Abstract
Background: Castleman’s disease (CD), also known as angiofollicular lymph node hyperplasia, describes a rare group of diseases manifesting with enlarged lymph nodes and various inflammatory symptoms. The association between Castleman’s disease, paraneoplastic pemphigus and bronchiolitis obliterans has been described in the literature and is depicted thoroughly in this case. Case Presentation: We present a case of severe bronchiolitis obliterans developing in a 17-year-old female with paraneoplastic pemphigus and unicentric Castleman’s disease. Conclusion: Surgical resection of unicentric Castleman’s disease remains the treatment of choice due to its efficacy in preventing the recurrence of associated morbidity caused by bronchiolitis obliterans and paraneoplastic pemphigus.
1. Introduction
Castleman’s disease (CD), also known as angiofollicular lymph node hyperplasia, is a rare lymphoproliferative disorder that may present as unicentric (UCD) or multicentric (MCD), with distinct clinical and histopathological features [1,2,3]. While UCD is often cured with surgical excision, MCD is more heterogeneous and may be associated with viral infections, such as human herpesvirus-8 (HHV-8), and systemic inflammation [2,3]. Importantly, CD can be complicated by paraneoplastic pemphigus (PNP), a severe autoimmune blistering disease, and bronchiolitis obliterans (BO), a progressive and often treatment-refractory small-airway disorder [4,5,6,7].
Although several cases of CD associated with PNP and BO have been described, the mechanisms remain incompletely understood, and treatment outcomes are not well established [8,9,10].
Here, we report a rare case of a young patient with UCD complicated by PNP and severe BO, highlighting diagnostic challenges, management decisions, and long-term outcomes following surgical resection and lung transplantation.
2. Case Presentation
A 17-year-old female patient was referred to our hospital because of rapidly worsening shortness of breath and a reduction in forced expiratory volume in 1 s (FEV1) down to 18% in an ambulatory performed lung-function test.
The patient had been living in Egypt her entire life and had only recently moved to Germany with her family. One year prior to the development of breathing difficulties, she had started experiencing oral blisters and mucosal ulcerations for the first time. At that time, her general condition was unremarkable.
A diagnosis of oral mucous membrane pemphigoid was made based on clinical signs with isolated erosive gingivitis and ulcerations of the tongue (Figure 1), with histology showing subepidermal split formation with detached basal keratinocytes and indirect immunofluorescence on salt-split skin demonstrating IgG deposition at the epidermal side of the blister. Direct immunofluorescence from the buccal mucosa, indirect immunofluorescence on monkey esophagus, and serology for circulating autoantibodies against various basement membrane proteins (BP180, BP230, collagen type VII, LAD-1, and laminin 332) remained negative at that time.

Figure 1.
(a) Erythematous and erosive gingivitis of the lower anterior gingiva, with diffuse mucosal inflammation and desquamation. The gingival margin exhibits marked erythema with early epithelial sloughing, typical of mucosal involvement in PNP. (b) Extensive erosive and ulcerative lesions of the dorsal tongue, with a broad area of denuded epithelium and pseudomembrane formation. The surrounding mucosa appears erythematous and edematous, consistent with the severe mucositis observed in autoimmune blistering diseases. Images reproduced from Bender et al. [11], under the terms of the Creative Commons Attribution 4.0 International License.
A treatment with prednisolone (initially 75 mg/d) and dapsone was initiated, leading to significant improvement in oral lesions, followed by tapering of systemic steroids. However, several months later, the patient began experiencing shortness of breath upon exertion and was not able to participate in sportive activities with her peers. She was seen by a pulmonologist, who, in turn, after documenting a reduction in FEV1-value and hypoxemia, prescribed the patient long-term oxygen therapy and referred her to our hospital. At that time, she was on an immunosuppressive therapy with 15 mg of prednisolone daily. Dapsone had been withdrawn 3 months prior to presentation when breathing difficulties had started.
Upon presentation at our department, the patient was in no respiratory distress but did require oxygen supplementation via a nasal cannula due to mild respiratory insufficiency. Lung-function tests revealed her FEV1 to have further diminished to 10% as well as showing evidence of advanced small-airway disease. A high-resolution CT scan (HRCT) of the chest showed a mosaic attenuation pattern at end-expiration (Figure 2). In light of the patient’s respiratory condition, a transbronchial biopsy was considered a high-risk procedure and was therefore omitted.
