Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity



Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Selection
2.2. Alternate Day Fasting-Low Carbohydrate (ADF-LC) Diet Protocol
2.2.1. Weight Loss Period (Month 0–3)
2.2.2. Weight Maintenance Period (Month 3–6)
2.3. Body Weight, Body Composition, Physical Activity, and Diet Adherence
2.4. Sleep Measures
2.5. Statistical Analysis
3. Results
3.1. Body Weight, Body Composition, Physical Activity, and Diet Adherence
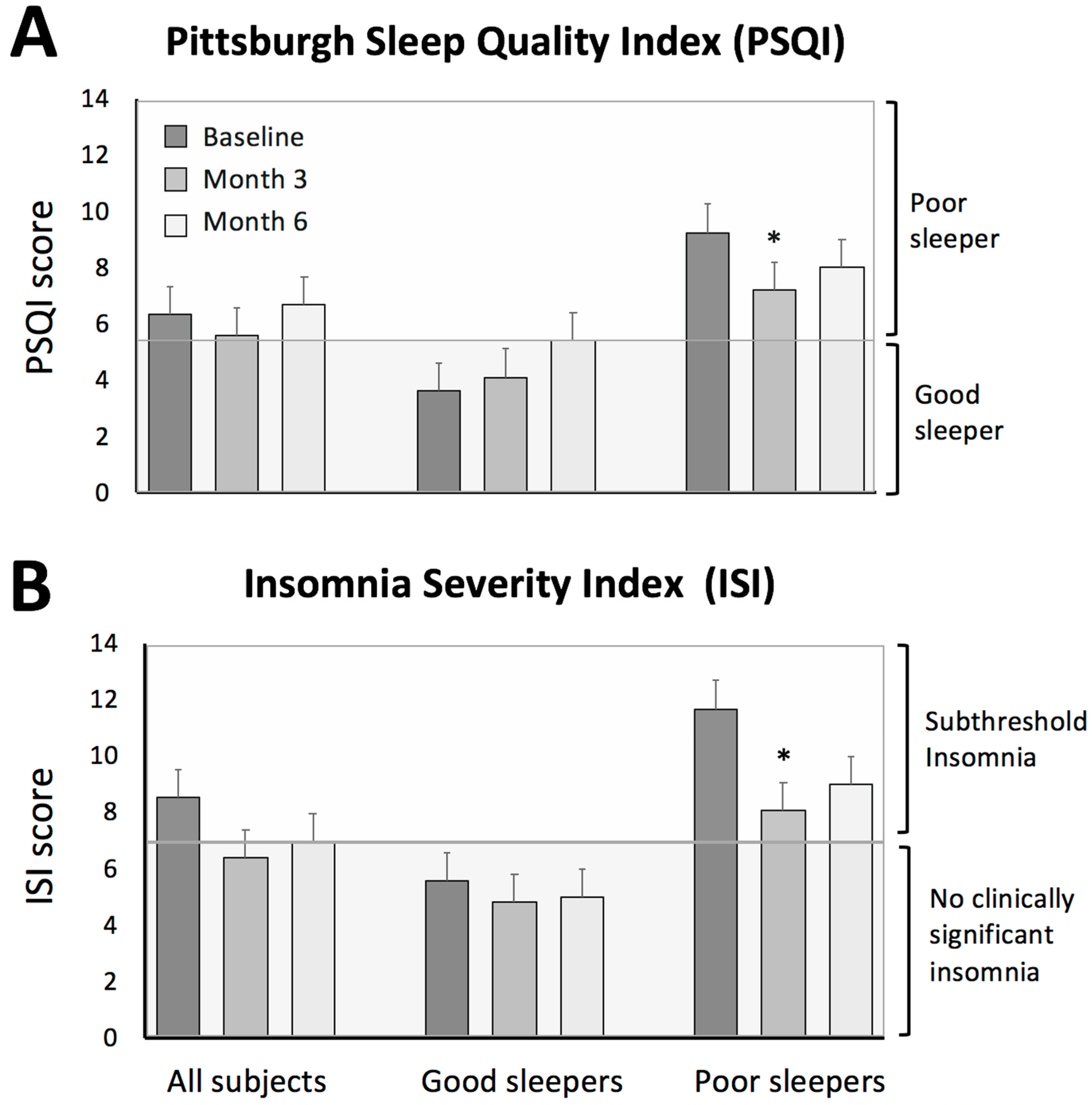
3.2. Sleep Quality
3.3. Insomnia Severity
3.4. Risk of Obstructive Sleep Apnea
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hales, C.M.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. In NCHS Data Brief, No. 360; National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- Beccuti, G.; Pannain, S. Sleep and obesity. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 402–412. [Google Scholar] [CrossRef]
- Hasler, G.; Buysse, D.J.; Klaghofer, R.; Gamma, A.; Ajdacic, V.; Eich, D.; Rössler, W.; Angst, J. The association between short sleep duration and obesity in young adults: A 13-year prospective study. Sleep 2004, 27, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chapman, D.P.W.A.; Cunningham, T.J.; Lu, H.; Croft, J.B. Prevalence of healthy sleep duration among adults—United States, 2014. MMWR Morb. Mortal Weekly Rep. 2016, 65, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.J.; Davidson, Z.E.; Bonham, M.; O’Driscoll, D.M.; Hamilton, G.S.; Truby, H. Weight loss from lifestyle interventions and severity of sleep apnoea: A systematic review and meta-analysis. Sleep Med. 2014, 15, 1173–1183. [Google Scholar] [CrossRef] [PubMed]
- Zimberg, I.Z.; Dâmaso, A.; Del Re, M.; Carneiro, A.M.; de Sá Souza, H.; Santos de Lira, F.; Tufik, S.; Túlio de Mello, M. Short sleep duration and obesity: Mechanisms and future perspectives. Cell Biochem. Funct. 2012, 30, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Sanders, M.H.; Millman, R.; Zammit, G.; Borradaile, K.E.; Newman, A.B.; Wadden, T.A.; Kelley, D.; Wing, R.R.; Sunyer, R.F.X.P.; et al. Sleep AHEAD research group. Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care 2009, 32, 1017–1019. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Caples, S.M.; Lopez-Jimenez, F.; Somers, V.K. Interactions between obesity and obstructive sleep apnea: Implications for treatment. Chest 2010, 137, 711–719. [Google Scholar] [CrossRef]
- Alfaris, N.; Wadden, T.A.; Sarwer, D.B.; Diwald, L.; Volger, S.; Hong, P.; Baxely, A.; Minnick, A.M.; Vetter, M.L.; Berkowitz, R.L.; et al. Effects of a 2-year behavioral weight loss intervention on sleep and mood in obese individuals treated in primary care practice. Obesity (Silver Spring) 2015, 23, 558–564. [Google Scholar] [CrossRef]
