Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Intervention
2.3. Participants
2.4. The Study Tool
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A.—The Indices and Questions Used in the Study
- 1.
- Knowledge: Mark the Correct Answer
- (1)
- What is COVID-19 disease?
- I A virus that originated from animals
- II A virus that was engineered in a laboratory
- III An upgraded flu virus
- IV A mutation of the Rubella virus
- (2)
- What are the characteristic signs and symptoms among COVID-19 patients?
- I Sweat, high fever, over-salivation
- II High fever, cough, respiratory distress
- III Elevated blood pressure, runny nose, slow pulse
- IV Decreased blood pressure, shortness of breath, weakness
- (3)
- Which of the following patients need to be in home-quarantine?
- I A person that returned from South Africa two days ago and now has a sore throat
- II A person that stayed at a distance of 5 m for 10 min from a confirmed COVID-19 patient
- III A person that returned from Thailand a week ago and now has a high fever and shortness of breath
- IV A patient that stayed in home-quarantine for 14 days, and a week after the end of the quarantine started to have a high fever and running nose
- (4)
- Which of the following activities contributes to the transmission of the COVID-19 virus?
- I Use of a surgical mask
- II Frequent washing of hands in soap and water
- III Use of common objects such as food utensils
- IV Isolation according to Ministry of Health’s regulations
- 2.
- Perceived KnowledgeTable A1. Perceived knowledge.
Item 1 = Completely
Disagree2 = Disagree 3 = Neutral 4 = Agree 5 =
Completely AgreeI am familiar with the guidelines of the Ministry of Health for preventing infection with COVID-19 1 2 3 4 5 I am familiar with the ways of transmitting and being infected with COVID-19 1 2 3 4 5 I feel uncertainty about everything related to COVID-19 1 2 3 4 5 I know the signs and symptoms of COVID-19 disease 1 2 3 4 5 I know who to approach upon suspected infection with COVID-19 1 2 3 4 5 I know what to do upon suspected infection with COVID-19 1 2 3 4 5 I know how to behave during home-isolation resulting from suspected exposure to COVID-19 1 2 3 4 5 - 3.
- Personal Resilience—This Tool is Protected by Copyright (CD-RISC ©2013) and Thus is Not Displayed
- 4.
- Perceived Safety
- 5.
- Practices
- 6.
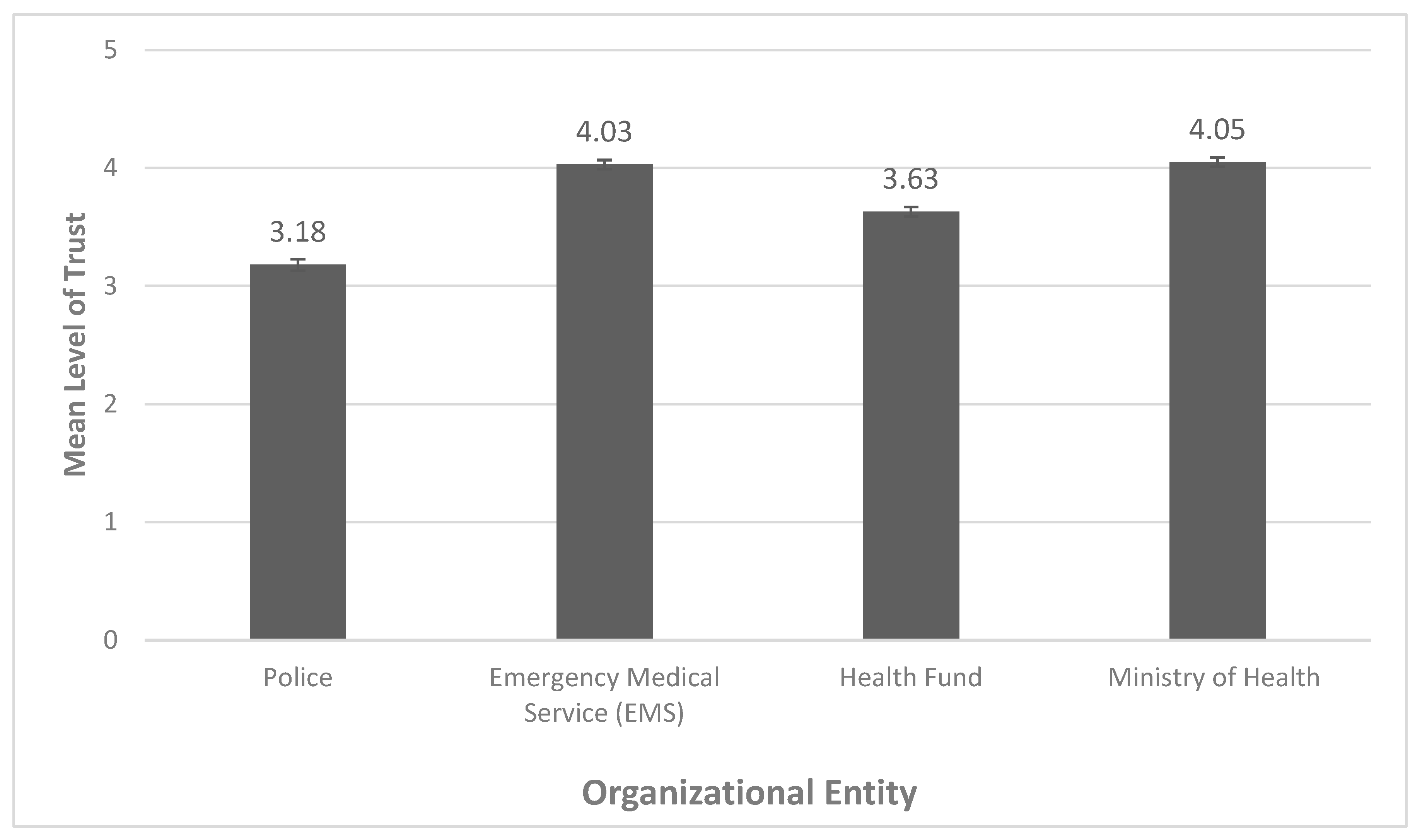
- Trust in authorities
- 7.
- Demographics
- Gender:
- 1.1
- Male
- 1.2
- Female
- 1.3
- Other
- Year of birth: ___________
- Area of residence: ______________
- Marital status:
- 4.1
- In a relationship without children
- 4.2
- In a relationship with children
- 4.3
- Not in a relationship without children
- 4.4
- Not in a relationship with children
- Number of children under 18 that reside with you at home: ____________
- Number of dependent adults (over 18) that reside with you at home: ____________
- What is your level of education?
- 7.1
- Up to 8 years of education
- 7.2
- Up to 12 years of education
- 7.3
- Vocational
- 7.4
- Academic
- Level of religiosity:
- 8.1
- Secular
- 8.2
- Traditional
- 8.3
- Religious
- 8.4
- Ultra-religious
- Level of income:
- 9.1
- Below mean
- 9.2
- Mean
- 9.3
- Above mean
- 9.4
- Refuse to answer
