
Virtual Choirs in Care Homes: The Development and Early Assessment of a New Virtual Reality Choir Intervention
 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials
2.1. Co-Design and Specification
2.1.1. Technical Specification
- Ideally hardware-agnostic (compatible with various devices) for future scalability
- -
- PICO 4 headsets were used in this study, as the focus groups deemed them more comfortable than the Meta Quest 2, which was the alternative model available during development
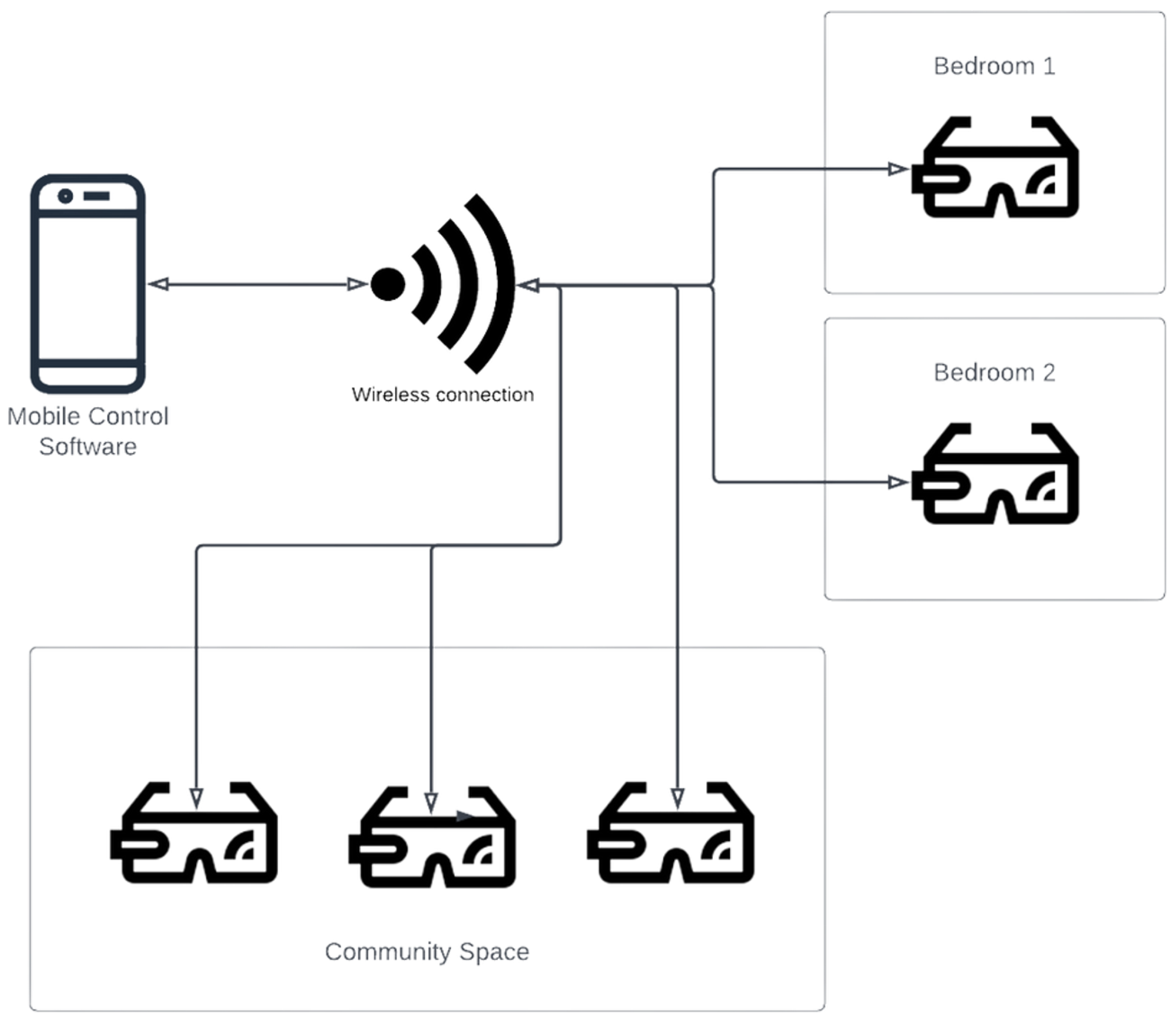
- System must run on local Wi-Fi connections and connect automatically to avoid reliance on varying internet connections that might impact the VR experience.
- Loading screens and ‘lobby area’ not confusing or disorientating
- Ease of use (easy both for care home staff to run the experience and for residents to engage with it)
- -
- The person experiencing VR only needs to put the headset on and look around
- -
- Remotely controlled by a tablet/phone (also very simple for care home staff to use so they can control what happens in VR). This includes connecting the headsets to the application (which occurs automatically upon connection with the app) and then choosing songs based on easily viewed icons and titles.
- -
- Minimal initial set-up (no expertise required and quick to set up)
- Minimise the potential hazards of using VR through experience design
- -
- A seated experience with 3 degrees of freedom, whereby the user has a 360 degree experience as they rotate their head but the VR environment is static from that position, so there is no need for the user to stand or move as they cannot move through the virtual environment.
