Evaluation of Apelin and Apelin Receptor Level in the Primary Tumor and Serum of Colorectal Cancer Patients

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Ethical Consideration
2.3. Tissue Extracts and Sera Isolation
2.4. Apelin Protein Level Determination
2.5. Transcript Level Quantification
2.6. Statistical Analysis
3. Results
3.1. Comparison of Apelin and Apelin Receptor mRNA Expression Level between Tumour and Normal Tissue of CRC Patients
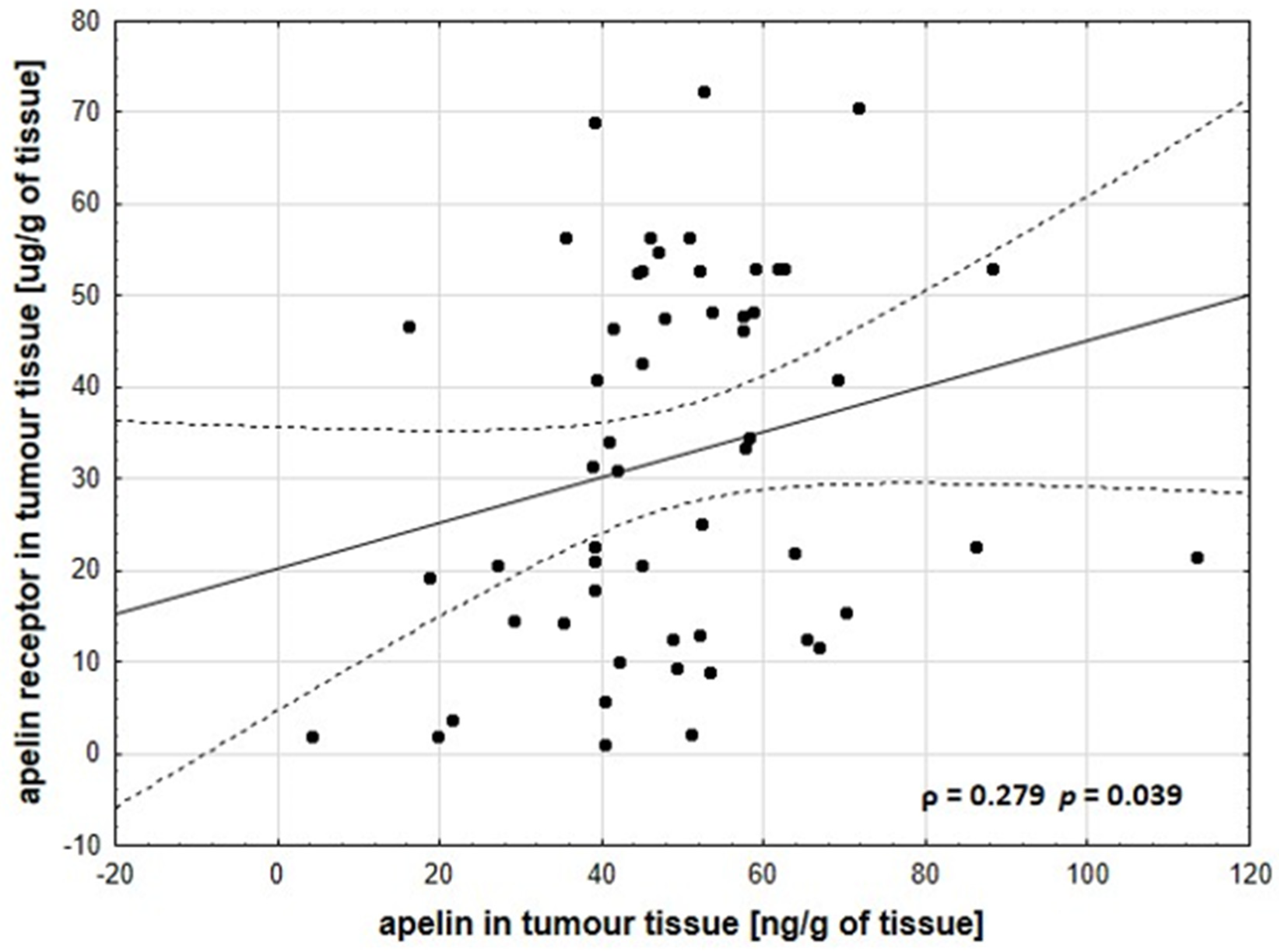
3.2. Concentration of Apelin and APJ on Protein Level
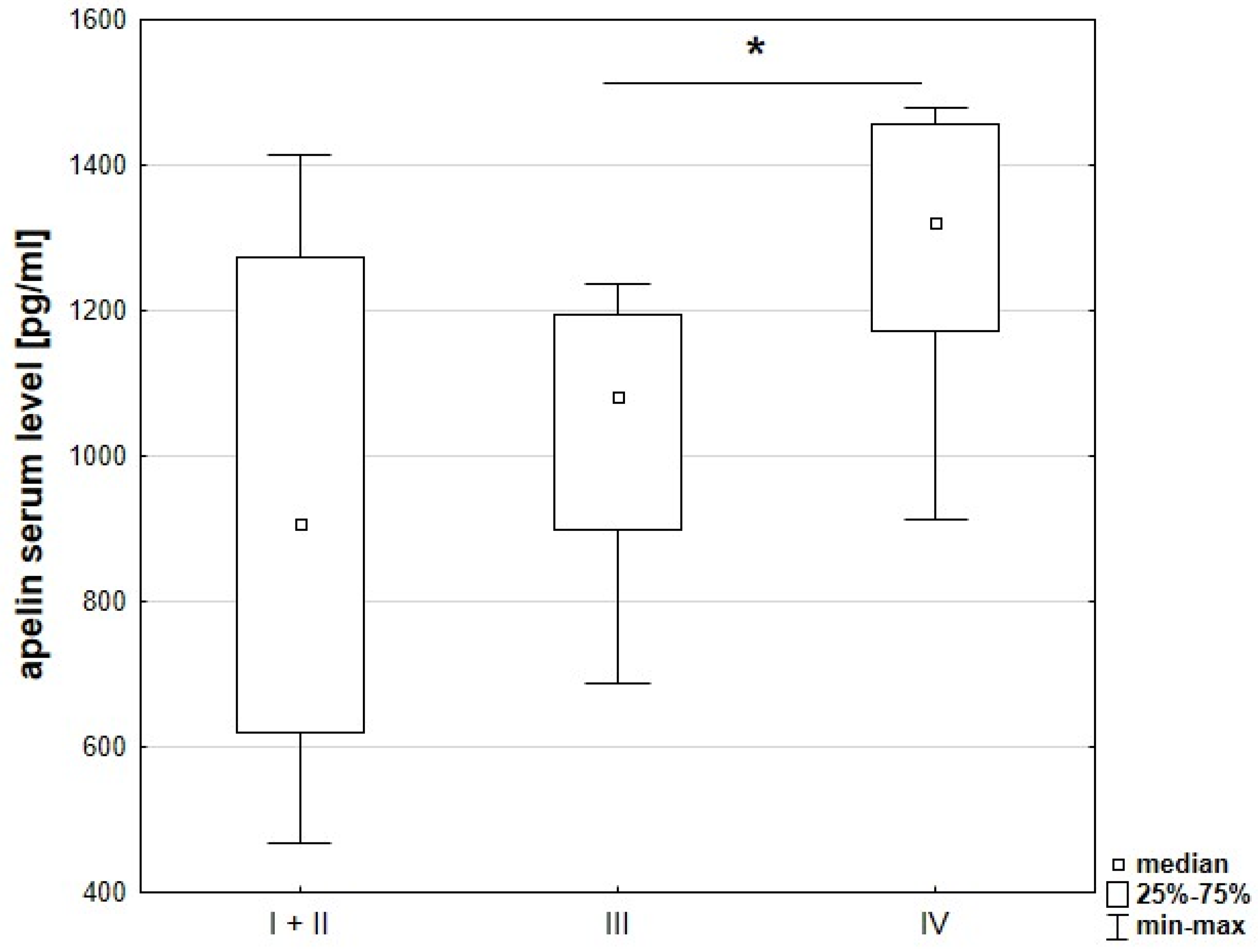
