Effects of Time-Restricted Feeding during Ramadan on Dietary Intake, Body Composition and Metabolic Outcomes


Abstract
1. Introduction
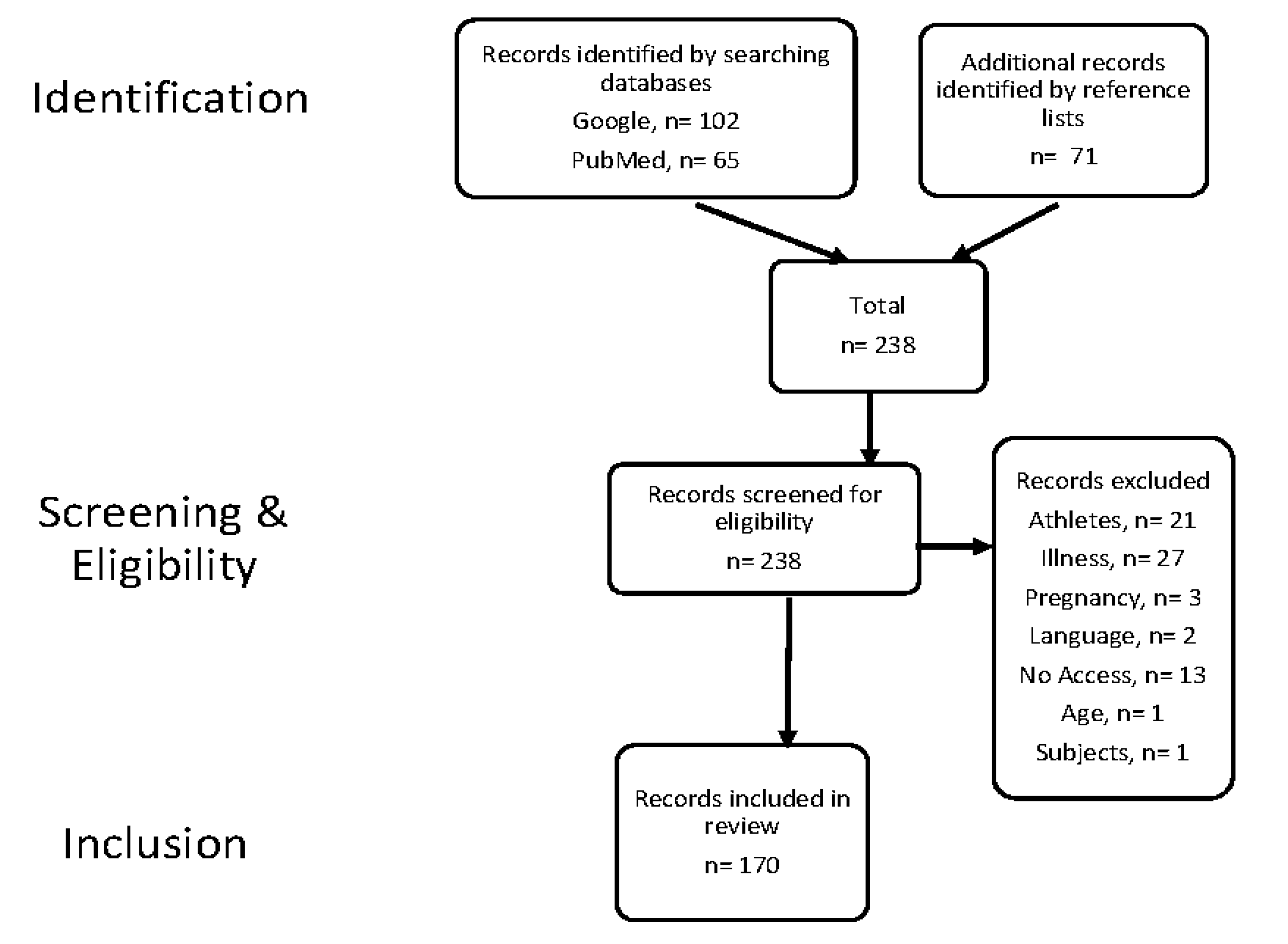
2. Materials and Methods
3. Changes in Dietary Intake
3.1. Fluid Intake
3.2. Food Intake Pattern
3.3. Macronutrient and Energy Intake
4. Changes in Body Composition
4.1. Normal Weight
4.2. Overweight and Obese
5. Metabolic Parameters
5.1. Glucose Homeostasis
5.2. Lipid Profile
Overweight and Obese
6. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Meo, S.A.; Hassan, A. Physiological changes during fasting in Ramadan. J. Pak. Med. Assoc. 2015, 65, S6–S14. [Google Scholar]
- Dikensoy, E.; Balat, O.; Cebesoy, B.; Ozkur, A.; Cicek, H.; Can, G. The effect of Ramadan fasting on maternal serum lipids, cortisol levels and fetal development. Arch. Gynecol. Obstet. 2009, 279, 119. [Google Scholar] [CrossRef]
- Prior, R. Ramadan: A History. CNN. 2019. Available online: https://edition.cnn.com/2019/05/05/world/history-of-ramadan-trnd/index.html (accessed on 24 July 2020).
- Baines, W. The Origins of Ramadan. Available online: https://www.beliefnet.com/faiths/islam/the-origins-of-ramadan.aspx (accessed on 24 July 2020).
- Alkandari, J.R.; Maughan, R.J.; Roky, R.; Aziz, A.R.; Karli, U. The implications of Ramadan fasting for human health and well-being. J. Sports Sci. 2012, 30, S9–S19. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef]
- Chaix, A.; Zarrinpar, A.; Miu, P.; Panda, S. Time-restricted feeding is a preventative and therapeutic intervention against diverse nutritional challenges. Cell Metab. 2014, 20, 991–1005. [Google Scholar] [CrossRef]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-restricted feeding and risk of metabolic disease: A review of human and animal studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef]
- Trepanowski, J.F.; Bloomer, R.J. The impact of religious fasting on human health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef]
- Ibrahim, N.S.I.; Hardinsyah, H.; Setiawan, B. Hydration status and liver function of young men before and after Ramadan fasting. J. Gizi Dan Pangan 2018, 13, 33–38. [Google Scholar] [CrossRef]
- Mustafa, K.; Mahmoud, N.; Gumaa, K.; Gader, A. The effects of fasting in Ramadan: 2. Fluid and electrolyte balance. Br. J. Nutr. 1978, 40, 583–589. [Google Scholar] [CrossRef]
- Leiper, J.B.; Molla, A. Effects on health of fluid restriction during fasting in Ramadan. Eur. J. Clin. Nutr. 2003, 57, S30–S38. [Google Scholar] [CrossRef]
- Hosseini, S.R.A.; Sardar, M.A.; Hejazi, K.; Farahati, S. The effect of Ramadan fasting and physical activity on body composition, serum osmolarity levels and some parameters of electrolytes in females. Int. J. Endocrinol. Metab. 2013, 11, 88. [Google Scholar]
- Dikme, O.; Fasting, D.O.R. Its influence on serum osmolality in emergency patients. J. Emerg Med. Crit. Care 2016, 2, 4. [Google Scholar]
- Trabelsi, K.; El Abed, K.; Trepanowski, J.F.; Stannard, S.R.; Ghlissi, Z.; Ghozzi, H.; Masmoudi, L.; Jammoussi, K.; Hakim, A. Effects of Ramadan fasting on biochemical and anthropometric parameters in physically active men. Asian J. Sports Med. 2011, 2, 134. [Google Scholar] [CrossRef] [PubMed]
- Azwany, N.; Aziz, A.; Mohammad, W. The Impact of ramadan fasting on hydration status of type 2 diabetics in kubang kerian, kelantan. J. Kesihat. Masy. 2004, 10, 31–34. [Google Scholar]
- Bouhlel, E.; Denguezli, M.; Zaouali, M.; Tabka, Z.; Shephard, R.J. Ramadan fasting’s effect on plasma leptin, adiponectin concentrations, and body composition in trained young men. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 617–627. [Google Scholar] [CrossRef]
- Ramadan, J.; Telahoun, G.; Al-Zaid, N.S.; Barac-Nieto, M. Responses to exercise, fluid, and energy balances during Ramadan in sedentary and active males. Nutrition 1999, 15, 735–739. [Google Scholar] [CrossRef]
- Abushady, M.; Samy, M.; Bekhet, M.; Abdullah, A. Effect of Ramadan fasting on renal function in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2019, 153, 176–183. [Google Scholar] [CrossRef]
- Shao, Y.; Lim, G.J.; Chua, C.L.; Wong, Y.F.; Yeoh, E.C.K.; Low, S.K.M.; Sum, C.F. The effect of Ramadan fasting and continuing sodium-glucose co-transporter-2 (SGLT2) inhibitor use on ketonemia, blood pressure and renal function in Muslim patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2018, 142, 85–91. [Google Scholar] [CrossRef]
- NasrAllah, M.M.; Osman, N.A. Fasting during the month of Ramadan among patients with chronic kidney disease: Renal and cardiovascular outcomes. Clin. Kidney J. 2014, 7, 348–353. [Google Scholar] [CrossRef]
- Alawadi, F.; Rashid, F.; Bashier, A.; Abdelgadir, E.; Al Saeed, M.; Abuelkheir, S.; Khalifa, A.; Bachet, F.; Elsayed, M.; Abdallah, K. The use of Free Style Libre Continues Glucose Monitoring (FSL-CGM) to monitor the impact of Ramadan fasting on glycemic changes and kidney function in high-risk patients with diabetes and chronic kidney disease stage 3 under optimal diabetes care. Diabetes Res. Clin. Pract. 2019, 151, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Eldeeb, A.A.; Mahmoud, M.A.; Ibrahim, A.B.; Yousef, E.A.; Sabry, A.A. Effect of Ramadan fasting on arterial stiffness parameters among Egyptian hypertensive patients with and without chronic kidney disease. Saudi J. Kidney Dis. Transplant. 2020, 31, 582. [Google Scholar]
- Al-Hourani, H.; Atoum, M. Body composition, nutrient intake and physical activity patterns in young women during Ramadan. Singap. Med. J. 2007, 48, 906. [Google Scholar]
- Foundation, B.N. Traditional Ramadan Foods from around the World. Available online: https://www.nutrition.org.uk/healthyliving/seasons/ramadan.html?start=1 (accessed on 26 February 2020).