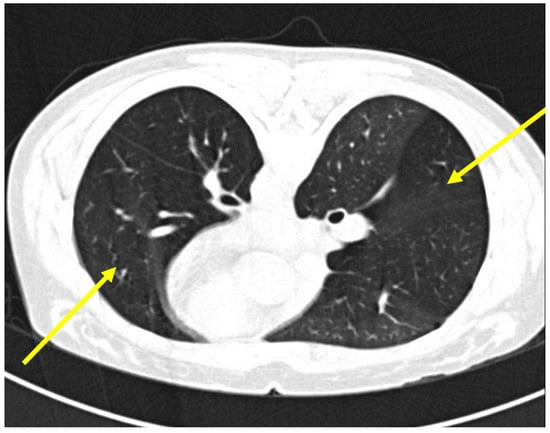
Figure 2.
High-resolution computed tomography (HRCT) scan of the chest demonstrating features of bronchiolitis obliterans. Mosaic attenuation pattern, characterized by areas of differing lung density. This is most prominently seen in the right lower and left upper lobes (indicated by yellow arrows), where geographic areas of hypoattenuation suggest air trapping due to small airway obstruction.
Following an interdisciplinary case discussion, a preliminary diagnosis of bronchiolitis obliterans was made. Due to the known association of bronchiolitis obliterans with paraneoplastic pemphigus, further examination of the previously obtained serum samples and of a fresh serum sample were performed in a specialized laboratory. In both samples, IgG to recombinant envoplakin was detected by enzyme-linked immunosorbent assay (ELISA) in addition to epithelium-binding immunoglobulin G antibodies in indirect immunofluorescence (IIF) on rat bladder, confirming the diagnosis of paraneoplastic pemphigus.
Envoplakin immunoglobulin G (IgG) antibodies were detected using a commercially available ELISA kit (Euroimmun, Lübeck, Germany). Notably, seropositivity was confirmed at the time of diagnostic reassessment and coincided with the onset of pulmonary manifestations rather than preceding them.
A PET-CT scan showed increased uptake in the right lower quadrant of the abdomen, highly suspicious for an extraluminal mass (Figure 3). During work-up, the patient developed severe respiratory distress, which, despite high-dose steroid administration and supportive therapy, led to endotracheal intubation and to placement on mechanical ventilation. Given the development of severe respiratory failure prior to abdominal surgery and before a donor lung became available, veno-venous extracorporeal membrane oxygenation (VV-ECMO) was initiated as a bridging strategy. This measure provided stabilization and adequate oxygenation, allowing the patient to survive until definitive surgical resection and subsequent transplantation could be carried out. Simultaneously, the patient was evaluated for lung transplantation.
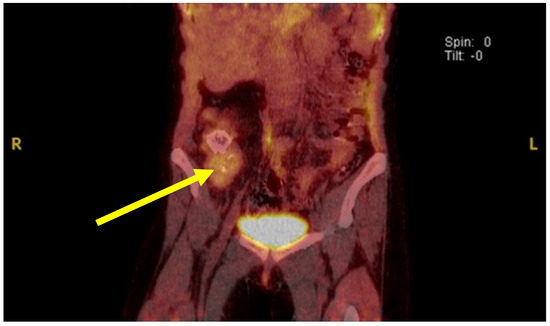
Figure 3.
PET-CT scan of the abdomen showing focal hypermetabolic activity. Coronal fused PET-CT image reveals a localized area of increased fluorodeoxyglucose (FDG) uptake in the right lower quadrant of the abdomen (indicated by the yellow arrow). The hypermetabolic focus is suggestive of an active lymphoproliferative lesion, potentially corresponding to the intra-abdominal mass later confirmed as unicentric Castleman’s disease. Image reproduced from Bender et al. [11], under the terms of the Creative Commons Attribution 4.0 International License.
