1. Introduction
Correctional officers across the nation deal with chronic high stress, long tumultuous shifts, and a constant requirement for high-level anxiety based on the nature of the job. Due to these specific factors, it has been proven that correctional staff suffer higher rates of post-traumatic stress disorder compared to military veterans and suicide rates that are two times as high as all other professions combined [
1,
2]. Despite the limited availability of the data, these have been identified as longstanding problems; for example, research from the 1990s have indicated that suicidal risk among correctional officers was 39% greater than that of the rest of the working age population [
3]. Although suicide may not be the main cause of premature death, there is a plethora of other factors that may exacerbate the decreased life expectancy that they all seem to have in common. Prison communities can be viewed as a visual representation of memory of the past states of our society due to stressful environment, including violence, and the lack of diversity. Many ethnic and minority groups, and specific social groups create self-imposed sub-communities that increase the likelihood for gang affiliations, along with other general issues that increase the difficulty for adequate monitoring and policing inside of these correctional facilities.
According to the U.S. Bureau of Justice Statistics, in 2016, there were 1,204,300 adults incarcerated in U.S. federal and state prisons [
4]. While only comprising 4.4% of the world’s population, the United States accounts for 22% of the world’s prison population. As of 2019, there were roughly 462,000 correctional officers employed in the U.S. [
5]. However, many underserved areas and facilities face a high inmate-to-correctional officer ratio, contributing to work stress among correctional officers.
Another common point of contention with correctional officers regarding their work-related stressors would be aspects of administrative stress. There has been a congruent notion within the correctional workforce population that effective correctional management of prisoners has been blatantly ignored and that current strategies are unsuccessful. As discussed in many studies, a majority of correctional staff believe that the correctional system is unsuccessful due to conflicting goals of inmate rehabilitation, lack of adequate training, and trial-and-error forms of management in correctional facilities that make adequate management almost impossible [
6,
7,
8]. This could directly correlate with the increased levels of stress and lack of job satisfaction as well as high turnover rate; in addition, these issues demand correctional organizations to spend enormous sums annually for sick leave, compensation, and liability claims [
9]. Prior studies have also demonstrated an eight-fold increase in workers’ compensation claims, from
$980,000 to approximately
$8 million over a decade [
10]. Even considering all of these integral factors, it is clear why the life expectancy of a correctional officer is only 59 years compared to the national average of 75 years—a reduction in lifespan by 21.3% [
1].
Many correctional staff face constant physical risk along with varying mental health stressors that also take a toll on their overall health profile. For example, 34% of correctional officers suffer from post-traumatic stress disorder (PTSD) compared to 14% of military veterans. With PTSD affecting only 7% of Americans in the general population, the rate that affects correctional officers across the country is almost five times that of the average citizen and more than twice the rate of military veterans. Moreover, alcoholism and divorce rates are higher for correctional officers than for the population in general, adding to the overall level of stress that correctional officers internalize [
9]. Mental health also has been directly correlated to higher incidence of substance abuse and this has been demonstrated true in the correctional officer population as well.
Although the exact cause of the increased level of stress and substance use is unknown, a culmination of many factors is understood and has been assumed to cause the plethora of health issues that plague the correctional officer community. Stress in correctional officers can manifest in many physical illnesses: hypertension, heart attacks, and ulcers at a higher rate than a compared population of police officers, who often face higher rates of stress-induced physical illness [
9].
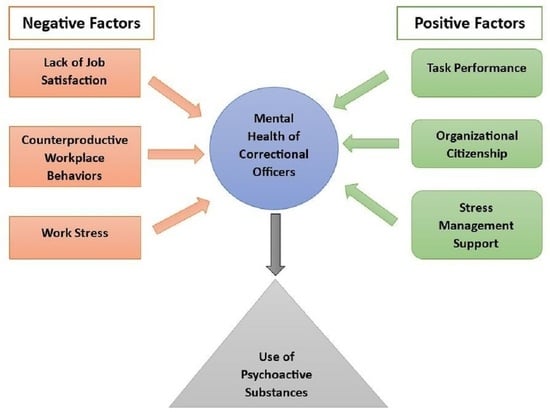
Intricacies of the prison population, crime within incarcerated populations, violence, and unsafe living conditions that are imposed on staff on a daily basis may explain the stress and stress-related health problems among correctional officers. These stipulations have resulted in a secondary cause for increased dependency on psychoactive substances and associated substance abuse due to assumed work-related stressors. The aim was to delve into the nuanced relationships between the challenging work environment, substance use patterns, and the choices correctional officers make regarding stress management support. A comprehensive investigation was conducted to contribute valuable insights into the multifaceted dynamics that impact correctional officers’ well-being and coping mechanisms.