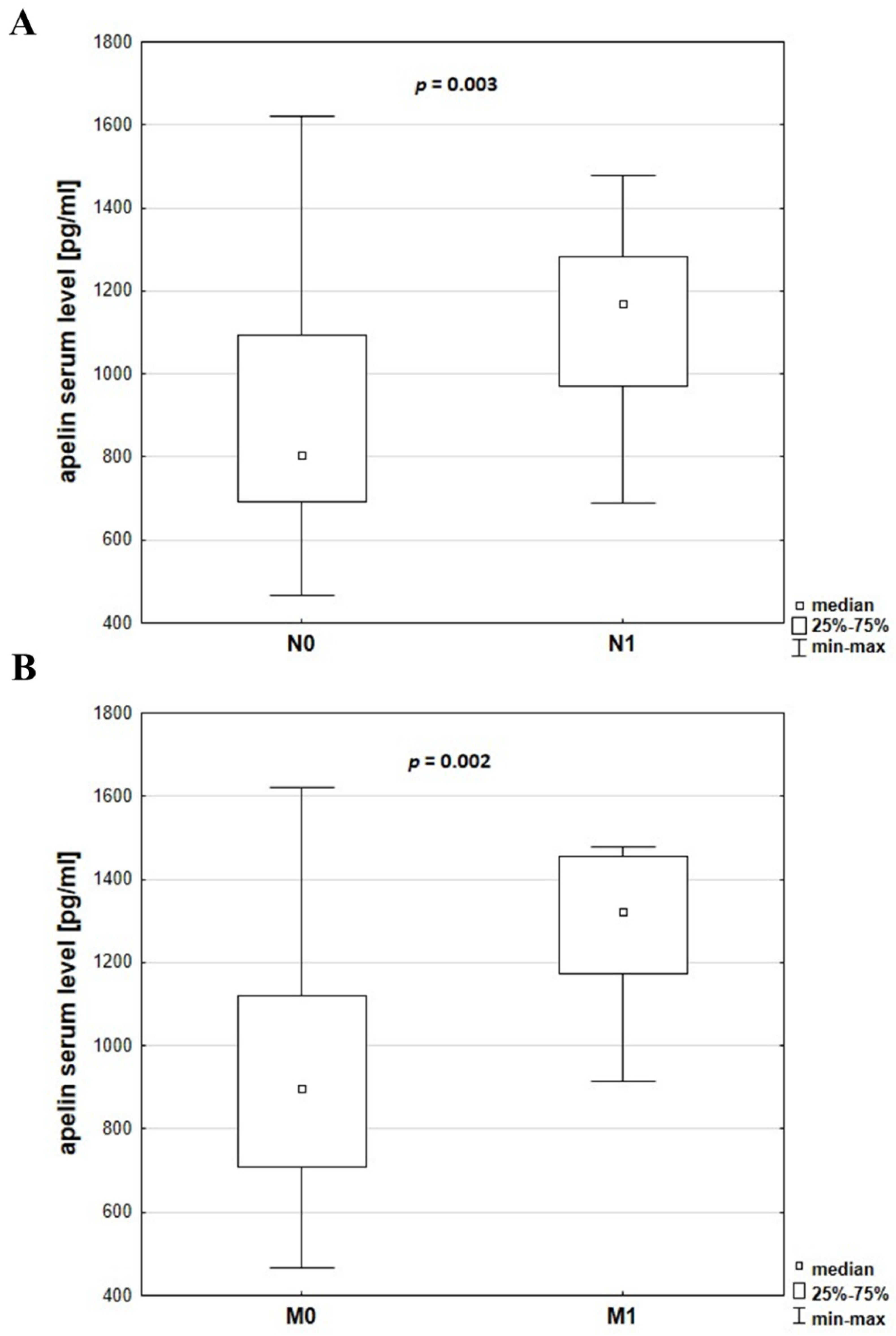
3.3. Serum Levels of Apelin and Apelin Receptor in Cancer Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Recio-Boiles, A.; Cagir, B. Cancer, Colon. 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470380/ (accessed on 27 June 2019).