- Bakhotmah, B.A. The puzzle of self-reported weight gain in a month of fasting (Ramadan) among a cohort of Saudi families in Jeddah, Western Saudi Arabia. Nutr. J. 2011, 10, 84. [Google Scholar] [CrossRef]
- Ali, Z.; Abizari, A.-R. Ramadan fasting alters food patterns, dietary diversity and body weight among Ghanaian adolescents. Nutr. J. 2018, 17, 75. [Google Scholar] [CrossRef]
- Pirsaheb, S.; Pasdar, Y.; Navabi, S.J.; Rezaei, M.; Darbandi, M.; Niazi, P. Fasting consequences during Ramadan on lipid profile and dietary patterns. J. Nutr. Fasting Health 2013, 1, 6–12. [Google Scholar]
- Rahman, M.; Rashid, M.; Basher, S.; Sultana, S.; Nomani, M. Improved serum HDL cholesterol profile among Bangladeshi male students during Ramadan fasting. EMHJ East. Mediterr. Health J. 2004, 10, 131–137. [Google Scholar]
- El Ati, J.; Beji, C.; Danguir, J. Increased fat oxidation during Ramadan fasting in healthy women: An adaptative mechanism for body-weight maintenance. Am. J. Clin. Nutr. 1995, 62, 302–307. [Google Scholar] [CrossRef]
- Sweileh, N.; Schnitzler, A.; Hunter, G.; Davis, B. Body composition and energy metabolism in resting and exercising muslims during Ramadan fast. J. Sports Med. Phys. Fit. 1992, 32, 156–163. [Google Scholar]
- Frost, G.; Pirani, S. Meal frequency and nutritional intake during Ramadan: A pilot study. Hum. Nutrition. Appl. Nutr. 1987, 41, 47–50. [Google Scholar]
- Yeoh, E.; Zainudin, S.B.; Loh, W.N.; Chua, C.L.; Fun, S.; Subramaniam, T.; Sum, C.F.; Lim, S.C. Fasting during Ramadan and associated changes in glycaemia, caloric intake and body composition with gender differences in Singapore. Ann. Acad. Med. Singap. 2015, 44, 202–206. [Google Scholar] [PubMed]
- Lamine, F.; Bouguerra, R.; Jabrane, J.; Marrakchi, Z.; Ben, M.R.; Ben, C.S.; Gaigi, S. Food intake and high density lipoprotein cholesterol levels changes during ramadan fasting in healthy young subjects. La Tunis. Médicale 2006, 84, 647–650. [Google Scholar]
- Sadiya, A.; Ahmed, S.; Siddieg, H.H.; Babas, I.J.; Carlsson, M. Effect of Ramadan fasting on metabolic markers, body composition, and dietary intake in Emiratis of Ajman (UAE) with metabolic syndrome. Diabetes Metab. Syndr. Obes. 2011, 4, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Bouhlel, E.; Salhi, Z.; Bouhlel, H.; Mdella, S.; Amamou, A.; Zaouali, M.; Mercier, J.; Bigard, X.; Tabka, Z.; Zbidi, A. Effect of Ramadan fasting on fuel oxidation during exercise in trained male rugby players. Diabetes Metab. 2006, 32, 617–624. [Google Scholar] [CrossRef]
- Poh, B.; Zawiah, H.; Ismail, M.; Henry, C. Changes in body weight, dietary intake and activity pattern of adolescents during Ramadan. Malays. J. Nutr. 1996, 2, 1–10. [Google Scholar]
- Suriani, I.; Shamsuddin, K.; Abdul Latif, K.; Saad, H.A. The effect of the Malaysian Food Guideline guidance on a group of overweight and obese women during Ramadan. Saudi Med. J. 2015, 36, 40–45. [Google Scholar] [CrossRef]
- Savas, E.; Öztürk, Z.A.; Tanrıverdi, D.; Kepekçi, Y. Do Ramadan fasting restrictions alter eating behaviours in obese women? J. Relig. Health 2014, 53, 135–140. [Google Scholar] [CrossRef]
- Khaled, B.M.; Belbraouet, S. Effect of Ramadan fasting on anthropometric parameters and food consumption in 276 type 2 diabetic obese women. Int. J. Diabetes Dev. Ctries. 2009, 29, 62. [Google Scholar] [CrossRef]
- Karaagaoglu, N.; Yucecan, S. Some behavioral changes observed among fasting subjects, their nutritional habits and energy expenditure in Ramadan. Int. J. Food Sci. Nutr. 2000, 51, 125. [Google Scholar]
- Khattak, M.M.A.K.; Mamat, N.M.; Bakar, W.A.M.A.; Shaharuddin, M.F.N. Does religious fasting affect energy and macro-nutrients intakes? Nutr. Food Sci. 2013, 43, 254–260. [Google Scholar] [CrossRef]
- Adlouni, A.; Ghalim, N.; Benslimane, A.; Lecerf, J.M.; Saïle, R. Fasting during Ramadan induces a marked increase in high-density lipoprotein cholesterol and decrease in low-density lipoprotein cholesterol. Ann. Nutr. Metab. 1997, 41, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Aksungar, F.B.; Eren, A.; Ure, S.; Teskin, O.; Ates, G. Effects of intermittent fasting on serum lipid levels, coagulation status and plasma homocysteine levels. Ann. Nutr. Metab. 2005, 49, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Shalaei, N.; Motaghedi Larijani, A.; Mohajeri, S.A.R.; Norouzy, A.; Nematy, M.; Sheikhol Vaezin, F.; Jahandoost, F.; Safarian, M. Changes in dietary intake during Ramadan in north east of Iran population. J. Fasting Health 2013, 1, 19–22. [Google Scholar]
- Adlouni, A.; Ghalim, N.; Saïle, R.; Hda, N.; Parra, H.-J.; Benslimane, A. Beneficial effect on serum apo AI, apo B and Lp AI levels of Ramadan fasting. Clin. Chim. Acta 1998, 271, 179–189. [Google Scholar] [CrossRef]
- Hozoori, M.; Kohandani, A.; Mohammadi Veldani, A.; Mirizadeh, M. Nutrient intake during Ramadan in fasting people referring to health centers in Qom, Iran. Health Spiritual. Med. Ethics 2017, 4, 9–11. [Google Scholar]
- Husain, R.; Duncan, M.; Cheah, S.; Ch’Ng, S. Effects of fasting in Ramadan on tropical Asiatic Moslems. Br. J. Nutr. 1987, 58, 41–48. [Google Scholar] [CrossRef]
- Fakhrzadeh, H.; Lariiani, B.; Sanjari, M.; Baradar-Jalili, R.; Amini, M. Effect of Ramadan fasting on clinical and biochemical parameters in healthy adults. Ann. Saudi Med. 2003, 23, 223–226. [Google Scholar] [CrossRef]
- López-Bueno, M.; González-Jiménez, E.; Navarro-Prado, S.; Montero-Alonso, M.A.; Schmidt-RioValle, J. Influence of age and religious fasting on the body composition of Muslim women living in a westernized context. Nutr. Hosp. 2015, 31, 1067–1073. [Google Scholar]
- Norouzy, A.; Salehi, M.; Philippou, E.; Arabi, H.; Shiva, F.; Mehrnoosh, S.; Mohajeri, S.M.; Mohajeri, S.A.; Motaghedi Larijani, A.; Nematy, M. Effect of fasting in Ramadan on body composition and nutritional intake: A prospective study. J Hum Nutr Diet 2013, 26 Suppl 1, 97–104. [Google Scholar] [CrossRef]
- Sezen, Y.; Altiparmak, I.H.; Erkus, M.E.; Kocarslan, A.; Kaya, Z.; Gunebakmaz, O.; Demirbag, R. Effects of Ramadan fasting on body composition and arterial stiffness. J. Pak. Med. Assoc. 2016, 66, 1522–1527. [Google Scholar]
