Abstract
Introduction: Tobacco smoking is a known risk factor for adverse surgical outcomes, including delayed wound healing and an increased risk of infection and nonunion. The rising use of cannabis products and alternative nicotine products, such as smokeless tobacco and electronic cigarette devices present new challenges for perioperative management, yet their influence in foot and ankle surgery is not well studied. Objectives: This scoping review aims to synthesize the existing literature on tobacco use, cannabis, and electronic cigarettes and their influence on postoperative outcomes in foot and ankle surgery. Methods: A comprehensive search of PubMed was performed using PRISMA-ScR guidelines. Eligible studies included observational studies and reviews that focus on the relationship between perioperative substance use and foot and ankle surgery complications. Results: There is a wide range of evidence that supports increased wound and bone healing complications with use of combustible tobacco. Data on the effects of smokeless tobacco, electronic cigarettes, and cannabis on this patient population is limited, with most evidence drawn from animal studies or broader orthopaedic literature. Conclusions: The existing data raises potential concern for adverse effects with use of these products. By identifying existing findings and gaps in the literature, this review highlights the need for further research on the perioperative effects of these substances in foot and ankle surgery.
1. Introduction
Tobacco smoking is associated with poor surgical outcomes, particularly in orthopaedic procedures, where they can contribute to impaired wound healing, increased rates of infection, and delayed or failed osseous union [1,2]. Combustible tobacco use, in the form of cigarette smoking, causes vasoconstriction, tissue hypoxia, and impaired inflammatory and cellular responses [3]. Smoking has been independently associated with increased rates of wound healing complications, delayed union, nonunion, and poorer functional outcomes after foot and ankle surgery [3,4].
While the negative outcomes of combustible tobacco are well understood, the impacts of smokeless tobacco, electronic cigarettes, and cannabis have not been as extensively studied. Despite a decline in smoking rates over the last 50 years in the United States (U.S.), the use of tobacco products is still prevalent. Recent data estimate that 41 million adults (18.7%) in the U.S. use tobacco products, including cigarettes (11.5%), electronic cigarettes (e-cigarettes) (4.5%), cigars (3.5%), and smokeless tobacco (2.1%) [5].
1.1. Combustible Tobacco
Combustible tobacco, such as cigarette smoking, contains more than 4000 toxic compounds. Among these include carbon monoxide and hydrogen cyanide, which reduce oxygenation to tissues and can impair cellular function [6,7]. Nicotine is rapidly absorbed during smoking and stimulates the sympathetic nervous system. This results in catecholamine release and sustained vasoconstriction [7,8]. As a result, this physiological response leads to decreased perfusion and impaired tissue oxygenation. In the context of foot and ankle surgery, smoking in the perioperative period has been linked to delayed wound healing, as well as increased rates of infection and nonunion [4,9,10].
1.2. Smokeless Tobacco
Smokeless tobacco products, such as chewing tobacco and snuff, contain nicotine but lack the combustion byproducts present in cigarettes. Nicotine from smokeless products is readily absorbed through the oral mucosa and can reach plasma concentrations comparable to, or even exceeding, those achieved from cigarettes. Recent literature indicates rising nicotine pouch use, especially in the younger population. These pouches are sold in various flavors and are marketed on social media platforms that are frequented by younger populations [11]. Between 2023 and 2024, nicotine pouch prevalence doubled from 1.3% to 2.6% among U.S. high school students [12]. Although smokeless tobacco products may be perceived as safer alternatives to smoking, they still can deliver high concentrations of nicotine that can cause vasoconstriction and impair the tissue healing processes [13,14]. The effects of smokeless tobacco use on surgical outcomes, particularly foot and ankle specific, remain scarce in the literature, warranting further investigation.
1.3. E-Cigarettes and Vaping
E-cigarettes, also known as vaping devices, have gained popularity as an alternative to cigarette smoking since the early 2000s. These devices consist of a cartridge filled with an e-liquid solution (containing propylene glycol, vegetable glycerin, flavorings, and other chemical additives), a heating element, and a battery. Nicotine is delivered through these aerosolized liquids [15]. In 2021, 4.5% of adults in the U.S. reported current e-cigarette use which is disproportionately higher in adults ages 18–24 (11%). Evidence from youth surveys indicates a shift toward dual nicotine use with both vape devices and nicotine pouches [4].
E-cigarettes have been associated with biological effects that may negatively impact tissue repair, which include oxidative stress, inflammation, and endothelial dysfunction [16]. Higher-powered vaping devices can deliver nicotine concentrations that are comparable to traditional cigarettes, raising similar concerns for potential negative effects at the tissue level [17]. Like smokeless tobacco, there is limited literature reporting the impact of electronic cigarette use on orthopaedic surgery outcomes.