- Martin, C.K.; Bhapkar, M.; Pittas, A.G.; Pieper, C.F.; Das, S.K.; Williamson, D.A.; Scott, T.; Redman, L.M.; Stein, R.; Gilhooly, C.H.; et al. Effect of calorie restriction on mood, quality of life, sleep, and sexual function in healthy nonobese adults: The CALERIE 2 randomized clinical trial. JAMA Intern. Med. 2016, 176, 743–752. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Shechter, A. Sleep disturbances, body fat distribution, food intake and/or energy expenditure: Pathophysiological aspects. Horm. Mol. Biol. Clin. Investig. 2014, 17, 29–37. [Google Scholar] [CrossRef]
- Hoddy, K.K.; Potts, K.S.; Bazzano, L.A.; Kirwan, J.P. Sleep extension: A potential target for obesity treatment. Curr. Diab. Rep. 2020, 20, 81. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.A.; Morrow, K.L.; Flatt, S.W.; Wertheim, B.C.; Perfect, M.M.; Ravia, J.J.; Sherwood, N.E.; Karanja, N.; Rocket, C.L. Relationship between sleep quality and quantity and weight loss in women participating in a weight-loss intervention trial. Obesity (Silver Spring) 2012, 20, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; de Cabo, R. Effects of intermittent fasting on health, aging, and disease. Reply. N. Engl. J. Med. 2020, 382, 1773–1774. [Google Scholar] [PubMed]
- Patterson, R.E.; Sears, D.D. Metabolic effects of intermittent fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.C.; Bhutani, S.; Hoddy, K.K.; Gabel, K.; Freels, S.; Rigdon, J.; Roodet, J.; et al. Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults: A randomized clinical trial. JAMA Int. Med. 2017, 177, 930–938. [Google Scholar] [CrossRef]
- Afaghi, A.; O’Connor, H.; Chow, C.M. Acute effects of the very low carbohydrate diet on sleep indices. Nutr. Neurosci. 2008, 11, 146–154. [Google Scholar] [CrossRef]
- Tanaka, E.; Yatsuya, H.; Uemura, M.; Murata, C.M.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Sasaki, S.; Kawaguchi, L.; Aoyama, A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. J. Epidemiol. 2013, 23, 132–138. [Google Scholar] [CrossRef]
- Lindseth, G.; Lindseth, P.; Thompson, M. Nutritional effects on sleep. West J. Nurs. Res. 2013, 35, 497–513. [Google Scholar] [CrossRef]
- Zhou, J.; Kim, J.E.; Armstrong, C.L.H.; Chen, N.; Campbell, W.W. Higher-protein diets improve indexes of sleep in energy-restricted overweight and obese adults: Results from 2 randomized controlled trials. Am. J. Clin. Nutr. 2016, 103, 766–774. [Google Scholar] [CrossRef]
- Castro, A.I.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Granero, R.; Aguera, Z.; Jimenez-Murcia, S.; Sajoux, I.; Lopez-Jaramillo, P.; Fernandez-Aranda, F.; Casanueva, F.F. Effect of a very low-calorie ketogenic diet on food and alcohol cravings, physical and sexual activity, sleep disturbances, and quality of life in obese patients. Nutrients 2018, 10, 1348. [Google Scholar] [CrossRef]
