
The Effect of Minimum and Maximum Air Temperatures in the Summer on Heat Stroke in Japan: A Time-Stratified Case-Crossover Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
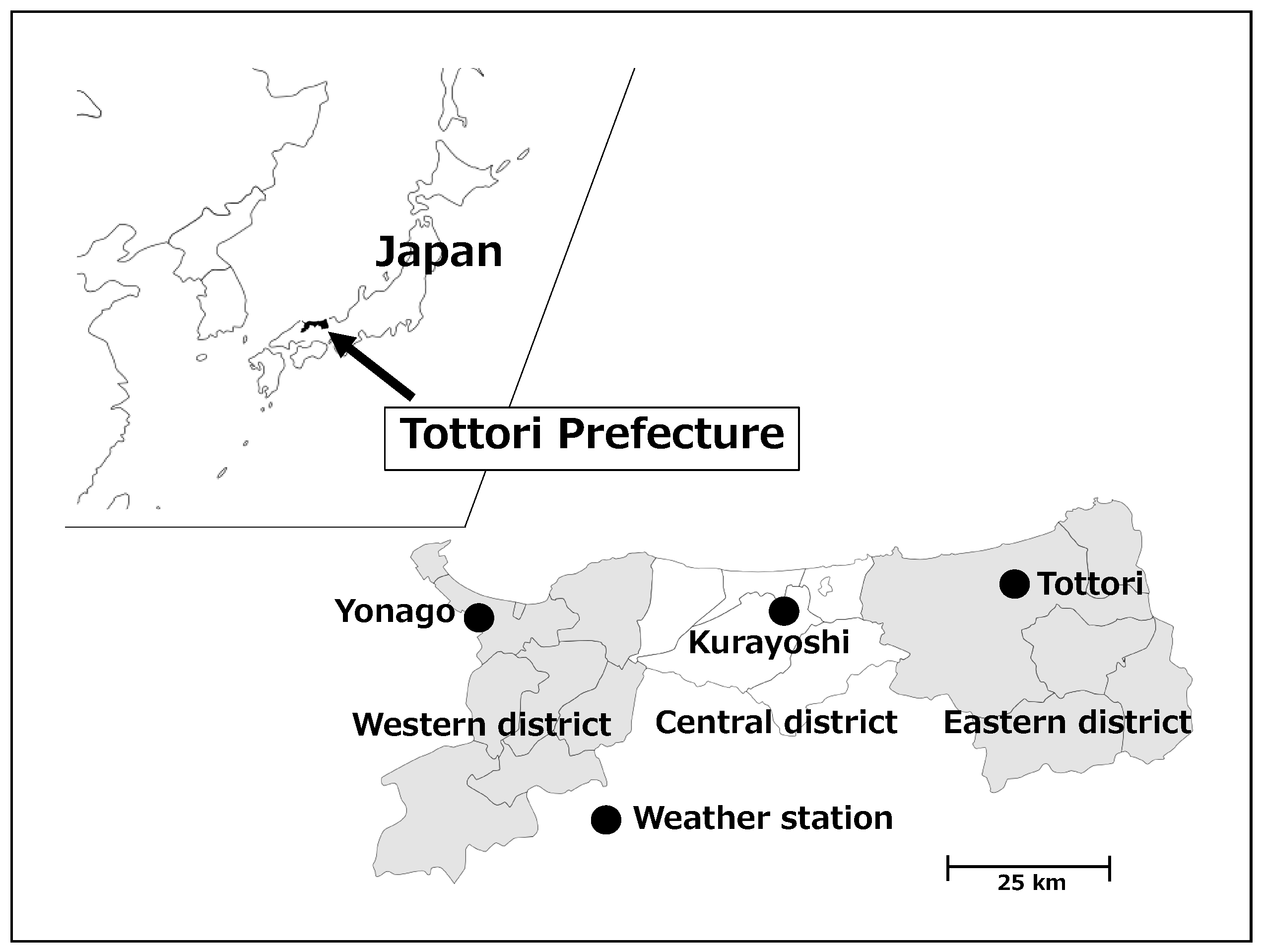
2.1. Study Design and Sites
2.2. Ambulance Transport Data
2.3. Meteorological Data
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Minimum, Average and Maximum Air Temperatures at the Study Sites
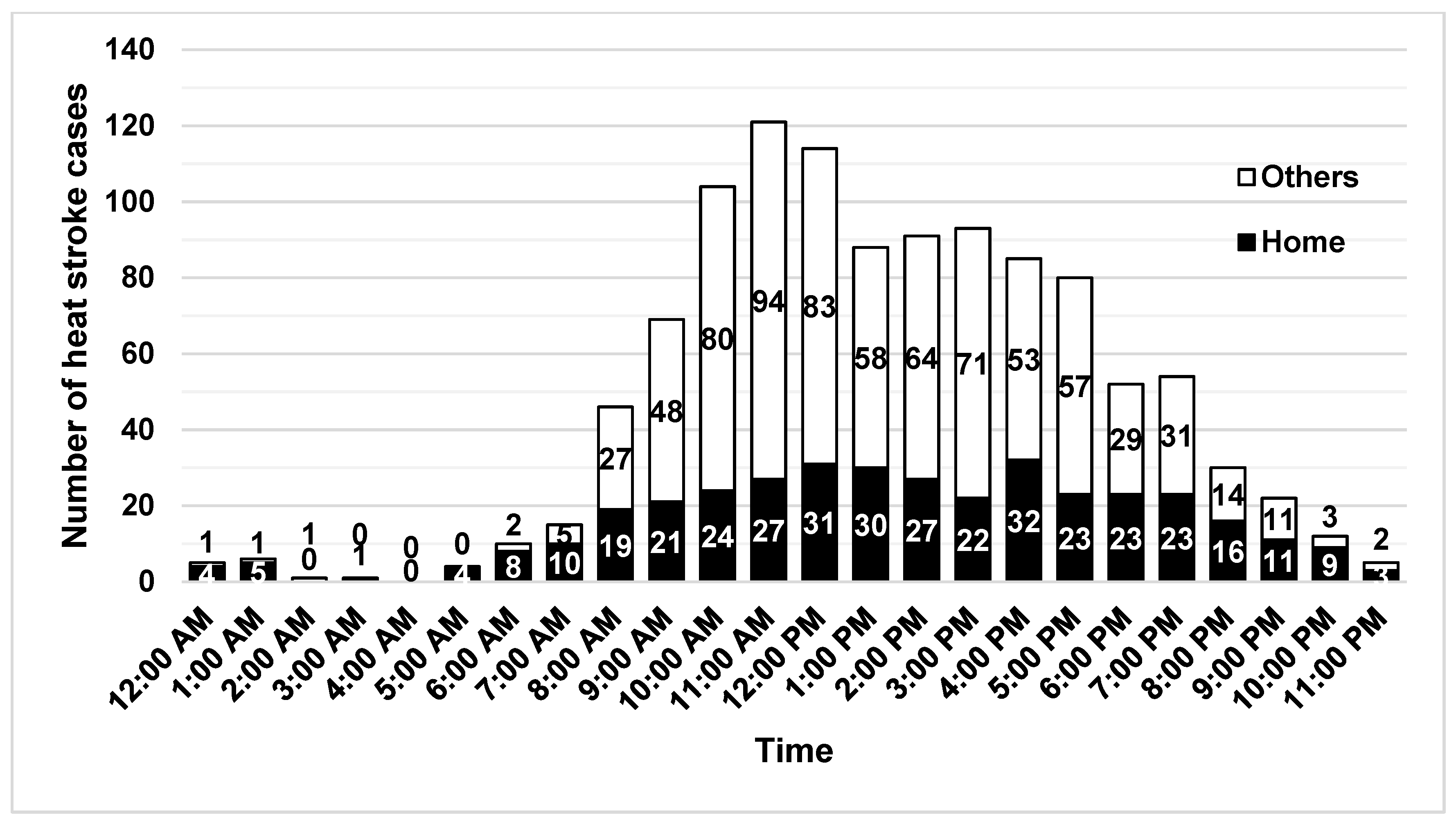
3.2. Ambulance Transport Data
3.3. Case-Crossover Analysis
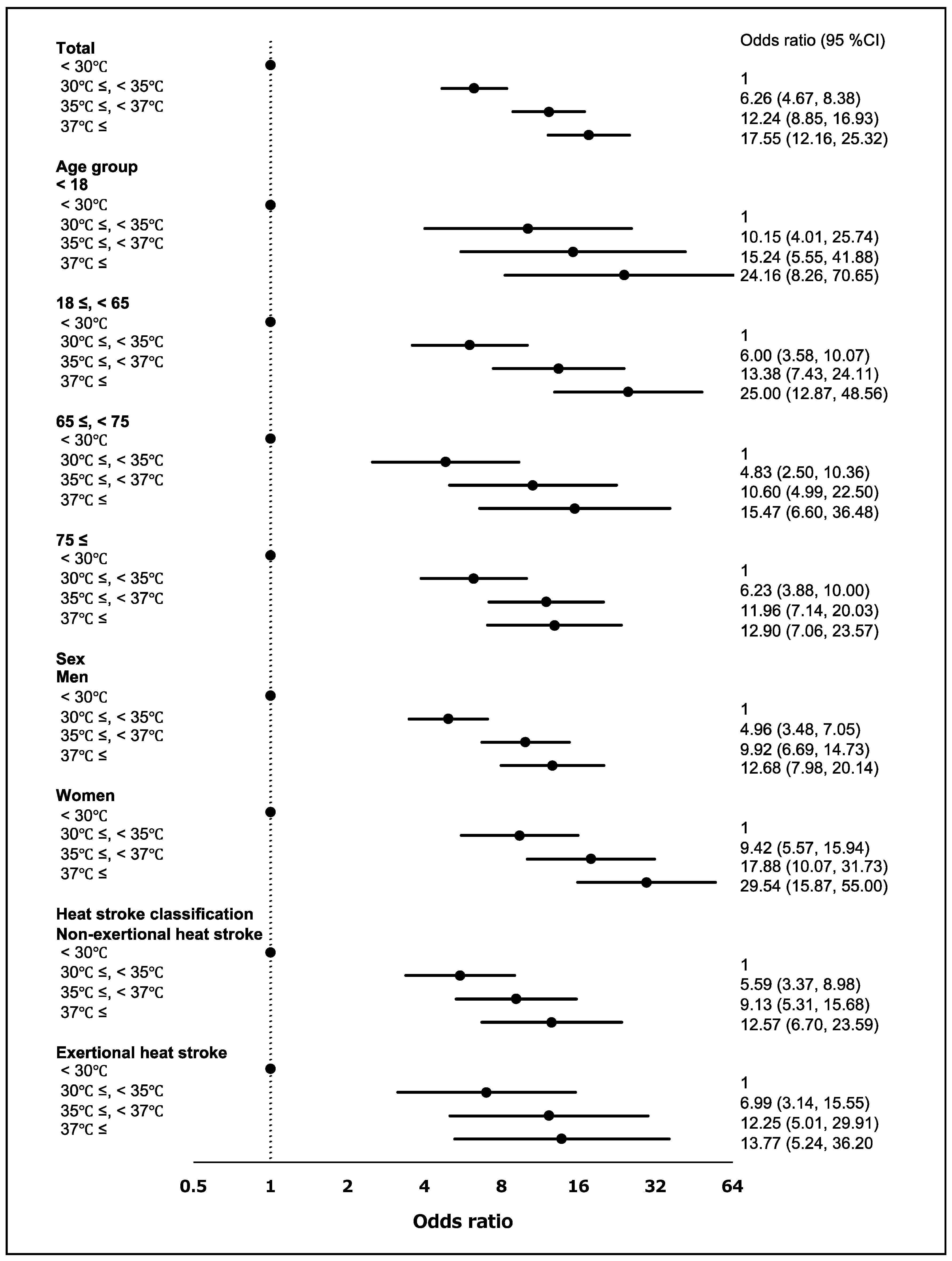
3.3.1. Maximum Air Temperature
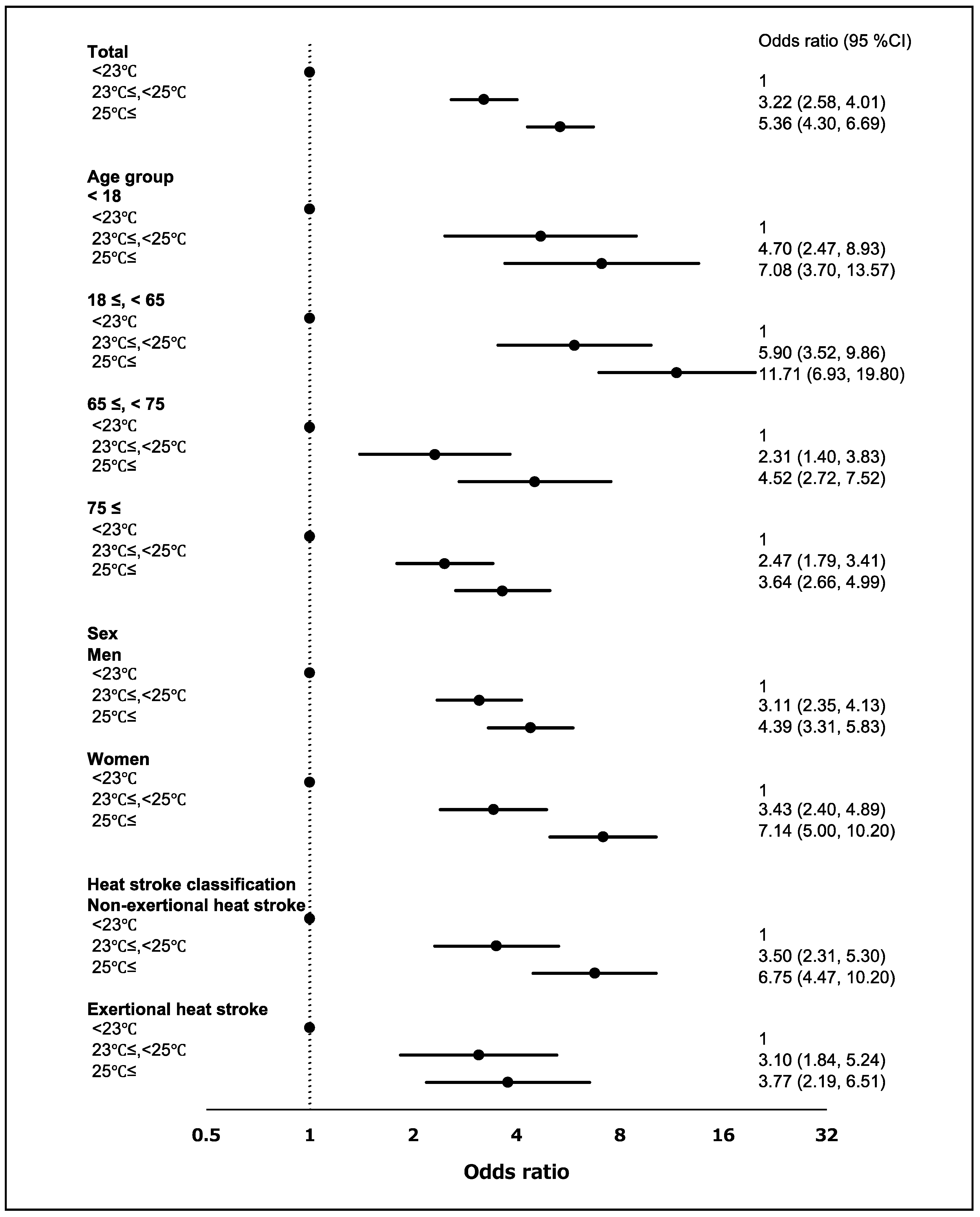
3.3.2. Minimum Air Temperature
3.4. Relationship between Air Temperature and Heat Stroke Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Epstein, Y.; Yanovich, R. Heatstroke. N. Engl. J. Med. 2019, 380, 2449–2459. [Google Scholar] [CrossRef]
- Ministry of the Environment, Guidelines for Heat Stroke Prevention at Summer Events 2020. Available online: https://www.wbgt.env.go.jp/pdf/gline/heatillness_guideline_full.pdf (accessed on 22 September 2020). (In Japanese)