- Thanikachalam, K.; Khan, G. Colorectal cancer and nutrition. Nutrients 2019, 11, 164. [Google Scholar] [CrossRef]
- Riondino, S.; Roselli, M.; Palmirotta, R.; Della-Morte, D.; Ferroni, P.; Guadagni, F. Obesity and colorectal cancer: Role of adipokines in tumor initiation and progression. World J. Gastroenterol. 2014, 14, 5177–5190. [Google Scholar] [CrossRef]
- Trayhurn, P.; Bing, C.; Wood, I.S. Adipose tissue and adipokines—Energy regulation from the human perspective. J. Nutr. 2006, 136, 1935–1939. [Google Scholar] [CrossRef]
- Tatemoto, K.; Hosoya, M.; Habata, Y.; Fujii, R.; Kakegawa, T.; Zou, M.-X.; Kawamata, Y.; Fukusumi, S.; Hinuma, S.; Kitada, C.; et al. Isolation and Characterization of a Novel Endogenous Peptide Ligand for the Human APJ Receptor. Biochem. Biophys. Res. Commun. 1998, 251, 471–476. [Google Scholar] [CrossRef]
- Wysocka, M.B.; Pietraszek-Gremplewicz, K.; Nowak, D. The role of apelin in cardiovascular diseases, obesity and cancer. Front. Physiol. 2018, 9, 15. [Google Scholar] [CrossRef]
- Zuurbier, L.; Rahman, A.; Cordes, M.; Scheick, J.; Wong, T.J.; Rustenburg, F.; Christopher Joseph, J.; Dynoodt, P.; Casey, R.; Drillenburg, P.; et al. Apelin: A putative novel predictive biomarker for bevacizumab response in colorectal cancer. Oncotarget 2017, 27, 42949–42961. [Google Scholar] [CrossRef]
- Diakowska, D.; Markocka-Ma̧czka, K.; Szelachowski, P.; Grabowski, K. Serum levels of resistin, adiponectin, and apelin in gastroesophageal cancer patients. Dis. Mark. 2014, 2014, 619649. [Google Scholar] [CrossRef]
- Feng, M.; Yao, G.; Yu, H.; Qing, Y.; Wang, K. Tumor apelin, not serum apelin, is associated with the clinical features and prognosis of gastric cancer. BMC Cancer 2016, 16, 794. [Google Scholar] [CrossRef]
- Berta, J.; Kenessey, I.; Dobos, J.; Tovari, J.; Klepetko, W.; Jan Ankersmit, H.; Hegedus, B.; Renyi-Vamos, F.; Varga, J.; Lorincz, Z.; et al. Apelin expression in human non-small cell lung cancer: role in angiogenesis and prognosis. J. Thorac. Oncol. 2010, 5, 1120–1129. [Google Scholar] [CrossRef]
- Yang, L.; Li, Y.-L.; Li, X.-Q.; Zhang, Z. High Apelin Level Indicates a Poor Prognostic Factor in Muscle-Invasive Bladder Cancer. Dis. Mark. 2019, 2019, 4586405. [Google Scholar] [CrossRef]
- Hall, C.; Ehrlich, L.; Venter, J.; O’Brien, A.; White, T.; Zhou, T.; Dang, T.; Meng, F.; Invernizzi, P.; Bernuzzi, F.; et al. Inhibition of the apelin/apelin receptor axis decreases cholangiocarcinoma growth. Cancer Lett. 2017, 386, 179–188. [Google Scholar] [CrossRef]
- Aktan, M.; Kiziltunc Ozmen, H. A preliminary study of serum apelin levels in patients with head and neck cancer. Eurasian J. Med. 2019, 51, 57–59. [Google Scholar] [CrossRef]
- Wan, Y.; Zeng, Z.C.; Xi, M.; Wan, S.; Hua, W.; Liu, Y.L.; Zhou, Y.L.; Luo, H.W.; Jiang, F.N.; Zhong, W.D. Dysregulated microRNA-224/apelin axis associated with aggressive progression and poor prognosis in patients with prostate cancer. Hum. Pathol. 2015, 46, 295–303. [Google Scholar] [CrossRef]
- Hoffmann, M.; Fiedor, E.; Ptak, A. Bisphenol A and its derivatives tetrabromobisphenol A and tetrachlorobisphenol A induce apelin expression and secretion in ovarian cancer cells through a peroxisome proliferator-activated receptor gamma-dependent mechanism. Toxicol. Lett. 2017, 269, 15–22. [Google Scholar] [CrossRef]
