
Minorities’ Diminished Psychedelic Returns: Gender, Perceived Stigma, and Distress


Abstract
1. Introduction
2. Data and Methods
2.1. Study Replications
2.2. Key Dependent Variable: Stigma
2.3. Key Independent Variables: Gender, Psychological Distress, and Psychedelic Use
2.4. Socioeconomic, Demographic, and Drug Use Control Variables
2.5. Analytic Strategy
3. Results
3.1. Descriptive Statistics
3.2. Do Psychedelic Users Perceive Less Stigma?
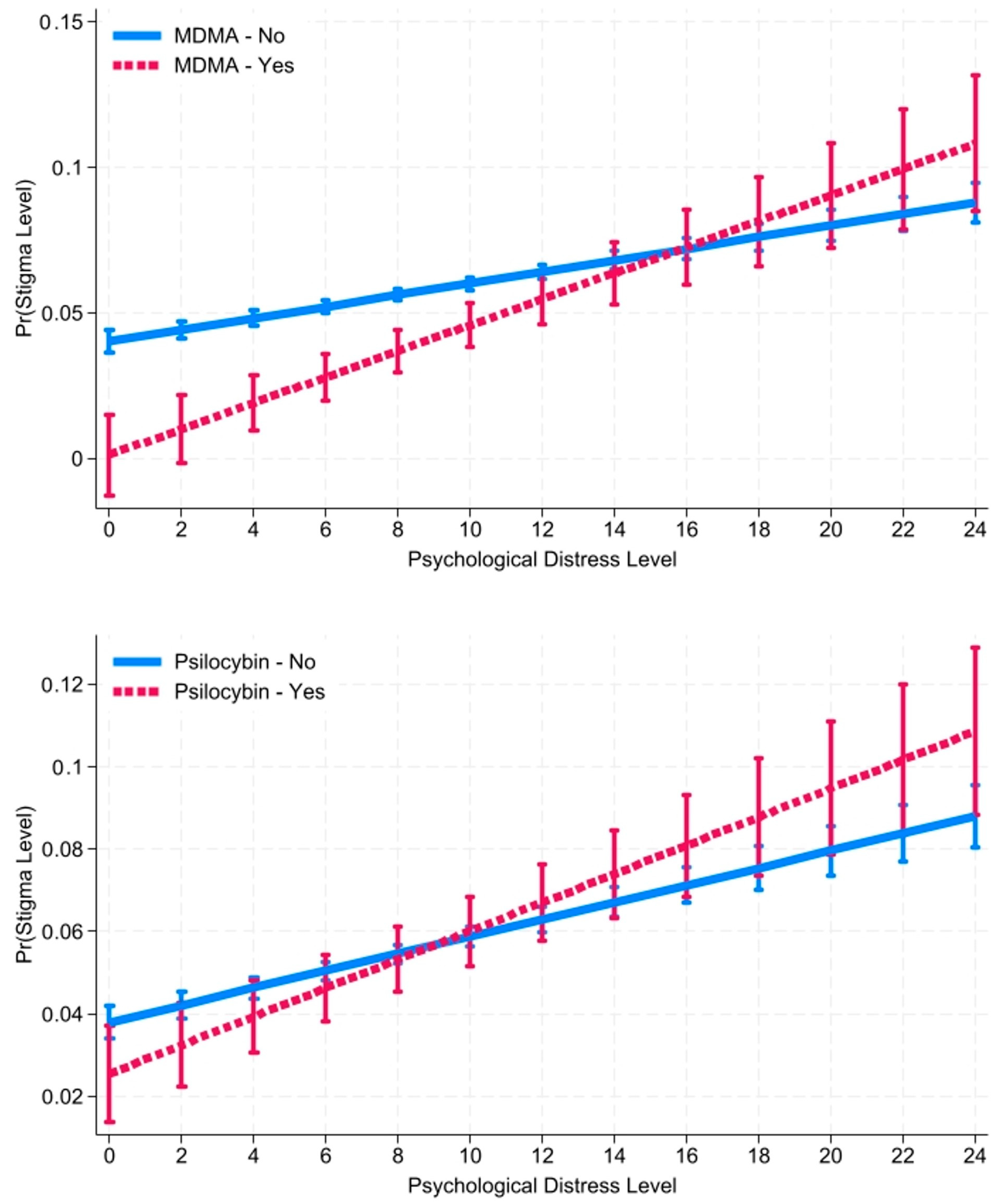
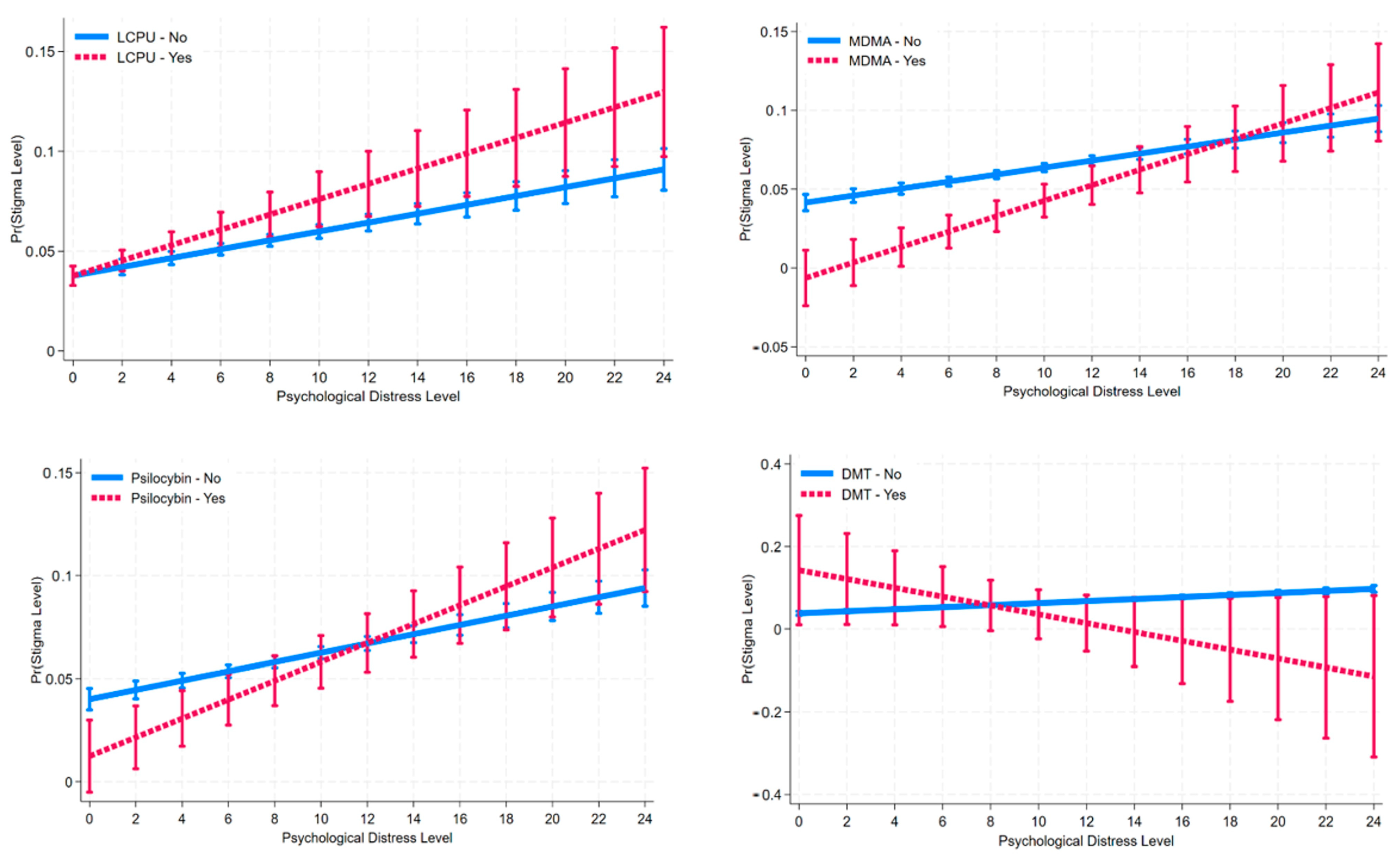
3.3. Does Psychedelic Use Moderate Distress on Stigma?
4. Discussion
5. Limitations and Future Directions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luoma, J.B.; Chwyl, C.; Bathje, G.J.; Davis, A.K.; Lancelotta, R. A Meta-Analysis of Placebo-Controlled Trials of Psychedelic-Assisted Therapy. J. Psychoact. Drugs 2020, 52, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.M.; Nock, M.K. Race and Ethnicity Moderate the Associations between Lifetime Psychedelic Use (MDMA and Psilocybin) and Psychological Distress and Suicidality. Sci. Rep. 2022, 37, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.M.; Nock, M.K. MDMA/Ecstasy Use and Psilocybin Use Are Associated with Lowered Odds of Psychological Distress and Suicidal Thoughts in a Sample of US Adults. J. Psychopharmacol. 2022, 36, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Maclean, K.A.; Johnson, M.W.; Griffiths, R.R. Mystical experiences occasioned by the hallucinogen psilocybin lead to increases in the personality domain of openness. J. Psychoph. 2011, 25, 1453–1461. [Google Scholar] [CrossRef]
- Griffiths, R.R.; Richards, W.A.; McCann, U.; Jesse, R. Psilocybin Can Occasion Mystical-Type Experiences Having Substantial and Sustained Personal Meaning and Spiritual Significance. Psychopharmacology 2006, 187, 268–283. [Google Scholar] [CrossRef] [PubMed]