- Kodera, S.; Nishimura, T.; Rashed, E.A.; Hasegawa, K.; Takeuchi, I.; Egawa, R.; Hirata, A. Estimation of heat-related morbidity from weather data: A computational study in three prefectures of Japan over 2013–2018. Environ. Int. 2019, 130, 104907. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC), Climate Change 2014: Synthesis Report. Available online: https://www.ipcc.ch/report/ar5/syr/ (accessed on 22 September 2020).
- Li, D.W.; Yuan, J.C.; Kopp, R.E. Escalating global exposure to compound heat-humidity extremes with warming. Environ. Res. Lett. 2020, 15. [Google Scholar] [CrossRef]
- Miyatake, N.; Nakao, M.; Sakano, N.; Suna, S.; Suzue, T.; Hirao, T. Higher Temperatures Were Closely Associated with Higher Ambulance Transports in Takamatsu Area, Japan. J. Environ. Prot. 2011, 2, 72–75. [Google Scholar] [CrossRef]
- Miyatake, N.; Sakano, N.; Murakami, S. The relation between ambulance transports stratified by heat stroke and air temperature in all 47 prefectures of Japan in August, 2009: Ecological study. Environ. Health Prev. Med. 2012, 17, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, N.; Sakano, N.; Murakami, S. The relation between ambulance transports due to heat stroke and air temperature using daily data in Okayama prefecture, Japan. Open J. Prev. Med. 2012, 2, 112–115. [Google Scholar] [CrossRef]
- Ng, C.F.; Ueda, K.; Ono, M.; Nitta, H.; Takami, A. Characterizing the effect of summer temperature on heatstroke-related emergency ambulance dispatches in the Kanto area of Japan. Int. J. Biometeorol. 2014, 58, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Akahane, M.; Imamura, T. Impact of Temperature in Summer on Emergency Transportation for Heat-Related Diseases in Japan. Chin. Med. J. 2018, 131, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, C.; Luo, S.; He, J.; Cheng, Y.; Jin, Y. Impacts of extremely high temperature and heatwave on heatstroke in Chongqing, China. Environ. Sci. Pollut. Res. Int. 2017, 24, 8534–8540. [Google Scholar] [CrossRef]