- -
- A safety announcement in VR to remind the user they are in VR and can remove the headset anytime
- -
- Guidance reminding users not to use the VR headset for longer than 15 min in any session
2.1.2. Choir Video Content
- All recordings should take place in visually interesting surroundings—ideally outside.
- The group should be directed and taught the songs by rote as part of the recording.
- The songs should be easy to sing.
- -
- The recordings should be made up of well-known songs and melodies.
- -
- The songs should be within a standard vocal range (not extreme tessituras).
- -
- Only simple harmonies should be involved (those that enrich the experience but do not necessarily need to be sung).
- The experience should involve musical material that is likely to be known to the users but is outside of copyright.
- A warm-up video of a few minutes should be included and led by the choir director (while remaining seated).
- The director and choir should engage with the video camera so the person in VR feels included.
2.1.3. Alpha Version and Testing
2.1.4. Beta Version and Testing
- A mobile app controller.
- A very simple user interface.
- Automatic connection to a local IP address.
- A new virtual environment for the lobby area (the virtual lobby that people experienced while the app was loading).
- A bank of nine song recordings was included.
- -
- Warm Up.
- -
- Fellowship Song.
- -
- Light of Mine.
- -
- Loch Lomond.
- -
- Original Song.
- -
- Peace Song.
- -
- Danny Boy.
- -
- White Cliffs of Dover.
- A warm-up video.
3. Feasibility Studies: Methods
- Ad hoc engagement: Understand the practicalities of utilising the technology within the daily running of residential care homes.
- Pre-feasibility study: Develop and test a feasible protocol to assess the efficacy and wellbeing benefits of the intervention.
3.1. Ethical Approval
3.2. Participants
3.3. Ad Hoc Engagement: Method
Ad Hoc Engagement: Intervention Delivery
3.4. Pre-Feasibility: Method
3.4.1. Pre-Feasibility: Intervention Delivery
3.4.2. Pre-Feasibility: Data Collection
- UWIST [27]: This is a list of 24 adjectives to be ticked against a scale of affinity with that item. This was chosen due to its previously reported use in VR studies involving elderly populations [28]. However, this was only completed by three participants in session one in Care Home 1 and was found to be too complex for residents. Therefore, no results are reported here.
- Circumplex model of affect [29]: Participants were asked to place a mark on a mood wheel (reflecting the circumplex model) that best represented how they felt in that moment. This tool was adopted from Day 1 in Care Home 2 after the UWIST tool was found to be unsuitable, to see whether a single-item visual scale would be less onerous.
- Gender-adjusted Self Assessment Manikin [30]: This tool is commonly associated with research in a VR context and was added to the protocol on Day 8 to assess its usefulness as a simple visual scale compared to the mood wheel.
- Health-related quality of life (HRQoL): HRQoL was measured using the EuroQol 5 Dimensions (EQ-5D-5L (Rabin et al, 2001). This profiles health-related quality of life (HRQoL) on the dimensions of mobility, self-care, usual activities, pain/discomfort and anxiety/depression based on five levels of severity (no problems = 1; extreme problems = 5). A UK national population tariff was applied to create a summary score value for each health state described. For the UK, as recommended by NICE (NICE PMG36, 2023), the crosswalk range of scores is −0.532 to 0.987 [37] with 1 representing full health and 0 representing death, while negative values relate to states worse than death. Additionally, a visual analogue score was completed by each participant, indicating their individual evaluation of their own health state (range 0 to 100 with 0 representing death and 100 full health).
- ICEpop CAPability measure for Older People (ICECAP-O): The ICEpop CAPability measure for Older People (ICECAP-O) assesses five capabilities that are important to one’s wellbeing, comprising attachment, security, role, enjoyment, and control [38]. The instrument can be used as an important addition to generic health questionnaires when evaluating quality of life extending beyond health; for example, in settings such as care homes. NICE explicitly refers to the use of ICECAP-O in its guidance [33,39] for the economic evaluation of interventions funded by the public sector with a social care focus. ICECAP-O uses a UK general population tariff based on best–worst scaling with 0 indicating no capability and 1 representing full capability, to enable its use in economic evaluation both within the field of health and across public policy generally [34].
- SWEMWBS: The Short Warwick–Edinburgh Mental Wellbeing Scale enables the monitoring of mental wellbeing in the general population [35]. The 7-item SWEMWBS is useful to save space and time in evaluations. The instrument asks for responses to the following 7 statements;
- I’ve been feeling optimistic about the future.
- I’ve been feeling useful.
- I’ve been feeling relaxed.
- I’ve been dealing with problems well.
- I’ve been thinking clearly.
- I’ve been feeling close to other people.
- I’ve been able to take up my own mind about things.
The participant gives each statement a score from 1 to 5, which encompasses things that they experience none of the time (1) to all of the time (5), using a Likert Scale; thus, higher raw scores indicate that the individual is experiencing better mental wellbeing.