- Shruthi, B.; Abrar, H.; Reddy, B. The effect of Ramadan fasting on the body composition, blood pressure, heart rate of healthy young adults. Int. J. Recent Trends Sci. Technol. 2013, 8, 31–35. [Google Scholar]
- Syam, A.F.; Sobur, C.S.; Abdullah, M.; Makmun, D. Ramadan fasting decreases body fat but not protein mass. Int. J. Endocrinol. Metab. 2016, 14, e29687. [Google Scholar]
- Nomani, M.; Hallak, M.; Siddiqui, I. Effects of Ramadan fasting on plasma uric acid and body weight in healthy men. J. Am. Diet. Assoc. 1990, 90, 1435–1436. [Google Scholar] [PubMed]
- Nachvak, S.M.; Pasdar, Y.; Pirsaheb, S.; Darbandi, M.; Niazi, P.; Mostafai, R.; Speakman, J.R. Effects of Ramadan on food intake, glucose homeostasis, lipid profiles and body composition composition. Eur. J. Clin. Nutr. 2019, 73, 594–600. [Google Scholar] [CrossRef]
- Harder-Lauridsen, N.M.; Rosenberg, A.; Benatti, F.B.; Damm, J.A.; Thomsen, C.; Mortensen, E.L.; Pedersen, B.K.; Krogh-Madsen, R. Ramadan model of intermittent fasting for 28 d had no major effect on body composition, glucose metabolism, or cognitive functions in healthy lean men. Nutrition 2017, 37, 92–103. [Google Scholar] [CrossRef]
- Ramadan, J. Does fasting during Ramadan alter body composition, blood constituents and physical performance? Med. Princ. Pr. 2002, 11 (Suppl 2), 41–46. [Google Scholar] [CrossRef]
- Racinais, S.; Périard, J.; Li, C.; Grantham, J. Activity patterns, body composition and muscle function during Ramadan in a Middle-East Muslim country. Int. J. Sports Med. 2012, 33, 641–646. [Google Scholar] [CrossRef]
- Finch, G.M.; Day, J.E.; Welch, D.A.; Rogers, P.J. Appetite changes under free-living conditions during Ramadan fasting. Appetite 1998, 31, 159–170. [Google Scholar] [CrossRef]
- Mazidi, M.; Karimi, E.; Rezaee, P.; Nematy, M.; Salehi, M. The effects of Ramadan fasting on body composition. Shiraz E Med. J. 1973, 15, e19733. [Google Scholar] [CrossRef]
- Al-Numair, K. Body weight and some biochemical changes associated with Ramadan fasting in healthy Saudi men. J. Med. Sci. 2006, 6, 112–116. [Google Scholar]
- Shehab, A.; Abdulle, A.; El Issa, A.; Al Suwaidi, J.; Nagelkerke, N. Favorable changes in lipid profile: The effects of fasting after Ramadan. PLoS ONE 2012, 7, e47615. [Google Scholar] [CrossRef] [PubMed]
- Jahrami, H.A.; Alsibai, J.; Clark, C.C.; Mo’ez Al-Islam, E.F. A systematic review, meta-analysis, and meta-regression of the impact of diurnal intermittent fasting during Ramadan on body weight in healthy subjects aged 16 years and above. Eur. J. Nutr. 2020, 59, 2291–2316. [Google Scholar] [CrossRef] [PubMed]
- Fernando, H.A.; Zibellini, J.; Harris, R.A.; Seimon, R.V.; Sainsbury, A. Effect of Ramadan fasting on weight and body composition in healthy non-athlete adults: A systematic review and meta-analysis. Nutrients 2019, 11, 478. [Google Scholar] [CrossRef] [PubMed]
- Hajek, P.; Myers, K.; Dhanji, A.-R.; West, O.; McRobbie, H. Weight change during and after Ramadan fasting. J. Public Health 2011, 34, 377–381. [Google Scholar] [CrossRef]
- Sadeghirad, B.; Motaghipisheh, S.; Kolahdooz, F.; Zahedi, M.J.; Haghdoost, A.A. Islamic fasting and weight loss: A systematic review and meta-analysis. Public Health Nutr. 2014, 17, 396–406. [Google Scholar] [CrossRef]
- Kocaaga, T.; Tamer, K.; Karli, U.; Yarar, H. Effects of Ramadan fasting on physical activity level and body composition in young males. Int. J. Appl. Exerc. Phy. 2019, 8, 2322–3537. [Google Scholar]
- Amiri, F.; Azimi Nezhad, M.; Alinezhad-Namaghi, M.; Jarahi, L.; Nematy, M.; Norouzy, A. Effects of Ramadan fasting on inflammatory biomarkers and body composition in healthy subjects. J. Nutr. Fasting Health 2016, 4, 136–139. [Google Scholar]
- Al-barha, N.S.; Aljaloud, K.S. The effect of Ramadan fasting on body composition and metabolic syndrome in apparently healthy men. Am. J. Men’s Health 2019, 13, 1557988318816925. [Google Scholar] [CrossRef]
- Khaled, T.; Ahmed, C.; Zohra, G.; Choumous, K.; Zouheir, S.; Mounir, Z.K.; Ahmed, H. Physical activity during Ramadan fasting: Effects on body composition, hematological and biochemical parameters. Iosr J. Pharm. 2012, 2, 33–41. [Google Scholar] [CrossRef]
- Trabelsi, K.; El Abed, K.; Stannard, S.R.; Jammoussi, K.; Zeghal, K.M.; Hakim, A. Effects of fed-versus fasted-state aerobic training during Ramadan on body composition and some metabolic parameters in physically active men. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 11–18. [Google Scholar] [CrossRef]
- Haghdoost, A.; Poorranjbar, M. The interaction between physical activity and fasting on the serum lipid profile during Ramadan. Singap. Med. J. 2009, 50, 897–901. [Google Scholar]
- Yucel, A.; Degirmenci, B.; Acar, M.; Albayrak, R.; Haktanir, A. The effect of fasting month of Ramadan on the abdominal fat distribution: Assessment by computed tomography. Tohoku J. Exp. Med. 2004, 204, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Khattak, M.M.A.K.; Bakar, I.A.; Yeim, L. Does religious fasting increase fat free mass (FFM) and reduce abdominal obesity? Nutr. Food Sci. 2012, 42, 87–96. [Google Scholar] [CrossRef]
- Khan, A.; Khattak, M. Islamic fasting: An effective strategy for prevention and control of obesity. Pak. J. Nutr. 2002, 1, 185–187. [Google Scholar]
- Rohin, M.A.; Rozano, N.; Abd Hadi, N.; Mat Nor, M.N.; Abdullah, S.; Dandinasivara Venkateshaiah, M. Anthropometry and body composition status during Ramadan among higher institution learning centre staffs with different body weight status. Sci. World J. 2013, 2013, 308041. [Google Scholar] [CrossRef]
- Ünalacak, M.; Kara, I.H.; Baltaci, D.; Erdem, Ö.; Bucaktepe, P.G.E. Effects of Ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab. Syndr. Relat. Disord. 2011, 9, 157–161. [Google Scholar] [CrossRef]
- Celik, A.; Saricicek, E.; Saricicek, V.; Sahin, E.; Ozdemir, G.; Bozkurt, S.; Okumus, M.; Sucakli, M.H.; Cikim, G.; Coskun, Y. Effect of Ramadan fasting on serum concentration of apelin-13 and new obesity indices in healthy adult men. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2014, 20, 337. [Google Scholar]
- Suriani, I.; Shamsuddin, K.; Khalib, A.; Hazizi, A.; Fadlan, M. The effect of Ramadan weight loss on body composition of overweight and obese Muslims in University Putra Malaysia. Int. J. Public Health Clin. Sci. 2015, 2, 61–68. [Google Scholar]
