Intensity Thresholds and Maximal Lactate Steady State in Small Muscle Group Exercise



Abstract
:1. Introduction
2. Materials and Methods
2.1. Used Devices and Measuring Methods
2.2. Data Analysis and Turn Point Determination
2.3. Test Procedures
2.3.1. One Repetition Maximum (1RM)
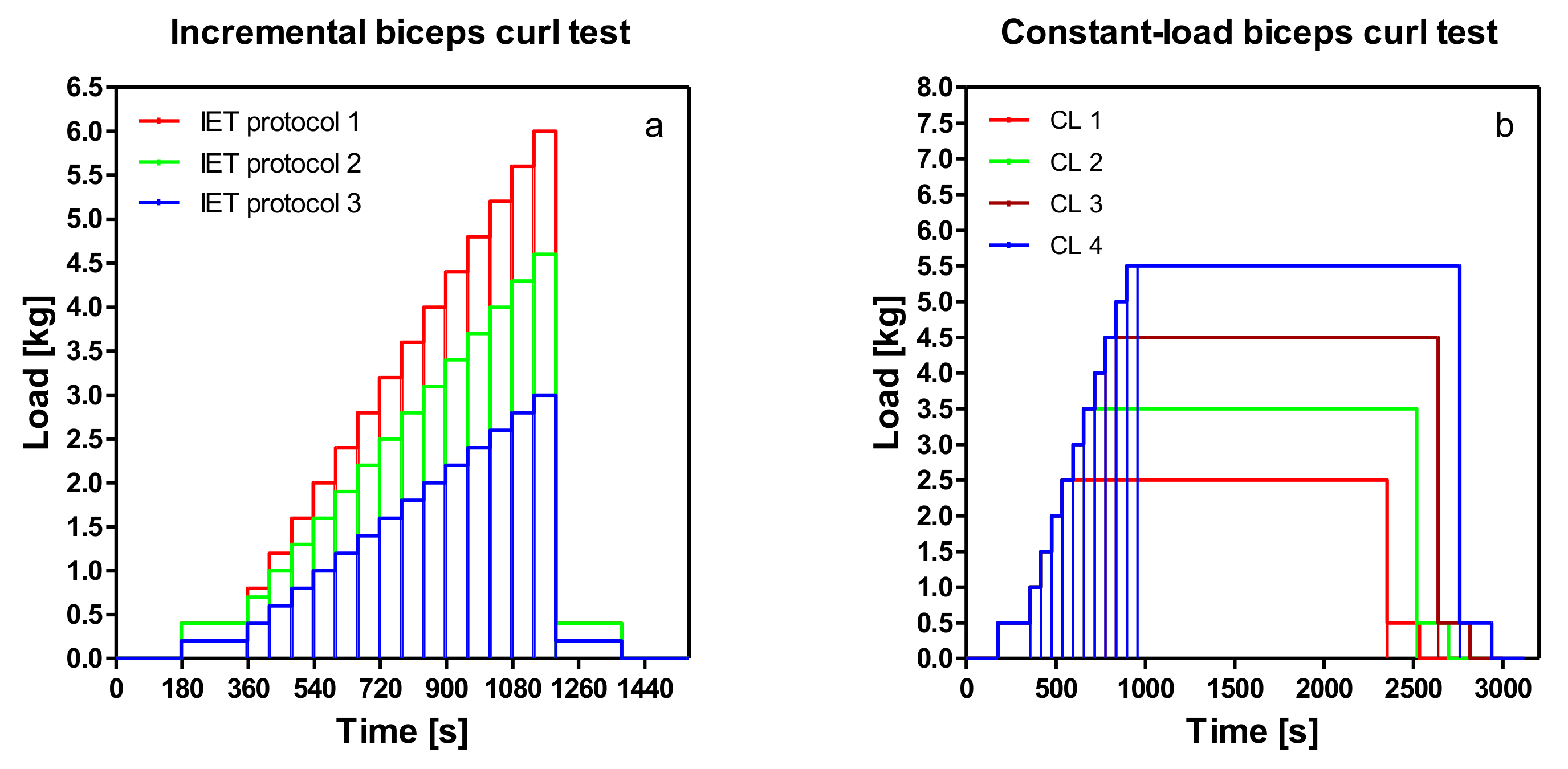
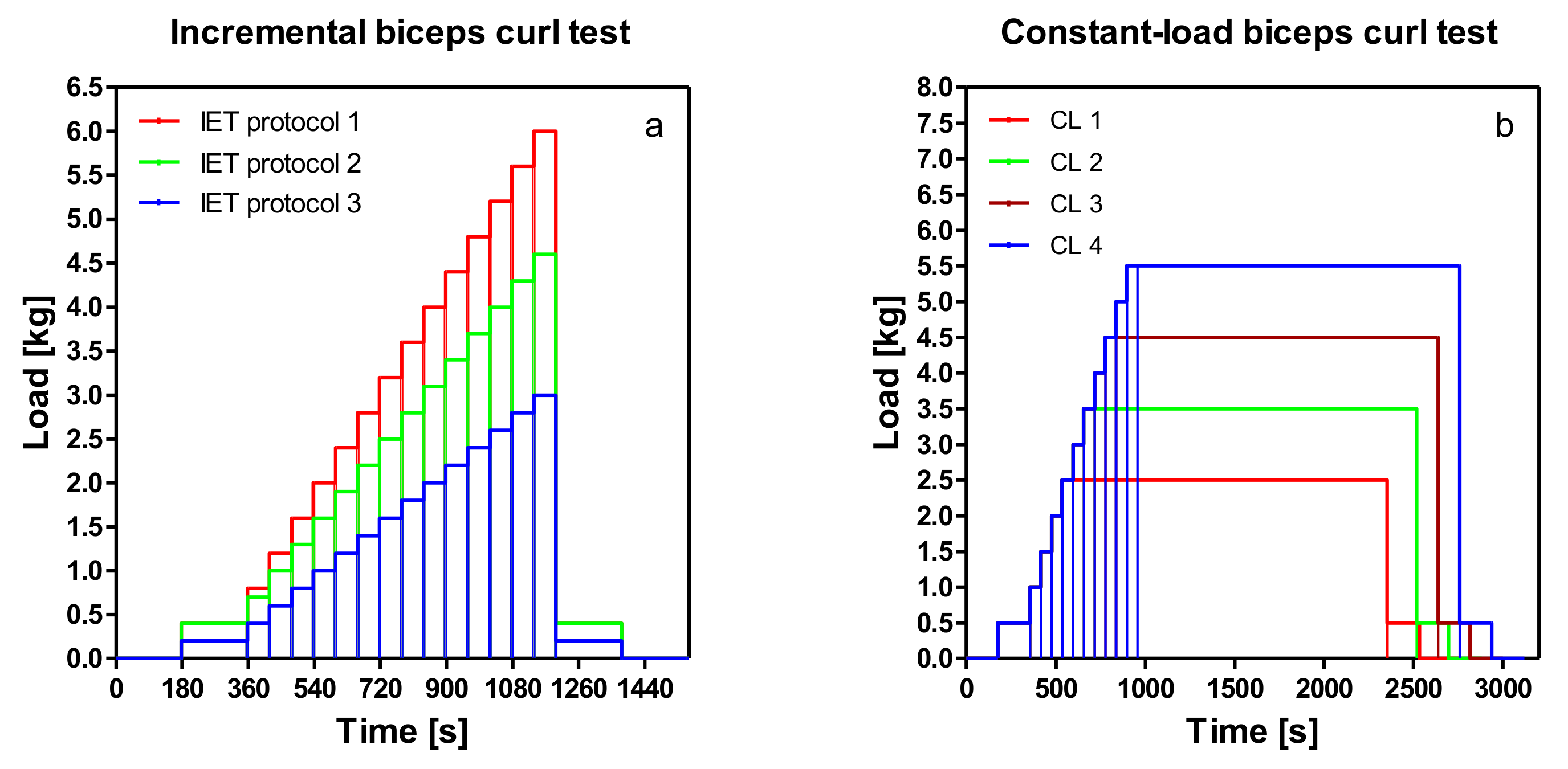
2.3.2. Incremental Bicep Curl Test
2.3.3. Constant-Load Tests
2.3.4. Statistical Analysis
3. Results
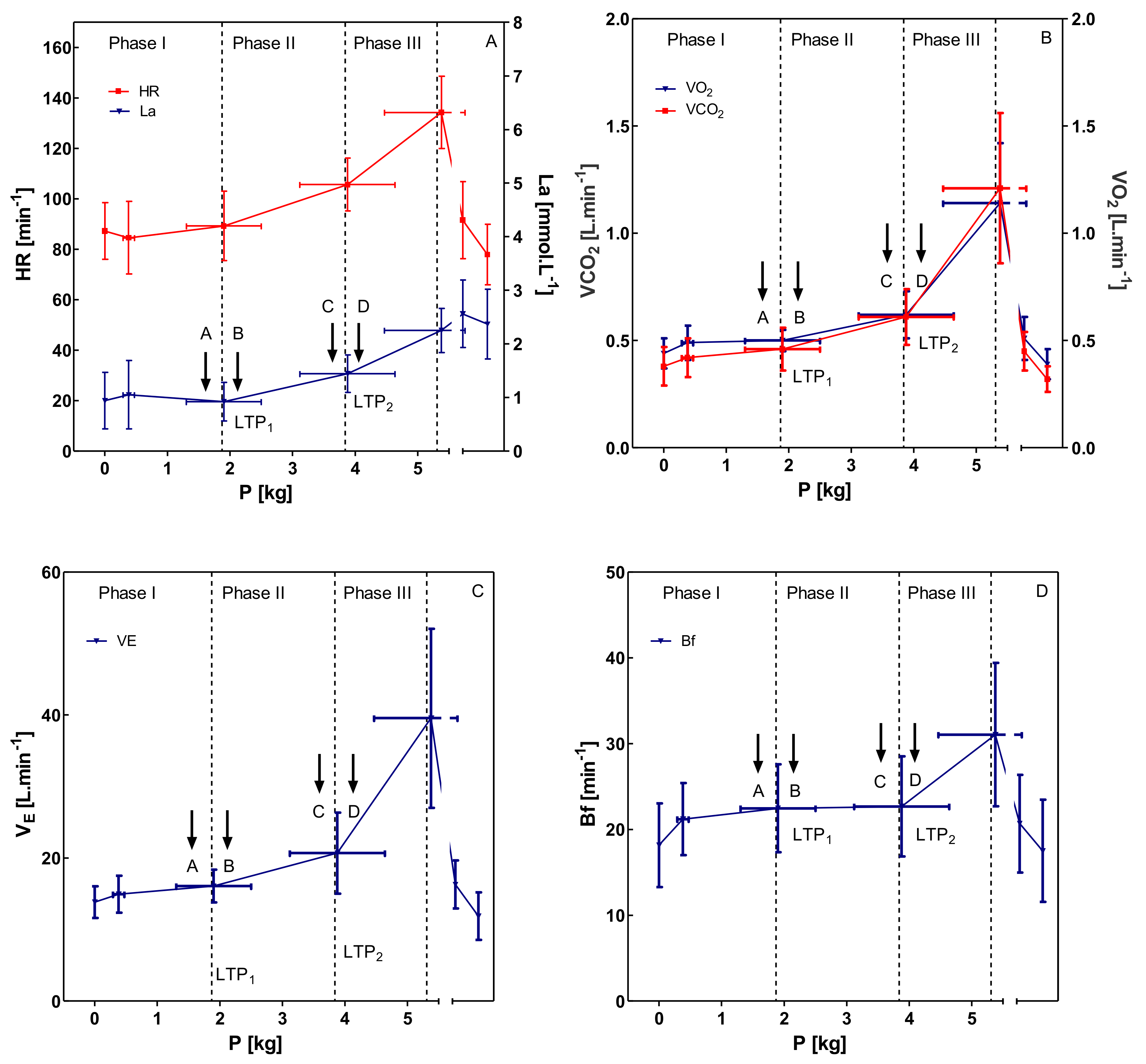
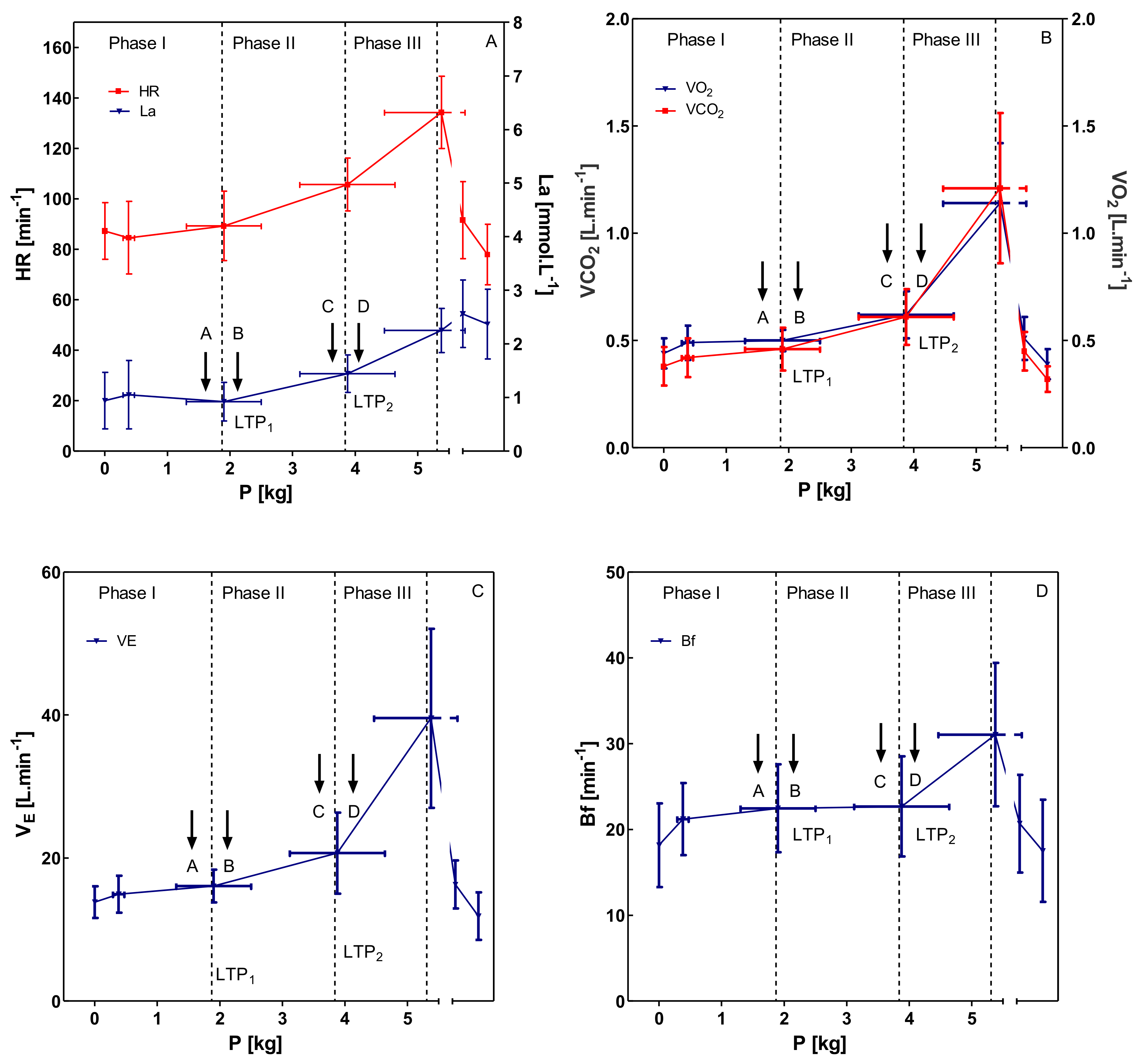
3.1. Incremental Bicep Curl Test
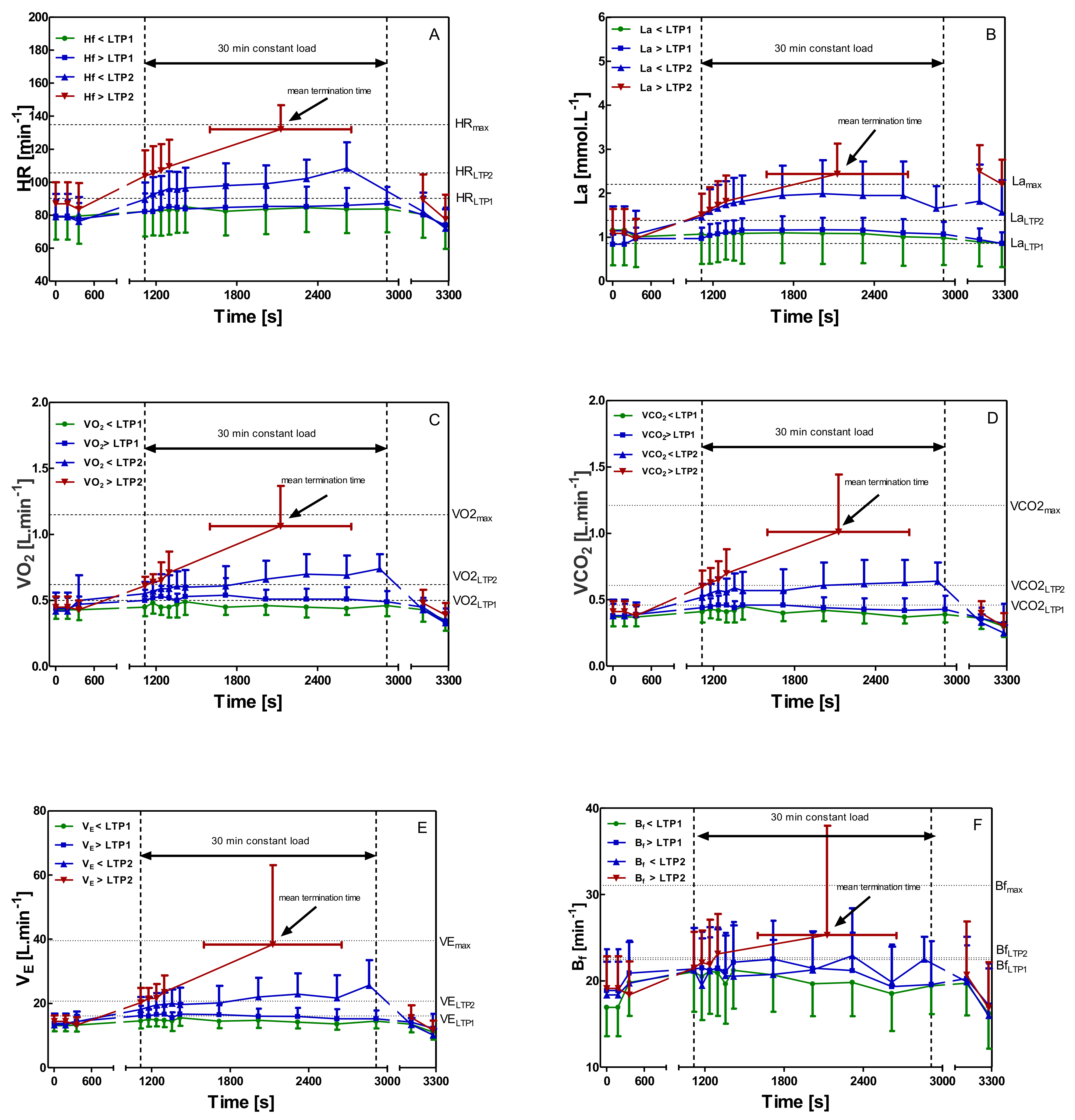
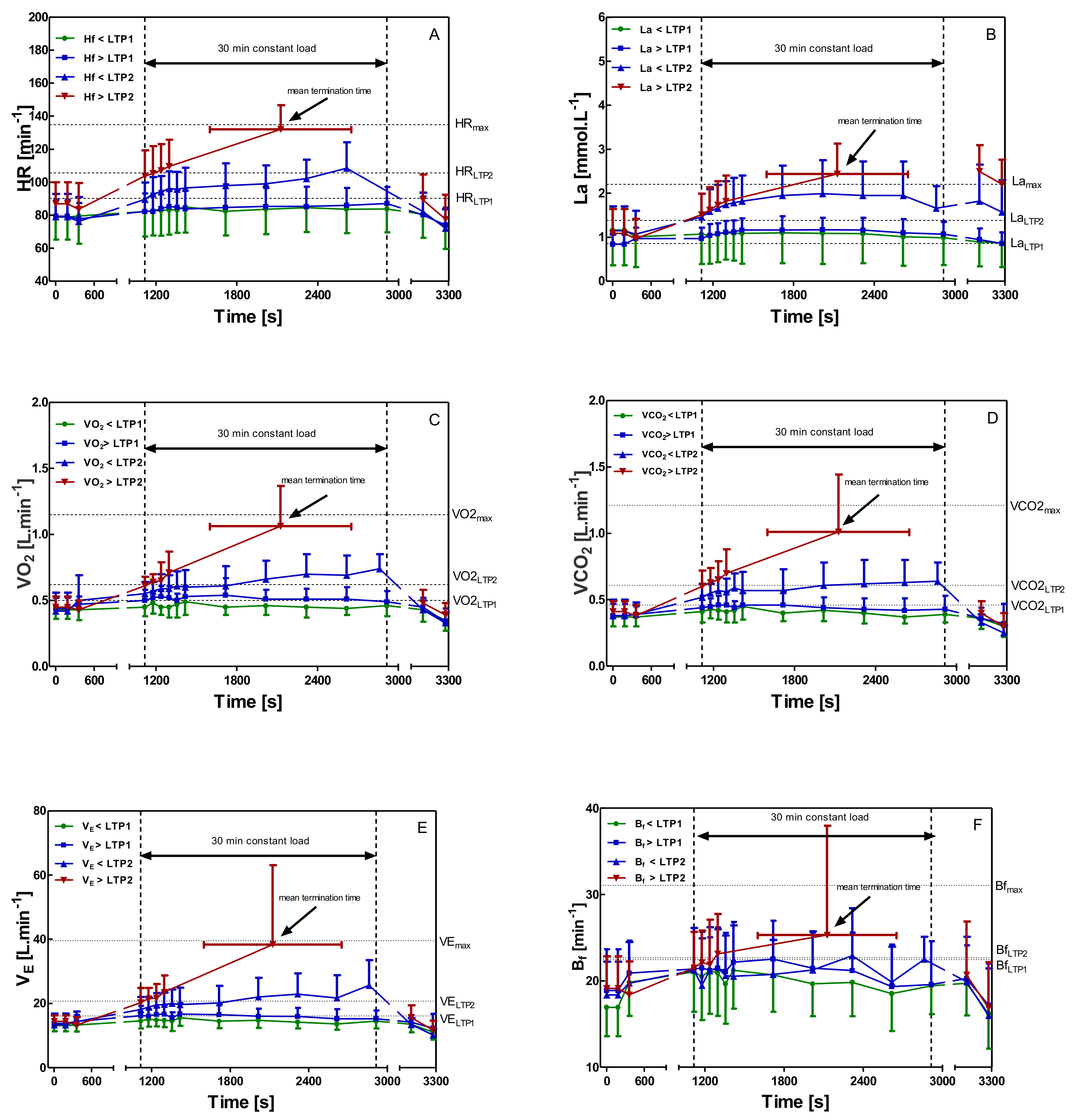
3.2. Constant-Load Bicep Curl Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brooks, G.A. Lactate shuttles in nature. Biochem. Soc. Trans. 2002, 30, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. Cell-cell and intracellular lactate shuttles. J. Physiol. 2009, 587, 5591–5600. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. The science and translation of lactate shuttle theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, P.; Tschakert, G. Special Needs to Prescribe Exercise Intensity for Scientific Studies. Cardiol. Res. Pract. 2011, 2011, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, P.; Wonisch, M.; Pokan, R.; Schwaberger, G.; Smekal, G.; von Duvillard, S.P. Beta1-adrenoceptor mediated origin of the heart rate performance curve deflection. Med. Sci. Sports Exerc. 2005, 37, 1704–1709. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A.; Hashimoto, T. Investigation of the lactate shuttle in skeletal muscle mitochondria. J. Physiol. 2007, 584, 705. [Google Scholar] [CrossRef]