- Do you personally know a person diagnosed with COVID-19?

{kind=link}
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Working Group for NCIP Epidemic Response; Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liuxingbingxue Zazhi 2020, 41, 145–151. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. J. Am. Med. Assoc. 2020, 323, 1061. [Google Scholar] [CrossRef]
- COVID-19 Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 23 May 2020).
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 19 June 2020).
- Smith, R.D. Responding to global infectious disease outbreaks: Lessons from SARS on the role of risk perception, communication and management. Soc. Sci. Med. 2006, 63, 3113–3123. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, 27. [Google Scholar] [CrossRef]
- Tognotti, E. Lessons from the History of Quarantine, from Plague to Influenza A. Emerg. Infect. Dis. 2013, 19, 254–259. [Google Scholar] [CrossRef]
- WHO. Managing Epidemics: Key Facts about Major Deadly Diseases; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241565530. [Google Scholar]
- Ahmed, F.; Zviedrite, N.; Uzicanin, A. Effectiveness of workplace social distancing measures in reducing influenza transmission: A systematic review. BMC Public Health 2018, 18, 518. [Google Scholar] [CrossRef]
- Fung, I.C.-H.; Cairncross, S. Effectiveness of handwashing in preventing SARS: A review. Trop. Med. Int. Health 2006, 11, 1749–1758. [Google Scholar] [CrossRef]
- Kitagawa, K. Questioning “integrated” disaster risk reduction and “all of society” engagement: Can “preparedness pedagogy” help? Comp. A J. Comp. Int. Educ. 2018, 49, 851–867. [Google Scholar] [CrossRef]
- Chan, S.S.C.; So, W.K.W.; Wong, D.C.; Lee, A.C.; Tiwari, A. Improving older adults’ knowledge and practice of preventive measures through a telephone health education during the SARS epidemic in Hong Kong: A pilot study. Int. J. Nurs. Stud. 2007, 44, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.; Mossad, S.B.; Taksler, G.B.; Emery, J.; Schramm, S.; Rothberg, M.B. Impact of Video Education on Influenza Vaccination in Pregnancy. J. Reprod. Med. 2015, 60, 471–479. [Google Scholar] [PubMed]
- Al-Mohrej, A.; Agha, S. Are Saudi medical students aware of middle east respiratory syndrome coronavirus during an outbreak? J. Infect. Public Health 2017, 10, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Maslen, S.; Hayes, J. Preventing black swans: Incident reporting systems as collective knowledge management. J. Risk Res. 2016, 19, 1246–1260. [Google Scholar] [CrossRef]
- Goni, M.D.; Hasan, H.; Naing, N.N.; Wan-Arfah, N.; Deris, Z.Z.; Arifin, W.N.; Baaba, A.A.; Goni; Arfah, W. Assessment of Knowledge, Attitude and Practice towards Prevention of Respiratory Tract Infections among Hajj and Umrah Pilgrims from Malaysia in 2018. Int. J. Environ. Res. Public Health 2019, 16, 4569. [Google Scholar] [CrossRef] [PubMed]
- Noé, A.; Ribeiro, R.M.; Anselmo, R.; Maixenchs, M.; Sitole, L.; Munguambe, K.; Blanco, S.; Le Souëf, P.; García-Basteiro, A.L. Knowledge, attitudes and practices regarding tuberculosis care among health workers in Southern Mozambique. BMC Pulm. Med. 2017, 17, 2. [Google Scholar] [CrossRef]