1.4. Cannabis
Cannabis is one of the most used psychoactive substances in the U.S., with both recreational and medicinal use increasing following expanding legalization. In 2024, an estimated 17% of U.S. adults reported cannabis use [18]. In this review, “cannabis” includes all forms of Cannabis sativa and its derivatives, regardless of route of administration. The term “marijuana” is used interchangeably throughout the literature, including in this review, to refer to cannabis products that contain delta-9-tetrahydrocannabinol (THC), the primary psychoactive compound. Cannabis contains over 100 cannabinoids, including THC and cannabidiol (CBD), which have been studied for potential therapeutic applications [2,19,20]. In addition to the numerous formulations of cannabis, there is also variability in route of administration (inhalation, edibles, topicals), frequency of use, and medical versus recreational use.
Within orthopaedic literature, marijuana use has been examined in relation to bone mineral density, fracture healing, and perioperative outcomes [2]. Given the variability in findings and the growing prevalence of cannabis use among surgical patients, understanding its perioperative implications has become increasingly relevant for surgeons.
Together, cigarette smoking, smokeless tobacco, e-cigarettes, and cannabis represent a range of commonly used substances that may have an impact on surgical outcomes. Synthesizing the current evidence on their perioperative use in foot and ankle surgery can help identify patterns in the literature, ultimately guiding patient education and clinical decision making. The purpose of this scoping review is to summarize existing studies that evaluate the effects of these substances on postoperative outcomes in foot and ankle procedures.
2. Materials and Methods
This scoping review synthesizes current literature on the effects of smoking, smokeless tobacco, e-cigarette use, and cannabis on outcomes in foot and ankle surgery. The objective of this review is to provide a broad but clinically relevant overview of the available literature without conducting a formal analysis. PRISMA-ScR guidelines were followed, and a pre-registered protocol was not conducted.
The PubMed database was used to perform a targeted literature search on 1 July 2025. This database was selected for its extensive coverage of peer-reviewed biomedical and clinical literature, as well as its accessibility and relevance to the scope of this review. The following search terms were used: “smoking,” “tobacco,” “smokeless tobacco,” “e-cigarette,” “electronic cigarette,” “vaping,” cannabis,” “marijuana,” AND “foot surgery,” “ankle surgery,” “postoperative,” “outcomes,” or “complications.” This search was limited to publications in English, as well those involving human subjects.
Studies were included if they evaluated the impact of any of the previously mentioned substances on surgical outcomes related to the foot and/or ankle and provided clearly defined methods and measurable postoperative outcomes. Eligible studies included case studies, randomized controlled trails, cohort studies, case–control studies, and systematic reviews. Studies that did not focus on postoperative outcomes with reference to substance use or were not specific to foot and ankle procedures were excluded. Additionally, animal studies and non-peer-reviewed sources were excluded from the review’s primary analysis. During the data extraction phase, overlaps between individual studies and the reference lists of included systematic reviews were identified. When a primary study was also included in a systematic review, we recorded it separately but noted the overlap to avoid over-representing the findings during interpretation.
The initial screening was conducted based on literature titles and abstracts to assess for relevance to this review. Then, a full-text review was performed for all articles that met the initial criteria. These articles were selected based on the lead author’s assessment of their relevance to the relationship between the previously defined substance use and surgical outcomes in foot and ankle surgery. Final inclusion was guided by each study’s methodological transparency, as well as clarity of reported outcomes and overall study quality.
A data charting form was created to extract key information from each included study. The following data were collected: author information, year of publication, study design, population demographics, sample size, substance investigated, surgical procedure performed, outcome measures, and overall findings. No assumptions were made beyond the reported data in the studies.
Studies were grouped by substance type: smoking, smokeless tobacco, e-cigarettes/vaping, and cannabis. Studies that examined tobacco smoking and smokeless tobacco separately were included; those that examined all forms of tobacco together were excluded. Overall themes, trends in outcomes, and study strengths/deficiencies were identified. A formal critical appraisal of individual studies was not conducted, but study design, sample size, methodological quality, and relevance to this review’s goals were considered during the selection process. The final selection for study inclusion was made by the lead author. A meta-analysis was not performed due to the heterogeneity of the included studies, as well as the scoping nature of this review, which aimed to identify patterns and gaps in the existing literature rather than to statistically synthesize outcomes.
A total of 548 studies were identified through the PubMed database search on 1 July 2025. After the initial screening of titles and abstracts, 510 studies remained. Following a full text review, 10 studies were included in the final analysis (Figure 1). Articles were excluded due to lack of relevance, absence of surgical outcome data, or failure to focus on the effects of the substances of interest.