- Chamari, K.; Padulo, J. ‘Aerobic’and ‘Anaerobic’terms used in exercise physiology: A critical terminology reflection. Sports Med. Open 2015, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J.P. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef]
- Moser, O.; Tschakert, G.; Mueller, A.; Groeschl, W.; Hofmann, P.; Pieber, T.; Lawrence, J.; Koehler, G. Short-acting insulin reduction strategies for continuous cycle ergometer exercises in patients with type 1 diabetes mellitus. Asian J. Sports Med. 2017, 8, e42160. [Google Scholar] [CrossRef] [Green Version]
- Smekal, G.; Scharl, A.; von Duvillard, S.P.; Pokan, R.; Baca, A.; Baron, R.; Tschan, H.; Hofmann, P.; Bachl, N. Accuracy of neuro-fuzzy logic and regression calculations in determining maximal lactate steady-state power output from incremental tests in humans. Eur. J. Appl. Physiol. 2002, 88, 264–274. [Google Scholar] [CrossRef]
- Tschakert, G.; Hofmann, P. High-intensity intermittent exercise: Methodological and physiological aspects. Int. J. Sports Physiol. Perform. 2013, 8, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G. Assessment of functional capacity in clinical and research settings: A scientific statement from the American Heart Association Committee on Exercise, Rehabilitation, and Prevention of the Council on Clinical Cardiology and the Council on Cardiovascular Nursing. Circulation 2007, 116, 329–343. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, N.M.F.; Magosso, R.F.; Pereira, G.B.; Leite, R.D.; Arakelian, V.M.; Montagnolli, A.N.; Perez, S.A.; Baldissera, V. The measurement of lactate threshold in resistance exercise: A comparison of methods. Clin. Physiol. Funct. Imaging 2011, 31, 376–381. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, N.M.F.; Magosso, R.F.; Pereira, G.B.; Souza, M.V.C.; Vieira, A.; Marine, D.A.; Perez, S.E.A.; Baldissera, V. Acute cardiorespiratory and metabolic responses during resistance exercise in the lactate threshold intensity. Int. J. Sports Med. 2012, 33, 108–113. [Google Scholar] [CrossRef]
- De Sousa, N.M.F.; Magosso, R.F.; Dipp, T.; Plentz, R.D.; Marson, R.A.; Montagnolli, A.N.; Martins, R.A.S.; Perez, S.E.A.; Baldissera, V. Continuous blood pressure response at different intensities in leg press exercise. Eur. J. Prev. Cardiol. 2013, 21, 1324–1331. [Google Scholar] [CrossRef]
- Domínguez, R.; Maté-Muñoz, J.L.; Serra-Paya, N.; Garnacho-Castaño, M.V. Lactate Threshold as a Measure of Aerobic Metabolism in Resistance Exercise. Int. J. Sports Med. 2018, 39, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Castaño, M.V.; Domínguez, R.; Ruiz-Solano, P.; Maté-Muñoz, J.L. Acute Physiological and Mechanical Responses during Resistance Exercise at the Lactate Threshold Intensity. J. Strength Cond. Res. 2015, 29, 2867–2873. [Google Scholar] [CrossRef]
- Garnacho-Castaño, M.V.; Domínguez, R.; Maté-Muñoz, J.L. Understanding the meaning of lactate threshold in resistance exercises. Int. J. Sports Med. 2015, 36, 371–377. [Google Scholar] [CrossRef]
- Maté-Muñoz, J.L.; Domínguez, R.; Barba, M.; Monroy, A.J.; Rodríguez, B.; Ruiz-Solano, P.; Garnacho-Castaño, M.V. Cardiorespiratory and Metabolic Responses to Loaded Half Squat Exercise Executed at an Intensity Corresponding to the Lactate Threshold. J. Sports Sci. Med. 2015, 14, 648–656. [Google Scholar]