3.5. Debrief Interviews
4. Results
4.1. Pre-Feasibility Study: Results
4.1.1. Baseline Characteristics
4.1.2. Engagement with the Intervention
4.1.3. Acute Measures of Mood
4.1.4. Loneliness Measures
4.1.5. Health-Related Quality of Life (EQ-5D-5L)
4.1.6. ICECAP-O
4.1.7. SWEMWEBS
4.1.8. Researchers’ Observations
‘All residents except 2 sang along, the 2 were seen to be tapping their feet and looking around the environment in the headset’.
‘Overall, the session went very smoothly and the residents seemed to enjoy the experience and are looking forward to next week’s session’.
‘[all participants] sang along, [2 participants] replicated hand movements of Sing from your seat song, [two others] both tapped their feet’.
‘The other three participants stayed in for all 9 tracks and we also played half of ‘Light of Mine’ and all of ‘Loch Lomond’ again for them, I think they would have happily stayed in longer’.
‘We asked several times throughout if anyone had had enough and only [one participant] said yes’.
‘[Three participants] all sang along with most of the music. [One participant] told me afterwards that she enjoyed it but she found some of the higher notes difficult, asked if anything could be done about that’.
‘[One participant] enjoyed the application very much, singing along to most songs, and would only stop using the application if it saved us time. Went through all songs. Also commented that she liked the headset and idea of VR in general’.
‘I asked [one participant] if she enjoyed the experience as she never sings, though one of the care staff commented that she had joined in a little in the warm-up’.
‘[Participant] said she does enjoy it. I asked “do you enjoy just listening to it?” and she said yes’.
‘First session had a resident who was…“not a singer”, but they were singing along throughout all songs’.
‘One participant was adamant, again, that she wouldn’t sing. In this intervention, she was seated next to another participant who was actively singing, instead of across the room from them as with last week. Saw her mouthing along to lyrics this time around’.
‘[One participant] didn’t sing at all, had her arms crossed throughout, but she did start tapping her foot to the beat after a while and stayed in the whole time’.
‘Participants gossiping with us about other participants from the previous weeks’.
‘[Participant] was very chatty today, she called me over to gossip at the beginning (she was in the room when we arrived because her room had maintenance going on). She said it was very interesting to have learnt a lot about [another participant] the previous week because “she never talks to anyone here”. We had a bit of a chat about [participant]’s life, she was a librarian and worked in book shops’.
‘[Participant] was very excited to go in again and convinced [another participant] to join after he said no then [that participant] sang along during loch lomond!’
‘Said it didn’t make her feel angry like last week because she knew what to expect. [participant A] was very pleased to see that [participant B] was enjoying it. [Participant B] sang along to the ones she knew. Didn’t sing to fellowship song or peace song but did applaud at end. Hummed along with Original Song, didn’t sing many words. [Participant B] said she really enjoyed it. At one point when we asked if she had had enough she said “no, this is fun!”
Both [participants A and B] gestured to the choir (ie waving during warm up).
Participant B started singing during the warmup and continued throughout the session.
Participant A was not singing but tapped her feet to the beat (specifically during loch lomond).
Participant B’s singing stopped when she didn’t know lyrics → later on she would hum, vocalise, or use ‘la’ to the melody.
Participant A stopped participating after loch lomond → said she got bored but was happy Participant B was enjoying herself.
Participant B really liked it and got into it!
Participant B wanted to keep singing but didn’t want to ‘burden’ us (kept saying things along the lines of “I don’t want to put you through it/take too much of your time/etc” when asked if she wanted to continue → we were able to reassure her that she could do as many songs as she wanted and she ended up doing all of them.
Participant B specifically asked for a cheery song at one point so we played fellowship song.
Participant B clapped after songs and followed the hand gestures/dances the choir was doing.
Participants A and B seem to have a stronger relationship each week they are in the experience together, noticeably chatting before and after more so than in initial weeks.
Participant A spent her longest time in the experience, still not fully enjoying it but seeming to stay in longer due to participant B enjoying it.
[Participant A] sang! She began singing in Danny Boy, saying “I’ll give singing a go, as this ones a bit lower.” She had commented before we began that she has a very low voice, like a Tenor.
Participant B sang during Danny Boy, Light of Mine, Loch Lomond, White Cliffs. She left after White Cliffs.
Participant B was looking around behind her in Light of Mine’.
‘[Participant] came in with a bit of a shaky leg which stopped once she was in the VR (would occasionally tap/shake but not to the same extent)’.
‘was asking the people in VR if they had a “spare book” and gesturing to them, because she didn’t know the words to the verses of ‘Light of Mine’’
‘One participant left about halfway through, she said the headset was making her nose hurt.’
‘[One participant] seemed to enjoy the VR but it wasn’t his type of music. He told me he likes acoustic guitar music. He wasn’t as engaged with the singing, but he was looking around a lot in VR.’
4.2. Ad Hoc Engagement: Results
- Started singing along.
- Was moving along to the music.
- Didn’t want to stop!