Surgical excision of the intra-abdominal mass was performed under ECMO. Macroscopy of the resection specimen showed a heavily calcified mass. On a microscopic level, there was a tumor-forming lymphoid lesion with dense sclerotic zones and ossification. Blood vessels with hyalinization were seen, occasionally with lollipop-like concentric arrangements of lymphocytes (Figure 4). There were no residual lymph node structures detectable in the specimen. The initial pathologic assessment considered the findings consistent with the hyaline vascular variant of Castleman’s disease. Tumor samples were subsequently sent to a German reference center for lymph node diagnostics. The microscopic findings were described as Castleman-like hamartomatous lesion. However, due to the notion of a pre-existing lymph node, these findings were compatible with the hyaline vascular variant of Castleman’s disease. The serology for HHV-8 infection was negative.
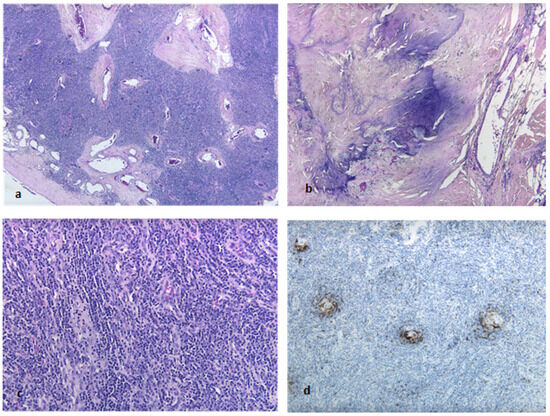
Figure 4.
Resection specimen showing a lymphoid lesion with sclerotic areas consistent with a Castleman-like hamartomatous reactive lymphoproliferation. (a) H&E, low-power: perivascular sclerosis. (b) H&E, intermediate-power: dense sclerosis with focal calcification. (c) H&E, high-power: abundance of high endothelial venules. CD23 immunohistochemistry, intermediate-power: follicular dendritic cells in concentric arrangement around blood vessels (d). (magnification 200:1).
In the absence of contraindications and since the patient had a high lung allocation score (LAS), a bilateral sequential lung transplantation was performed. Prior to lung transplantation, the patient received tocilizumab, an IL-6 receptor monoclonal antibody, with the rationale of significantly reducing dominant HLA antibodies in order to prevent antibody-mediated rejection, consistent with evidence supporting IL-6 blockade in this setting [12]. The specimens of the explanted lungs revealed bronchiolitis obliterans characterized by fibrous obliteration of small bronchioles, associated peribronchiolar lymphocytic inflammation and occasionally a residual aspergilloma (Figure 5). These features confirmed the diagnoses of bronchiolitis obliterans.
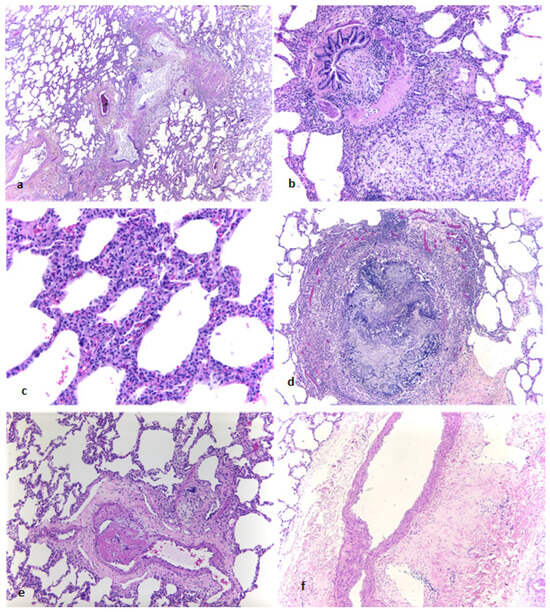
Figure 5.
Explanted lung showing bronchiolitis obliterans and associated findings. (a) H&E, low-power: bronchiolar lumina obliterated by fibrous tissue with adjacent foamy macrophages and hyalinization. (b) H&E, intermediate-power: aggregates of foamy macrophages in peribronchiolar tissue. (c) H&E, high-power: increased interstitial inflammatory infiltrates consistent with interstitial pneumonia. (d) H&E, intermediate-power: residual aspergilloma following antifungal (antimycotic) therapy. (e) H&E, intermediate-power: occasional microthrombi in small pulmonary vessels. (f) H&E, intermediate-power: perivascular hyalinization in larger vessels. (magnification 200:1).