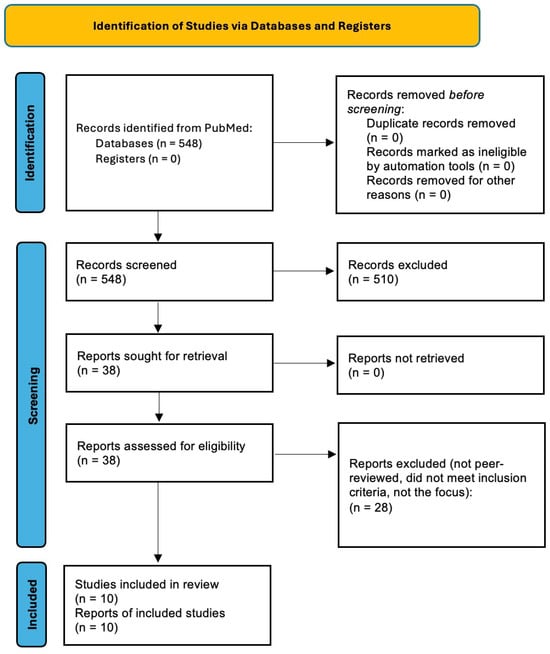
Figure 1.
PRISMA scoping review flow diagram of study-selection process.
3. Results
Ten studies examining postoperative outcomes in foot and ankle surgery in relation to tobacco, e-cigarette, and cannabis use were selected for the final analysis in this scoping review. Retrospective cohort studies, systematic reviews, and meta-analyses that focused on postoperative foot and ankle surgery outcomes were included. Study selection prioritized clinical relevance, methodological strength, and clarity of results. This approach was taken to ensure a focused but comprehensive analysis that aligned with the goals of this review. The characteristics of the included studies are summarized in Table 1, Table 2 and Table 3, including the design, population, and main findings.
3.1. Tobacco Smoking
Seven studies were compared regarding the effects of tobacco smoking on foot and ankle surgery (Table 1). A systematic review by Pour Jafar et al. compared various foot and ankle procedure outcomes among smokers and non-smokers [4]. They reported smokers exhibiting a 14.8% wound infection rate. Higher rates of malunion and non-union were reported in smokers (14.5%) as compared to non-smokers (6.7%). Additionally, smokers who underwent total ankle replacements (TAR) had lower reported postoperative functional outcome scores. A systematic review by Le et al. focused primarily on smoking influence on TAR outcomes and found an increase in wound healing complications in patients who smoked, especially during the perioperative period [21].

Table 1.
Summary of Included Studies on Tobacco Smoking in Foot and Ankle Surgery.
Table 1.
Summary of Included Studies on Tobacco Smoking in Foot and Ankle Surgery.
| Citation | Study Design | Procedure | Sample Size | Outcomes Measured | Key Findings | Notes |
|---|---|---|---|---|---|---|
| Pour Jafar et al. [4] | Systematic Review | Various foot and ankle surgeries | 15 studies included | Wound complications, delayed unions, nonunion, and infection | Smoking associated with increased risk of wound complications, delayed union, nonunion, and infection; lower functional outcome scores | - |
| Le et al. [21] | Meta-analysis | TAR | 12 studies included | Postoperative complications | Smoking is a significant risk factor for poor outcomes following TAR | - |
| Lampley et al. [22] a | Retrospective Cohort | TAR | 642 patients | Postoperative infection, wound dehiscence, and revisions | Current smokers had significantly higher wound breakdown (11.8%) complications compared to nonsmokers (p = 0.047) | Compared current, former, and non-smokers separately |
| Bettin et al. [23] | Retrospective Cohort | Forefoot surgery | 602 patients | Wound healing and postoperative infection | Current smokers had more postoperative complications (36.4%) (delayed union, infection, delayed wound healing, pain) than former smokers (16.5%) and nonsmokers (8.5%) | Compared current, former, and non-smokers separately |
| Jerjes et al. [24] | Retrospective Comparative | Ankle fracture ORIF | 440 patients | Time to fracture union, wound healing, swelling, pain, and infection | Chronic heavy smokers had increased rates of postoperative pain, swelling at fracture site, superficial and deep infection, and delayed wound healing and osseous union |
|
| Ischikawa et al. [25] | Retrospective Cohort | Hindfoot arthrodesis | 148 patients | Wound and osseous healing | Relative risk of developing a nonunion was 2.7 times higher for active smokers than nonsmokers | Compared current, former, and non-smokers separately |
| Lee et al. [26] | Retrospective Cohort | Lateral ankle ligament reconstruction | 105 patients | Wound healing, infection, and outcome scores | No difference in outcomes between groups. Wound complications more common in smoking group (not significant) |
|
Abbreviations: ORIF, open reduction internal fixation; TAR, total ankle replacement. a Study also included in systematic review by Pour Jafar et al.