- Madkour, M.I.; Obaideen, A.K.; Dalah, E.Z.; Hasan, H.A.; Radwan, H.; Jahrami, H.A.; Hamdy, O.; Mohammad, M.G. Effect of Ramadan diurnal fasting on visceral adiposity and serum adipokines in overweight and obese individuals. Diabetes Res. Clin. Pract. 2019, 153, 166–175. [Google Scholar]
- Radhakishun, N.N.E. Childhood Obesity: Medical, Cultural and Psychological Factors. Ph.D. Thesis, Utrecht University, Utrecht, The Netherlands, 2014. [Google Scholar]
- Salehi, M.; Neghab, M. Effects of fasting and a medium calorie balanced diet during the holy month Ramadan on weight, BMI and some blood parameters of overweight males. Pak. J. Biol. Sci. 2007, 10, 968–971. [Google Scholar] [CrossRef][Green Version]
- Ganjali, N.; Mozaffari-Khosravi, H.; Afkhami Ardakani, M.; Shahraki, M.; Fallahzadeh, H. Effect of islamic fasting on glucose, lipid profiles and Body Mass Index, adiponectin and leptin in obese individuals. J. Nutr. Fasting Health 2016, 4, 57–63. [Google Scholar]
- Ongsara, S.; Boonpol, S.; Prompalad, N.; Jeenduang, N. The Effect of Ramadan fasting on biochemical parameters in healthy Thai subjects. J. Clin. Diagn Res. 2017, 11, BC14–BC18. [Google Scholar] [CrossRef] [PubMed]
- Larijani, B.; Zahedi, F.; Sanjari, M.; Amini, M.; Jalili, R.; Adibi, H.; Vassigh, A. The effect of Ramadan fasting on fasting serum glucose in healthy adults. Med. J. Malays. 2003, 58, 678–680. [Google Scholar]
- Shariatpanahi, Z.V.; Shariatpanahi, M.V.; Shahbazi, S.; Hossaini, A.; Abadi, A. Effect of Ramadan fasting on some indices of insulin resistance and components of the metabolic syndrome in healthy male adults. Br. J. Nutr. 2008, 100, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Sarraf-Zadegan, N.; Atashi, M.; Naderi, G.A.; Baghai, A.M.; Asgary, S.; Fatehifar, M.R.; Samarian, H.; Zarei, M. The effect of fasting in Ramadan on the values and interrelations between biochemical, coagulation and hematological factors. Ann. Saudi Med. 2000, 20, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Ziaee, V.; Razaei, M.; Ahmadinejad, Z.; Shaikh, H.; Yousefi, R.; Yarmohammadi, L.; Bozorgi, F.; Behjati, M.J. The changes of metabolic profile and weight during Ramadan fasting. Singap. Med. J. 2006, 47, 409. [Google Scholar]
- Azizi, F.; Rasouli, H. Serum glucose, bilirubin, calcium, phosphorus, protein and albumin concentrations during Ramadan. Med. J. Islamic Repub. Iran. 1987, 1, 38–41. [Google Scholar]
- Kiyani, M.M.; Memon, A.R.; Amjad, M.I.; Ameer, M.R.; Sadiq, M.; Mahmood, T. Study of human Biochemical parameters during and after Ramadan. J. Relig. Health 2017, 56, 55–62. [Google Scholar] [CrossRef]
- Beltaifa, L.; Bouguerra, R.; Ben Slama, C.; Jabrane, H.; El Khadhi, A.; Rayana, B.; Doghri, T. Food intake, and anthropometrical and biological parameters in adult Tunisians during Ramadan. EMHJ East. Mediterr. Health J. 2002, 8, 603–611. [Google Scholar]
- Radhakishun, N.; Blokhuis, C.; van Vliet, M.; von Rosenstiel, I.; Weijer, O.; Heymans, M.; Beijnen, J.; Brandjes, D.; Diamant, M. Intermittent fasting during Ramadan causes a transient increase in total, LDL, and HDL cholesterols and hs-CRP in ethnic obese adolescents. Eur. J. Pediatrics 2014, 173, 1103–1106. [Google Scholar] [CrossRef]
- Roky, R.; Houti, I.; Moussamih, S.; Qotbi, S.; Aadil, N. Physiological and chronobiological changes during Ramadan intermittent fasting. Ann. Nutr. Metab. 2004, 48, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.S.; Bandyopadhyay, A. Effect of Ramadan intermittent fasting on haematological parameters, lipid profile, and renal markers in young Muslim males of Kolkata, India. Indian J. Physiol Pharm. 2017, 61, 361–367. [Google Scholar]
- Mendelson, M.; Michallet, A.S.; Monneret, D.; Perrin, C.; Estève, F.; Lombard, P.; Faure, P.; Lévy, P.; Favre-Juvin, A.; Pépin, J.L. Impact of exercise training without caloric restriction on inflammation, insulin resistance and visceral fat mass in obese adolescents. Pediatric Obes. 2015, 10, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.K.; Huggins, C.E.; Bonham, M.P. Effect of meal timing on postprandial glucose responses to a low glycemic index meal: A crossover trial in healthy volunteers. Clin. Nutr. 2019, 38, 465–471. [Google Scholar] [CrossRef]
- Darzabi, T.; Hejazi, K.; Shahrokhi, H. The effects of Ramadan fasting on metabolic syndrome and body composition in male students. J. Client Cent. Nurs. Care 2019, 5, 239–246. [Google Scholar]
- Gnanou, J.V.; Caszo, B.A.; Khalil, K.M.; Abdullah, S.L.; Knight, V.F.; Bidin, M.Z. Effects of Ramadan fasting on glucose homeostasis and adiponectin levels in healthy adult males. J. Diabetes Metab. Disord. 2015, 14, 55. [Google Scholar] [CrossRef]
- Mafauzy, M.; Mohammed, W.; Anum, M.; Zulkifli, A.; Ruhani, A. A study of the fasting diabetic patients during the month of Ramadan. Med. J. Malays. 1990, 45, 14–17. [Google Scholar]
- Lessan, N.; Hannoun, Z.; Hasan, H.; Barakat, M. Glucose excursions and glycaemic control during Ramadan fasting in diabetic patients: Insights from continuous glucose monitoring (CGM). Diabetes Metab. 2015, 41, 28–36. [Google Scholar] [CrossRef]
- Al-Hader, A.F.A.; Abu-Farsakh, N.A.; Khatib, S.Y.; Hasan, Z.A. The effects of Ramadan fasting on certain biochemical parameters in normal subjects and in type II diabetic patients. Ann. Saudi Med. 1994, 14, 139–141. [Google Scholar] [CrossRef]
- Yarahmadi, S.; Larijani, B.; Bastanhagh, M.; Pajouhi, M.; Baradar, R.J.; Zahedi, F.; Zendehdel, K.; Akrami, S. Metabolic and clinical effects of Ramadan fasting in patients with type II diabetes. J. Coll. Physicians Surg. Pak. 2003, 13, 329–332. [Google Scholar]
- Alabbood, M.H.; Ho, K.W.; Simons, M.R. The effect of Ramadan fasting on glycaemic control in insulin dependent diabetic patients: A literature review. Diabetes Metab. Syndr. 2017, 11, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Khatib, F.A.; Shafagoj, Y.A. Metabolic alterations as a result of Ramadan fasting in non-insulin-dependent diabetes mellitus patients in relation to food intake. Saudi Med. J. 2004, 25, 1858–1863. [Google Scholar] [PubMed]
- Khaled, B.M.; Bendahmane, M.; Belbraouet, S. Ramadan fasting induces modifications of certain serum components in obese women with type 2 diabetes. Saudi Med. J. 2006, 27, 23. [Google Scholar] [PubMed]