The postoperative course was complicated by significant intra-abdominal bleeding within the first 24 h, requiring reoperation and transfusion. Peritonitis developed on day 10 and was managed with surgical revision and broad-spectrum antibiotics, with gradual resolution. After lung transplantation, acute renal failure occurred in the second postoperative week, necessitating temporary renal replacement therapy. The patient remained in the ICU for approximately 6 weeks, with progressive stabilization under multidisciplinary management, and was eventually weaned from intensive support.
The patient has shown great recovery and is currently at over 2 years after lung transplantation, undergoing routine surveillance with no signs of acute rejection and a FEV1-value of 82%. She does not require oxygen supplementation. In addition, she did not develop any new mucocutaneous erosions under immunosuppression with tacrolimus, mycophenolate mofetil and prednisolone to prevent graft rejection.
A timeline of the clinical milestones, including symptom onset, therapeutic interventions and major procedures, is shown in Figure 6.
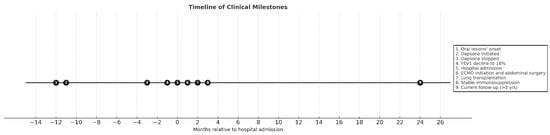
Figure 6.
Timeline of clinical milestones.
Published experiences with transplantation in CD-associated bronchiolitis obliterans are summarized in Table 1.

Table 1.
Published cases/series of lung transplantation in Castleman’s disease complicated by paraneoplastic pemphigus (PNP) and bronchiolitis obliterans (BO): patient age, CD subtype, interval from diagnosis to lung transplantation (LT), ECMO use, and outcomes. Cases include early pediatric experience and contemporary adult reports/series. NR = not reported.
3. Discussion
Castleman disease (CD) is a rare, heterogeneous group of lymphoproliferative disorders defined by distinctive lymph node histopathology. Clinically, CD presents either as involvement limited to a single nodal basin—unicentric CD (UCD)—or as a systemic process with generalized lymphadenopathy and inflammatory manifestations—multicentric CD (MCD). MCD comprises several etiologic subtypes, including HHV-8-associated disease, POEMS-related disease, and HHV-8-negative/idiopathic MCD (iMCD) [1,2,3].
In UCD, nodal architecture spans a spectrum from classic hyaline-vascular (HV) changes to plasmacytic features, with mixed forms showing elements of both. HV-type histology predominates in UCD and is typically not accompanied by constitutional symptoms or pronounced cytokine excess [15,16].
Bronchiolitis obliterans (BO) and paraneoplastic pemphigus (PNP) are rare and ominous complications of CD.
Paraneoplastic pemphigus (PNP) is a severe autoimmune mucocutaneous blistering disorder characterized by painful oral erosions and polymorphic skin lesions. Diagnosis is based on clinical presentation, histology, and the detection of autoantibodies (such as envoplakin and periplakin) through immunofluorescence and ELISA. Treatment includes immunosuppression with corticosteroids and steroid-sparing agents, but long-term control remains difficult. Differential diagnoses include pemphigus vulgaris, bullous pemphigoid and mucous membrane pemphigoid, which can be excluded by immunopathological testing [17].
Bronchiolitis obliterans (BO) manifests as progressive dyspnea and airflow limitation, with diagnosis established by pulmonary function testing mainly by observing severe obstruction and decrease in FEV1, high-resolution CT imaging demonstrating air trapping in end-expiration, and, when feasible, histology. BO is largely refractory to immunosuppression, and while tumor resection may prevent further autoimmune stimulation, respiratory decline often progresses. Differential diagnoses include infectious and autoimmune-related bronchiolitis and interstitial lung diseases, which must be ruled out by clinical and radiological evaluation.
Infectious bronchiolitis was excluded on the basis of negative microbiological cultures and the absence of radiological findings suggestive of acute infection. An immunotherapy-related etiology was considered unlikely, as the patient had not been exposed to immune checkpoint inhibitors or other targeted immunotherapies before the onset of bronchiolitis obliterans.
Taken together, these manifestations are encompassed by paraneoplastic autoimmune multiorgan syndrome (PAMS) and have been described in association with a range of tumors, including hematologic malignancies, carcinoid tumors and melanoma [18].