- Fujitani, Y.; Otani, S.; Majbauddin, A.; Amano, H.; Masumoto, T.; Kurozawa, Y. Impact of Maximum Air Temperature on Ambulance Transports Owing to Heat Stroke During Spring and Summer in Tottori Prefecture, Japan: A Time-stratified Case-crossover Analysis. Yonago Acta Med. 2019, 62, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Mohajerani, A.; Bakaric, J.; Jeffrey-Bailey, T. The urban heat island effect, its causes, and mitigation, with reference to the thermal properties of asphalt concrete. J. Environ. Manag. 2017, 197, 522–538. [Google Scholar] [CrossRef] [PubMed]
- Heaviside, C.; Macintyre, H.; Vardoulakis, S. The Urban Heat Island: Implications for Health in a Changing Environment. Curr. Environ. Health Rep. 2017, 4, 296–305. [Google Scholar] [CrossRef]
- Japan Meteorological Agency, Heat Island Monitoring Report 2017. Available online: https://www.data.jma.go.jp/cpdinfo/himr/h30/himr_2017.pdf (accessed on 22 September 2020). (In Japanese)
- Ministry of the Environment, Heat Island Measures Manual. Available online: https://www.env.go.jp/air/life/heat_island/manual_01/01_chpt1-1.pdf (accessed on 22 September 2020).