- Maté-Muñoz, J.L.; Domínguez, R.; Lougedo, J.H.; Garnacho-Castaño, M.V. The lactate and ventilatory thresholds in resistance training. Clin. Physiol. Funct. Imaging 2017, 37, 518–524. [Google Scholar] [CrossRef]
- Moreira, S.; Arsa, G.; Oliveira, H.B.; Lima, L.C.J.; Campbell, C.S.G.; Simões, H.G. Methods to identify the lactate and glucose thresholds during resistance exercise for individuals with type 2 diabetes. J. Strength Cond. Res. 2008, 22, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Aragón-Vela, J.; Barranco-Ruiz, Y.; Casals, C.; Plaza-Díaz, J.; Casuso, R.A.; Fontana, L.; Huertas, J.R. A Novel Electromyographic Approach to Estimate Fatigue Threshold in Maximum Incremental Strength Tests. Motor Control 2017, 22, 170. [Google Scholar] [CrossRef] [PubMed]
- Simões, R.P.; Mendes, R.G.; Castello, V.; Machado, H.G.; Almeida, L.B.; Baldissera, V.; Catai, A.M.; Arena, R.; Borghi-Silva, A. Heart-rate variability and blood-lactate threshold interaction during progressive resistance exercise in healthy older men. J. Strength Cond. Res. 2010, 24, 1313–1320. [Google Scholar] [CrossRef]
- Simões, R.P.; Castello-Simões, V.; Mendes, R.G.; Archiza, B.; Santos, D.A.; Machado, H.G.; Bonjorno, J.C.; Oliveira, C.R.; Reis, M.S.; Catai, A.M.; et al. Lactate and heart rate variability threshold during resistance exercise in the young and elderly. Int. J. Sports Med. 2013, 34, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Simões, R.P.; Castello-Simões, V.; Mendes, R.G.; Archiza, B.; dos Santos, D.A.; Bonjorno, J.C., Jr.; de Oliveira, C.R.; Catai, A.M.; Arena, R.; Borghi-Silva, A. Identification of anaerobic threshold by analysis of heart rate variability during discontinuous dynamic and resistance exercise protocols in healthy older men. Clin. Physiol. Funct. Imaging 2014, 34, 98–108. [Google Scholar] [CrossRef]