‘Ok… still looking for Rock Music but said he really enjoyed it’.
‘[participant] enjoyed 3 music songs and was very calm and relaxed after’.
‘Loved taking part. Very contented during the session. Looked relaxed and engaged. Feet tapping away. Said her neck was a bit sore’.
‘enjoyed the time. really good and had fun. Was singing along. Very happy session.’
‘Happy initially, however became emotional when she listened to some of her husbands favourite songs’.
‘LOVED IT: very used to VR headset as he is a big gamer/ Wants more modern music.’
‘Love it. Coped well with Headset and music. So engaged. Great session.’
‘Loved the music - Loved Singing along. Did state the headset feels a bit too heavy: would try it again!’
‘Good enjoyed singing along. Happy to stay for the session.’
‘Enjoyed it very much. Would have stayed longer—but her head was feeling heavy!’
‘Enjoyed 3 music songs and was very calm and relaxed after’.
- Found the headset uncomfortable.
- The headset was too heavy.
- Wanted more music/a different choice of music.
- Wanted the words on the screen.
4.2.1. Cost of the Intervention
4.2.2. Agency
4.3. Ease of Use
4.4. Limitations
5. Discussion
5.1. Limitations
5.1.1. Application Design
5.1.2. Pre-Feasibility Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gardiner, C.; Laud, P.; Heaton, T.; Gott, M. What is the prevalence of loneliness amongst older people living in residential and nursing care homes? A systematic review and meta-analysis. Age Ageing 2020, 49, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Franck, L.; Molyneux, N.; Parkinson, L. Systematic review of interventions addressing social isolation and depression in aged care clients. Qual. Life Res. 2016, 25, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Sedlackova, K.B.; Bartova, A.; Holmerova, I. Feeling Lonely, Isolated and Depressed. Older Adults’ Feelings in Long-term Term Facilities: A Scoping Review. J. Popul. Ageing 2024, 17, 861–914. [Google Scholar] [CrossRef]
- Waters, B.; Sousa, L.; Orrell, M.; McDermott, O. Analysing the use of music to facilitate social interaction in care home residents with dementia: Narrative synthesis systematic review. Dementia 2022, 21, 2072–2094. [Google Scholar] [CrossRef]
- Amano, T.; Hooley, C.; Strong, J.; Inoue, M. Strategies for implementing music-based interventions for people with dementia in long-term care facilities: A systematic review. Int. J. Geriatr. Psychiatry 2022, 37, gps.5641. [Google Scholar] [CrossRef]
- Garabedian, C.E. ‘I’D RATHER HAVE MUSIC!’: The Effects of Live and Recorded Music for People with Dementia Living in Care Homes, and Their Carers. Ph.D. Thesis, University of Stirling, Stirling, UK, 2014. [Google Scholar]
- Agres, K.R.; Schaefer, R.S.; Volk, A.; Van Hooren, S.; Holzapfel, A.; Dalla Bella, S.; Müller, M.; De Witte, M.; Herremans, D.; Ramirez Melendez, R.; et al. Music, Computing, and Health: A Roadmap for the Current and Future Roles of Music Technology for Health Care and Well-Being. Music Sci. 2021, 4, 2059204321997709. [Google Scholar] [CrossRef]
- Kuot, A.; Barton, E.; Tiri, G.; McKinlay, T.; Greenhill, J.; Isaac, V. Personalised music for residents with dementia in an Australian rural aged-care setting. Aust. J. Rural. Health 2021, 29, 71–77. [Google Scholar] [CrossRef]
- Taylor, J.R.; Milne, A.J.; Macritchie, J. New musical interfaces for older adults in residential care: Assessing a user-centred design approach. Disabil. Rehabil. Assist. Technol. 2023, 18, 519–531. [Google Scholar] [CrossRef]
- MacRitchie, J.; Floridou, G.A.; Christensen, J.; Timmers, R.; De Witte, L. The use of technology for arts-based activities in older adults living with mild cognitive impairment or dementia: A scoping review. Dementia 2023, 22, 252–280. [Google Scholar] [CrossRef]
- Lee, S.; O’Neill, D.; Moss, H. Dementia-inclusive group-singing online during COVID-19: A qualitative exploration. Nord. J. Music. Ther. 2022, 31, 308–326. [Google Scholar] [CrossRef]