- Mans, K.; Kettner, H.; Erritzoe, D.; Haijen, E.C.H.M.; Kaelen, M.; Carhart-Harris, R.L. Sustained, Multifaceted Improvements in Mental Well-Being Following Psychedelic Experiences in a Prospective Opportunity Sample. Front. Psychiatry 2021, 12, 647909. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.E.; Chambers, R.; Liknaitzky, P. Combining Psychedelic and Mindfulness Interventions: Synergies to Inform Clinical Practice. In ACS Pharmacology and Translational Science; American Chemical Society: Washington, DC, USA, 2021; pp. 416–423. [Google Scholar] [CrossRef]
- Søndergaard, A.; Madsen, M.K.; Ozenne, B.; Armand, S.; Knudsen, G.M.; Fisher, P.M.D.; Stenbæk, D.S. Lasting Increases in Trait Mindfulness after Psilocybin Correlate Positively with the Mystical-Type Experience in Healthy Individuals. Front. Psychol. 2022, 13, 948729. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, R.G.; Bouso, J.C.; Alcázar-Córcoles, M.Á.; Hallak, J.E.C. Efficacy, Tolerability, and Safety of Serotonergic Psychedelics for the Management of Mood, Anxiety, and Substance-Use Disorders: A Systematic Review of Systematic Reviews. In Expert Review of Clinical Pharmacology; Taylor and Francis Ltd.: Oxfordshire, UK, 2018; pp. 889–902. [Google Scholar] [CrossRef]
- Hendricks, P.S.; Thorne, C.B.; Clark, C.B.; Coombs, D.W.; Johnson, M.W. Classic Psychedelic Use Is Associated with Reduced Psychological Distress and Suicidality in the United States Adult Population. J. Psychopharmacol. 2015, 29, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.H.W.; Davis, A.K.; Xin, Y.; Williams, M.T. Effects of Psychedelic Use on Racial Trauma Symptoms and Ethnic Identity among Asians in North America. J. Psychoact. Drugs 2023, 55, 19–29. [Google Scholar] [CrossRef]
- Williams, D.R. Stress and the Mental Health of Populations of Color: Advancing Our Understanding of Race-Related Stressors. J. Health Soc. Behav. 2018, 59, 466–485. [Google Scholar] [CrossRef]
- Williams, D.Z. Examining the Relationship between Race-Related Stressors and Post-Traumatic Stress Disorder among African American; Washington State University, College of Education: Washington, DC, USA, 2007. [Google Scholar]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon & Schuster, Inc.: New York, NY, USA, 1963. [Google Scholar]