- Salman, T.; Demir, L.; Varol, U.; Akyol, M.; Oflazoglu, U.; Yildiz, Y.; Taskaynatan, H.; Cengiz, H.; Guvendi, G.; Kucukzeybek, Y.; et al. Serum apelin levels and body composition changes in breast cancer patients treated with an aromatase inhibitor. J. BUON 2016, 21, 1419–1424. [Google Scholar]
- Diakowska, D.; Markocka-Mączka, K.; Nienartowicz, M.; Rosińczuk, J.; Krzystek-Korpacka, M. Assessment ofapelin, apelin receptor, resistin, and adiponectin levels in the primary tumor and serum of patients with esophageal squamous cell carcinoma. Adv. Clin. Exp. Med. 2019, 28, 671–678. [Google Scholar] [CrossRef]
- Maden, M.; Pamuk, O.N.; Pamuk, G.E. High apelin levels could be used as a diagnostic marker in multiple myeloma: A comparative study. Cancer Biomark. 2017, 17, 391–396. [Google Scholar] [CrossRef]
- Harford-Wright, E.; Andre-Gregoire, G.; Jacobs, K.A.; Treps, L.; Le Gonidec, S.; Leclair, H.M.; Gonzalez-Diest, S.; Roux, Q.; Guillonneau, F.; Loussouarn, D.; et al. Pharmacological targeting of apelin impairs glioblastoma growth. Brain 2017, 140, 2939–2954. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 7th ed.; Wiley-Blackwell: Oxford, UK, 2010. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2-ΔΔCT method. Methods 2001. [Google Scholar] [CrossRef]
- Boucher, J.; Masri, B.; Daviaud, D.; Gesta, S.; Guigné, C.; Mazzucotelli, A.; Castan-Laurell, I.; Tack, I.; Knibiehler, B.; Carpéné, C.; et al. Apelin, a newly identified adipokine up-regulated by insulin and obesity. Endocrinology 2005, 146, 1764–1771. [Google Scholar] [CrossRef]
- De Falco, M.; De Luca, L.; Onori, N.; Cavallotti, I.; Artigiano, F.; Esposito, V.; De Luca, B.; Laforgia, V.; Groeger, A.M.; De Luca, A. Apelin expression in normal human tissues. In Vivo (Brooklyn) 2002, 16, 333–336. [Google Scholar]
- Podgórska, M.; Pietraszek-Gremplewicz, K.; Nowak, D. Apelin Effects Migration and Invasion Abilities of Colon Cancer Cells. Cells 2018, 7, 113. [Google Scholar] [CrossRef]
- Al-harithy, R.N.; Al-otaibi, W.A. Apelin-12 levels in Obese Patients with Colon Cancer. Cancer Immunol. Immunother. 2015, 1, 5. [Google Scholar] [CrossRef]
- Yoo, N.J.; Kim, M.S.; Lee, J.H.; An, C.H.; Lee, S.H. Expressional analysis of APLNR, an essential gene for cancer immunotherapy, in colon and prostate cancers. Pathol. Res. Pract. 2018. [Google Scholar] [CrossRef]
- Kälin, R.E.; Kretz, M.P.; Meyer, A.M.; Kispert, A.; Heppner, F.L.; Brändli, A.W. Paracrine and autocrine mechanisms of apelin signaling govern embryonic and tumor angiogenesis. Dev. Biol. 2007, 305, 599–614. [Google Scholar] [CrossRef]
- Chapman, N.A.; Dupré, D.J.; Rainey, J.K. The apelin receptor: physiology, pathology, cell signalling, and ligand modulation of a peptide-activated class A GPCR. Biochem. Cell Biol. 2014, 92, 431–440. [Google Scholar] [CrossRef]
- Buscail, E.; Chiche, L.; Laurent, C.; Vendrely, V.; Denost, Q.; Denis, J.; Thumerel, M.; Lacorte, J.; Bedel, A.; Moreau-Gaudry, F.; et al. Tumor-proximal liquid biopsy to improve diagnostic and prognostic performances of circulating tumor cells. Mol. Oncol. 2019, 13, 1811–1826. [Google Scholar] [CrossRef]