Bronchiolitis obliterans (BO) is a recognized, severe pulmonary complication that develops in roughly one-third of patients with CD-associated PNP—even after surgical excision of the mass—and is thought to arise from cross-reactive autoantibodies directed against desmoplakin and antigens within the respiratory epithelium [6,19]. BO is associated with the poorest outcomes in PNP, and, in advanced cases, lung transplantation often becomes the only remaining option [6,8,9,10].
4. Materials and Methods
Materials for this case report were obtained from the corresponding authors as well as open sources online and scientific work relevant to the case on hand. When the work is referenced, the author does not have any restrictions on the availability of the material or information presented in this case report.
5. Conclusions
CD includes a group of rare and heterogeneous disorders with characteristic lymph node abnormalities. It may be associated with the development and progress of BO and PNP.
The treatment of choice for patients with advanced BO and CD remains surgical, including the resection of the culprit lesion followed by lung transplantation. A recurrence of the disease or its pulmonary manifestation has not been reported in the literature and was not observed in our patient [15,16,18].
Author Contributions
W.K. contributed to patient care, contacting all involved physicians, gathering relevant information and images, and putting the report together. V.B., S.W., A.D. and S.C.H. were directly involved in patient care. S.C.H. provided substantial contributions to the proofreading and critical revision of the manuscript, with a particular focus on dermatology-specific content. D.T. and S.B. were the involved pathologists in the case, with E.S. contributing to the revised initial pathology report aiding in the diagnosis of paraneoplastic pemphigus. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was waived due to the retrospective and non-interventional nature of the study, which utilized anonymized clinical data. This exemption is consistent with German regulatory guidance and the “One Study–One Vote” procedure endorsed by the German Medical Association and AKEK (https://rwr-regs.com/germany-nis-considerations/ accessed on 29 September 2024).
Informed Consent Statement
Informed consent was obtained from the patient involved in the case report.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| BO | Bronchiolitis Obliterans |
| CD | Castleman’s Disease |
| CT | Computed Tomography |
| ECMO | Extracorporeal Membrane Oxygenation |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| FDG | Fluorodeoxyglucose |
| FEV1 | Forced Expiratory Volume in 1 Second |
| HHV-8 | Human Herpesvirus-8 |
| HRCT | High-Resolution Computed Tomography |
| IIF | Indirect Immunofluorescence |
| IgG | Immunoglobulin G |
| LAS | Lung Allocation Score |
| LT | Lung Transplantation |
| MCD | Multicentric Castleman’s Disease |
| PET-CT | Positron Emission Tomography–Computed Tomography |
| PNP | Paraneoplastic Pemphigus |
| PAMS | Paraneoplastic Autoimmune Multiorgan Syndrome |
| UCD | Unicentric Castleman’s Disease |
| VV-ECMO | Veno-Venous Extracorporeal Membrane Oxygenation |
References
- Cronin, D.M.; Warnke, R.A. Castleman disease: An update on classification and the spectrum of associated lesions. Adv. Anat. Pathol. 2009, 16, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Tu, M.; Cortes, J.; Xu-Monette, Z.Y.; Miranda, R.N.; Zhang, J.; Oelowski, R.Z.; Neelapu, S.; Boddu, P.C.; Akosile, M.A.; et al. Clinical and pathological characteristics of HIV- and HHV-8-negative Castleman disease. Blood 2017, 129, 1658–1668. [Google Scholar] [CrossRef] [PubMed]