- Albesa-Albiol, L.; Serra-Payá, N.; Garnacho-Castaño, M.A.; Cano, L.G.; Cobo, E.P.; Maté-Muñoz, J.L.; Garnacho-Castano, M.V. Ventilatory efficiency during constant-load test at lactate threshold intensity: Endurance versus resistance exercises. PLoS ONE 2019, 14, e0216824. [Google Scholar] [CrossRef] [Green Version]
- Hamberg-van Reenen, H.H.; van der Beek, A.J.; Blatter, B.M.; van Mechelen, W.; Bongers, P.M. Age-related differences in muscular capacity among workers. Int. Arch. Occup. Environ. Health 2009, 82, 1115–1121. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hofmann, P.; Bunc, V.; Leitner, H.; Pokan, R.; Gaisl, G. Heart rate threshold related to lactate turn point and steady-state exercise on a cycle ergometer. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 132–139. [Google Scholar] [CrossRef]
- Hofmann, P.; Pokan, R.; von Duvillard, S.P.; Seibert, F.J.; Zweiker, R.; Schmid, P. Heart rate performance curve during incremental cycle ergometer exercise in healthy young male subjects. Med. Sci. Sports Exerc. 1997, 29, 762–768. [Google Scholar] [CrossRef]
- Stanley, W.C.; Gertz, E.W.; Wisneski, J.A.; Morris, D.L.; Neese, R.A.; Brooks, G.A. Systemic lactate kinetics during graded exercise in man. Am. J. Physiol. Endocrinol. Metab. 1985, 249, E595–E602. [Google Scholar] [CrossRef] [PubMed]
- Griffin, L.; Garland, S.J.; Ivanova, T.; Hughson, R.L. Blood flow in the triceps brachii muscle in humans during sustained submaximal isometric contractions. Eur. J. Appl. Physiol. 2001, 84, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.H.T. Myothermal and intramuscular pressure measurements during isometric contractions of the human quadriceps muscle. J. Physiol. 1972, 224, 29–58. [Google Scholar]