3. Results
In consideration of both phases (
N = 1083), the mean age of correctional officers was 38.60 years (SD = 11.55), 71.38% were male, 62.88% were White, and 16.99% were veterans. The mean stress signs and symptoms was 1.42 (SD = 0.67, higher = better, max = 4) (
Table 1). Furthermore, 70.82% drank alcohol, and 17.15% used sedatives occasionally to help sleep. Of those who answered phase-1 (see limitations), only 5.49% reported that they had used marijuana and only 3.89% reported that they used illegal drugs.
In the initial phase (n = 515) of our study, four key indices, namely stress signs and symptoms, organizational citizenship, task performance, and counterproductive workplace behaviors, underwent rigorous validation. The Kaiser–Meyer–Olkin (KMO) measure demonstrated excellent sampling adequacy for each index (KMO = 0.956, 0.904, 0.893, and 0.882, respectively), substantiating their appropriateness for factor analysis. Barlett’s test for sphericity, yielding p-values < 0.001 across all indices, further confirmed their suitability. Moreover, the internal consistency, assessed through Cronbach’s α, exhibited high reliability for stress signs and symptoms (α = 0.955), organizational citizenship (α = 0.895), task performance (α = 0.787), and counterproductive workplace behaviors (α = 0.854), thereby affirming the robustness of these indices for subsequent analytical procedures. The mean of relevant items in each index was employed for further in-depth analysis.
For phase-1 (
n = 515), all four indices, i.e., stress signs and symptoms, organizational citizenship, task performance, and counterproductive workplace behaviors, were significantly associated with correctional officers’ use of sedative drugs occasionally to help their sleep (
Table 2).
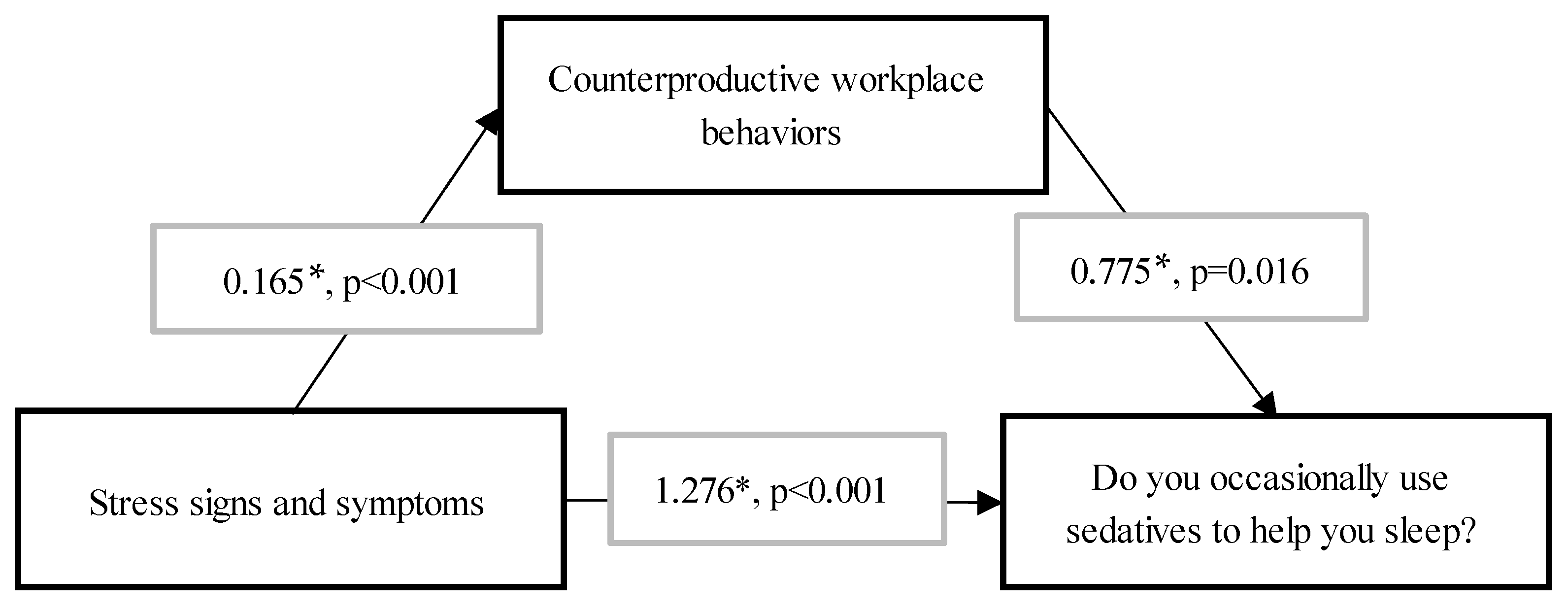
In mediation effect modeling, stress signs and symptoms had a significant direct effect on sedative use (direct effect = 1.28,
p < 0.001), whereas a mediation effect was found through counterproductive workplace behaviors (indirect effect = 0.128,
p < 0.001) (
Figure 1). Marijuana and illegal drugs were excluded from further analysis due to small numbers, whereas alcohol was excluded from mediation effect modeling since the stress signs and symptoms index (i.e., main predictor of interest) was not statistically significantly associated with alcohol use.
In ANOVA of the full sample (i.e., two phases combined), mean stress signs and symptoms (F2,1061 = 6.417, p = 0.002) and mean age (F2,1068 = 4.629, p = 0.010) were significantly associated with the preference for stress management support. Subsequently, a multinomial logistic regression model was performed to determine if any variables, including stress and age, predict the preference for stress support venues as well as the strength and direction of any relationship.