- Link, B.G.; Phelan, J.C. Conceptualizing Stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J.C. Labeling and Stigma. In Handbook of the Sociology of Mental Health; Aneshensel, C.S., Phelan, J.C., Bierman, A., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 525–541. [Google Scholar] [CrossRef]
- Levy, B.R.; Pilver, C.E. Residual Stigma: Psychological Distress among the Formerly Overweight. Soc. Sci. Med. 2012, 75, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.W.; Watson, A.C. The Paradox of Self-Stigma and Mental Illness. Clin. Psychol. Sci. Pract. 2002, 9, 35–53. [Google Scholar] [CrossRef]
- Pescosolido, B.A.; Martin, J.K. The Stigma Complex. Annu. Rev. Sociol. 2015, 41, 87–116. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, B.A.; Halpern-Manners, A.; Luo, L.; Perry, B. Trends in Public Stigma of Mental Illness in the US, 1996–2018. JAMA Netw. Open 2021, 4, e2140202. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, B.A. The Public Stigma of Mental Illness: What Do We Think; What Do We Know; What Can We Prove? J. Health Soc. Behav. 2013, 54, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.T.; Cabral, V.; Faber, S. Psychedelics and Racial Justice. Int. J. Ment. Health Addict. 2023, 1–17. [Google Scholar] [CrossRef]
- Thrul, J.; Garcia-Romeu, A. Whitewashing Psychedelics: Racial Equity in the Emerging Field of Psychedelic-Assisted Mental Health Research and Treatment. In Drugs: Education, Prevention and Policy; Taylor and Francis Ltd.: Oxfordshire, UK, 2021; pp. 211–214. [Google Scholar] [CrossRef]
- Neitzke-Spruill, L. Race as a Component of Set and Setting: How Experiences of Race Can Influence Psychedelic Experiences. J. Psychedelic Stud. 2019, 4, 51–60. [Google Scholar] [CrossRef]
- Korman, B.A. Could Classic Psychedelics Influence Immigrants’ Acculturation Process? A Narrative Review Contemplating How. Drug Sci. Policy Law 2023, 9, 20503245231191400. [Google Scholar] [CrossRef]
- Carlin, S. MDMA Therapy Training for Communities of Color. MAPS Bull. Res. 2020, 30, 12–18. [Google Scholar]
- Williams, M.T. Race-Based Trauma: The Challenge and Promise of MDMA-Assisted Psychotherapy; 2016. Available online: https://www.researchgate.net/publication/300920255 (accessed on 1 February 2024).