Lampley et al. compared TAR complications among active smokers, former smokers, and nonsmokers. They found a statistically significant increased risk of wound breakdown postoperatively in the active smoking group (p = 0.47) [22]. Active smokers in this study had an increased rate of infection and revision surgery; however, the findings were not statistically significant (p = 0.39 and p = 0.47, respectively). Similarly, Bettin et al. reported a higher risk of forefoot surgery postoperative complications in active smokers (36.4%) than patients who previously smoked (16.5%) or never smoked (8.5%) [23].
A 2024 retrospective comparative review with 220 age- and sex-matched individuals who were chronic heavy smokers (CHSs), or nonsmokers were evaluated for closed ankle fracture healing [24]. The surgical cohort of CHSs exhibited a significant increase in ankle fracture time to union, as well as increased postoperative pain, swelling at fracture site, and infection. Ischikawa et al. reported that active smoking in the hindfoot arthrodesis perioperative was associated with a 2.7-fold increased risk of nonunion [25]. Lastly, Lee et al. compared postoperative outcomes after lateral ankle ligament reconstruction between smokers and nonsmokers and found no significant differences overall, although the smoking cohort did demonstrate higher wound healing complications that did not reach statistical significance [26].
3.2. Smokeless Tobacco
Only one study met inclusion criteria for smokeless tobacco use in the context of foot and ankle surgery (Table 2). Winter et al. conducted a retrospective cohort that evaluated 131 patients who used smokeless tobacco and underwent hindfoot or ankle arthrodesis [13]. This study found that within 90 days of the procedure, smokeless tobacco users experienced significantly higher rates of hardware removals, wound complications, infection, and nonunion compared to the tobacco-naïve cohort. To date, this was the only study identified that met inclusion criteria which evaluated smokeless tobacco use as a distinct exposure in a foot and ankle surgical population.
Table 2.
Summary of the Included Study on Smokeless Tobacco in Foot and Ankle Surgery.
Table 2.
Summary of the Included Study on Smokeless Tobacco in Foot and Ankle Surgery.
| Citation | Study Design | Procedure | Sample Size | Outcomes Measured | Key Findings | 1-Year Complications Tobacco Users vs. Tobacco-Naïve | Notes |
|---|---|---|---|---|---|---|---|
| Winter et al. [13] | Retrospective Cohort | Ankle or hindfoot arthrodesis | 655 | Postoperative complications at 90 days, 1 year and 2 years | Higher complication rates in smokeless tobacco users at all postoperative time points compared to tobacco-naïve patients |
| Compared non-tobacco users, smokers, and smokeless tobacco users separately |
3.3. E-Cigarette/Vaping
No studies evaluating the impact of e-cigarette or vaping use on postoperative outcomes in foot and ankle surgery met the inclusion criteria for this review.
3.4. Cannabis
Two studies met inclusion criteria for cannabis use in the perioperative period after foot and ankle surgery (Table 3). Holle et al. conducted a retrospective cohort study among patients who underwent ankle or hindfoot arthrodesis and found no statistically significant difference between cannabis users and the control group on 90-day and 2-year postoperative risks [18]. Dhodapkar examined cannabis users who underwent operative fixation for ankle fractures [27]. No increase in 90-day postoperative complications or readmission in the cannabis user cohort was found when compared to the control cohort. Both studies also evaluated tobacco and dual-use cohorts, but for this review, only cohorts with cannabis use in isolation were included.
Table 3.
Summary of the Included Studies on Cannabis use in Foot and Ankle Surgery.
Table 3.
Summary of the Included Studies on Cannabis use in Foot and Ankle Surgery.
| Citation | Study Design | Procedure | Sample Size | Outcomes Measured | Key Findings | Notes |
|---|---|---|---|---|---|---|
| Holle et al. [18] | Retrospective Cohort | Ankle or hindfoot arthrodesis | 380 cannabis-only users | 90-day and 2-year postoperative complications | No increased risk of complications compared to non-users |
|
| Dhodapkar et al. [27] | Retrospective Cohort | Ankle fracture ORIF | 867 cannabis-only users | 90-day postoperative complications | No increased risk of complications compared to non-users |
|
Lastly, Table 4 was created to summarize findings of all the substance uses. Perioperative smoking and smokeless tobacco both negatively impact postoperative outcomes. Cannabis use in the foot and ankle literature was not shown to increase postoperative risk.
Table 4.
Overview of Substance Use and Surgical Outcomes.
4. Discussion
The goal of this scoping review was to evaluate the impact of various forms of substance use (tobacco smoking, smokeless tobacco, e-cigarettes, and cannabis) on postoperative outcomes in foot and ankle surgery. Among the included studies, tobacco smoking was the most consistently associated with increased complications, including delayed wound healing, infection, and nonunion. Fewer studies were identified for smokeless tobacco, e-cigarettes and cannabis. Additionally, the evidence remains limited in these areas. While the findings suggest potential risks related to certain substances, the overall heterogeneity of study designs and each study’s exposure definitions made direct comparisons difficult. These results stress the importance of further research to better understand how substance use may affect foot and ankle surgery outcomes.