- Norcic, G. Liquid biopsy in colorectal cancer-current status and potential clinical applications. Micromachines 2018, 9, 300. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | CRC Patients (n = 56) |
|---|---|
| Gender: | |
| Female | 24 (42.9) |
| Male | 32 (57.1) |
| Age (years) | 68.4 ± 11.1 |
| Age ranges (years): | |
| <60 | 13 (23.2) |
| ≥60 | 43 (76.8) |
| BMI (kg/m2) | 27.5 ± 4.1 |
| Disease stage (TNM): | |
| I | 17 (30.4) |
| II | 17 (30.4) |
| III | 13 (23.2) |
| IV | 9 (16.0) |
| Primary tumor progression (T): | |
| T1 | 5 (8.9) |
| T2 | 14 (25.0) |
| T3 | 33 (58.9) |
| T4 | 4 (7.1) |
| Lymph node metastasis (N): | |
| N0 (no regional lymph node metastasis) | 34 (60.7) |
| N1 (regional lymph node metastasis) | 22 (39.3) |
| Distant metastasis (M): | |
| M0 (no distant metastasis) | 47 (83.9) |
| M1 (distant metastasis) | 9 (16.1) |
| Differentiation: | |
| G2 | 53 (94.6) |
| G3 | 3 (5.4) |
| Tumor location: | |
| Right colon | 20 (35.7) |
| Left colon | 33 (58.9) |
| Rectum | 3 (5.4) |
| Gene Expression | Non-tumour tissue. mean ± SD median (min–max) | Tumour tissue. mean ± SD median (min–max) | Tumour/non-tumour ratio mean ± SD median (min–max) | p-Value |
|---|---|---|---|---|
| Apelin | 0.003 ± 0.02 0.00 (0.00–0.13) | 0.006 ± 0.02 0.00065 (0.00–0.049) | 2.56 ± 6.51 0.00 (0.00–35.46) | 0.0007 * |
| Apelin receptor | 0.08 ± 0.15 0.03 (0.00–0.82) | 0.11 ± 0.17 0.04 (0.00–0.76) | 4.24 ± 8.25 1.64 (0.00–49.69) | 0.03 * |
| Variable | Non-Tumour tissue. mean ± SD median (min–max) | Tumour tissue. mean ± SD median (min–max) | Tumour/non-Tumour ratio mean ± SD median (min–max) | p-Value |
|---|---|---|---|---|
| Apelin (ng/g of tissue) | 36.00 ± 17.33 34.27 (6.05–101.6) | 48.91 ± 18.30 47.77 (4.24–113.37) | 1.68 ± 1.37 1.4 (0.21–8.44) | <0.0001 * |
| Apelin receptor (μg/g of tissue) | 10.34 ± 13.07 5.29 (0.19–54.7) | 32.32 ± 20.20 31.46 (1.11–72.35) | 7.98 ± 9.59 5.58 (0.2–53.52) | <0.0001 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podgórska, M.; Diakowska, D.; Pietraszek-Gremplewicz, K.; Nienartowicz, M.; Nowak, D. Evaluation of Apelin and Apelin Receptor Level in the Primary Tumor and Serum of Colorectal Cancer Patients. J. Clin. Med. 2019, 8, 1513. https://doi.org/10.3390/jcm8101513
Podgórska M, Diakowska D, Pietraszek-Gremplewicz K, Nienartowicz M, Nowak D. Evaluation of Apelin and Apelin Receptor Level in the Primary Tumor and Serum of Colorectal Cancer Patients. Journal of Clinical Medicine. 2019; 8(10):1513. https://doi.org/10.3390/jcm8101513
Chicago/Turabian StylePodgórska, Marta, Dorota Diakowska, Katarzyna Pietraszek-Gremplewicz, Miroslaw Nienartowicz, and Dorota Nowak. 2019. "Evaluation of Apelin and Apelin Receptor Level in the Primary Tumor and Serum of Colorectal Cancer Patients" Journal of Clinical Medicine 8, no. 10: 1513. https://doi.org/10.3390/jcm8101513
APA StylePodgórska, M., Diakowska, D., Pietraszek-Gremplewicz, K., Nienartowicz, M., & Nowak, D. (2019). Evaluation of Apelin and Apelin Receptor Level in the Primary Tumor and Serum of Colorectal Cancer Patients. Journal of Clinical Medicine, 8(10), 1513. https://doi.org/10.3390/jcm8101513