- Michaels, T.I.; Purdon, J.; Collins, A.; Williams, M.T. Inclusion of People of Color in Psychedelic-Assisted Psychotherapy: A Review of the Literature. BMC Psychiatry 2018, 18, 245. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.T.; Reed, S.; Aggarwal, R. Culturally Informed Research Design Issues in a Study for MDMA-Assisted Psychotherapy for Posttraumatic Stress Disorder. J. Psychedelic Stud. 2019, 4, 40–50. [Google Scholar] [CrossRef]
- Link, B.G.; Cullen, F.T.; Struening, E.; Shrout, P.E.; Dohrenwend, P.B. A Modified Labeling Theory Approach to Mental Disorders: An Empirical Assessment Published. Am. Sociol Rev. 1989, 54, 400–423. [Google Scholar] [CrossRef]
- Borenstein, J. Stigma, Prejudice and Discrimination Against People with Mental Illness; American Psychiatric Assocation: Washington, DC, USA, 2020; Available online: https://www.psychiatry.org/patients-families/stigma-and-discrimination (accessed on 1 February 2024).
- Pescosolido, B.A.; Medina, T.R.; Martin, J.K.; Long, J.S. The “Backbone” of Stigma: Identifying the Global Core of Public Prejudice Associated with Mental Illness. Am. J. Public Health 2013, 103, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Noorani, T. Containment Matters: Set and Setting in Contemporary Psychedelic Psychiatry. Philos. Psychiatry Psychol. 2021, 28, 201–216. [Google Scholar] [CrossRef]
- Doering, L.; Thébaud, S. The Effects of Gendered Occupational Roles on Men’s and Women’s Workplace Authority: Evidence from Microfinance. Am. Sociol Rev. 2017, 82, 542–567. [Google Scholar] [CrossRef]
- Harder, B.M.; Sumerau, J.E. Understanding Gender as a Fundamental Cause of Health: Simultaneous Linear Relationships between Gender, Mental Health, and Physical Health over Time. Sociol. Spectr. 2018, 38, 387–405. [Google Scholar] [CrossRef]
- Hochschild, A.; Machung, A. The Second Shift: Working Families and the Revolution at Home, 3rd ed.; Penguin Books Ltd.: London, UK, 2012. [Google Scholar]
- WHO. Global, Regional, and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence against Women; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Naaman, E.; Gelfand Saar, L.; Naftali Ben-Haim, L.; Barak, Y.; Bar, N.; Labardini, C.; Soudry, S. Examination of Inattentive Gender Bias in Medicine: Patients’ Form of Addressing Male and Female Physicians. Cogent. Soc. Sci. 2022, 8, 2136605. [Google Scholar] [CrossRef]
- Monzani, D.; Vergani, L.; Pizzoli, S.F.M.; Marton, G.; Mazzocco, K.; Bailo, L.; Messori, C.; Pancani, L.; Cattelan, M.; Pravettoni, G. Sexism Interacts with Patient–Physician Gender Concordance in Influencing Patient Control Preferences: Findings from a Vignette Experimental Design. Appl. Psychol. Health Well Being 2020, 12, 471–492. [Google Scholar] [CrossRef]
- Champagne-Langabeer, T.; Hedges, A.L. Physician Gender as a Source of Implicit Bias Affecting Clinical Decision-Making Processes: A Scoping Review. BMC Med. Educ. 2021, 21, 171. [Google Scholar] [CrossRef]
- Hartogsohn, I. Set and Setting, Psychedelics and the Placebo Response: An Extra-Pharmacological Perspective on Psychopharmacology. J. Psychopharmacol. 2016, 30, 1259–1267. [Google Scholar] [CrossRef]
- Viña, S.M. Minorities’ Diminished Psychedelic Returns: Cardio-Metabolic Health. Drug Sci. Policy Law 2024, 10, 1–13. [Google Scholar] [CrossRef]
- Viña, S.M.; Stephens, A.L. Minorities’ Diminished Psychedelic Returns. Drug Sci. Policy Law 2023, 9, 1–19. [Google Scholar] [CrossRef]
- Viña, S.M.; Stephens, A.L. Psychedelics and Workplace Harm. Front. Psychiatry 2023, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Viña, S.M. Diminished Psychedelic Returns on Distress: Marital Status and Household Size. PLoS ONE 2024, 19, 1–23. [Google Scholar] [CrossRef]
- Viña, S. The Harmful Relationship Between Classic Psychedelic Use and Religion on Mental Health. In Proceedings of the American Sociological Association 117th Annual Meeting: Bureaucracies of Displacement, Los Angeles, CA, USA, 5–9 August 2022. [Google Scholar]