- Cheng, J.; Xu, Z.; Zhu, R.; Wang, X.; Jin, L.; Song, J.; Su, H. Impact of diurnal temperature range on human health: A systematic review. Int. J. Biometeorol. 2014, 58, 2011–2024. [Google Scholar] [CrossRef]
- Vered, S.; Paz, S.; Negev, M.; Tanne, D.; Zucker, I.; Weinstein, G. High ambient temperature in summer and risk of stroke or transient ischemic attack: A national study in Israel. Environ. Res. 2020, 187, 109678. [Google Scholar] [CrossRef]
- Hausfater, P.; Megarbane, B.; Dautheville, S.; Patzak, A.; Andronikof, M.; Santin, A.; Andre, S.; Korchia, L.; Terbaoui, N.; Kierzek, G.; et al. Prognostic factors in non-exertional heatstroke. Intensive Care Med. 2010, 36, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Alele, F.O.; Malau-Aduli, B.S.; Malau-Aduli, A.E.O.; Crowe, M.J. Epidemiology of Exertional Heat Illness in the Military: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public Health 2020, 17, 7037. [Google Scholar] [CrossRef]
- Yeargin, S.W.; Dompier, T.P.; Casa, D.J.; Hirschhorn, R.M.; Kerr, Z.Y. Epidemiology of Exertional Heat Illnesses in National Collegiate Athletic Association Athletes During the 2009–2010 Through 2014–2015 Academic Years. J. Athl. Train. 2019, 54, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Portal Site of Official Statistic of Japan, Population Concentration Areas of Each Prefecture, Ministry of Internal Affairs and Communications. Available online: https://www.e-stat.go.jp/dbview?sid=0003413758 (accessed on 18 October 2020). (In Japanese)
- Portal Site of Official Statistic of Japan, Number and percentage of consumer goods owned per 1,000 households by prefecture, Ministry of Internal Affairs and Communications. Available online: https://www.e-stat.go.jp/dbview?sid=0003108720 (accessed on 18 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2019. Available online: https://www.fdma.go.jp/disaster/heatstroke/items/heatstroke004_houdou01.pdf (accessed on 16 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2018. Available online: https://www.fdma.go.jp/disaster/heatstroke/item/heatstroke003_houdou01.pdf (accessed on 16 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2017. Available online: https://www.fdma.go.jp/disaster/heatstroke/item/heatstroke001_houdou_01.pdf (accessed on 16 October 2020). (In Japanese)
- World Health Organization, ICD-10 Version: 2019. Available online: https://icd.who.int/browse10/2019/en#/T67.0 (accessed on 17 October 2020).