- Sari, R.; Balci, M.K.; Akbas, S.H.; Avci, B. The effects of diet, sulfonylurea, and Repaglinide therapy on clinical and metabolic parameters in type 2 diabetic patients during Ramadan. Endocr. Res. 2004, 30, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Benaji, B.; Mounib, N.; Roky, R.; Aadil, N.; Houti, I.; Moussamih, S.; Maliki, S.; Gressier, B.; El Ghomari, H. Diabetes and Ramadan: Review of the literature. Diabetes Res. Clin. Pract. 2006, 73, 117–125. [Google Scholar] [CrossRef]
- Norouzy, A.; Mohajeri, S.; Shakeri, S.; Yari, F.; Sabery, M.; Philippou, E.; Varasteh, A.; Nematy, M. Effect of Ramadan fasting on glycemic control in patients with Type 2 diabetes. J. Endocrinol. Investig. 2012, 35, 766. [Google Scholar]
- Pallayova, M.; Zaghloul, H.B.; Arora, T.; Choudhury, S.M.; Omar, O.M.; Chagoury, O.L.; Taheri, S. Investigating physiological glucose excursions before, during, and after Ramadan in adults without diabetes mellitus. Physiol. Behav. 2017, 179, 110–115. [Google Scholar] [CrossRef]
- Hassanein, M.; Rashid, F.; Elsayed, M.; Basheir, A.; Al Saeed, M.; Abdelgadir, E.; AbuelKheir, S.; Khalifa, A.; Al Sayyah, F.; Bachet, F. Assessment of risk of fasting during Ramadan under optimal diabetes care, in high-risk patients with diabetes and coronary heart disease through the use of FreeStyle Libre flash continuous glucose monitor (FSL-CGMS). Diabetes Res. Clin. Pract. 2019, 150, 308–314. [Google Scholar] [CrossRef]
- Salti, I.; Bénard, E.; Detournay, B.; Bianchi-Biscay, M.; Le Brigand, C.; Voinet, C.; Jabbar, A. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: Results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004, 27, 2306–2311. [Google Scholar] [CrossRef]
- Hassan, A.; Meo, S. Diabetes during Ramadan: Underestimated, under-investigated, needs more attention. Eur. Rev. Med. Pharm. Sci. 2014, 18, 3528–3533. [Google Scholar]
- Monnier, L.; El Azrak, A.; Lessan, N.; Rochd, D.; Colette, C.; Bonnet, F. Ramadan and diabetes: What we see, learn and understand from continuous glucose monitoring. Diabetes Metab. 2015, 41, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Lessan, N.; Hasan, H.; Barakat, M.T. Ramadan fasting: A study of changes in glucose profiles among patients with diabetes using continuous glucose monitoring. Diabetes Care 2012, 35, e37. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jabbar, A.; Hassanein, M.; Beshyah, S.A.; Boye, K.S.; Yu, M.; Babineaux, S.M. CREED study: Hypoglycaemia during Ramadan in individuals with Type 2 diabetes mellitus from three continents. Diabetes Res. Clin. Pr. 2017, 132, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Malik, U.; Mahmood, N.; Khan, K.A.; Hameed, M.; Randhawa, F.A.; Salman, S.; Riaz, A.; Waheed, K.; Rasheed, A. Glycemic control of type 2 diabetic patients during ramazan fasting. J. Ayub. Med. Coll. Abbottabad 2017, 29, 102–106. [Google Scholar] [PubMed]
- Ahmadani, M.; Riaz, M.; Fawwad, A.; Hydrie, M.; Hakeem, R.; Basit, A. Glycaemic trend during Ramadan in fasting diabetic subjects: A study from Pakistan. Pak. J. Biol. Sci. 2008, 11, 2044–2047. [Google Scholar] [CrossRef][Green Version]
- Lamri-Senhadji, M.; El Kebir, B.; Belleville, J.; Bouchenak, M. Assessment of dietary consumption and time-course of changes in serum lipids and lipoproteins before, during and after Ramadan in young Algerian adults. Singap. Med. J. 2009, 50, 288. [Google Scholar]
- Haouari-Oukerro, F.; Ben-Attia, M.; Kaâbachi, N.; Haouari, M. Ramadan fasting influences on food intake consumption, sleep schedule, body weight and some plasma parameters in healthy fasting volunteers. Afr. J. Biotechnol. 2013, 12, 3327–3332. [Google Scholar]
- Mansi, K.M.S. Study the effects of Ramadan fasting on the serum glucose and lipid profile among healthy Jordanian students. Am. J. Appl Sci 2007, 4, 565–569. [Google Scholar]
- Maislos, M.; Khamaysi, N.; Assali, A.; Abou-Rabiah, Y.; Zvili, I.; Shany, S. Marked increase in plasma high-density-lipoprotein cholesterol after prolonged fasting during Ramadan. Am. J. Clin. Nutr. 1993, 57, 640–642. [Google Scholar] [CrossRef]
- Zare, A.; Hajhashemi, M.; Hassan, Z.; Zarrin, S.; Pourpak, Z.; Moin, M.; Salarilak, S.; Masudi, S.; Shahabi, S. Effect of Ramadan fasting on serum heat shock protein 70 and serum lipid profile. Singap. Med. J. 2011, 52, 491–495. [Google Scholar]
- Akanji, A.; Mojiminiyi, O.; Abdella, N. Beneficial changes in serum apo A-1 and its ratio to apo B and HDL in stable hyperlipidaemic subjects after Ramadan fasting in Kuwait. Eur. J. Clin. Nutr. 2000, 54, 508. [Google Scholar] [CrossRef] [PubMed]
- Maislos, M.; Abou-Rabiah, Y.; Zuili, I.; Iordash, S.; Shany, S. Gorging and plasma HDL-cholesterol—The Ramadan model. Eur. J. Clin. Nutr. 1998, 52, 127. [Google Scholar] [CrossRef] [PubMed]
- Temizhan, A.; Tandogan, I.; Dönderici, Ö.; Demirbas, B. The effects of Ramadan fasting on blood lipid levels. Am. J. Med. 2000, 109, 341. [Google Scholar] [CrossRef]
- Qujeq, D.; Bijani, K.; Kalavi, K.; Mohiti, J.; Aliakbarpour, H. Effects of Ramadan fasting on serum low-density and high-density lipoprotein-cholesterol concentrations. Ann. Saudi Med. 2002, 22, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Akaberi, A.; Golshan, A.; Moojdekanloo, M.; Hashemian, M. Does fasting in Ramadan ameliorate Lipid profile? A prospective observational study. Pak. J. Med Sci. 2014, 30, 708. [Google Scholar]
- Nematy, M.; Alinezhad-Namaghi, M.; Rashed, M.M.; Mozhdehifard, M.; Sajjadi, S.S.; Akhlaghi, S.; Sabery, M.; Mohajeri, S.A.R.; Shalaey, N.; Moohebati, M. Effects of Ramadan fasting on cardiovascular risk factors: A prospective observational study. Nutr. J. 2012, 11, 69. [Google Scholar] [CrossRef]
- Dowood, T. Effects of Ramadan fasting on blood lipids and sugar. Pak. J. Med. Sci. 2004, 20, 308–310. [Google Scholar]
- Hosseini, S.R.A.; Hejazi, K. The effects of Ramadan fasting and physical activity on blood hematological-biochemical parameters. Iran. J. Basic Med Sci. 2013, 16, 845. [Google Scholar]
- Al Hourani, H.M.; Atoum, M.F.; Akel, S.; Hijjawi, N.; Awawdeh, S. Effects of Ramadan fasting on some haematological and biochemical parameters. Jordan J. Biol Sci 2009, 2, 103–108. [Google Scholar]