- Ofosu, E.; De Nys, L.; Connelly, J.; Ryde, G.; Whittaker, A. A realist evaluation of the feasibility of a randomised controlled trial of a digital music and movement intervention for older people living in care homes. BMC Geriatr. 2023, 23, 125. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wilke, C.; Shiyanov, I.; Muschalla, B. Impact of Virtual Reality-Based Group Activities on Activity Level and Well-Being Among Older Adults in Nursing Homes: Longitudinal Exploratory Study. JMIR Serious Games 2024, 12, e50796. [Google Scholar] [CrossRef] [PubMed]
- Perez, P.; Vallejo, E.; Revuelta, M.; Redondo Vega, M.V.; Guervós Sánchez, E.; Ruiz, J. Immersive Music Therapy for Elderly Patients. In Proceedings of the ACM International Conference on Interactive Media Experiences, Aveiro, Portugal, 22–24 June 2022; pp. 47–52. [Google Scholar] [CrossRef]
- Lee, L.N.; Kim, M.J.; Hwang, W.J. Potential of Augmented Reality and Virtual Reality Technologies to Promote Wellbeing in Older Adults. Appl. Sci. 2019, 9, 3556. [Google Scholar] [CrossRef]
- Leiper, T. A Study of the Impact on Health and Wellbeing of Amateur Choir Singers as Face-to-Face Group Singing Moved Online. Voice Speech Rev. 2023, 17, 48–65. [Google Scholar] [CrossRef]
- Tamplin, J.; Thompson, Z. How health-focused choirs adapted to the virtual world during the COVID-19 pandemic—An international survey. Arts Psychother. 2023, 82, 101997. [Google Scholar] [CrossRef]
- Tamplin, J.; Haines, S.J.; Baker, F.A.; Sousa, T.V.; Thompson, Z.; Crouch, H.; Dunn, S.; Tull, V.; Vogel, A.P.; Morris, M.E. ParkinSong Online: Feasibility of Telehealth Delivery and Remote Data Collection for a Therapeutic Group Singing Study in Parkinson’s. Neurorehabilit. Neural Repair 2024, 38, 122–133. [Google Scholar] [CrossRef]
- MacDonald, R.; Zumbansen, A. Successful Online Choir for People Living with Dementia: A Qualitative Case Study. OBM Integr. Complement. Med. 2023, 8, 1–20. [Google Scholar] [CrossRef]
- Paparo, S.A. Real Voices, Virtual Ensemble 2.0: Perceptions of Participation in Eric Whitacre’s Virtual Choirs. Int. J. Res. Choral Sing. 2021, 9, 92–115. [Google Scholar]
- Paparo, S.A. Real Voices, Virtual Ensemble: The Meaning of Participation in Eric Whitacre’s Virtual Choirs. In Meanings of Music Participation; Routledge: London, UK, 2022; pp. 157–177. [Google Scholar]
- Tamplin, J.; Loveridge, B.; Clarke, K.; Li, Y.; J Berlowitz, D. Development and feasibility testing of an online virtual reality platform for delivering therapeutic group singing interventions for people living with spinal cord injury. J. Telemed. Telecare 2020, 26, 365–375. [Google Scholar] [CrossRef]
- Daffern, H.; Balmer, K.; Brereton, J. Singing together, yet apart: The experience of UK choir members and facilitators during the Covid-19 pandemic. Front. Psychol. 2021, 12, 624474. [Google Scholar] [CrossRef]
- Schneider, J.; Ablewhite, J.; Bloska, J.; Gold, C.; Orrell, M.; Dowson, B.; McArdle, C.; Tooth, H.; Trevers, S.; Narippatta, S.M. Music in Care Home Settings: Guidelines for Implementation and Evaluation Based on the Music Interventions for Depression and Dementia in ELderly Care (MIDDEL) Study in the UK. J. Long-Term Care 2024, 252–262. [Google Scholar] [CrossRef]
- Rees-Jones, J.; Daffern, H. The hills are alive: Capturing and presenting an outdoor choral performance for virtual reality. In Proceedings of the Audio Engineering Society Conference: 2019 AES International Conference on Immersive and Interactive Audio, York, UK, 27–29 March 2019. [Google Scholar]
- Pentikäinen, E.; Kimppa, L.; Pitkäniemi, A.; Lahti, O.; Särkämö, T. Longitudinal effects of choir singing on aging cognition and wellbeing: A two-year follow-up study. Front. Hum. Neurosci. 2023, 17, 1174574. [Google Scholar] [CrossRef] [PubMed]