- Paton, D.; Johnston, D. Disaster Resilience: An. Integrated Approach, 2nd ed.; Charles, C., Ed.; Thomas Publisher: Springfield, Illinois, USA, 2017; ISBN 9780398091699. [Google Scholar]
- Lopes, R. Community disaster education. In Proceedings of the Planning for Earthquakes in New Zealand Conference, IRL Conference Centre, Gracefield, Lower Hutt: Insitute of Geological and Nuclear Sciences, Gracefield, Canada, February 2000. [Google Scholar]
- Ainuddin, S.; Routray, J.K. Community resilience framework for an earthquake prone area in Baluchistan. Int. J. Disaster Risk Reduct. 2012, 2, 25–36. [Google Scholar] [CrossRef]
- Kupika, O.L.; Gandiwa, E.; Nhamo, G.; Kativu, S. Local Ecological Knowledge on Climate Change and Ecosystem-Based Adaptation Strategies Promote Resilience in the Middle Zambezi Biosphere Reserve, Zimbabwe. Available online: https://www.hindawi.com/journals/scientifica/2019/3069254/ (accessed on 19 June 2020).
- Stirling, B.V.; Harmston, J.; Alsobayel, H. An educational programme for nursing college staff and students during a MERS- coronavirus outbreak in Saudi Arabia. BMC Nurs. 2015, 14, 20. [Google Scholar] [CrossRef]
- Masten, A.S.; Obradović, J. Competence and Resilience in Development. Ann. N. Y. Acad. Sci. 2006, 1094, 13–27. [Google Scholar] [CrossRef]
- Becker, J.; Paton, D.; Johnston, D.M.; Ronan, K. Salient Beliefs about Earthquake Hazards and Household Preparedness. Risk Anal. 2013, 33, 1710–1727. [Google Scholar] [CrossRef]
- Jaffe, E.; Aviel, E.; Aharonson-Daniel, L.; Kodinsky, N.; Knobler, H. First Aid Training among Civilians in a Time of War: Gaining Necessary Skills for Coping with Anxiety. Prehospital Disaster Med. 2010, 25, S72–S73. [Google Scholar] [CrossRef]
- Hays, R.D.; Liu, H.; Kapteyn, A. Use of Internet panels to conduct surveys. Behav. Res. Methods 2015, 47, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.E.; Ruiter, R.A.C.; Markham, C.M.; Kok, G. Theory and evidence-based health promotion program planning: Intervention mapping. Front. Public Health 2019, 7, 209. [Google Scholar] [CrossRef] [PubMed]
- Brame, C.J. Effective Educational Videos: Principles and Guidelines for Maximizing Student Learning from Video Content. CBE Life Sci. Educ. 2016, 15, es6. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, S.; Vigoda-Gadot, E.; Cohen, N. Drivers of trust in emergency organizations networks: The role of readiness, threat perceptions and participation in decision making. Public Manag. Rev. 2019, 22, 1–21. [Google Scholar] [CrossRef]
- Drury, J.; Carter, H.; Cocking, C.; Ntontis, E.; Guven, S.T.; Amlôt, R. Facilitating Collective Psychosocial Resilience in the Public in Emergencies: Twelve Recommendations Based on the Social Identity Approach. Front. Public Health 2019, 7, 141. [Google Scholar] [CrossRef]
- Rice, V.; Liu, B. Personal resilience and coping with implications for work. Part I: A review. Work 2016, 54, 325–333. [Google Scholar] [CrossRef]
- Rosenbloom, T.; Perlman, A. Personal resilience, discipline and safety of military drivers. Transp. Res. Part. F: Traffic Psychol. Behav. 2016, 41, 66–73. [Google Scholar] [CrossRef]
- Crane, M.F.; Brabazon, G.; Gucciardi, D.F.; Loveday, T.; Wiggins, M. General Self-Efficacy and Psychological Resilience Promote Skill Acquisition Rate under Psychological Pressure. Australas. J. Organ. Psychol. 2017, 10, 10. [Google Scholar] [CrossRef]