- Kalam, F.; Gabel, K.; Cienfuegos, S.; Wiseman, E.; Ezpeleta, M.; Steward, M.; Pavlou, V.; Varady, K.A. Alternate day fasting combined with a low-carbohydrate diet for weight loss, weight maintenance, and metabolic disease risk reduction. Obes. Sci. Pract. 2019, 5, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. Validation of the Berlin questionnaire and American society of anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008, 108, 822–830. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity. Cell Metab. 2020, 32, 366–378.e3. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020, 31, 92–104. [Google Scholar] [CrossRef]
- Yannakoulia, M.; Anastasiou, C.A.; Karfopoulou, E.; Pehlivanidis, A.; Panagiotakos, D.B.; Vgontzas, A. Sleep quality is associated with weight loss maintenance status: The MedWeight study. Sleep Med. 2017, 34, 242–245. [Google Scholar] [CrossRef]
- Yajima, K.; Seya, T.; Iwayama, K.; Hibi, M.; Hari, S.; Nakashima, Y.; Ogata, H.; Omi, N.; Satoh, M.; Tokuyama, K. Effects of nutrient composition of dinner on sleep architecture and energy metabolism during sleep. J. Nutr. Sci. Vitaminol. 2014, 60, 114–121. [Google Scholar] [CrossRef]
- Lindseth, G.; Murray, A. Dietary macronutrients and sleep. West J. Nurs. Res. 2016, 38, 938–958. [Google Scholar] [CrossRef]
- Daneshzad, E.; Daneshzad, E.; Keshavarz, S.-A.; Qorbani, M.; Larijani, B.; Azadbakht, L. Association between a low-carbohydrate diet and sleep status, depression, anxiety, and stress score. J. Sci. Food Agric. 2020, 100, 2946–2952. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.L.; Zhou, J.; Campbell, W.W. Adults who are overweight or obese and consuming an energy-restricted healthy US-style eating pattern at either the recommended or a higher protein quantity perceive a shift from “Poor” to “Good” sleep: A randomized controlled trial. J. Nutr. 2020, 150, 3216–3223. [Google Scholar] [CrossRef] [PubMed]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef]
- Silva-Costa, A.; Rotenberg, L.; Nobre, A.A.; Chor, D.; Aquino, E.M.; Melo, E.C.; Barreto, S.M.; Schmidt, M.I.; Griepcorresponding, R.H. Sex differences in the association between self-reported sleep duration, insomnia symptoms and cardiometabolic risk factors: Cross-sectional findings from Brazilian longitudinal study of adult health. Arch. Publ. Health 2020, 78, 48. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Perumean-Chaney, S.; Desmond, R.; Lewis, C.E.; Yan, L.L.; Person, S.D.; Allison, D.B. Gender differences in the association between sleep duration and body composition: The cardia study. Int. J. Endorcinol. 2010, 10, 26. [Google Scholar] [CrossRef]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Lucassen, E.A.; Zhao, X.; Rother, K.I.; Mattingly, M.S.; Courville, A.B.; de Jonge, L.; Csako, G.; Cizza, G. Sleep extension study group. Evening chronotype is associated with changes in eating Behavior, more sleep apnea, and increased stress hormones in short sleeping obese individuals. PLoS ONE 2013, 8, 56519. [Google Scholar] [CrossRef]


{kind=link}