The multinomial logistic regression model considered preferred stress support venues alongside various independent variables (
Table 3). Compared to non-veterans, veterans were significantly less likely to seek stress management support from any service, i.e., from the Department of Corrections (OR = 0.55; 95%CI = 0.31, 0.99) and outside venues (OR = 0.51; 95%CI = 0.29, 0.90). Married officers were 84% more likely than their unmarried counterparts to prefer stress management support from the department (OR = 1.84; 95%CI = 1.10, 3.08). Finally, correctional officer age was positively associated with seeking stress management support from outside venues with one year increase in age predicting a 3% increase in the likelihood of seeking support from outside sources (OR = 1.03; 95%CI = 1.01, 1.06). The model achieved an overall classification accuracy rate of 45.5%.
With the combined data for both phases, the multinomial regression model was considered for the behavioral effect of the correctional officers with various independent variables (
Table 4). For the combined behavioral effect, 29% accounts for prescription drugs used, 5.3% for sedatives used to help sleep, and 12% for the concurrent use of both. The model indicated that individuals who had not experienced the loss or breakup of someone they cared about in the last month were approximately 0.31 times less likely to use sedatives compared to those who had experienced such a loss. For each one-year increase in the age of the correctional officers at the time of the interview, the odds of using prescription drugs increased by approximately 6%, and both the use of prescription drugs and sedatives increased by approximately 10% compared to not using any drugs. The odds of being in the “prescription drug” category were 0.22 times lower for individuals who reported feeling a lot of stress compared to those who did not report feeling a lot of stress. The odds of being in the “both prescription drug and sedatives” category were 0.14 times lower for individuals who reported feeling a lot of stress compared to those who did not report feeling a lot of stress. Individuals who did not encounter a co-worker complaint in the previous year were roughly 4.08 times more inclined to abstain from any drug use, compared to those who reported a co-worker complaint, with prescription drug use as the reference.