- Quinn, D.M.; Williams, M.K.; Weisz, B.M. From Discrimination to Internalized Mental Illness Stigma: The Mediating Roles of Anticipated Discrimination and Anticipated Stigma. Psychiatr. Rehabil. J. 2015, 38, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Simonsson, O.; Sexton, J.D.; Hendricks, P.S. Associations between Lifetime Classic Psychedelic Use and Markers of Physical Health. J. Psychopharmacol. 2021, 35, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Simonsson, O.; Hendricks, P.S.; Carhart-Harris, R.; Kettner, H.; Osika, W. Association between Lifetime Classic Psychedelic Use and Hypertension in the Past Year. Hypertension 2021, 77, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, P.S.; Crawford, M.S.; Cropsey, K.L.; Copes, H.; Sweat, N.W.; Walsh, Z.; Pavela, G. The Relationships of Classic Psychedelic Use with Criminal Behavior in the United States Adult Population. J. Psychopharmacol. 2018, 32, 37–48. [Google Scholar] [CrossRef]
- Choi, N.G.; DiNitto, D.M.; Marti, C.N. Treatment Use, Perceived Need, and Barriers to Seeking Treatment for Substance Abuse and Mental Health Problems among Older Adults Compared to Younger Adults. Drug Alcohol. Depend 2014, 145, 113–120. [Google Scholar] [CrossRef]
- Mason, M.J.; Keyser-Marcus, L.; Snipes, D.; Benotsch, E.; Sood, B. Perceived Mental Health Treatment Need and Substance Use Correlates among Young Adults. Psychiatr. Serv. 2013, 64, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B.; Neicun, J.; Yang, J.C.; Roman-Urrestarazu, A. Substance Use among Sexual Minorities in the US—Linked to Inequalities and Unmet Need for Mental Health Treatment? Results from the National Survey on Drug Use and Health (NSDUH). J. Psychiatr. Res. 2021, 135, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Salameh, T.; Hall, L.; Crawford, T.; Hall, M. Perceived Barriers to Mental Health and Substance Use Treatment among US Childbearing-Aged Women: NSDUH 2008–2014. Women Health 2021, 61, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Gearing, R.E.; Polyanskaya, O. Influence of Health Beliefs and Stigma on Choosing Internet Support Groups over Formal Mental Health Services. Psychiatr. Serv. 2012, 63, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Bromet, E.; Cuitan, M.; Furukawa, T.A.; Oye, G.; Hinkov, H.; Hu, C.Y.; et al. Screening for Serious Mental Illness in the General Population with the K6 Screening Scale: Results from the WHO World Mental Health (WMH) Survey Initiative. Int. J. Methods Psychiatr. Res. 2010, 19 (Suppl. S1), 4–22. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short Screening Scales to Monitor Population Prevalences and Trends in Non-Specific Psychological Distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Cotton, S.M.; Menssink, J.; Filia, K.; Rickwood, D.; Hickie, I.B.; Hamilton, M.; Hetrick, S.; Parker, A.; Herrman, H.; McGorry, P.D.; et al. The Psychometric Characteristics of the Kessler Psychological Distress Scale (K6) in Help-Seeking Youth: What Do You Miss When Using It as an Outcome Measure? Psychiatry Res. 2021, 305, 114182. [Google Scholar] [CrossRef] [PubMed]
- Umucu, E.; Fortuna, K.; Jung, H.; Bialunska, A.; Lee, B.; Mangadu, T.; Storm, M.; Ergun, G.; Mozer, D.A.; Brooks, J. A National Study to Assess Validity and Psychometrics of the Short Kessler Psychological Distress Scale (K6). Rehabil. Couns Bull. 2022, 65, 140–149. [Google Scholar] [CrossRef]
- Ly, C.; Greb, A.C.; Cameron, L.P.; Wong, J.M.; Barragan, E.V.; Wilson, P.C.; Burbach, K.F.; Soltanzadeh Zarandi, S.; Sood, A.; Paddy, M.R.; et al. Psychedelics Promote Structural and Functional Neural Plasticity. Cell Rep. 2018, 23, 3170–3182. [Google Scholar] [CrossRef]
- NIDA. MDMA (Ecstasy/Molly) Drug Facts. NIDA. MDMA (Ecstasy/Molly) DrugFacts. National Institute on Drug Abuse Website. Available online: https://nida.nih.gov/publications/drugfacts/mmdma-ecstasymolly (accessed on 15 October 2023).