The findings from Winter et al. suggest that smokeless tobacco may be associated with an increased risk of complications following ankle or hindfoot arthrodesis [13]. Although the foot and ankle literature is sparse in isolating smokeless tobacco specifically, this study provides the preliminary evidence that smokeless tobacco, like chewing tobacco, may negatively affect surgical outcomes. In other orthopaedic populations, such as total hip arthroplasty, smokeless tobacco users were found to have significantly higher rates of wound dehiscence, readmission rates, and longer hospital stays as compared to the tobacco naïve controls [28]. Similarly, smokeless tobacco users who underwent anterior cruciate ligament reconstruction were found to have an increased risk of postoperative complications and emergency department utilization [29]. The scarcity of smokeless tobacco-related research on foot and ankle surgery patient populations highlights the need for further research on outcomes.
While no foot and ankle specific studies related to e-cigarette and vaping use were identified, there are several investigations in the orthopaedic and surgical literature that suggests that e-cigarette use may affect postoperative healing. In 2023, Ashour et al. conducted a systematic review that reported delayed healing, disrupted collagen organization, and altered inflammatory responses after e-cigarette use [30]. This systematic review included articles with human volunteers, human cell lines, and animal rat models. Authors concluded that e-cigarettes should be treated the same as tobacco cigarettes and should not be used in the perioperative setting.
Troiano et al. raised and repaired skin flaps on rat models who were exposed to e-cigarette vapors and e-cigarette smoke [31]. This experiment found no difference in flap necrosis between the e-cigarette vapor and cigarette smoke-exposed rats. However, there was a significant difference in flap necrosis in both e-cigarette vapor and cigarette smoke exposed groups to the control. Authors of this study concluded that the use of vaping/e-cigarettes were equally detrimental to wound healing as cigarette smoking and that e-cigarettes should not be used as an alternative to combustible smoking in the perioperative setting. Lastly, Amaro et al. reviewed the perioperative risks of vaping in orthopaedic patients. Ultimately, authors reported that vaping negatively impacts surgical outcomes, as the vapors are associated with cytotoxicity, pro-inflammatory effects, and a decrease in microbial defense [32].
Foot and ankle surgery-specific literature evaluating the effects of cannabis use is limited. Differences in route of administration, dosage, and cannabinoid content may influence perioperative outcomes in different ways. Unfortunately, most existing studies in foot and ankle surgery do not report or control for these factors, limiting the ability to draw conclusions about specific risks and benefits. This area of heterogeneity underscores an area for additional research, particularly in studies that stratify patient outcomes by use patterns or cannabis formulations. In this review, among the two studies that met inclusion criteria for cannabis use in the perioperative setting, both reported no increase in complications postoperatively with isolated cannabis use [18,27]. It is worth noting that both studies evaluated the complication rates with combined cannabis and tobacco use as well, with the dual-use cohort reporting higher rates of postoperative complications.
When investigating the broader orthopaedic literature, Health et al. reported that cannabis use may interfere with bone metabolism and delay fracture and wound healing in pediatric patients [33]. Their study found an increased time to fracture healing among adolescent cannabis users. Similarly, Albelo et al. found that preoperative recreational marijuana use was associated with poorer patient outcomes 2-years postoperatively [34].
Conversely, some literature suggests that cannabis use does not significantly increase postoperative risks. For example, Ruckle et al. found no increase in wound healing complications or infection rates following orthopaedic surgery in active marijuana users [35]. Additionally, Moon et al. reported no connection between marijuana use and mortality after orthopaedic surgery [36]. Of note, variations in cannabis dose, route of administration, and frequency were not controlled and may account for conflicting results. It is evident that cannabis use in current orthopaedic literature is inconclusive but does raise concern for possible risks related to healing and postoperative complications. This is especially true when cannabis is used in combination with tobacco products. More high-quality studies are needed, focusing on the foot and ankle patient population, for guided perioperative counseling.
Smoking cessation before surgery and during the postoperative period is recommended, as continued use is linked to increased complications [4,21,22,23,24,25,26]. Patients undergoing TAR may be at particularly elevated risks for postoperative complications. The presence of metallic implants increases the risk of periprosthetic infection due to the potential for bacterial adhesion and biofilm formation, protecting pathogens from immune responses and antimicrobial therapy. Infections in this situation are difficult to eradicate and can compromise the prosthetic joint. This point is relevant in the context of modifiable risk factors such as nicotine use, which impairs perfusion and the immune system [22,37]. Rozinthe et al. found that smokers who stopped smoking preoperatively had less wound healing complications and lower complication rates than those who continued smoking during the perioperative period [3]. Literature recommends patients stop smoking 4–8 weeks before surgery to allow for partial reversal of vasoconstriction and inflammatory effects [3,38,39]. In foot and ankle surgery literature, Lampley et al. found that there was no significant difference in TAR outcome scores when comparing former smokers to nonsmokers, suggesting that tobacco cessation efforts may improve overall outcomes [22]. In the setting of TAR, E-cigarette, smokeless tobacco, and cannabis cessation in the perioperative period is not as extensively studied, indicating a need for future research in this area.