4. Discussion
Correctional officers play a crucial role in our criminal justice system as they maintain order within correctional facilities, therefore, ensuring the safety of inmates and staff is pivotal to the continuance of our current infrastructure. However, due to the tedious nature of the job as well as the strenuous job requirements, many officers struggle with stress management and have been found to have severe repercussions [
18]. This study is consistent with previous studies with juvenile correctional officers (
n = 413), which revealed that their work environment was more stressful than that of the normal workforce [
18]. As evidenced by Frost’s research [
19], approximately 25% of correctional officers reported psychological distress symptoms, aligning with the alarming suicide rate among correction officers of the Massachusetts Department of Correction, which was seven times higher than the national average and nearly 12 times higher than the Massachusetts state’s average. Correctional workers, particularly healthcare workers, experienced a high level of psychological symptoms during the COVID-19 pandemic compared to correctional officers, with a significant proportion reporting depressive, anxiety, burnout, and post-traumatic stress symptoms, along with sleep disturbance; however, despite the mental health burden, correctional workers demonstrated high resilience [
20]. Occasional sedative use was found to be a significant problem associated with work stress. However, there is a significant difference in gender for occasional sedative use, where 21.4% of females used occasional sedatives while males were 15.4%. Prior studies have outlined patterns of multiple and substitute addictions in various populations for different reasons [
21], so future studies should include methods and questions to investigate these patterns among correctional officers. After being asked specific questions about their overall need for stress management help in this study, approximately 27.17% answered that they do not need any support, highlighting the need for interventions for raising awareness of stress management, including its importance, evidence-based techniques, available services, and new resources available online [
22]. A higher percentage of females (76.03%) were looking for stress management help either inside or outside of the department compared to males (71.55%).
Four key indices, namely stress signs and symptoms, organizational citizenship, task performance, and counterproductive workplace behaviors, were developed and evaluated in this study. These indices were meticulously constructed by combining and assessing item blocks from the original dataset to represent specific domains relevant to correctional officers’ professional performance and well-being. The stress signs and symptoms index, measured on a scale ranging from 0 to 4, aimed to evaluate the officers’ stress manifestations, where higher scores indicated better adaptation and coping mechanisms. Similarly, the organizational citizenship index, on a scale from 0 to 5, gauged the officers’ commitment and dedication to their workplace, with higher scores reflecting increased engagement and support. The task performance index, also measured on a 0 to 5 scale, indicated the quality and efficiency of the officers’ task execution. Likewise, the counterproductive workplace behaviors index, scored from 0 to 5, assessed the workplace. Results from the phase-1 analysis revealed a significant association between all four indices and the occasional use of sedative drugs by correctional officers to aid sleep. Specifically, higher scores in stress signs and symptoms, counterproductive workplace behaviors, and lower scores in organizational citizenship and task performance were associated with increased sedative use.
Chronic stressors among correctional officers are based on a unique set of tasks that are required in their daily duties [
23]. Within these daily stressors, come the recurrent desire from many correctional officers to self-medicate or reduce their overall stress levels. After being asked about other fellow correctional officers’ current baseline stress level, only 12.40% answered not at all, 56.69% answered somewhat concerned, and 30.91% answered very concerned. Exposures to violence, threats from inmates, long working hours, understaffing, and limited opportunities for emotional/mental support outside of the state-funded support systems [
24] all can justify this level of perceived stress among coworkers in the workforce, but also further support the desperate need for implemented improvements and change. Chronic stress is directly correlated with psychological well-being, but also takes a drastic toll on physical health and mental stability. This may partially explain the findings from the 1981 assessment by the American Federation of State, County, and Municipal Employees [
23], which showed that correctional officers’ life expectancy was 59 years, compared to the population average of 75 years. In this study, the sample population regarding correctional officers had an average age being 39 years old, with a minimum age of 19 and a maximum age of 72. Regarding gender, previous studies found that White females reported the highest stress levels [
25], although such an association was not found in this study. This is also supported by an alternate finding from previous studies, which reported that female correction officers are more likely to be divorced and to use social support as a means of dealing with work-related stress [
26]. Furthermore, women in the correctional workforce have also been reported to have more day-to-day interactions of attempted manipulation, and attempts of sexual harassment from inmates [
27], along with sexist behavior from male officers and other coworkers [
28].
Approximately 72% of the correctional workforce receives assistance with stress management and still are more likely to use narcotic substances or alcohol. High stress levels were previously associated with lower job satisfaction [
29,
30] and increased levels of job-related stress were directly correlated with a range of negative outcomes including poor health, decreased job efficiency, and increased employee turnover [
18].