- Mitchell, J.M.; Bogenschutz, M.; Lilienstein, A.; Harrison, C.; Kleiman, S.; Parker-Guilbert, K.; Ot’alora, G.M.; Garas, W.; Paleos, C.; Gorman, I.; et al. MDMA-Assisted Therapy for Severe PTSD: A Randomized, Double-Blind, Placebo-Controlled Phase 3 Study. Nat. Med. 2021, 27, 1025–1033. [Google Scholar] [CrossRef]
- Brewerton, T.D.; Wang, J.B.; Lafrance, A.; Pamplin, C.; Mithoefer, M.; Yazar-Klosinki, B.; Emerson, A.; Doblin, R. MDMA-Assisted Therapy Significantly Reduces Eating Disorder Symptoms in a Randomized Placebo-Controlled Trial of Adults with Severe PTSD. J. Psychiatr. Res. 2022, 149, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Mithoefer, M.C.; Feduccia, A.A.; Jerome, L.; Mithoefer, A.; Wagner, M.; Walsh, Z.; Hamilton, S.; Yazar-Klosinski, B.; Emerson, A.; Doblin, R. MDMA-Assisted Psychotherapy for Treatment of PTSD: Study Design and Rationale for Phase 3 Trials Based on Pooled Analysis of Six Phase 2 Randomized Controlled Trials. Psychopharmacology 2019, 236, 2735–2745. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.H.W.; Williams, M.T.; Wang, J.B.; Jerome, L.; Yazar-Klosinski, B.; Emerson, A.; Doblin, R. MDMA-Assisted Therapy for Posttraumatic Stress Disorder: A Pooled Analysis of Ethnoracial Differences in Efficacy and Safety from Two Phase 2 Open-Label Lead-in Trials and a Phase 3 Randomized, Blinded Placebo-Controlled Trial. J. Psychopharmacol. 2022, 36, 974–986. [Google Scholar] [CrossRef] [PubMed]
- Simonsson, O.; Osika, W.; Carhart-Harris, R.; Hendricks, P.S. Associations between Lifetime Classic Psychedelic Use and Cardiometabolic Diseases. Sci. Rep. 2021, 11, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Clemens, K.J.; McGregor, I.S.; Hunt, G.E.; Cornish, J.L. MDMA, Methamphetamine and Their Combination: Possible Lessons for Party Drug Users from Recent Preclinical Research. Drug Alcohol Rev. 2007, 26, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Rigg, K.K. Motivations for Using MDMA (Ecstasy/Molly) among African Americans: Implications for Prevention and Harm-Reduction Programs. J. Psychoact. Drugs 2017, 49, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Palamar, J.J.; Keyes, K.M. Trends in Drug Use among Electronic Dance Music Party Attendees in New York City, 2016–2019. Drug Alcohol Depend. 2020, 209, 107889. [Google Scholar] [CrossRef] [PubMed]
- Johnstad, P.G. Who Is the Typical Psychedelics User? Methodological Challenges for Research in Psychedelics Use and Its Consequences. Nord. Stud. Alcohol Drugs 2021, 38, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Viña, S.M. Socioeconomic Status and Minorities’ Diminished Psychedelic Return on Distress. J. Race Ethn. Health Disparities 2024. Accepted (Forthcoming). [Google Scholar]
- Jones, P.N. The Native American Church, Peyote, and Health: Expanding Consciousness for Healing Purposes. Contemp. Justice Rev. 2007, 10, 411–425. [Google Scholar] [CrossRef]
- Halpern, J.H.; Sherwood, A.R.; Hudson, J.I.; Yurgelun-Todd, D.; Pope, H.G. Psychological and Cognitive Effects of Long-Term Peyote Use among Native Americans. Biol. Psychiatry 2005, 58, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Viña, S.M. Religion, Psychedelics, Risky Behavior, and Violence. J. Psychoact. Drugs 2024, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Long, J.S.; Freese, J. Regression Models for Categorical Dependent Variables Using Stata, 3rd ed.; Stata Press: College Station, TX, USA, 2014. [Google Scholar]
- Long, J.S. Group Comparisons in Logit and Probit Using Predicted Probabilities; Indiana University Bloomington: Bloomington, Indiana, 2009; Available online: http://www.indiana.edu/~jslsoc/files_research/groupdif/groupwithprobabilities/groups-with-prob-2009-06-25.pdf (accessed on 1 February 2024).