- Craig, R.J. Assessing Personality and Mood With Adjective Check List Methodology: A Review. Int. J. Test. 2005, 5, 177–196. [Google Scholar] [CrossRef]
- Montana, J.I.; Matamala-Gomez, M.; Maisto, M.; Mavrodiev, P.A.; Cavalera, C.M.; Diana, B.; Mantovani, F.; Realdon, O. The benefits of emotion regulation interventions in virtual reality for the improvement of wellbeing in adults and older adults: A systematic review. J. Clin. Med. 2020, 9, 500. [Google Scholar] [CrossRef]
- Russell, J.A. A circumplex model of affect. J. Personal. Soc. Psychol. 1980, 39, 1161. [Google Scholar] [CrossRef]
- Sainz-de Baranda Andujar, C.; Gutiérrez-Martín, L.; Miranda-Calero, J.Á.; Blanco-Ruiz, M.; López-Ongil, C. Gender biases in the training methods of affective computing: Redesign and validation of the Self-Assessment Manikin in measuring emotions via audiovisual clips. Front. Psychol. 2022, 13, 955530. [Google Scholar] [CrossRef]
- Gosling, C.J.; Colle, R.; Cartigny, A.; Jollant, F.; Corruble, E.; Frajerman, A. Measuring loneliness: A head-to-head psychometric comparison of the 3-and 20-item UCLA Loneliness Scales. Psychol. Med. 2024, 54, 3821–3827. [Google Scholar] [CrossRef]
- Lok, I.; Dunn, E. The UBC State Social Connection Scale: Factor Structure, Reliability, and Validity. Soc. Psychol. Personal. Sci. 2023, 14, 835–844. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. NICE Health Technology Evaluations: The Manual; Process and Methods [PMG36]; NICE: London, UK, 2022. [Google Scholar]
- Flynn, T.N.; Huynh, E.; Peters, T.J.; Al-Janabi, H.; Clemens, S.; Moody, A.; Coast, J. Scoring the Icecap-a Capability Instrument. Estimation of a UK General Population Tariff. Health Econ. 2015, 24, 258–269. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Well-Being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Hernández Alava, M.; Pudney, S.; Wailoo, A. Estimating the Relationship Between EQ-5D-5L and EQ-5D-3L: Results from a UK Population Study. PharmacoEconomics 2023, 41, 199–207. [Google Scholar] [CrossRef]
- Coast, J.; Flynn, T.N.; Natarajan, L.; Sproston, K.; Lewis, J.; Louviere, J.J.; Peters, T.J. Valuing the ICECAP capability index for older people. Soc. Sci. Med. 2008, 67, 874–882. [Google Scholar] [CrossRef] [PubMed]
- De Nys, L.; Oyebola, E.F.; Connelly, J.; Ryde, G.C.; Whittaker, A.C. Digital music and movement intervention to improve health and wellbeing in older adults in care homes: A pilot mixed methods study. BMC Geriatr. 2024, 24, 733. [Google Scholar] [CrossRef]
- Baker, S.; Waycott, J.; Robertson, E.; Carrasco, R.; Neves, B.B.; Hampson, R.; Vetere, F. Evaluating the use of interactive virtual reality technology with older adults living in residential aged care. Inf. Process. Manag. 2020, 57, 102105. [Google Scholar] [CrossRef]
- Paravati, E.; Naidu, E.; Gabriel, S. Thank you for the music: Music as a social surrogate that protects against social threats. Psychol. Music 2025, 03057356241312219. [Google Scholar] [CrossRef]
- Ko, B.; Kim, K. Assessing music-related memory in people with dementia: A scoping review. Aging Ment. Health 2023, 27, 876–886. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| ID | Age | Gender | EQ-5D 5L Scores | EQ-5D 5L Visual Analogue Scores | ICECAP-O | SWEMWBS |
|---|---|---|---|---|---|---|
| 1 | X | X | x | x | x | x |
| 2 | 79 | Female | ✓ | ✓ | ✓ | ✓ |
| 3 | X | X | x | x | x | x |
| 4 | 94 | Female | ✓ | ✓ | ✓ | x |
| 5 | 75 | Female | x | x | x | x |
| 6 | 41 | Male | x | x | ✓ | ✓ |
| 7 | 80 | Female | x | x | x | x |
| 8 | 43 | Female | ✓ | ✓ | ✓ | x |
| 9 | 87 | Female | x | x | x | x |
| 10 | 84 | Male | ✓ | x | x | ✓ |
| 11 | 60 | Female | x | x | x | x |
| 12 | 81 | Female | x | x | x | x |
| 13 | X | X | x | x | x | x |
| Average 72.4 | Female 8/10 | Complete scores at all time points = (✓) not completed at all time points = (x) | ||||
| Male 2/10 | 4 | 3 | 4 | 3 | ||