- Yamamoto, T.; Fujita, M.; Oda, Y.; Todani, M.; Hifumi, T.; Kondo, Y.; Shimazaki, J.; Shiraishi, S.; Hayashida, K.; Yokobori, S.; et al. Evaluation of a Novel Classification of Heat-Related Illnesses: A Multicentre Observational Study (Heat Stroke STUDY 2012). Int. J. Environ. Res. Public Health 2018, 15, 1962. [Google Scholar] [CrossRef]
- Luo, X.; Sorock, G.S. Analysis of recurrent event data under the case-crossover design with applications to elderly falls. Stat. Med. 2008, 27, 2890–2901. [Google Scholar] [CrossRef] [PubMed]
- Byrwa-Hill, B.M.; Venkat, A.; Presto, A.A.; Rager, J.R.; Gentile, D.; Talbott, E. Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region. Int. J. Environ. Res. Public Health 2020, 17, 8619. [Google Scholar] [CrossRef] [PubMed]
- Contiero, P.; Boffi, R.; Tagliabue, G.; Scaburri, A.; Tittarelli, A.; Bertoldi, M.; Borgini, A.; Favia, I.; Ruprecht, A.A.; Maiorino, A.; et al. A Case-Crossover Study to Investigate the Effects of Atmospheric Particulate Matter Concentrations, Season, and Air Temperature on Accident and Emergency Presentations for Cardiovascular Events in Northern Italy. Int. J. Environ. Res. Public Health 2019, 16, 4627. [Google Scholar] [CrossRef]
- Parry, M.; Green, D.; Zhang, Y.; Hayen, A. Does Particulate Matter Modify the Short-Term Association between Heat Waves and Hospital Admissions for Cardiovascular Diseases in Greater Sydney, Australia? Int. J. Environ. Res. Public Health 2019, 16, 3270. [Google Scholar] [CrossRef]
- Zhang, P.; Wiens, K.; Wang, R.; Luong, L.; Ansara, D.; Gower, S.; Bassil, K.; Hwang, S.W. Cold Weather Conditions and Risk of Hypothermia Among People Experiencing Homelessness: Implications for Prevention Strategies. Int. J. Environ. Res. Public Health 2019, 16, 3259. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Suzuki, E.; Kashima, S. Hourly differences in air pollution and risk of respiratory disease in the elderly: A time-stratified case-crossover study. Environ. Health 2014, 13, 67. [Google Scholar] [CrossRef]
- Basu, R.; Dominici, F.; Samet, J.M. Temperature and mortality among the elderly in the United States: A comparison of epidemiologic methods. Epidemiology 2005, 16, 58–66. [Google Scholar] [CrossRef]
- Spector, J.T.; Bonauto, D.K.; Sheppard, L.; Busch-Isaksen, T.; Calkins, M.; Adams, D.; Lieblich, M.; Fenske, R.A. A Case-Crossover Study of Heat Exposure and Injury Risk in Outdoor Agricultural Workers. PLoS ONE 2016, 11, e0164498. [Google Scholar] [CrossRef]
- Westwood, C.S.; Fallowfield, J.L.; Delves, S.K.; Nunns, M.; Ogden, H.B.; Layden, J.D. Individual risk factors associated with exertional heat illness: A systematic review. Exp. Physiol. 2020. [Google Scholar] [CrossRef]
- Iriki, M.; Simon, E. Heat disorder in Yamanashi Prefecture during the summer from 1995 to 2004. Ind. Health 2006, 44, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Japan Meteorological Agency, Terms Used in Weather Forecasting, etc. Available online: https://www.jma.go.jp/jma/kishou/know/yougo_hp/kion.html (accessed on 22 September 2020). (In Japanese)
- Obradovich, N.; Migliorini, R.; Mednick, S.C.; Fowler, J.H. Nighttime temperature and human sleep loss in a changing climate. Sc.i Adv. 2017, 3, e1601555. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhou, M.; Li, M.; Yin, P.; Wang, B.; Pilot, E.; Liu, Y.; van der Hoek, W.; van Asten, L.; Krafft, T.; et al. Diurnal temperature range in relation to death from stroke in China. Environ. Res 2018, 164, 669–675. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Ageing 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 23 September 2020).