- Oberfichtner, M.; Tauchmann, H. Stacked Linear Regression Analysis to Facilitate Testing of Hypotheses across OLS Regressions. Stata J. Promot. Commun. Stat. Stata 2021, 21, 411–429. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to Use the Bonferroni Correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.M. Race and Ethnicity Moderate the Associations between Lifetime Psychedelic Use (MDMA/Ecstasy and Psilocybin) and Major Depressive Episodes. J. Psychopharmacol. 2023, 37, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Meyers, S.A.; Earnshaw, V.A.; D’Ambrosio, B.; Courchesne, N.; Werb, D.; Smith, L.R. The Intersection of Gender and Drug Use-Related Stigma: A Mixed Methods Systematic Review and Synthesis of the Literature. Drug Alcohol Depend. 2021, 223, 108706. [Google Scholar] [CrossRef] [PubMed]
- Newhart, M.; Dolphin, W. The Medicalization of Marijuana: Legitimacy, Stigma, and the Patient Experience; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Back, S.E.; Payne, R.L.; Wahlquist, A.H.; Carter, R.E.; Stroud, Z.; Haynes, L.; Hillhouse, M.; Brady, K.T.; Ling, W. Comparative Profiles of Men and Women with Opioid Dependence: Results from a National Multisite Effectiveness Trial. Am. J. Drug Alcohol Abus. 2011, 37, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Cormier, Z. No Link Found between Psychedelics and Psychosis. Nature 2015. [Google Scholar] [CrossRef]
- Lenzenweger, M.F. Schizotypy, Schizotypic Psychopathology and Schizophrenia. World Psychiatry 2018, 17, 25–26. [Google Scholar] [CrossRef]
- Barber, G.; Nemeroff, C.B.; Siegel, S. A Case of Prolonged Mania, Psychosis, and Severe Depression After Psilocybin Use: Implications of Increased Psychedelic Drug Availability. Am. J. Psychiatry 2022, 179, 892–896. [Google Scholar] [CrossRef]
- Morton, E.; Sakai, K.; Ashtari, A.; Pleet, M.; Michalak, E.E.; Woolley, J. Risks and Benefits of Psilocybin Use in People with Bipolar Disorder: An International Web-Based Survey on Experiences of ‘Magic Mushroom’ Consumption. J. Psychopharmacol. 2023, 37, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, B.A.; Martin, J.K.; Link, B.G.; Kikuzawa, S.; Burgos, G.; Swingle, R.; Phelan, J. Americans’ Views of Mental Health and Illness at Century’s End: Continuity and Change; Indiana University: Bloomington, IN, USA, 2006. [Google Scholar]
- Corrigan, P.W.; Nieweglowski, K.; Sayer, J. Self-Stigma and the Mediating Impact of the “Why Try” Effect on Depression. J. Community Psychol. 2019, 47, 698–705. [Google Scholar] [CrossRef] [PubMed]
- McGuffey, C.S. “Saving Masculinity”: Gender Reaffirmation, Sexuality, Race, and Parental Responses to Male Child Sexual Abuse. Soc. Probl. 2008, 55, 216–237. [Google Scholar] [CrossRef]
- NIH. National Survey on Drug Use and Health (NSDUH); NIH: Washington, DC, USA, 2021. [Google Scholar]
- SAMHSA Substance Abuse and Mental Health Service Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health. 2021. Available online: https://jslsoc.sitehost.iu.edu/files_research/groupdif/groupwithprobabilities/groups-with-prob-2009-05-28.pdf (accessed on 1 June 2023).
- Marlan, D. The Myth of Psychedelic Exceptionalism. Harvard Law: Bill of Health. Available online: https://blog.petrieflom.law.harvard.edu/2021/03/24/psychedelic-exceptionalism-drug-policy/ (accessed on 1 June 2023).


{kind=link}
{kind=link}
{kind=link}
| Mean | SD | n | %/Min–Max | |
|---|---|---|---|---|
| Key Predictor Variable | ||||
| Stigma | 0.02 | 0.21 | 456,512 | 0–6 |
| Psychological Distress | 9.52 | 6.06 | 151,683 | 0–24 |
| Lifetime Psychedelic Use | ||||
| MDMA | 32,468 | 7.09 | ||
| Psilocybin | 43,294 | 9.45 | ||
| DMT | 370 | 0.08 | ||
| Ayahuasca | 41 | 0.01 | ||
| Peyote/Mescaline | 19,997 | 4.36 | ||
| LSD | 48,413 | 10.56 | ||
| Lifetime Classic Psychedelic Use | 63,893 | 13.94 | ||
| Control Variables s | ||||
| Missed Prescribed Mental Health Treatment | 23,339 | 5.11 | ||
| Age | 14.82 | 2.06 | 458,372 | 8–17 |
| Education | 2.77 | 1.02 | 458,372 | 1–4 |
| Family Income | 4.97 | 2.02 | 458,372 | 1–7 |
| Women | 237,730 | 51.86 | ||