- Bodas, M.; Peleg, K.; Shenhar, G.; Adini, B. Light search and rescue training of high school students in Israel—Longitudinal study of effect on resilience and self-efficacy. Int. J. Disaster Risk Reduct. 2019, 36, 101089. [Google Scholar] [CrossRef]
- Bateman, J.M.; Edwards, B. Gender and Evacuation: A Closer Look at Why Women Are More Likely to Evacuate for Hurricanes. Nat. Hazards Rev. 2002, 3, 107–117. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. What predicts psychological resilience after disaster? The role of demographics, resources, and life stress. J. Consult. Clin. Psychol. 2007, 75, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Burkam, D.; Lee, V. Inequality at the Starting Gate: Social Background Differences in Achievement as Children Begin School; Economic Policy Institute: Washington, DC, USA, 2002. [Google Scholar]
- Schaap, D.P. The Police, the Public, and the Pursuit of Trust. A Cross-National, Dynamic Study of Trust in the Police and Police Trust Building; Den Haag: Eleven International Publishing: Hague, Netherlands, 2018. [Google Scholar]
- Adini, B.; Peleg, K.; Amelung, V.; Stein, V.; Goodwin, N.; Balicer, R.; Nolte, E.; Suter, E. Integrated Care Concerning Mass Casualty Incidents/Disasters: Lessons Learned from Implementation in Israel. In Handbook Integrated Care; Springer Science and Business Media LLC: Cham, Switzerland, 2017; pp. 439–448. [Google Scholar]
- Tiargan-Orr, R.; Eran-Jona, M. The Israeli public’s perception of the IDF: Stability and change. Armed Forces Soc. 2016, 42, 324–343. [Google Scholar] [CrossRef]
- Zakrison, T.L.; Hamel, P.A.; Hwang, S.W. Homeless people’s trust and interactions with police and paramedics. J. Hered. 2004, 81, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Bodas, M.; Peleg, K. Self-Isolation Compliance in the COVID-19 Era Influenced By Compensation: Findings from a Recent Survey in Israel. Health Aff. 2020, 39, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Condon, B.J.; Sinha, T. Who is that masked person: The use of face masks on Mexico City public transportation during the Influenza A (H1N1) outbreak. Health Policy 2010, 95, 50–56. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Ng, M.W.; Fielding, R. Situational Awareness and Health Protective Responses to Pandemic Influenza A (H1N1) in Hong Kong: A Cross-Sectional Study. PLoS ONE 2010, 5, e13350. [Google Scholar] [CrossRef]
- Agüero, F.; Adell, M.N.; Pérez-Giménez, A.; Medina, M.J.L.; García-Continente, X. Adoption of preventive measures during and after the 2009 influenza A (H1N1) virus pandemic peak in Spain. Prev. Med. 2011, 53, 203–206. [Google Scholar] [CrossRef]
- Sim, K.; Chua, H.C.; Vieta, E.; Fernandez, G. The anatomy of panic buying related to the current COVID-19 pandemic. Psychiatry Res. Neuroimaging 2020, 288, 113015. [Google Scholar] [CrossRef]

| Characteristic | Number (Percentage) N = 501 |
|---|---|
| Age | |
| 18–21 | 53 (10.6%) |
| 22–40 | 209 (41.7%) |
| 41–60 | 176 (35.1%) |
| 60–70 | 63 (12.6%) |
| Gender | |
| Male | 253 (50.5%) |
| Female | 248 (49.5%) |
| Religiosity | |
| Secular | 214 (42.7%) |
| Traditional | 184 (36.7%) |
| Religious | 53 (10.8%) |
| Ultra-religious | 48 (9.8%) |