This review is not without limitations. First, even with a structed and targeted literature search, this review was limited to one database, PubMed, which may have excluded relevant studies published elsewhere. Second, the heterogeneity across study designs, outcome measures, surgical procedures, and patient populations limited the direct comparison of results across studies. Third, only studies that evaluated tobacco smoking or smokeless tobacco as separate exposures, not combined, were included. Studies that grouped multiple forms of tobacco together without differentiating their effects were excluded in attempt to maintain clarity. For example, Dhodapkar et al. found that, in general, tobacco users who underwent ankle open reduction internal fixation had worse postoperative outcomes. However, authors did not distinguish the forms of tobacco that were evaluated [27]. As a result, this study was excluded from the summary.
Another limitation of this scoping review is the absence of a preregistered protocol. While a structed and systematic approach was used to gather the literature included, the absence of protocol registration may introduce potential for selection bias. No formal risk of bias assessment was conducted in this review. Without multiple independent reviewers, subjectivity may have also been introduced in the literature selection process. The lead author selected studies based on their relevance to the topic and methodological quality which was determined via full-text review.
Lastly, another identified limitation of this review was the presence of overlap between an included primary study and one summarized within a systematic review [4,22]. Both studies were retained in this synthesis due to their differing scopes and levels of evidence; however, it is important to note this as to not over-emphasize the findings. This is a known occurrence in scoping reviews, particularly when both types of evidence are included to broadly map the current literature.
Patients who undergo procedures such as TAR and ankle arthrodesis may face complications such as infection, wound healing issues, and nonunion, so the role of modifiable risk factors such as tobacco and cannabis use warrants close consideration. This is especially relevant in the context of existing literature that outlines the baseline risk of postoperative complications following these procedures [4,13,18,22,40].
5. Conclusions
This review highlights tobacco smoking as a well-established risk factor for postoperative complications in foot and ankle surgery. In contrast, the evidence for smokeless tobacco, e-cigarettes, and cannabis is limited, particularly in the setting of foot and ankle surgery. Although emerging data suggest these substances may contribute to impaired healing or increased complication risk, the current literature lacks consistent reporting on patterns of use, routes of administration, and perioperative outcomes. These findings highlight the importance of preoperative screening and patient counseling, as well as the need for more focused research to better understand the perioperative risks in this surgical population.
Author Contributions
Conceptualization, methodology, investigation, writing, review, and editing: J.A.K. and L.K.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
This article is a comprehensive review and does not include any original data. The sources of all the derived data are cited throughout the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ORIF | Open reduction internal fixation |
| TAR | Total ankle replacement |
References
- Hernigou, J.; Schuind, F. Tobacco and bone fractures: A review of the facts and issues that every orthopaedic surgeon should know. Bone Jt. Res. 2019, 8, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Heath, D.M.; Koslosky, E.J.; Bartush, K.C.; Hogue, G.D. Marijuana in Orthopaedics: Effects on Bone Health, Wound-Healing, Surgical Complications, and Pain Management. JBJS Rev. 2022, 10, e21.00184. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.T. Wound healing and infection in surgery: The pathophysiological impact of smoking, smoking cessation, and nicotine replacement therapy: A systematic review. Ann. Surg. 2012, 255, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Pour Jafar, S.; Garibaldi, R.; Seidel, A.; Soares, S. Smoking-related complications in foot and ankle surgery: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 4691–4700. [Google Scholar] [CrossRef]