- van Rhee, F.; Oksenhendler, E.; Srkalovic, G.; Voorhees, P.; Lim, M.; Dispenzieri, A.; Ide, M.; Parennte, S.; Schey, S.; Streetly, M.; et al. International evidence-based consensus diagnostic and treatment guidelines for unicentric Castleman disease. Blood Adv. 2020, 4, 6039–6050. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Shimatsu, Y.; Kazama, T.; Kimura, K.; Otsuka, T.; Hashimoto, T. Paraneoplastic pemphigus associated with bronchiolitis obliterans. Chest 2000, 117, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Morita, M.; Enomoto, K. Bronchiolitis obliterans with pemphigus vulgaris and Castleman’s disease of hyaline-vascular type: An autopsy case analyzed by computer-aided 3-D reconstruction of the airway lesions. Hum. Pathol. 1997, 28, 1310–1312. [Google Scholar] [CrossRef] [PubMed]
- Nousari, H.C.; Deterding, R.; Wojtczak, H.; Aho, S.; Uitto, J.; Hashimoto, T.; Anhalt, G.J. The mechanism of respiratory failure in paraneoplastic pemphigus. N. Engl. J. Med. 1999, 340, 1406–1410. [Google Scholar] [CrossRef] [PubMed]
- Raza, H.A. Unicentric Castleman disease complicated by paraneoplastic bronchiolitis obliterans and pemphigus. Respir. Med. Case Rep. 2018, 25, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Chin, A.C.; Stich, D.; White, F.V.; Radhakrishnan, J.; Holterman, M.J. Paraneoplastic pemphigus and bronchiolitis obliterans associated with a mediastinal mass: A rare case of Castleman’s disease with respiratory failure requiring lung transplantation. J. Pediatr. Surg. 2001, 36, E22. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhao, L.; Guo, L.; Zhao, L.; Niu, H.; Lian, H.; Dai, H.; Chen, J.; Wang, C. Clinical and pathological features of bronchiolitis obliterans requiring lung transplantation in paraneoplastic pemphigus associated with Castleman disease. Clin. Respir. J. 2022, 16, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Yue, B.; Huang, J.; Jing, L.; Yu, H.; Wei, D.; Zhang, J.; Chen, W.; Chen, J. Bilateral lung transplantation for Castleman disease with end-stage bronchiolitis obliterans. Clin. Transpl. 2022, 36, e14496. [Google Scholar] [CrossRef] [PubMed]
- Bender, S.T.; Balakirski, G.; Kteiche, W.; Schmidt, E.; Hofmann, S.C. Morbus Castleman-assoziierter paraneoplastischer Pemphigus bei einer 16-jährigen Patientin. Dermatologie. 2024, 75, 641–646. [Google Scholar] [CrossRef] [PubMed]
- January, S.E.; Fester, K.A.; Halverson, L.P.; Witt, C.A.; Byers, D.E.; Vazquez-Guillamet, R.; Alexander-Brett, J.; Tague, L.K.; Kreisel, D.; Gelman, A.; et al. Tocilizumab for antibody-mediated rejection treatment in lung transplantation. J. Heart Lung Transpl. 2023, 42, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Hommelgaard, L.; Perch, M.; Bendstrup, E. Lung Transplantation in a Patient with Severe Bronchiolitis Obliterans Secondary to Castleman Disease. Respir. Med. Case Rep. 2025, 57, 102266. [Google Scholar] [CrossRef] [PubMed]
- Al-Bayati, S.; Villamizar, J.P.; Machuca, T.; Buitrago, D.; Pipkin, M.; Manickavel, S.; Sinha, N.; Pelaez, A.; Salgado, J.; Fernandez, J. ECMO Bridge to Bilateral Lung Transplant for Castleman Disease. J. Heart Lung Transplant. 2024, 43, S479. [Google Scholar] [CrossRef]
- Keller, A.R.; Hochholzer, L.; Castleman, B. Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer 1972, 29, 670–683. [Google Scholar] [CrossRef] [PubMed]
- Herrada, J.; Cabanillas, F.; Rice, L.; Manning, J.; Pugh, W. The clinical behavior of localized and multicentric Castleman disease. Ann. Intern. Med. 1998, 128, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.C.; Juratli, H.A.; Eming, R. Bullous autoimmune dermatoses. J. Dtsch. Dermatol. Ges. 2018, 16, 1339–1358. [Google Scholar] [CrossRef] [PubMed]
- Didona, D.; Dizenzo, G.; Joly, P. Paraneoplastic autoimmune multiorgan syndrome. Ital. J. Dermatol. Venerol. 2020, 156, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Maruta, C.W.; Miyamoto, D.; Aoki, V.; Carvalho, R.G.R.; Cunha, B.M.; Santi, C.G. Paraneoplastic pemphigus: A clinical, laboratorial, and therapeutic overview. An. Bras. Dermatol. 2019, 94, 388–398. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).