- Bonde-Petersen, F.; Henriksson, J.; Lundin, B. Blood flow in thigh muscle during bicycling exercise at varying work rates. Eur. J. Appl. Physiol. Occup. Physiol. 1975, 34, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Bonde-Petersen, F.; Mørk, A.L.; Nielsen, E. Local muscle blood flow and sustained contractions of human arm and back muscles. Eur. J. Appl. Physiol. Occup. Physiol. 1975, 34, 43–50. [Google Scholar] [CrossRef]
- Hill, D.W.; Butler, S.D. Haemodynamic Responses to Weightlifting Exercise. Sports Med. 1991, 12, 1–7. [Google Scholar] [CrossRef]
- Hofmann, P.; Von Duvillard, S.P.; Seibert, J.; Pokan, R.; Wonisch, M.; Lemura, L.M.; Schwaberger, G. %HRmax target heart rate is dependent on heart rate performance curve deflection. Med. Sci. Sports Exerc. 2001, 10, 1726–1731. [Google Scholar] [CrossRef]
- Thomas, G.D.; Segal, S.S. Neural control of muscle blood flow during exercise. J. Appl. Physiol. 2004, 97, 731–738. [Google Scholar] [CrossRef]
- De Matos, D.G.; Aidar, F.J.; Filho, M.L.M.; da Silva Salgueiro, R.; de Oliveira, J.C.; Klain, I.P.; Hickner, R.C.; Carneiro, A.L.; Dantas, E.H.M. Analysis of hemodynamic responses to resistance exercise performed with different intensities and recovery intervals. Health 2013, 5, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Pokan, R.; Hofmann, P.; Preidler, K.; Leitner, H.; Dusleag, J.; Eber, B.; Schwaberger, G.; Füger, G.F.; Klein, W. Correlation between inflection of heart rate/work performance curve and myocardial function in exhausting cycle ergometer exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 385–388. [Google Scholar] [CrossRef]