- Asgary, S.; Aghaei, F.; Naderi, G.A.; Kelishadi, R.; Gharipour, M.; Azali, S. Effects of Ramadan fasting on lipid peroxidation, serum lipoproteins and fasting blood sugar. Med. J. Islamic World Acad. Sci. 2000, 13, 35–38. [Google Scholar]
- Furuncuoglu, Y.; Karaca, E.; Aras, S.; Yönem, A. Metabolic, biochemical and psychiatric alterations in healthy subjects during Ramadan. Pak. J. Nutr. 2007, 6, 209–211. [Google Scholar]
- Mahoob, S.; Sattarivand, R.; Nouri, M.; Arefhosseini, S. Effect of Ramadan fasting on serum lipid profiles in normal and hyperlipidemic subjects. Saudi Med. J. 1999, 20, 947–950. [Google Scholar]
- Saleh, S.A.; Elsharouni, S.A.; Cherian, B.; Mourou, M. Effects of Ramadan fasting on waist circumference, blood pressure, lipid profile, and blood sugar on a sample of healthy Kuwaiti men and women. Malays. J. Nutr. 2005, 11, 143–150. [Google Scholar]
- Thannoun, A.M. Effect of fastnig in Ramadan on blood glucose and lipid profile. Mesop. J. Agric. 2010, 38, 11–15. [Google Scholar] [CrossRef][Green Version]
- Marbut, M.M.; Manssor, A.J.; Abdulrahman, M.A. The effect of Ramadan fasting & Moderate exercise on body weight, serum glucose & lipid profile in healthy fasting subjects. Med. J. Tikrit 2006, 2, 26–30. [Google Scholar]
- Akhtaruzzaman, M.; Hoque, N.; Choudhury, M.; Uddin, M.J.; Parvin, T. Effect of Ramadan fasting on serum lipid profile of Bangladeshi female volunteers. Bangladesh J. Med. Biochem. 2014, 7, 47–51. [Google Scholar] [CrossRef]
- Ismail, W.I.; Haron, N. Effect of Ramadan fasting on serum lipid profile among healthy students in UiTM. In Proceedings of the International Conference on Biological, Chemical and Environmental Sciences (BCES-2014), Penang, Malaysia, 14–15 June 2014; pp. 51–53. [Google Scholar]
- Pathan, M.; Patil, R. Effect of Ramadan fasting on body weight and lipid profile. Biomed. Pharmacol. J. 2015, 3, 167–170. [Google Scholar]
- Shahsavan, F.; Askarizadeh, F.; Namaty, M.; Heravian, J.; Mahmodi, Z.; Rakhshandadi, T.; Sedaghat, M.R. Effect of Ramadan fasting on blood pressure and lipid profiles. J. Nutr. Fasting Health 2015, 3, 126–131. [Google Scholar]
- Khan, N.; Rasheed, A.; Ahmed, H.; Aslam, F.; Kanwal, F. Effect of Ramadan fasting on glucose level, lipid profile, HbA1c and uric acid among medical students in Karachi, Pakistan. Emhj-East. Mediterr. Health J. 2017, 23, 274–279. [Google Scholar]
- Indra, M.R.; Satuman, S.; Widodo, E.; Tinny, E.; Endang, S.; Sudiarto, S.; Soemardini, S. Study of some biochemical parameters in young men as effected by Ramadan Fasting. Yarsi Med. J. 2007, 15. [Google Scholar] [CrossRef]
- Patsch, J.R.; Karlin, J.B.; Scott, L.W.; Smith, L.C.; Gotto, A.M. Inverse relationship between blood levels of high density lipoprotein subfraction 2 and magnitude of postprandial lipemia. Proc. Natl. Acad. Sci. USA 1983, 80, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Afrasiabi, A.; Hassanzadeh, S.; Sattarivand, R.; Nouri, M.; Mahbood, S. Effects of low fat and low calorie diet on plasma lipid levels in the fasting month of Ramadan. Saudi Med. J. 2003, 24, 184–188. [Google Scholar] [PubMed]
- Azizi, F. Islamic fasting and health. Ann. Nutr. Metab. 2010, 56, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Gumaa, K.; Mustafa, K.; Mahmoud, N.; Gader, A. The effects of fasting in Ramadan: 1. Seram uric acid and lipid concentrations. Br. J. Nutr. 1978, 40, 573–581. [Google Scholar] [CrossRef]
- Fedail, S.S.; Murphy, D.; Salih, S.; Bolton, C.; Harvey, R. Changes in certain blood constituents during Ramadan. Am. J. Clin. Nutr. 1982, 36, 350–353. [Google Scholar] [CrossRef]
- Shoukry, M. Effect of fasting in Ramadan on plasma lipoproteins and apoproteins. Saudi Med J. 1986, 7, 561–565. [Google Scholar]
- Hallak, M.H.; Nomani, M.Z.A. Body weight loss and changes in blood lipid levels in normal men on hypocaloric diets during Ramadan fasting. Am. J. Clin. Nutr. 1988, 48, 1197–1210. [Google Scholar] [CrossRef]
- Albrink, M.J.; Ullrich, I.H. Interaction of dietary sucrose and fiber on serum lipids in healthy young men fed high carbohydrate diets. Am. J. Clin. Nutr. 1986, 43, 419–428. [Google Scholar] [CrossRef]
- Nagra, S.; Rahman, Z.; Javaria, M.; Qadri, A.J. Study of some biochemical parameters in young women as affected by Ramadan fasting. Int. J. Ramadan Fasting Res. 1998, 2, 1–5. [Google Scholar]
- Kul, S.; Savaş, E.; Öztürk, Z.A.; Karadağ, G. Does Ramadan fasting alter body weight and blood lipids and fasting blood glucose in a healthy population? A meta-analysis. J. Relig. Health 2014, 53, 929–942. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Karimi, E.; Salehi, M.; Nematy, M. Effects of Ramadan fasting on lipid profile: A narrative review. J. Nutr. Fasting Health 2014, 2, 57–61. [Google Scholar]
- Mazidi, M.; Rezaie, P.; Chaudhri, O.; Karimi, E.; Nematy, M. The effect of Ramadan fasting on cardiometabolic risk factors and anthropometrics parameters: A systematic review. Pak. J. Med. Sci. 2015, 31, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, B.; Faghfoori, Z.; Samadi, N.; Karami, H.; Ahmadi, Y.; Badalzadeh, R.; Shafiei-Irannejad, V.; Majidinia, M.; Ghavimi, H.; Jabbarpour, M. The effects of Ramadan fasting on endothelial function in patients with cardiovascular diseases. Eur. J. Clin. Nutr. 2014, 68, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Kacimi, S.; Ref’at, A.; Fararjeh, M.A.; Bustanji, Y.K.; Mohammad, M.K.; Salem, M.L. Intermittent fasting during Ramadan attenuates proinflammatory cytokines and immune cells in healthy subjects. Nutr. Res. 2012, 32, 947–955. [Google Scholar]
- Askari, V.; Alavinezhad, A.; Boskabady, M.H. The impact of “Ramadan fasting period” on total and differential white blood cells, haematological indices, inflammatory biomarker, respiratory symptoms and pulmonary function tests of healthy and asthmatic patients. Allergol. Et Immunopathol. 2016, 44, 359–367. [Google Scholar] [CrossRef]
- Rahbar, A.R.; Safavi, E.; Rooholamini, M.; Jaafari, F.; Darvishi, S.; Rahbar, A. Effects of intermittent fasting during Ramadan on insulin-like growth factor-1, interleukin 2, and lipid profile in healthy Muslims. Int. J. Prev. Med. 2019, 10. [Google Scholar] [CrossRef]