| All Subjects (n = 31) | Good Sleepers (n = 16) | Poor Sleepers (n = 15) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Month 3 | Month 6 | Baseline | Month 3 | Month 6 | Baseline | Month 3 | Month 6 | |
| Demographics | |||||||||
| Age | 48 ± 2 | 49 ± 3 | 48 ± 2 | ||||||
| Sex (Female/Male) | 25/6 | 12/4 | 13/2 | ||||||
| Race/Ethnicity | |||||||||
| White | 1 | 0 | 1 | ||||||
| Black | 18 | 9 | 9 | ||||||
| Asian | 3 | 3 | 0 | ||||||
| Hispanic | 9 | 4 | 5 | ||||||
| Anthropometrics | |||||||||
| Body weight (kg) | 100 ± 3 | 95 ± 3 * | 94 ± 4 * | 100 ± 5 | 94 ± 5 * | 94 ± 5 * | 100 ± 5 | 96 ± 5 * | 94 ± 5 * |
| Fat mass (kg) | 46 ± 2 | 42 ± 2 * | 41 ± 3 * | 46 ± 3 | 42 ± 3 * | 41 ± 3 * | 45 ± 3 | 42 ± 4 * | 40 ± 4 * |
| Lean mass (kg) | 49 ± 2 | 48 ± 1 * | 49 ± 2 | 49 ± 2 | 48 ± 2 * | 49 ± 2 | 50 ± 2 | 48 ± 2 * | 49 ± 2 |
| Visceral fat mass (kg) | 1.4 ± 0.1 | 1.2 ± 0.1 | 1.2 ± 0.1 | 1.4 ± 0.2 | 1.3 ± 0.2 | 1.3 ± 0.2 | 1.3 ± 0.1 | 1.2 ± 0.2 | 1.2 ± 0.2 |
| Steps/day | 6931 ± 842 | 8070 ± 989 | 7648 ± 773 | 8104 ± 1365 | 8852 ± 1496 | 8449 ± 1168 | 6019 ± 1019 | 7461 ± 1391 | 7025 ± 992 |
| Pittsburgh Sleep Quality Index (PSQI) | |||||||||
| Total score | 6.4 ± 0.7 | 5.6 ± 0.5 | 6.7 ± 0.7 | 3.6 ± 0.4 | 4.1 ± 0.6 | 5.4 ± 1.1 | 9.3 ± 0.9 | 7.2 ± 0.7 * | 8.0 ± 0.9 |
| Wake time (h:min) | 6:05 ± 0:25 | 6:20 ± 0:30 | 6:00 ± 0:20 | 5:50 ± 0:20 | 5:45 ± 0:20 | 5:40 ± 0:20 | 5:20 ± 0:15 | 5:35 ± 0:20 | 5:20 ± 0:25 |
| Bedtime (h:min) | 22:30 ± 0:20 | 22:15 ± 0:15 | 22:10 ± 0:25 | 22:20 ± 0:15 | 22:10 ± 0:20 | 22:00 ± 0:20 | 22:35 ± 0:15 | 22:20 ± 0:15 | 22:20 ± 0:20 |
| Sleep duration (h:min) | 7:35 ± 0:20 | 8:05 ± 0:25 | 7:50 ± 0:20 | 7:30 ± 0:15 | 7:35 ± 0:20 | 7:40 ± 0:20 | 6:45 ± 0:15 | 7:15 ± 0:20 | 7:00 ± 0:20 |
| Insomnia severity index (ISI) | |||||||||
| Total score | 8.5 ± 1.0 | 6.4 ± 0.9 | 6.9 ± 1.1 | 5.6 ± 0.9 | 4.8 ± 1.0 | 5.0 ± 1.6 | 11.7 ± 1.3 | 8.1 ± 1.4 * | 9.0 ± 1.5 |
| Berlin questionnaire | |||||||||
| High risk of obstructive sleep apnea (%) | 45% | 42% | 32% | 38% | 38% | 31% | 53% | 47% | 33% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalam, F.; Gabel, K.; Cienfuegos, S.; Ezpeleta, M.; Wiseman, E.; Varady, K.A. Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity. Nutrients 2021, 13, 211. https://doi.org/10.3390/nu13010211
Kalam F, Gabel K, Cienfuegos S, Ezpeleta M, Wiseman E, Varady KA. Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity. Nutrients. 2021; 13(1):211. https://doi.org/10.3390/nu13010211
Chicago/Turabian StyleKalam, Faiza, Kelsey Gabel, Sofia Cienfuegos, Mark Ezpeleta, Eric Wiseman, and Krista A. Varady. 2021. "Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity" Nutrients 13, no. 1: 211. https://doi.org/10.3390/nu13010211
APA StyleKalam, F., Gabel, K., Cienfuegos, S., Ezpeleta, M., Wiseman, E., & Varady, K. A. (2021). Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity. Nutrients, 13(1), 211. https://doi.org/10.3390/nu13010211