While this study has indicated that correctional officers are at a heightened risk of specific substance use, specifically sedatives, according to our knowledge, empirical evidence on this topic is either absent or limited. Approximately 17% of correctional officers in this study reported that they use sedatives occasionally to help with sleep problems. Commonly used sedative drugs, including barbiturates, benzodiazepines, opioids, and sleep-inducing drugs, are used regularly when individuals struggle with sleep due to insomnia, night terrors, and PTSD. The chemical dependency arising from the long-term use of these prescription medications can cause serious side effects despite the temporary relief they provide. They also can have latency effects that may take away the officers’ ability to perform their job consistently and efficiently. Stress management programs within correctional institutions are aimed at equipping officers with healthier coping strategies [
22] and ensuring that management techniques will decrease the overall dependency on the identified prescription drugs. This could have a plethora of issues for the concurrent management and retention of correctional officers in the workforce.
Marijuana, although legalized in many states throughout the United States is still federally illegal and has been banned in most correction institutions per federal regulations [
31]. Many correctional officers still admit to using marijuana on a regular basis even with the concern for possible judgment bias regarding their personal use possibly causing administration issues due to federal regulations banning recreational marijuana use. Of the correctional officers questioned in the study, over 5% of officers admitted to using marijuana on a regular basis, although such self-reported data often underestimate the actual prevalence. Coping using illegal substances such as marijuana may not be as physiologically dangerous as prescription pills, but can still pose dependency issues and cause limitations on the correctional officer’s ability to maintain a correct code of conduct based on their job requirements.
Alcohol abuse is also an often-discussed issue that disproportionately affects certain groups within American society. Broadly, 1 in 8 men and 1 in 10 women meet the diagnostic criteria for alcohol use disorder (AUD), which is more than 10% of the adult population in the U.S.A. [
32]. When asked if they drink alcohol, over 70% of correctional officers admitted to using alcohol. Most people with AUD have developed their dependency on alcohol due to habits formed from inadequate coping mechanisms to deal with stress. Alcohol dependency, although it may not be specifically what was asked in this study, is also more likely to form when recurrent habits and routines such as drinking to destress are repeated for at least three months. Without knowing the frequency at which they use alcohol, one should assume that the majority (53%) of Americans admit that they drink from one to seven drinks per week [
33]. One concern with management should be the inability of correctional officers to function if they do become dependent on alcohol use as it has many rebound effects and may inhibit their functioning from a healthy perspective.
A major issue regarding correction officers is the lack of assistance they have for stress management and options available for developing healthy coping mechanisms, compared to care-seeking behaviors among other populations [
24]. It is reasonable to assume that many officers can receive help through their facility [
34], but one can assume that they are unlikely to respond to treatment options completely and transparently from their employer due to their fear of grudges. One-third (66%) of correctional officers answered that they would seek services or assistance from outside of the department, potentially indicating that they feel uncomfortable getting assistance from their department.
Multiple factors can result in substance abuse, but chronic stressors, lack of adequate stress relief mechanisms and management support, and reduced accessibility to therapy and relief outside of the facility may exacerbate the desire to use substances in an attempt to cope to reduce stress levels. Suggested methods per administration in previous cases include redefining clear guidelines for job performance, support systems, the incorporation of mutual input for decision making, bilateral improvements in communication between employees and management, interdependence, and improving organizational guidelines [
23]. Specific concepts regarding management improvements and options that could reduce the overall stressors could work to reduce substance or alcohol use and dependency within the workforce. A prior analysis of the correctional officer data substantiated through this finding revealed the role of ambiguity, lack of administration support, and lack of input into decision making were primary causes of correctional officer stress [
23]. Reduction in life expectancy within the workforce could also be attributed to drug and alcohol use along with chronic stress that ensues within the work population. Reducing the levels of chronic stressors and drug dependency habits should be a major goal from the management perspective to hopefully enhance the lifestyle dynamic of the workforce.
In the amalgamated data from both research phases, our investigation sought to discern shared behavioral impacts on correctional officers. By merging two questions pertaining to behavioral effects, we aimed to unveil overarching patterns in drug use among correctional officers. The multinomial regression models provided insightful perspectives on how various independent variables influenced drug use patterns. Notably, individuals who had not experienced recent personal losses were found to be less likely (0.31 times) to use sedatives, emphasizing the potential role of emotional well-being in substance use choices. Age emerged as a significant factor, with each additional year correlating with a 6% increase in the odds of using prescription drugs and a 10% increase for those using both prescription drugs and sedatives. Stress levels also played a role, as individuals reporting high stress were 0.22 times less likely to be in the “prescription drug” category and 0.14 times less likely to be in the “both prescription drug and sedatives” category. Intriguingly, correctional officers not reporting co-worker complaints in the previous year were approximately 4.08 times more inclined to abstain from drug use, providing insights into the potential impact of workplace dynamics on substance use behaviors. These findings underscore the complex interplay of personal and occupational factors in shaping the substance use patterns of correctional officers, with implications for both workplace interventions and broader policy considerations.