- Asadi, H.; Abolfathi, A.A.; Badalzadeh, R.; Majidinia, M.; Yaghoubi, A.; Asadi, M.; Yousefi, B. Effects of ramadan fasting on serum amyloid A and protein carbonyl group levels in patients with cardiovascular diseases. J. Cardiovasc. Thorac. Res. 2015, 7, 55. [Google Scholar] [CrossRef]
- Mushtaq, R.; Akram, A.; Mushtaq, R.; Khwaja, S.; Ahmed, S. The role of inflammatory markers following Ramadan Fasting. Pak. J. Med. Sci. 2019, 35, 77. [Google Scholar] [CrossRef]
- Yakoob, M.Y. Fasting during Ramadan and obesity. J. Pak. Med Assoc. 2011, 61, 303. [Google Scholar]
- Madkour, M.I.; El-Serafi, A.T.; Jahrami, H.A.; Sherif, N.M.; Hassan, R.E.; Awadallah, S. Ramadan diurnal intermittent fasting modulates SOD2, TFAM, Nrf2, and sirtuins (SIRT1, SIRT3) gene expressions in subjects with overweight and obesity. Diabetes Res. Clin. Pract. 2019, 155, 107801. [Google Scholar] [CrossRef]
- Kassab, S.; Abdul-Ghaffar, T.; Nagalla, D.S.; Sachdeva, U.; Nayar, U. Serum leptin and insulin levels during chronic diurnal fasting. Asia Pac. J. Clin. Nutr. 2003, 12, 483–487. [Google Scholar] [PubMed]
- Alzoghaibi, M.A.; Pandi-Perumal, S.R.; Sharif, M.M.; BaHammam, A.S. Diurnal intermittent fasting during Ramadan: The effects on leptin and ghrelin levels. PLoS ONE 2014, 9, e92214. [Google Scholar] [CrossRef] [PubMed]
- Verdich, C.; Toubro, S.; Buemann, B.; Holst, J.J.; Bülow, J.; Simonsen, L.; Søndergaard, S.B.; Christensen, N.J.; Astrup, A. Leptin levels are associated with fat oxidation and dietary-induced weight loss in obesity. Obes. Res. 2001, 9, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Marbut, M.M.; Al-Najjar, H.A.-D.S.; Mustafa, A. Effect of Ramadan fasting on some physiological parameters. Med. J. Tikrit 2005, 2, 6–8. [Google Scholar]
- Patterson, R.E.; Sears, D.D. Metabolic effects of intermittent fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Dawn Meal (Suhoor) | Breaking Fast Meal (Iftar) | ||||
|---|---|---|---|---|---|
| Starters | Main | Others | Drinks | ||
| Algeria |
|
|
|
| |
| Bangladesh |
|
|
|
| |
| Egypt |
|
|
|
| |
| Saudi Arabia |
|
|
|
|
|
| Singapore |
|
|
|
|
|
| Authors | Date | Country | Subjects (n) | Effect of Ramadan on Nutrient Intake |
|---|---|---|---|---|
| Rahman et al. [30] | 2004 | Bangladesh | 20 males | No change in energy, carbohydrate or protein |
| Increase in fat | ||||
| El Ati et al. [31] | 1995 | Tunisia | 16 females | Increase in protein and fat |
| Frost and Pirani [33] | 1987 | Saudi Arabia | 15 | Increase in carbohydrate, protein and fat |
| Yeoh et al. [34] | 2015 | Singapore | 29 | No change in energy, carbohydrate or protein |
| Increase in fat | ||||
| Lamine et al. [35] | 2006 | Tunisia | 30 | Increase in fat |
| Sadiya et al. [36] | 2011 | UAE | 19 | Decrease in protein, increase in fat |
| Bouhlel et al. [37] | 2006 | Tunisia | 9 | Decrease in carbohydrate and protein |
| Increase in fat | ||||
| Poh et al. [38] | 1996 | Malaysia | 117 | No change in protein. Decrease in carbohydrate and fat |
| Suriani et al. [39] | 2015 | Malaysia | 84 | Decrease in carbohydrate |
| Khattak et al. [43] | 2013 | Malaysia | 30 | No change in energy or macronutrient intake |
| Date | Country | Subjects (n) | Effect on Body Mass | Effect on Body Fat Percentage | |
|---|---|---|---|---|---|
| Bouhlel et al. [18] | 2008 | Tunisia | 9 males | Significant reduction of 1.8 kg | Significant reduction of 1.3% |
| López-Bueno et al. [51] | 2015 | Spain | 62 females | Significant reduction of 1.6% | Significant reduction of 2.2% |
| Nachvak et al. [57] | 2019 | Iran | 160 males | Significant reduction of 1.93 kg | Significant reduction of 0.3% |
| Norouzy et al. [52] | 2013 | Iran | 240 | Significant reduction of 2.2% in males and 1.4% in females aged ≤ 35 years | Significant reduction of 2.5% in males ≤ 35 years and 1.1% in males 36 to 70 years |
| Shruthi et al. [54] | 2013 | India | 50 | Significant reduction of 0.59 kg | Significant reduction of 3.155% |
| Syam et al. [55] | 2016 | Indonesia | 43 | Significant reduction of 0.874 kg | Significant reduction of 0.484 kg |
| Kocaaga et al. [69] | 2019 | Turkey | 33 males | Significant reduction of 0.84 kg | Significant reduction of 1.32% |
| Amiri et al. [70] | 2016 | Iran | 51 | Significant reduction of 0.78 kg | Significant reduction of 0.49 kg |
| El Ati et al. [31] | 1995 | Tunisia | 16 females | No significant change | No significant change |
| Harder-Lauridsen et al. [58] | 2017 | Denmark | 10 males | No significant change | No significant change |
| Ramadan [59] | 2002 | Kuwait | 16 males | No significant change | No significant change |
| Racinais et al. [60] | 2012 | Qatar | 11 males | No significant change | No significant change |
| Finch et al. [61] | 1998 | UK | 41 | No significant change | No significant change |
| Al-barha et al. [71] | 2019 | Saudi Arabia | 44 | No significant change | No significant change |
| Authors | Date | Country | Subjects (n) | Effect on Body Mass | Effect on Body Fat Percentage | Effect on Visceral Adiposity |
|---|---|---|---|---|---|---|
| Khattak et al. [76] | 2012 | Malaysia | 25 | Significant reduction of 15.8 kg in males and 15.4 kg in females | No change | - |
| Khan et al. [77] | 2002 | Pakistan | 10 males | Significant reduction of 3.2 ± 1.7 kg | - | - |
| Rohin et al. [78] | 2013 | Malaysia | 27 | Significant reduction of 0.95 kg for overweight subjects and 2.07 kg in obese subjects | No change | - |
| Celik et al. [80] | 2014 | Turkey | 42 | Significant reduction of 1.6 kg | - | - |
| Suriani et al. [81] | 2015 | Malaysia | 48 | Significant reduction of 1.76 kg | Significant reduction of 0.32% | Significant reduction of 0.75 kg |
| Khaled et al. [41] | 2009 | Algeria | 276 | Significant reduction of 3.12 kg | - | - |
| Madkour et al. [82] | 2019 | UAE | 56 | Significant reduction of 1.15 kg | Significant reduction of 1.22 kg | Significant reduction of 5.82 cm² |
| Ünalacak et al. [79] | 2011 | Turkey | 10 males | Significant reduction of 2.9 kg | - | - |
| Radhakishun et al. [83] | 2014 | Netherlands | 25 | No change | Significant reduction of 2.5% | - |
| Salehi et al. [84] | 2007 | Iran | 28 males | Significant reduction of 6% | - | - |
| Sezen et al. [53] | 2016 | Turkey | 70 | - | Significant reduction of 0.9 kg | Significant reduction of 0.5% |
