) | 8.6 (1.1) | 17.0 (0.9) | |
| Married | 56.4 (1.4) | 69.1 (2.1) | 54.2 (1.4) | |
| Live with Partner | 5.3 (0.6) | 3.3 (0.4) | 5.7 (0.7) | |
| Widowed | 5.9 (0.4) | 4.1 (0.6) | 6.3 (0.4) | |
| Separated | 2.7 (0.2) | 1.4 (0.4) | 3.0 (0.3) | |
| Divorced | 8.5 (0.5) | 8.2 (1.5) | 8.5 (0.5) | |
| Missing | 5.4 (1.6) | 5.4 (1.6) | 5.4 (1.7) | |
| Income to Poverty Ratio | <0.001 | |||
| At or Below Poverty | 13.1 (0.9) | 5.8 (0.9) | 14.4 (0.9) | |
| 1.0 to 2.0 Times Poverty | 18.9 (1.2) | 15.9 (1.6) | 19.4 (1.2) | |
| 2.01 to 3.0 Times Poverty | 14.4 (0.6) | 15.7 (1.3) | 14.1 (0.6) | |
| 3.01 to 4.0 Times Poverty | 12.7 (0.6) | 13.8 (1.1) | 12.5 (0.7) | |
| More than 4.0 Times Poverty | 33.3 (1.6) | 41.7 (2.0) | 31.8 (1.6) | |
| Missing | 7.6 (0.8) | 7.0 (1.1) | 7.8 (0.9) | |
| Telomere length base pairs, mean (SE) | 5821.7 (35.4) | 5630.0 (30.0) | 5855.8 (37.6) | <0.001 |
| Variables | Total Sample (n = 7820) | Prior Military Service (n = 1225) | No Prior Military Service (n = 6595) | p Value * |
|---|---|---|---|---|
| Smoking Status, percent (SE) | <0.001 | |||
| Current Smoker | 24.4 (0.9) | 23.8 (1.5) | 24.5 (1.1) | |
| Former Smoker | 25.5 (0.9) | 42.8 (1.5) | 22.4 (0.9) | |
| Never Smoker | 50.0 (1.3) | 33.4 (1.4) | 52.9 (1.3) | |
| Missing | 0.1 (0.04) | 0.03 (0.03) | 0.1 (0.05) | |
| Alcohol Consumption, percent (SE) | <0.001 | |||
| Lifetime Abstainer | 12.2 (1.6) | 4.5 (0.8) | 13.5 (1.8) | |
| Former Drinkers | 16.3 (0.8) | 23.7 (1.5) | 15.0 (0.9) | |
| Light Drinkers (no binge drinking) | 30.5 (1.0) | 26.3 (1.9) | 31.3 (1.2) | |
| Moderate Drinkers (no binge drinking) | 2.8 (0.3) | 2.9 (0.6) | 2.8 (0.3) | |
| Frequent Drinkers (no binge drinking) | 5.8 (0.5) | 9.6 (1.2) | 11.6 (0.6) | |
| Infrequent Binge Drinker | 15.4 (0.7) | 16.3 (1.4) | 15.3 (0.7) | |
| Frequent Binge Drinker | 11.9 (0.5) | 13.7 (1.1) | 11.6 (0.6) | |
| Missing | 5.1 (0.4) | 3.0 (0.6) | 5.5 (0.5) | |
| Body Mass Index, percent (SE) | <0.001 | |||
| Underweight | 5.4 (0.3) | 1.9 (0.3) | 6.0 (0.3) | |
| Normal weight | 28.4 (0.9) | 22.8 (1.7) | 29.4 (1.0) | |
| Overweight | 34.1 (0.9) | 42.9 (2.1) | 32.5 (1.0) | |
| Obese | 29.6 (1.0) | 30.2 (1.3) | 29.5 (1.1) | |
| Missing | 2.5 (0.3) | 2.3 (0.5) | 2.5 (0.3) | |
| Physical Activity Level Quartiles, percent (SE) | ||||
| Quartile 1 | 14.9 (0.7) | 13.7 (1.1) | 15.1 (0.9) | 0.006 |
| Quartile 2 | 14.6 (0.7) | 13.1 (1.1) | 14.8 (0.7) | |
| Quartile 3 | 17.1 (0.8) | 17.8 (1.6) | 16.9 (0.9) | |
| Quartile 4 | 15.9 (1.0) | 20.9 (2.2) | 15.1 (0.9) | |
| Missing | 37.5 (1.3) | 34.5 (1.7) | 38.0 (1.4) |