- Cornelius, M.E.; Loretan, C.G.; Jamal, A.; Lynn, B.C.D.; Mayer, M.; Alcantara, I.C.; Neff, L. Tobacco Product Use Among Adults —United States, 2021. MMWR Morb. Mortal Wkly. Rep. 2023, 72, 475–483. [Google Scholar] [CrossRef]
- Silverstein, P. Smoking and wound healing. Am. J. Med. 1992, 93, S22–S24. [Google Scholar] [CrossRef]
- McDaniel, J.C.; Browning, K.K. Smoking, chronic wound healing, and implications for evidence-based practice. J. Wound Ostomy Cont. Nurs. 2014, 41, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Seravalle, G.; A Calhoun, D.; Bolla, G.B.; Giannattasio, C.; Marabini, M.; Del Bo, A.; Mancia, G. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994, 90, 248–253. [Google Scholar] [CrossRef]
- Beahrs, T.R.; Reagan, J.; Bettin, C.C.; Grear, B.J.; Murphy, G.A.; Richardson, D.R. Smoking Effects in Foot and Ankle Surgery: An Evidence-Based Review. Foot Ankle Int. 2019, 40, 1226–1232. [Google Scholar] [CrossRef]
- Malay, D.S. Cigarette smoking and foot and ankle surgery. J. Foot Ankle Surg. 2011, 50, 515–516. [Google Scholar] [CrossRef]
- Han, D.-H.; Harlow, A.F.; Miech, R.A.; Bae, D.; Cho, J.; Dai, H.D.; Sussman, S.Y.; Sanchez, L.M.; Meza, L.; Leventhal, A.M. Nicotine Pouch and E-Cigarette Use and Co-Use Among US Youths in 2023 and 2024. JAMA Netw. Open 2025, 8, e2567399. [Google Scholar] [CrossRef]
- Park-Lee, E.; Jamal, A.; Cowan, H.; Sawdey, M.D.; Cooper, M.R.; Birdsey, H.; West, A.; Cullen, K.A. Notes from the Field: E-Cigarette and Nicotine Pouch Use Among Middle and High School Students—United States, 2024. MMWR Morb. Mortal. Wkly. Rep. 2024, 73, 774–778. [Google Scholar] [CrossRef]
- Winter, J.E.; Budin, J.S.; Delvadia, B.P.; Cole, M.W.; Waters, T.L.; Schiff, A.P.; Sherman, W.F. Association of Smokeless Tobacco and Complications Following Ankle and Hindfoot Arthrodesis. Foot Ankle Int. 2024, 45, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Heyes, G.; Weigelt, L.; Molloy, A.; Mason, L. The influence of smoking on foot and ankle surgery: A review of the literature. Foot 2021, 46, 101735. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Fraiman, J.B. Cardiovascular effects of electronic cigarettes. Nat. Rev. Cardiol. 2017, 14, 447–456. [Google Scholar] [CrossRef]
- Fetterman, J.L.; Weisbrod, R.M.; Feng, B.; Bastin, R.; Tuttle, S.T.; Holbrook, M.; Baker, G.; Robertson, R.M.; Conklin, D.J.; Bhatnagar, A.; et al. Flavorings in Tobacco Products Induce Endothelial Cell Dysfunction. Arter. Thromb. Vasc. Biol. 2018, 38, 1607–1615. [Google Scholar] [CrossRef]
- Prochaska, J.J.; A Vogel, E.; Benowitz, N. Nicotine delivery and cigarette equivalents from vaping a JUULpod. Tob. Control 2022, 31, e88–e93. [Google Scholar] [CrossRef] [PubMed]
- Holle, A.M.; Beckett, N.C.; Iturregui, J.M.; Haglin, J.M.; Kile, T.A. The Association of Cannabis and Tobacco Use With Postoperative Complications after Ankle and Hindfoot Arthrodesis. Foot Ankle Orthop. 2025, 10, 24730114251328669. [Google Scholar] [CrossRef]
- Leinen, Z.J.; Mohan, R.; Premadasa, L.S.; Acharya, A.; Mohan, M.; Byrareddy, S.N. Therapeutic Potential of Cannabis: A Comprehensive Review of Current and Future Applications. Biomedicines 2023, 11, 2630. [Google Scholar] [CrossRef]
- Andreae, M.H.; Carter, G.M.; Shaparin, N.; Suslov, K.; Ellis, R.J.; Ware, M.A.; Abrams, D.I.; Prasad, H.; Wilsey, B.; Indyk, D.; et al. Inhaled Cannabis for Chronic Neuropathic Pain: A Meta-analysis of Individual Patient Data. J. Pain 2015, 16, 1221–1232. [Google Scholar] [CrossRef]
- Le, Y.T.T.; Tran, D.N.A.; Nguyen, B.T.T.; Nguyen, T.T.; Chen, Y.-P.; Kuo, Y.-J. Is smoking a risk factor for complications following total ankle arthroplasty? A meta-analysis. Foot Ankle Surg. 2025, 31, 50–57. [Google Scholar] [CrossRef]