| Ganjali et al. [85] | 2016 | Iran | 24 | Significant reduction of 2.2 ± 1.81 kg | - | - |
| Authors | Date | Country | Subjects (n) | Effect of Ramadan Fasting on Fasting Blood Glucose Levels |
|---|---|---|---|---|
| Ongsara et al. [86] | 2017 | Thailand | 65 | Increase |
| Fakhrzadeh et al. [50] | 2003 | Iran | 91 | Decrease |
| Larijani et al. [87] | 2003 | Iran | 115 | Decrease |
| Sarraf-Zadegan et al. [89] | 2000 | Iran | 50 | No change |
| Ziaee et al. [90] | 2006 | Iran | 81 | Decrease |
| Azizi and Rasouli [91] | 1987 | Iran | 9 | No change |
| Kiyani et al. [92] | 2017 | Pakistan | 80 | Decrease |
| Ramadan [59] | 2002 | Kuwait | 16 | No change |
| Lamine et al. [35] | 2006 | Tunisia | 30 | No change |
| Beltaifa et al. [93] | 2002 | Tunisia | 20 | No change |
| Roy et al. [96] | 2017 | India | 37 males | Decrease |
| Darzabi et al. [99] | 2019 | Iran | 15 males | Decrease |
| Authors | Date | Country | Subjects (n) | Health Condition | Effect of Ramadan Fasting on Fasting Blood Glucose Levels |
|---|---|---|---|---|---|
| Sadiya et al. [36] | 2011 | UAE | 19 | Metabolic syndrome | Increase |
| Shariatpanahi et al. [88] | 2008 | Iran | 55 | Metabolic syndrome | Decrease |
| Radhakishun et al. [83] | 2014 | Netherlands | 25 | Obesity | No change |
| Mafauzy et al. [101] | 1990 | Malaysia | 22 | Type 2 diabetes | No change |
| Lessan et al. [102] | 2015 | UAE | 56 | Type 2 diabetes | No change |
| Al-Hader et al. [103] | 1994 | Jordan | 23 | Type 2 diabetes | No change |
| Yarahmadi et al. [104] | 2003 | Iran | 57 | Type 2 diabetes | No change |
| Khatib and Shafagoj [106] | 2004 | Jordan | 44 | Type 2 diabetes | Decrease |
| Khaled et al. [107] | 2006 | Algeria | 60 | Obesity and Type 2 diabetes | Decrease |
| Norouzy et al. [110] | 2012 | Iran | 89 | Type 2 diabetes | Increase |
| Authors | Date | Subjects (n) | Effect of Ramadan on Parameters |
|---|---|---|---|
| Adlouni et al. [44] | 1997 | 32 males | Increase in HDL |
| Reductions in TC, TG and LDL | |||
| Akaberi et al. [129] | 2014 | 43 | Increases in TC, HDL and LDL |
| No change in TG | |||
| Reductions in LDL/HDL and TG/HDL | |||
| Akanji et al. [125] | 2000 | 64 | Increases in apo A-1, apo A-1/apo B, apo A-1/HDL |
| No change in TC, TG or LDL | |||
| Al Hourani et al. [133] | 2009 | 57 females | No change in TC, HDL or LDL |
| Reduction in TG | |||
| Asgary et al. [134] | 2000 | 50 males | Reductions in TC and TG |
| Dowood [131] | 2004 | 60 | No change in TC, TG, HDL or VLDL |
| Reduction in LDL | |||
| Fakhrzadeh et al. [50] | 2003 | 91 | Increase in HDL |
| Reductions in TC, TG and LDL | |||
| Furuncuoglu et al. [135] | 2007 | 39 | No change in HDL |
| Reductions in TC and TG | |||
| Haghdoost and Poorranjbar [74] | 2009 | 93 | Reduction in TG |
| Haouari-Oukerro et al. [121] | 2013 | 38 males | Increase in HDL |
| No change in TC | |||
| Reductions in TG and LDL | |||
| Hosseini and Hejazi [132] | 2013 | 26 males | Increase in HDL |
| Reductions in TC, LDL, VLDL, LDL/HDL and TC/HDL | |||
| Lamri-Senhadji et al. [120] | 2009 | 46 | Increase in HDL |
| Reduction in LDL | |||
| Mahoob et al. [136] | 1999 | 35 males | Reductions in TG, LDL, TC/HDL and LDL/HDL |
| M Maislos et al. [126] | 1998 | 22 | Increase in HDL |
| No change in TC, TG, LDL or VLDL | |||
| M Maislos et al. [123] | 1993 | 24 | Increases in HDL, apo A-1 |
| No change in TC, TG, LDL or VLDL | |||
| Reductions in TC/HDL and LDL/HDL | |||
| Mansi [122] | 2007 | 70 | Increase in HDL |
| No change in TC or TG | |||
| Reduction in LDL | |||
| Nematy et al. [130] | 2012 | 82 | Increase in HDL |
| Reductions in TC, TG, LDL and VLDL | |||
| Qujeq et al. [128] | 2002 | 83 | Increase in HDL |
| Reduction in LDL | |||
| Rahman et al. [30] | 2004 | 20 males | Increase in HDL |
| No change in TC, TG or LDL | |||
| Reductions in TC/LDL and LDL/HDL | |||
| Saleh et al. [137] | 2005 | 60 | No change in TG, HDL or VLDL |
| Reductions in TC and LDL | |||
| Shehab et al. [64] | 2012 | 65 | Increase in HDL |
| No change in TC | |||
| Reductions in TG and LDL | |||
| Temizhan et al. [127] | 2000 | 52 | No change in HDL |
| Reductions in TC, TG, LDL and VLDL | |||
| Ünalacak et al. [79] | 2011 | 20 males | No change in TC, HDL or LDL |
| Reduction in TG | |||
| Zare et al. [124] | 2011 | 32 males | Increases in HDL and HSP70 |
| Reductions in TC, TG, LDL, LDL/HDL and TC/HDL | |||
| Ziaee et al. [90] | 2006 | 81 | Increase in LDL |
| No change in TC, TG or VLDL | |||
| Reduction in HDL | |||
| Thannoun et al. [138] | 2010 | 31 | Increase in HDL |
| Reduction in TC, LDL and TG | |||
| Marbut et al. [139] | 2006 | 30 males | Increase in HDL |
| Reduction in LDL | |||
| Akhtaruzzaman et al. [140] | 2014 | 28 females | Increase in HDL |
| Reduction in TC and LDL | |||
| Ismail et al. [141] | 2014 | 31 | Increase in HDL |
| Reduction in LDL and TG | |||
| Pathan et al. [142] | 2010 | 30 males | Increase in HDL |
| Reduction in TC, LDL, VLDL and TG | |||
| Dowod [131] | 2004 | 60 | Reduction in LDL |
| Shahsavan et al. [143] | 2015 | 89 | Reduction in TC and HDL |
| No change in LDL, TG or LDL/HDL | |||
| Khan et al. [144] | 2017 | Pakistan | Increase in LDL |
| Reduction in HDL | |||
| Indra et al. [145] | 2007 | Indonesia | Reduction in TC, LDL and TG |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osman, F.; Haldar, S.; Henry, C.J. Effects of Time-Restricted Feeding during Ramadan on Dietary Intake, Body Composition and Metabolic Outcomes. Nutrients 2020, 12, 2478. https://doi.org/10.3390/nu12082478
Osman F, Haldar S, Henry CJ. Effects of Time-Restricted Feeding during Ramadan on Dietary Intake, Body Composition and Metabolic Outcomes. Nutrients. 2020; 12(8):2478. https://doi.org/10.3390/nu12082478
Chicago/Turabian StyleOsman, Farhana, Sumanto Haldar, and Christiani Jeyakumar Henry. 2020. "Effects of Time-Restricted Feeding during Ramadan on Dietary Intake, Body Composition and Metabolic Outcomes" Nutrients 12, no. 8: 2478. https://doi.org/10.3390/nu12082478
APA StyleOsman, F., Haldar, S., & Henry, C. J. (2020). Effects of Time-Restricted Feeding during Ramadan on Dietary Intake, Body Composition and Metabolic Outcomes. Nutrients, 12(8), 2478. https://doi.org/10.3390/nu12082478