| Variables | Total (n = 7820) Est (95% CI) | Males (n = 3766) Est (95% CI) | Females (n = 4054) Est (95% CI) |
|---|---|---|---|
| Intercept | 6555.5 (6343.1, 6767.8) *** | 6455.9 (6261.7, 6650.1) *** | 6606.8 (6356.1, 6857.5) *** |
| Military Service | |||
| Military vs. No Military (ref) | −43.7 (−90.1, 2.7) | −47.2 (−92.9, −1.5) * | 21.4 (−211.3, 254.0) |
| Age in years | −13.7 (−15.1, −12.2) *** | −14.4 (−16.1, −12.6) *** | −13.2 (−14.9, −11.4) *** |
| Sex, Males vs. Females (ref) | −30.6 (−62.6, 1.5) | n/a | n/a |
| Race/Ethnicity | |||
| Non-Hispanic White (ref) | |||
| Non-Hispanic Black | 114.2 (33.1, 195.3) ** | 63.8 (−18.0, 145.5) | 161.8 (61.9, 261.7) ** |
| Mexican American | −98.2 (−208.6, 12.2) | −93.2 (−208.9, 22.5) | −104.3 (−223.8, 15.2) |
| Other Hispanic | 94.7 (−112.1, 301.4) | 68.4 (−129.8, 266.6) | 119.2 (−106.3, 344.6) |
| Other | −38.9 (−151.0, 73.2) | −57.0 (−188.4, 74.4) | −25.6 (−163.3, 112.1) |
| Education | |||
| Less than High School (ref) | |||
| High School Graduate or Equivalent | 55.3 (0.5, 110.1) * | 41.2 (−24.5, 106.9) | 66.3 (−15.9, 148.4) |
| Some College | 67.1 (6.0, 128.2) * | 54.0 (−1.3, 109.4) | 84.0 (−27.8, 195.8) |
| College Degree or More | 97.8 (31.0, 164.6) ** | 113.2 (41.5, 184.9) ** | 81.5 (−28.3, 191.3) |
| Missing | −22.5 (−594.2, 549.3) | −359.7 (−650.8, −68.6)* | 147.7 (−738.7, 1034.1) |
| Marital Status | |||
| Never Married (ref) | |||
| Married | −81.6 (−129.8, −33.4) ** | −84.1 (−143.7, −24.5) ** | −76.4 (−153.4, 0.7) |
| Live with Partner | −44.9 (−96.8, 7.0) | −56.0 (−177.4, 65.5) | −187.3 (−308.0, −66.5) ** |
| Widowed | −114.5 (−209.2, −19.7) * | −110.0 (−238.6, 18.8) | −42.0 (−127.5, 43.4) |
| Separated | −119.8 (−199.9, −30.8) * | −123.3 (−275.8, 29.1) | −144.0 (−256.9, −31.0) * |
| Divorced | −126.4 (−222.3, −30.6) * | −147.6 (−253.8, −41.5) ** | −104.2 (−219.1, 10.7) |
| Missing | 153.9 (12.7, 295.0) * | 137.0 (−13.2, 287.3) | 165.4 (−38.9, 369.7) |
| Income to Poverty Ratio | |||
| At or Below Poverty (ref) | |||
| 1.0 to 2.0 Times Poverty | −83.1 (−190.1, 23.8) | −35.6 (−142.7, 71.4) | −115.2 (−243.5, 13.2) |
| 2.01 to 3.0 Times Poverty | −48.3 (−158.9, 62.3) | −11.3 (−154.0, 131.3) | −74.8 (−202.1, 52.5) |
| 3.01 to 4.0 Times Poverty | −32.9 (−163.6, 97.8) | 46.6 (−106.0, 199.1) | −100.9 (−232.2, 30.4) |
| >4.0 Times Poverty | −47.3 (−113.2, 142.3) | 21.1 (−96.7, 174.3) | −101.6 (−249.1, 46.0) |
| Missing | 14.5 (−113.2, 142.3) | 61.0 (−52.3, 174.3) | −18.7 (−187.0, 149.6) |
| Smoking Status | |||
| Never Smoker (ref) | |||
| Current Smoker | −4.3 (−44.3, 35.7) | 36.2 (−17.8, 90.3) | −43.5 (−108.4, 21.5) |