| Marital Status | ||||
| Single | 120,128 | 26.21 | ||
| Married | 245,431 | 53.54 | ||
| Widowed | 27,879 | 6.08 | ||
| Divorced/Separated | 64,932 | 14.17 | ||
| Race | ||||
| White | 301,989 | 65.88 | ||
| Black | 53,430 | 11.66 | ||
| Native American | 2397 | 0.52 | ||
| Hawaiian | 1635 | 0.36 | ||
| Asian | 23,563 | 5.14 | ||
| Multi-Racial | 6715 | 1.46 | ||
| Hispanic | 68,640 | 14.97 | ||
| Religious Salience | 2.94 | 1.05 | 450,311 | 1–4 |
| Religious Attendance | 1.89 | 1.88 | 454,781 | 0–5 |
| Lifetime Drug Use | ||||
| Cocaine | 75,007 | 16.36 | ||
| Stimulants | 46,617 | 10.17 | ||
| Sedatives | 38,369 | 8.37 | ||
| Tranquilizer | 76,047 | 16.59 | ||
| Inhalants | 40,656 | 8.88 | ||
| Pain Relievers | 165,821 | 36.18 | ||
| Heroine | 9121 | 1.99 | ||
| Marijuana | 213,442 | 46.47 | ||
| PCP | 12,144 | 2.65 | ||
| MDMA/ecstasy | 44,156 | 6.55 | ||
| Tobacco | 264,590 | 57.72 | ||
| Age of First Alcohol Use | 2.87 | 1.15 | 458,372 | 1–5 |
| Self-Reported Risky Behavior | 1.60 | 0.74 | 456,796 | 1–4 |
| Mean | Mean Difference a | |||
|---|---|---|---|---|
| Men | Women | |||
| Stigma | 0.01 | 0.02 | −0.01 | *** |
| (0.000) | (0.005) | (0.000) | ||
| Psychological Distress in Last Month (K6) | 9.31 | 9.65 | −0.33 | *** |
| (0.035) | (0.035) | (0.049) | ||
| Lifetime Psychedelic Use | ||||
| MDMA | 0.08 | 0.05 | 0.02 | *** |
| Psilocybin | 0.13 | 0.06 | 0.06 | *** |
| DMT | 0.01 | 0.00 | 0.01 | *** |
| Ayahuasca | 0.00 | 0.00 | 0.00 | |
| Peyote/Mescaline | 0.06 | 0.02 | 0.03 | *** |
| LSD | 0.13 | 0.07 | 0.06 | *** |
| Classic Psychedelics | 0.18 | 0.10 | 0.08 | *** |
| Annual Household Income | 5.12 | 4.82 | 0.30 | *** |
| (0.008) | (0.009) | (0.008) | ||
| Educational Attainment | 2.75 | 2.79 | −0.04 | *** |
| (0.004) | (0.004) | (0.004) | ||
| Age | 14.76 | 14.88 | −0.11 | *** |
| (0.007) | (0.007) | (0.007) | ||
| Race | ||||
| White | 0.65 | 0.64 | 0.01 | ** |
| Black | 0.11 | 0.13 | −0.01 | *** |
| Native American | 0.01 | 0.01 | 0.00 | |
| Hawaiian/Pacific Islander | 0.00 | 0.00 | 0.00 | |
| Asian | 0.05 | 0.05 | −0.00 | * |
| Hispanic | 0.16 | 0.15 | 0.01 | *** |
| Two or More Race (non-Hispanic) | 0.02 | 0.02 | 0.00 | - |
| Marital Status | ||||
| Single, never Married | 0.28 | 0.26 | 0.05 | *** |
| Married | 0.55 | 0.51 | 0.04 | *** |
| Widowed | 0.03 | 0.08 | −0.05 | *** |
| Divorced/Separated | 0.12 | 0.15 | −0.03 | *** |
| Religious Attendance | 1.68 | 2.08 | −0.40 | *** |
| (0.007) | (0.006) | (0.009) | ||
| Religiosity | 4.64 | 5.20 | −0.56 | *** |
| (0.009) | (0.007) | (0.011) | ||
| Lifetime Drug Use | ||||
| Cocaine | 0.20 | 0.12 | 0.07 | *** |
| Marijuana | 0.51 | 0.41 | 0.10 | *** |
| MDMA/ecstasy | 0.03 | 0.01 | 0.02 | *** |
| PCP | 0.03 | 0.01 | 0.02 | *** |
| Inhalants | 0.12 | 0.05 | 0.06 | *** |
| Stimulants | 0.10 | 0.09 | 0.01 | *** |
| Sedatives | 0.07 | 0.08 | −0.01 | *** |
| Tranquilizer | 0.14 | 0.18 | −0.03 | *** |
| Heroine | 0.02 | 0.01 | 0.01 | *** |
| Pain Relievers | 0.36 | 0.35 | 0.01 | ** |
| Tobacco | 0.72 | 0.44 | 0.27 | *** |
| Age of First Alcohol Use | 2.65 | 3.07 | −0.41 | *** |
| (0.004) | (0.003) | (0.005) | ||
| Self-Reported Risky Behavior | 1.76 | 1.46 | 0.30 | *** |
| (0.002) | (0.002) | (0.003) | ||
| Missed Needed Treatment | 0.03 | 0.06 | −0.03 | *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viña, S.M. Minorities’ Diminished Psychedelic Returns: Gender, Perceived Stigma, and Distress. Psychoactives 2024, 3, 303-317. https://doi.org/10.3390/psychoactives3020019
Viña SM. Minorities’ Diminished Psychedelic Returns: Gender, Perceived Stigma, and Distress. Psychoactives. 2024; 3(2):303-317. https://doi.org/10.3390/psychoactives3020019
Chicago/Turabian StyleViña, Sean Matthew. 2024. "Minorities’ Diminished Psychedelic Returns: Gender, Perceived Stigma, and Distress" Psychoactives 3, no. 2: 303-317. https://doi.org/10.3390/psychoactives3020019
APA StyleViña, S. M. (2024). Minorities’ Diminished Psychedelic Returns: Gender, Perceived Stigma, and Distress. Psychoactives, 3(2), 303-317. https://doi.org/10.3390/psychoactives3020019