Correctional officers confront a myriad of stressors inherent to their challenging profession, evidenced by heightened anxiety, insomnia, and other manifestations. The correctional environment’s nature, marked by high-risk situations and interpersonal conflicts, significantly contributes to stress levels. Recognizing and addressing these stress signs is pivotal for officers’ well-being and the overall functionality of correctional facilities. The literature underscores the importance of organizational citizenship behaviors in correctional settings, involving discretionary efforts beyond formal job requirements [
35]. Fostering a culture that encourages and rewards organizational citizenship behaviors is associated with increased job satisfaction and organizational effectiveness. Additionally, task performance’s critical role is highlighted, closely linked to factors such as training and resource availability. Inadequate training or staffing levels can hinder task performance, impacting efficiency and safety. When individuals grapple with the strain of conflicting roles, it often leads to frustration [
36]. Consequently, they may exhibit behaviors that are hostile, aggressive, inappropriate, or counterproductive. Understanding and addressing the root causes of counterproductive workplace behaviors is crucial for promoting a positive workplace culture and maintaining correctional institutions’ effectiveness.
The findings of this study illuminate the intricate relationship between correctional officers’ substance use behaviors and critical workplace indexes, as aligned with the existing literature. As anticipated, correctional officers face substantial stressors inherent in their demanding profession, manifested through heightened anxiety, insomnia, and other stress-related symptoms. The correctional environment’s nature, marked by high-risk situations and potential violence, significantly contributes to elevated stress levels among officers. Recognizing and addressing these stress indicators is paramount for both individual well-being and the overall operational efficacy of correctional facilities. Moreover, the study underscores the pivotal role of organizational citizenship behaviors in promoting a cooperative work environment among correctional officers. While the consumption of alcohol and the occasional use of sedatives exhibit nuanced effects on stress signs, organizational citizenship, and task performance, both substances are associated with an increase in counterproductive workplace behaviors, posing a potential threat to the integrity of correctional institutions. Importantly, marijuana use is linked to higher stress levels and lower organizational citizenship scores, suggesting a need for targeted interventions to mitigate these impacts. Similarly, the study reveals a substantial increase in counterproductive workplace behaviors among officers engaged in illegal drug use, emphasizing the concerning association between substance use and workplace misconduct. These findings collectively emphasize the complexity of substance use behaviors in correctional settings, prompting a critical examination of preventive measures and intervention strategies to foster a positive work culture and uphold the effectiveness of correctional institutions.
This study had several strengths. First, the sample size was large even though correctional officers are generally considered a hard-to-reach population. Second, the original survey utilized random sampling methods; therefore, the sample was representative of Massachusetts and Texas, increasing the generalizability of the findings to the correctional officer population in the U.S. overall. Third, the response rate was much higher than that reported in prior surveys conducted among other professional populations [
37]. Finally, the phase-1 questionnaire comprehensively addressed many aspects of the correctional officer work environment, and the generated indices included all variables.
This study also had a few limitations. First, causal interpretations cannot be made from this analysis because the original survey was cross-sectional. Second, the questionnaire administered in phase-2 lacked variables related to some indices (i.e., task performance, organizational citizenship, and counterproductive workplace behaviors) and substance use behaviors (i.e., marijuana and illegal drugs); therefore, corresponding analyses were based on phase-1 data only. Third, sedatives are typically considered a subset of prescription drugs; however, 31% of sedative users said that they are not using any prescription drug for any reason, which is not accurate. This discrepancy could have been prevented by properly wording the question on prescription drugs (i.e., prescription drugs other than sedatives). Finally, prisons were selected based on convenience sampling (distance between the research site and prison), limiting the generalizability of findings, although officers within prisons were sampled randomly.






{kind=link}
{kind=link}