| Former Smoker | −34.0 (−82.0, 14.0) | −11.4 (−74.3, 51.4) | −50.7 (−114.4, 12.7) |
| Missing | 99.7 (−175.4, 374.7) | 271.3 (−130.8, 673.4) | 24.5 (−364.3, 413.3) |
| Alcohol Consumption, percent | |||
| Lifetime Abstainer | 41.6 (−40.6, 123.9) | 53.3 (−85.6, 192.2) | 20.4 (−67.3, 108.0) |
| Former Drinkers | −35.6 (−88.0, 16.7) | −10.2 (−107.9, 87.6) | −59.9 (−130.6, 10.8) |
| Light Drinkers (no binge drinking) (ref) | |||
| Moderate Drinkers (no binge drinking) | −39.6 (−99.3, 20.1) | 26.4 (−78.8, 131.4) | −108.1 (−235.4, 19.2) |
| Frequent Drinkers (no binge drinking) | 58.8 (4.9, 112.7) * | 59.1 (−43.9, 162.2) | 71.3 (1.7, 140.9) * |
| Infrequent Binge Drinker | 15.0 (−45.6, 75.6) | 17.1 (−80.3, 114.4) | 17.5 (−93.0, 128.1) |
| Frequent Binge Drinker | 14.4 (−41.4, 70.2) | 41.9 (−29.7, 113.5) | −54.9 (−180.2, 70.4) |
| Missing | 98.1 (16.8, 179.3) * | 154.9 (29.8, 280.1) * | 51.1 (−44.6, 146.9) |
| Body Mass Index | |||
| Normal weight (ref) | |||
| Underweight | −16.9 (−131.9, 98.1) | −30.6 (−165.1, 104.0) | 6.2 (−132.1, 144.4) |
| Overweight | −53.8 (−116.2, 8.6) | −52.8 (−127.9, 22.2) | −49.9 (−138.3, 18.5) |
| Obese | −77.9 (−132.7, −23.1) ** | −88.0 (−159.0, −17.1) * | −77.2 (−141.4, −12.9) * |
| Missing | −8.3 (−96.2, 79.7) | 154.9 (29.8, 280.1) * | 44.4 (−80.5, 169.3) |
| Physical Activity Level Quartiles | |||
| Quartile 1 (ref) | |||
| Quartile 2 | −45.9 (−116.2, 8.6) | 0.2 (−76.7, 77.2) | −87.0 (−203.2, 29.2) |
| Quartile 3 | −5.0 (−84.8, 74.8) | 15.5 (−56.2, 87.1) | −18.2 (−131.0, 94.7) |
| Quartile 4 | 55.3 (−0.7, 111.4) | 61.2 (7.6, 114.8) * | 68.8 (−43.4, 181.1) |
| Missing | −14.1 (−68.0, 39.7) | 45.3 (−5.4, 96.0) | −64.1 (−150.5, 22.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howard, J.T.; Janak, J.C.; Santos-Lozada, A.R.; McEvilla, S.; Ansley, S.D.; Walker, L.E.; Spiro, A.; Stewart, I.J. Telomere Shortening and Accelerated Aging in US Military Veterans. Int. J. Environ. Res. Public Health 2021, 18, 1743. https://doi.org/10.3390/ijerph18041743
Howard JT, Janak JC, Santos-Lozada AR, McEvilla S, Ansley SD, Walker LE, Spiro A, Stewart IJ. Telomere Shortening and Accelerated Aging in US Military Veterans. International Journal of Environmental Research and Public Health. 2021; 18(4):1743. https://doi.org/10.3390/ijerph18041743
Chicago/Turabian StyleHoward, Jeffrey T., Jud C. Janak, Alexis R. Santos-Lozada, Sarah McEvilla, Stephanie D. Ansley, Lauren E. Walker, Avron Spiro, and Ian J. Stewart. 2021. "Telomere Shortening and Accelerated Aging in US Military Veterans" International Journal of Environmental Research and Public Health 18, no. 4: 1743. https://doi.org/10.3390/ijerph18041743