- Leyk, D.; Hoitz, J.; Becker, C.; Glitz, K.J.; Nestler, K.; Piekarski, C. Health Risks and Interventions in Exertional Heat Stress. Dtsch. Arztebl. Int. 2019, 116, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Ono, M.; Nakazawa, K.; Kayaba, M.; Minakuchi, E.; Sugimoto, K.; Honda, Y. Population at high-risk of indoor heatstroke: The usage of cooling appliances among urban elderlies in Japan. Environ. Health Prev. Med. 2013, 18, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Khare, S.; Hajat, S.; Kovats, S.; Lefevre, C.E.; de Bruin, W.B.; Dessai, S.; Bone, A. Heat protection behaviour in the UK: Results of an online survey after the 2013 heatwave. BMC Public Health 2015, 15, 878. [Google Scholar] [CrossRef]
- Kravchenko, J.; Abernethy, A.P.; Fawzy, M.; Lyerly, H.K. Minimization of heatwave morbidity and mortality. Am. J. Prev. Med. 2013, 44, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Aruga, T.; Inoue, K.; Okudera, H.; KItahara, T.; Shimazaki, S.; Tsuruta, R.; Maekawa, T.; Yokota, H. The characteristics of classical heatstroke in Japan. Jpn. J. Intensive Care Med. 2009, 33, 309–315. (In Japanese) [Google Scholar]
- Alele, F.; Malau-Aduli, B.; Malau-Aduli, A.; Crowe, M. Systematic review of gender differences in the epidemiology and risk factors of exertional heat illness and heat tolerance in the armed forces. BMJ Open 2020, 10, e031825. [Google Scholar] [CrossRef] [PubMed]
- Chung, N.K.; Pin, C.H. Obesity and the occurrence of heat disorders. Mil. Med. 1996, 161, 739–742. [Google Scholar] [CrossRef] [PubMed]
- Nutong, R.; Mungthin, M.; Hatthachote, P.; Ukritchon, S.; Imjaijit, W.; Tengtrakulcharoen, P.; Panichkul, S.; Putwatana, P.; Prapaipanich, W.; Rangsin, R. Personal risk factors associated with heat-related illness among new conscripts undergoing basic training in Thailand. PLoS ONE 2018, 13, e0203428. [Google Scholar] [CrossRef] [PubMed]
- Budd, G.M. Wet-bulb globe temperature (WBGT—Its history and its limitations. J. Sci. Med. Sport 2008, 11, 20–32. [Google Scholar] [CrossRef]
- Harlan, S.L.; Chowell, G.; Yang, S.; Petitti, D.B.; Morales Butler, E.J.; Ruddell, B.L.; Ruddell, D.M. Heat-related deaths in hot cities: Estimates of human tolerance to high temperature thresholds. Int. J. Environ. Res. Public Health 2014, 11, 3304–3326. [Google Scholar] [CrossRef] [PubMed]
- Steadman, R.G. The Assessment of Sultriness. Part I: A Temperature-Humidity Index Based on Human Physiology and Clothing Science. J. Appl. Meteorol. 1979, 18, 861–873. [Google Scholar] [CrossRef]
- Parsons, K. Heat stress Standard ISO 7243 and its global application. Ind. Health 2006, 44, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Zauli Sajani, S.; Scotto, F.; Miglio, R.; Marchesi, S.; Lauriola, P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia-Romagna, Italy. Environ. Res. 2011, 111, 1192–1200. [Google Scholar] [CrossRef]
- Peters, A.; von Klot, S.; Berglind, N.; Hormann, A.; Lowel, H.; Nyberg, F.; Pekkanen, J.; Perucci, C.A.; Stafoggia, M.; Sunyer, J.; et al. Comparison of different methods in analyzing short-term air pollution effects in a cohort study of susceptible individuals. Epidemiol. Perspect. Innov. 2006, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Lumley, T.; Levy, D. Bias in the case-crossover design: Implications for studies of air pollution. Environmetrics 2000, 11, 689–704. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| July | August | |||||
|---|---|---|---|---|---|---|
| Minimum Value | Average Value | Maximum Value | Minimum Value | Average Value | Maximum Value | |
| Tottori | 23.6 (22.0) | 27.3 (25.7) | 32.1 (30.4) | 23.9 (22.9) | 28.0 (27.0) | 33.5 (32.2) |
| Kurayoshi | 22.8 (21.7) | 26.0 (24.9) | 29.8 (28.8) | 22.9 (22.4) | 26.6 (26.0) | 30.8 (30.2) |
| Yonago | 23.9 (22.3) | 27.3 (25.6) | 31.5 (29.6) | 24.3 (23.3) | 28.1 (26.9) | 32.8 (31.2) |
| July | August | |||||
|---|---|---|---|---|---|---|