- Lampley, A.; Gross, C.E.; Green, C.L.; DeOrio, J.K.; Easley, M.; Adams, S.; Nunley, J.A., 2nd. Association of Cigarette Use and Complication Rates and Outcomes Following Total Ankle Arthroplasty. Foot Ankle Int. 2016, 37, 1052–1059. [Google Scholar] [CrossRef]
- Bettin, C.C.; Gower, K.; McCormick, K.; Wan, J.Y.; Ishikawa, S.N.; Richardson, D.R.; Murphy, G.A. Cigarette smoking increases complication rate in forefoot surgery. Foot Ankle Int. 2015, 36, 488–493. [Google Scholar] [CrossRef]
- Jerjes, W.; Ramsay, D.; Stevenson, H.; Yousif, A. Effect of chronic heavy tobacco smoking on ankle fracture healing. Foot Ankle Surg. 2024, 30, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, S.N.; Murphy, G.A.; Richardson, E.G. The effect of cigarette smoking on hindfoot fusions. Foot Ankle Int. 2002, 23, 996–998. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-O.; Eom, J.-S.; Jung, H.-G. The effect of smoking on the outcomes of lateral ankle ligament reconstruction. J. Orthop. Sci. 2018, 23, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Dhodapkar, M.M.; Oghenesume, O.P.; Halperin, S.J.; Modrak, M.; Yoo, B.J.; Grauer, J.N. Adverse Events After Ankle Fracture Open Reduction Internal Fixation Among Patients With and Without Documented Cannabis and Tobacco Use. Foot Ankle Int. 2023, 44, 941–948. [Google Scholar] [CrossRef]
- Waters, T.L.; Collins, L.K.; Cole, M.W.; Springer, B.D.; Salas, Z.; Sherman, W.F. Smokeless Tobacco Use is Associated With Worse Medical and Surgical Outcomes Following Total Hip Arthroplasty. J. Arthroplast. 2024, 39, 441–447. [Google Scholar] [CrossRef]
- Holle, A.M.; Tummala, S.V.; Pejic, J.; Van Schuyver, P.R.; Chhabra, A.; Economopoulos, K.J. Association of Smokeless Tobacco Use With Perioperative Complications and Revision Surgery After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2025, 53, 308–314. [Google Scholar] [CrossRef]
- Ashour, O.; Al-Huneidy, L.; Noordeen, H. The implications of vaping on surgical wound healing: A systematic review. Surgery 2023, 173, 1452–1462. [Google Scholar] [CrossRef] [PubMed]
- Troiano, C.; Jaleel, Z.; Spiegel, J.H. Association of Electronic Cigarette Vaping and Cigarette Smoking With Decreased Random Flap Viability in Rats. AMA Facial Plast. Surg. 2019, 21, 5–10. [Google Scholar] [CrossRef]
- Amaro, E.J.; Shepard, N.; Moss, L.; Karamitopoulos, M.; Lajam, C. Vaping and Orthopaedic Surgery: A Review of Current Knowledge. JBJS Rev. 2019, 7, e5. [Google Scholar] [CrossRef]
- Heath, D.; Ghali, A.B.; Momtaz, D.B.; Lee, L.B.; Hogue, G. Marijuana Use Results in Increased Time to Union in Surgically Treated Pediatric Fracture Patients. J. Orthop. Trauma 2022, 36, e106–e110. [Google Scholar] [CrossRef]
- Albelo, F.D.; Baker, M.; Zhang, T.; Schneider, M.B.; Jauregui, J.J.; Nadarajah, V.; Meredith, S.J.; Packer, J.D.; Henn, R.F. Impact of pre-operative recreational marijuana use on outcomes two years after orthopaedic surgery. Int. Orthop. 2021, 45, 2483–2490. [Google Scholar] [CrossRef]
- Ruckle, D.; Chang, A.; Jesurajan, J.; Carlson, B.; Gulbrandsen, M.; Rice, R.C.; Wongworawat, M.D. Does Marijuana Smoking Increase the Odds of Surgical Site Infection After Orthopaedic Surgery? A Retrospective Cohort Study. J. Orthop. Trauma 2024, 38, 571–575. [Google Scholar] [CrossRef]
- Moon, A.S.; Smith, W.; Mullen, S.; Ponce, B.A.; McGwin, G.; Shah, A.; Naranje, S.M. Marijuana use and mortality following orthopedic surgical procedures. Subst. Abus. 2019, 40, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Rozinthe, A.; Ode, Q.; Subtil, F.; Fessy, M.-H.; Besse, J.-L. Impact of smoking cessation on healing after foot and ankle surgery. Orthop. Traumatol. Surg. Res. 2022, 108, 103338. [Google Scholar] [CrossRef]
- Møller, A.M.; Villebro, N.; Pedersen, T.; Tønnesen, H. Effect of preoperative smoking intervention on postoperative complications: A randomised clinical trial. Lancet 2002, 359, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Capece, G.; Di Gialleonardo, E.; Comisi, C.; Bocchino, G.; Cinelli, V.; Mascio, A.; Fulchignoni, C.; Greco, T.; Maccauro, G.; Perisano, C. Treatment Options of Prosthetic Joint Infections Following Total Ankle Arthroplasty: A Systematic Review. J. Clin. Med. 2025, 14, 718. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).