| Baseline | Day 1 | Day 8 | Day 15 | Day 22 | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | Mobility | Self-Care | Usual activities | Pain | Anxiety/depression | Mobility | Self-Care | Usual activities | Pain | Anxiety/depression | Mobility | Self-Care | Usual activities | Pain | Anxiety/depression | Mobility | Self-Care | Usual activities | Pain | Anxiety/depression | Mobility | Self-Care | Usual activities | Pain | Anxiety/depression |
| 1 | 1 | 1 | 3 | 4 | 2 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 2 | 3 | 1 | 2 | 4 | 2 | 3 | 2 | 2 | 3 | 2 | 3 | 2 | 3 | 4 | 1 | 3 | 2 | 3 | 3 | 1 | 3 | 2 | 2 | 3 | 2 |
| 3 | 3 | 2 | 3 | 2 | 3 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 4 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2 |
| 5 | 3 | 3 | 2 | 4 | 1 | X | X | X | X | X | X | X | X | X | X | X | XA | X | X | X | X | x | X | X | X |
| 6 | 3 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 3 | 2 | 3 | 1 | 2 | 2 | X | X | X | X | X | 3 | 1 | 2 | 2 | 2 |
| 7 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | 2 | 2 | 3 | 2 | X | X | X | X | X |
| 8 | 3 | 1 | 1 | 1 | 5 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 2 |
| 9 | 4 | 4 | 1 | 5 | 1 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 10 | 4 | 5 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 3 | 3 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 5 | 2 | 1 | 1 |
| 11 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 12 | X | X | X | X | X | 1 | 1 | 1 | 1 | 1 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 13 | X | X | X | X | X | X | X | X | X | X | 1 | 2 | 2 | 3 | 1 | X | X | X | X | X | X | X | X | X | |
| ID | Baseline | Day 1 | Day 8 | Day 15 | Day 22 |
|---|---|---|---|---|---|
| 1 | X | X | X | X | X |
| 2 | 0.497 | 0.578 | 0.307 | 0.575 | 0.578 |
| 3 | X | X | X | X | X |
| 4 | 0.837 | 0.837 | 0.902 | 0.871 | 0.704 |
| 5 | 0.312 | X | X | X | X |
| 6 | 0.619 | 0.616 | 0.635 | X | 0.669 |
| 7 | 0.7 | 0.697 | 0.617 | 0.578 | X |
| 8 | 0.314 | 0.817 | 0.985 | 0.89 | 0.847 |
| 9 | −0.029 | X | X | X | X |
| 10 | 0.541 | 0.946 | 0.68 | 0.989 | 0.871 |
| 11 | 0.889 | 0.889 | X | X | X |
| 12 | X | 0.988 | X | X | X |
| 13 | X | X | X | X | X |
| Total number of participants at this point | 9 | 8 | 6 | 5 | 5 |
| Average EQ-5D-5L score (all) | 0.520 | 0.796 | 0.688 | 0.781 | 0.734 |
| Average EQ-5D-5L score (complete case) | 0.547 | 0.795 | 0.719 | 0.831 | 0.750 |
| Average all | 72.4 | Average (complete case) | 76 |
| ID | Baseline | Day 1 | Day 8 | Day 15 | Day 22 |
|---|---|---|---|---|---|
| 1 | 60 | X | X | X | X |
| 2 | 60 | 75 | 65 | 75 | 67 |
| 3 | 50 | X | X | X | X |
| 4 | 95 | 80 | 80 | 95 | 85 |
| 5 | 70 | X | X | X | X |
| 6 | 50 | 70 | 85 | X | 70 |
| 7 | 85 | 75 | 72 | 50 | X |
| 8 | 80 | 25 | 75 | 50 | 50 |
| 9 | 50 | X | X | X | X |
| 10 | 85 | 80 | X | 80 | 75 |
| 11 | 60 | 50 | X | X | X |
| 12 | X | 99 | X | X | X |
| 13 | X | X | X | X | X |
| Complete case scores | |||||
| Mean | 78.3 | 60.0 | 73.3 | 73.3 | 67.3 |
| SD | 10.1 | 17.6 | 4.4 | 13.0 | 10.1 |
| 95%CI lb | 58.5 | 25.6 | 64.7 | 47.8 | 47.5 |
| 95%CI ub | 98.2 | 94.4 | 82.0 | 98.8 | 87.1 |
| All scores | |||||
| Mean | 67.7 | 69.3 | 75.4 | 70.0 | 69.4 |
| SD | 4.9 | 7.9 | 3.4 | 8.8 | 5.7 |
| 95%CI lb | 58.2 | 53.7 | 68.7 | 52.7 | 58.2 |
| 95%CI ub | 77.3 | 84.8 | 82.1 | 87.3 | 80.6 |
| Baseline | Day 22 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ID | Attachment | Security | Role | Enjoyment | Control | Attachment | Security | Role | Enjoyment | Control |
| 1 | 2 | 1 | 2 | 2 | 2 | X | X | X | X | X |
| 2 | 4 | 2 | 3 | 2 | 3 | 4 | 2 | 2 | 4 | 3 |
| 3 | 3 | 3 | 2 | 3 | 2 | X | X | X | X | X |
| 4 | 4 | 4 | 2 | 3 | 2 | 3 | 3 | 3 | 3 | 3 |
| 5 | 3 | 3 | 3 | 3 | 2 | X | X | X | X | X |
| 6 | 2 | 2 | 2 | 2 | 2 | 4 | 3 | 2 | 3 | 3 |
| 7 | 3 | 3 | 3 | 2 | 3 | X | X | X | X | X |
| 8 | 3 | 4 | 4 | 4 | 3 | 2 | 4 | 4 | 3 | 3 |
| 9 | 4 | 3 | 4 | 4 | 1 | X | X | X | X | X |
| 10 | 4 | 4 | 4 | 3 | 1 | X | 4 | 3 | 4 | 1 |