- Beneke, R.; Hütler, M.; Leithäuser, R.M. Maximal lactate-steady-state independent of performance. Med. Sci. Sports Exerc. 2000, 32, 1135–1139. [Google Scholar] [CrossRef] [PubMed]
- Billat, V.L.; Sirvent, P.; Py, G.; Koralsztein, J.P.; Mercier, J. The concept of maximal lactate steady state: A bridge between biochemistry, physiology and sport science. Sports Med. 2003, 33, 407–426. [Google Scholar] [CrossRef]
- Chudalla, R.; Baerwalde, S.; Schneider, G.; Maassen, N. Local and systemic effects on blood lactate concentration during exercise with small and large muscle groups. Pflügers Archiv. 2006, 452, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Jose, A.D.; Stitt, F.; Collison, D. The effects of exercise and changes in body temperature on the intrinsic heart rate in man. Am. Heart J. 1970, 79, 488–498. [Google Scholar] [CrossRef]
- Bar-Or, O. The growth and development of children’s physiologic and perceptional responses to exercise. In Children and Sport; Springer: Berlin/Heidelberg, Germany, 1984; pp. 3–17. [Google Scholar]
- Ekelund, L.G.; Holmgren, A. Central hemodynamics during exercise. Circulation 1967, 20, 227. [Google Scholar]
- Drescher, U.; Mookerjee, S.; Steegmanns, A.; Knicker, A.; Hoffmann, U. Gas exchange kinetics following concentric-eccentric isokinetic arm and leg exercise. Respir. Physiol. Neurobiol. 2017, 240, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Rhodes, E.C. Oxygen uptake kinetics during exercise. Sports Med. 1999, 27, 313–327. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Subjects | Sex | Age (years) | Height (cm) | Weight (kg) | BMI | 1RM (kg) | VO2max (Cycle) (mL·kg·min−1) |