| Education (in years) | |
| <12 years | 139 (27.7%) |
| Vocational (non-academic) | 102 (20.4%) |
| Academic | 260 (51.9%) |
| Area of residence | |
| North (from Haifa) | 132 (26.3%) |
| Central area | 206 (40.1%) |
| Jerusalem area | 55 (11%) |
| Southern area | 108 (21.6%) |
| Level of income * | |
| Much below mean | 56 (11.2%) |
| Below mean | 77 (15.4%) |
| Mean | 133 (26.5%) |
| Above mean | 138 (27.5%) |
| Much above mean | 44 (8.8%) |
| Refuse to answer | 53 (10.6%) |
| Marital status | |
| In a relationship without children | 107 (21.4%) |
| In a relationship with children | 254 (50.7%) |
| Not in a relationship, without children | 107 (21.4%) |
| Not in a relationship, with children | 33 (6.6%) |
| Variable | T1 | T2 | % Change | Effect Size * (Cohen’s d) ** | p-Value |
|---|---|---|---|---|---|
| Knowledge score | 3.21 ± 0.78 3.0 (3.0–4.0) | 3.46 ± 0.70 4.0 (3.0–4.0) | 7.8% | 0.34 | <0.001 |
| Knowledge perception | 4.06 ± 0.51 4.0 (3.7–4.4) | 4.28 ± 0.45 4.4 (4.0–4.6) | 5.4% | 0.44 | <0.001 |
| Perceived safety | 2.58 ± 1.15 2.0 (2.0–3.0) | 2.90 ± 1.16 3.0 (2.0–4.0) | 12.4% | 0.28 | <0.001 |
| Perceived personal resilience | 3.51 ± 0.69 3.5 (3.1–4.0) | 3.59 ± 0.76 3.7 (3.1–4.0) | 2.5% | 0.11 | <0.001 |
| Variable | Personal Resilience | Knowledge Score | Perceived Safety |
|---|---|---|---|
| T1 | |||
| Knowledge score | r = 0.062 p = 0.167 | r = − 0.073 p = 0.103 | |
| Perceived knowledge | r = 0.278 p < 0.001 | r = 0.121 p = 0.007 | r = 0.082 p = 0.067 |
| Personal resilience | r = −0.167 p = 0.501 | r = 0.402 p < 0.001 | |
| T2 | |||
| Personal Resilience | Knowledge Score | Perceived Safety | |
| Knowledge score | r = −0.050 p = 0.261 | r = −0.86 p = 0.054 | |
| Perceived knowledge | r = 0.238 p < 0.001 | r = 0.098 p = 0.029 | r = 0.147 p = 0.001 |
| Personal resilience | r = − 0.050 p = 0.261 | r = 0.469 p < 0.001 |
| Compared Entities | Significance |
|---|---|
| Police vs. Emergency Medical Services | p < 0.01 |
| Police vs. Health Fund | p < 0.01 |
| Police vs. Ministry of Health | p < 0.01 |
| Emergency Medical Services vs. Health Fund | p < 0.01 |
| Emergency Medical Services vs. Ministry of Health | p = 0.32 |
| Health Fund vs. Ministry of Health | p < 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaim, A.; Jaffe, E.; Siman-Tov, M.; Khairish, E.; Adini, B. Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis. Int. J. Environ. Res. Public Health 2020, 17, 5971. https://doi.org/10.3390/ijerph17165971
Kaim A, Jaffe E, Siman-Tov M, Khairish E, Adini B. Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis. International Journal of Environmental Research and Public Health. 2020; 17(16):5971. https://doi.org/10.3390/ijerph17165971
Chicago/Turabian StyleKaim, Arielle, Eli Jaffe, Maya Siman-Tov, Ella Khairish, and Bruria Adini. 2020. "Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis" International Journal of Environmental Research and Public Health 17, no. 16: 5971. https://doi.org/10.3390/ijerph17165971
APA StyleKaim, A., Jaffe, E., Siman-Tov, M., Khairish, E., & Adini, B. (2020). Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis. International Journal of Environmental Research and Public Health, 17(16), 5971. https://doi.org/10.3390/ijerph17165971