| 11 | 3 | 2 | 4 | 3 | 3 | X | X | X | X | X |
| ID | Age | Gender | Baseline | Day 22 |
|---|---|---|---|---|
| 1 | NA | NA | 0.52 | NA |
| 2 | 79 | Female | 0.8 | 0.8 |
| 3 | NA | NA | 0.74 | NA |
| 4 | 94 | Female | 0.83 | 0.87 |
| 5 | 75 | Female | 0.79 | NA |
| 6 | 41 | Male | 0.56 | 0.84 |
| 7 | 80 | Female | 0.82 | NA |
| 8 | 43 | Female | 0.95 | 0.85 |
| 9 | 87 | Female | 0.67 | NA |
| 10 | 84 | Male | 0.74 | NA |
| 11 | 60 | Female | 0.84 | NA |
| Average age | 71.44 | Total number of participants by time point | 11 | 4 |
| Average (all) | 72.4 | Average ICECAP-O score (all)(SD, min–max) | 0.75 (0.13), 0.52 to 0.95 | |
| Average (complete case) | 64.25 | Average ICECAP-O score (complete case) (SD, min–max) | 0.79 (0.17) 0.56 to 0.95 | 0.84 (0.03) 0.80 to 0.87 |
| Baseline | Day 22 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | Raw Score | Raw Score | ||||||||||||||
| 1 | 2 | 1 | 1 | 3 | 3 | 1 | 3 | 14 | X | X | X | X | X | X | X | X |
| 2 | 3 | 2 | 4 | 4 | 4 | 4 | 5 | 26 | 3 | 2 | 4 | 5 | 5 | 3 | 5 | 27 |
| 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | 19 | X | X | X | X | X | X | X | X |
| 4 | 2 | 1 | 5 | 5 | 5 | 3 | 4 | 25 | 3 | 4 | 5 | X | 5 | 4 | 4 | X |
| 5 | 2 | 4 | 3 | 4 | 4 | 4 | 4 | 25 | X | X | X | X | X | X | X | X |
| 6 | 4 | 2 | 3 | 3 | 3 | 3 | 5 | 23 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 21 |
| 7 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 21 | X | X | X | X | X | X | X | X |
| 8 | 3 | 3 | 4 | 4 | 2 | 1 | 5 | 22 | X | 4 | 5 | 5 | 2 | 1 | 5 | X |
| 9 | 4 | 1 | 4 | 3 | 5 | 4 | 4 | 25 | X | X | X | X | X | X | X | X |
| 10 | 4 | 4 | 5 | 4 | 5 | 5 | 4 | 31 | 5 | 1 | 3 | 3 | 2 | 4 | 5 | 23 |
| 11 | 3 | 4 | 3 | 3 | 2 | 3 | 2 | 20 | X | X | X | X | X | X | X | X |
| ID | Age | Gender | Baseline | Day 22 |
|---|---|---|---|---|
| 1 | X | X | 15.32 | X |
| 2 | 79 | Female | 23.21 | 24.11 |
| 3 | X | X | 17.98 | X |
| 4 | 94 | Female | 22.35 | X |
| 5 | 75 | Female | 22.35 | X |
| 6 | 41 | Male | 20.73 | 19.25 |
| 7 | 80 | Female | 19.25 | X |
| 8 | 43 | Female | 19.98 | X |
| 9 | 87 | Female | 22.35 | X |
| 10 | 84 | Male | 28.13 | 20.73 |
| 11 | 60 | Female | 18.59 | X |
| Average age | 71.44 | Total number of participants by time point | 11 | 3 |
| Average (all) | 72.4 | Average SWEMWEBS score (all) (SD, min–max) | 20.93 (3.35), 15.32 to 28.13 | |
| Average (complete case) | 64.25 | Average SWEMWBS score (complete case) (SD, min–max) | 24.02 (3.77, 20.73–28.13) | 21.36 (2.49, 19.25–24.11) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daffern, H.; Weatherly, H.; Saramago, P.; Steele, K.; Greaves, D.; Kavanagh, M.; Cooney, L.; Spreadborough, J.; Honnan, S.; Johnston, D.; et al. Virtual Choirs in Care Homes: The Development and Early Assessment of a New Virtual Reality Choir Intervention. Virtual Worlds 2025, 4, 8. https://doi.org/10.3390/virtualworlds4010008
Daffern H, Weatherly H, Saramago P, Steele K, Greaves D, Kavanagh M, Cooney L, Spreadborough J, Honnan S, Johnston D, et al. Virtual Choirs in Care Homes: The Development and Early Assessment of a New Virtual Reality Choir Intervention. Virtual Worlds. 2025; 4(1):8. https://doi.org/10.3390/virtualworlds4010008
Chicago/Turabian StyleDaffern, Helena, Helen Weatherly, Pedro Saramago, Kim Steele, Dana Greaves, Maeve Kavanagh, Lucy Cooney, Jake Spreadborough, Stephen Honnan, Daniel Johnston, and et al. 2025. "Virtual Choirs in Care Homes: The Development and Early Assessment of a New Virtual Reality Choir Intervention" Virtual Worlds 4, no. 1: 8. https://doi.org/10.3390/virtualworlds4010008
APA StyleDaffern, H., Weatherly, H., Saramago, P., Steele, K., Greaves, D., Kavanagh, M., Cooney, L., Spreadborough, J., Honnan, S., Johnston, D., & Toomer, R. (2025). Virtual Choirs in Care Homes: The Development and Early Assessment of a New Virtual Reality Choir Intervention. Virtual Worlds, 4(1), 8. https://doi.org/10.3390/virtualworlds4010008