| Tmin25 °C | Tmax30 °C | Tmax35 °C | Tmin25 °C | Tmax30 °C | Tmax35 °C | |
| Tottori | 19 | 70 | 36 | 31 | 81 | 36 |
| Kurayoshi | 11 | 49 | 2 | 11 | 57 | 3 |
| Yonago | 32 | 65 | 19 | 41 | 77 | 25 |
| Age Group | Men | Women | Total |
|---|---|---|---|
| <18 | 83 (1.901) | 85 (2.043) | 168 (1.970) |
| 18≤, <65 | 216 (1.488) | 86 (0.596) | 302 (1.043) |
| 65≤, <75 | 129 (3.27) | 58 (1.343) | 187 (2.242) |
| 75≤ | 210 (6.155) | 241 (4.086) | 451 (4.845) |
| Total | 638 (2.401) | 470 (1.769) | 1108 (1.994) |
| Home | Work | Exercise | Outing | Farm Work | Event | Tourism | Others | Total | |
|---|---|---|---|---|---|---|---|---|---|
| Severity | |||||||||
| Mild | 139 | 115 | 111 | 104 | 35 | 10 | 8 | 1 | 523 |
| Moderate | 219 | 113 | 62 | 90 | 55 | 6 | 7 | 1 | 553 |
| Severe | 14 | 3 | 0 | 4 | 7 | 0 | 0 | 0 | 28 |
| Death | 1 | 1 | 0 | 0 | 2 | 0 | 0 | 0 | 4 |
| Total | 373 | 232 | 173 | 198 | 99 | 16 | 15 | 2 | 1108 |
| Age group | |||||||||
| <18 | 7 | 11 | 110 | 26 | 0 | 11 | 3 | 0 | 168 |
| (42.9%) | (36.4%) | (35.5%) | (34.6%) | (–) | (36.4%) | (33.3%) | (–) | (35.7%) | |
| 18≤, <65 | 60 | 138 | 34 | 49 | 9 | 4 | 8 | 0 | 302 |
| (46.7%) | (48.6%) | (35.3%) | (38.8%) | (55.6%) | (25.0%) | (50%) | (–) | (45.0%) | |
| 65≤, <75 | 83 | 34 | 7 | 36 | 22 | 1 | 3 | 1 | 187 |
| (55.4%) | (38.2%) | (14.3%) | (61.1%) | (54.5%) | (100%) | (66.7%) | (100%) | (52.4%) | |
| 75≤ | 223 | 49 | 22 | 87 | 68 | 0 | 1 | 1 | 451 |
| (70.4%) | (67.3%) | (45.5%) | (50.6%) | (69.1%) | (–) | (0%) | (0%) | (64.5%) | |
| Total | 373 | 232 | 173 | 198 | 99 | 16 | 15 | 2 | 1108 |
| (62.7%) | (50.4%) | (35.8%) | (47.5%) | (64.6%) | (37.5%) | (46.7%) | (50%) | (52%) |
| Model 1 | |||||
| Variable | Coefficient | Standard error | p Value | 95% Confidence Interval | |
| Lower | Upper | ||||
| Age | 0.014 | 0.003 | <0.001 | 0.009 | 0.019 |
| Sex | −0.027 | 0.124 | 0.829 | −0.270 | 0.217 |
| Maximum air temperature | 0.041 | 0.034 | 0.232 | −0.026 | 0.108 |
| Relative humidity | 0.007 | 0.012 | 0.561 | −0.016 | 0.030 |
| Home | 0.254 | 0.140 | 0.070 | −0.021 | 0.529 |
| Exercise | −0.261 | 0.198 | 0.187 | −0.649 | 0.127 |
| Model 2 | |||||
| Variable | Coefficient | Standard error | p Value | 95% Confidence Interval | |
| Lower | Upper | ||||
| Age | 0.015 | 0.003 | <0.001 | 0.009 | 0.020 |
| Sex | −0.018 | 0.124 | 0.886 | −0.262 | 0.226 |
| Minimum air temperature | 0.068 | 0.040 | 0.086 | −0.010 | 0.146 |
| Relative humidity | 0.005 | 0.010 | 0.630 | −0.014 | 0.023 |
| Home | 0.233 | 0.141 | 0.098 | −0.043 | 0.509 |
| Exercise | −0.237 | 0.199 | 0.234 | −0.626 | 0.153 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otani, S.; Funaki Ishizu, S.; Masumoto, T.; Amano, H.; Kurozawa, Y. The Effect of Minimum and Maximum Air Temperatures in the Summer on Heat Stroke in Japan: A Time-Stratified Case-Crossover Study. Int. J. Environ. Res. Public Health 2021, 18, 1632. https://doi.org/10.3390/ijerph18041632
Otani S, Funaki Ishizu S, Masumoto T, Amano H, Kurozawa Y. The Effect of Minimum and Maximum Air Temperatures in the Summer on Heat Stroke in Japan: A Time-Stratified Case-Crossover Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1632. https://doi.org/10.3390/ijerph18041632
Chicago/Turabian StyleOtani, Shinji, Satomi Funaki Ishizu, Toshio Masumoto, Hiroki Amano, and Youichi Kurozawa. 2021. "The Effect of Minimum and Maximum Air Temperatures in the Summer on Heat Stroke in Japan: A Time-Stratified Case-Crossover Study" International Journal of Environmental Research and Public Health 18, no. 4: 1632. https://doi.org/10.3390/ijerph18041632
APA StyleOtani, S., Funaki Ishizu, S., Masumoto, T., Amano, H., & Kurozawa, Y. (2021). The Effect of Minimum and Maximum Air Temperatures in the Summer on Heat Stroke in Japan: A Time-Stratified Case-Crossover Study. International Journal of Environmental Research and Public Health, 18(4), 1632. https://doi.org/10.3390/ijerph18041632