|---|---|---|---|---|---|---|---|
| 1 | F | 22.0 | 175.3 | 62.4 | 20.3 | 7.5 | 53.17 |
| 2 | F | 25.0 | 170.1 | 78.9 | 27.3 | 9.0 | 37.03 |
| 3 | M | 24.0 | 187.6 | 84.0 | 23.9 | 15.0 | 50.11 |
| 4 | M | 22.0 | 174.6 | 64.3 | 21.1 | 12.5 | 60.19 |
| 5 | M | 26.0 | 193.0 | 90.0 | 24.2 | 19.0 | 54.22 |
| 6 | M | 25.0 | 174.5 | 69.8 | 22.9 | 15.0 | * |
| 7 | M | 31.0 | 178.0 | 78.0 | 24.6 | 18.5 | 49.23 |
| 8 | M | 25.0 | 177.0 | 75.4 | 24.1 | 14.0 | 51.33 |
| 9 | M | 22.0 | 184.8 | 72.2 | 21.1 | 14.5 | 55.50 |
| 10 | M | 23.0 | 189.0 | 85.0 | 23.8 | 20.0 | 49.70 |
| 11 | M | 22.0 | 187.7 | 75.3 | 21.4 | 12.5 | 54.45 |
| 12 | M | 30.0 | 184.7 | 76.4 | 22.4 | 16.0 | 47.25 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spendier, F.; Müller, A.; Korinek, M.; Hofmann, P. Intensity Thresholds and Maximal Lactate Steady State in Small Muscle Group Exercise. Sports 2020, 8, 77. https://doi.org/10.3390/sports8060077
Spendier F, Müller A, Korinek M, Hofmann P. Intensity Thresholds and Maximal Lactate Steady State in Small Muscle Group Exercise. Sports. 2020; 8(6):77. https://doi.org/10.3390/sports8060077
Chicago/Turabian StyleSpendier, Florian, Alexander Müller, Markus Korinek, and Peter Hofmann. 2020. "Intensity Thresholds and Maximal Lactate Steady State in Small Muscle Group Exercise" Sports 8, no. 6: 77. https://doi.org/10.3390/sports8060077
APA StyleSpendier, F., Müller, A., Korinek, M., & Hofmann, P. (2020). Intensity Thresholds and Maximal Lactate Steady State in Small Muscle Group Exercise. Sports, 8(6), 77. https://doi.org/10.3390/sports8060077