

Incobotulinumtoxin A and Yoga-like Isometric Exercise in Adolescent Idiopathic Lumbar Scoliosis—A Randomized Pilot Study


Abstract
1. Introduction
2. Results
3. Design
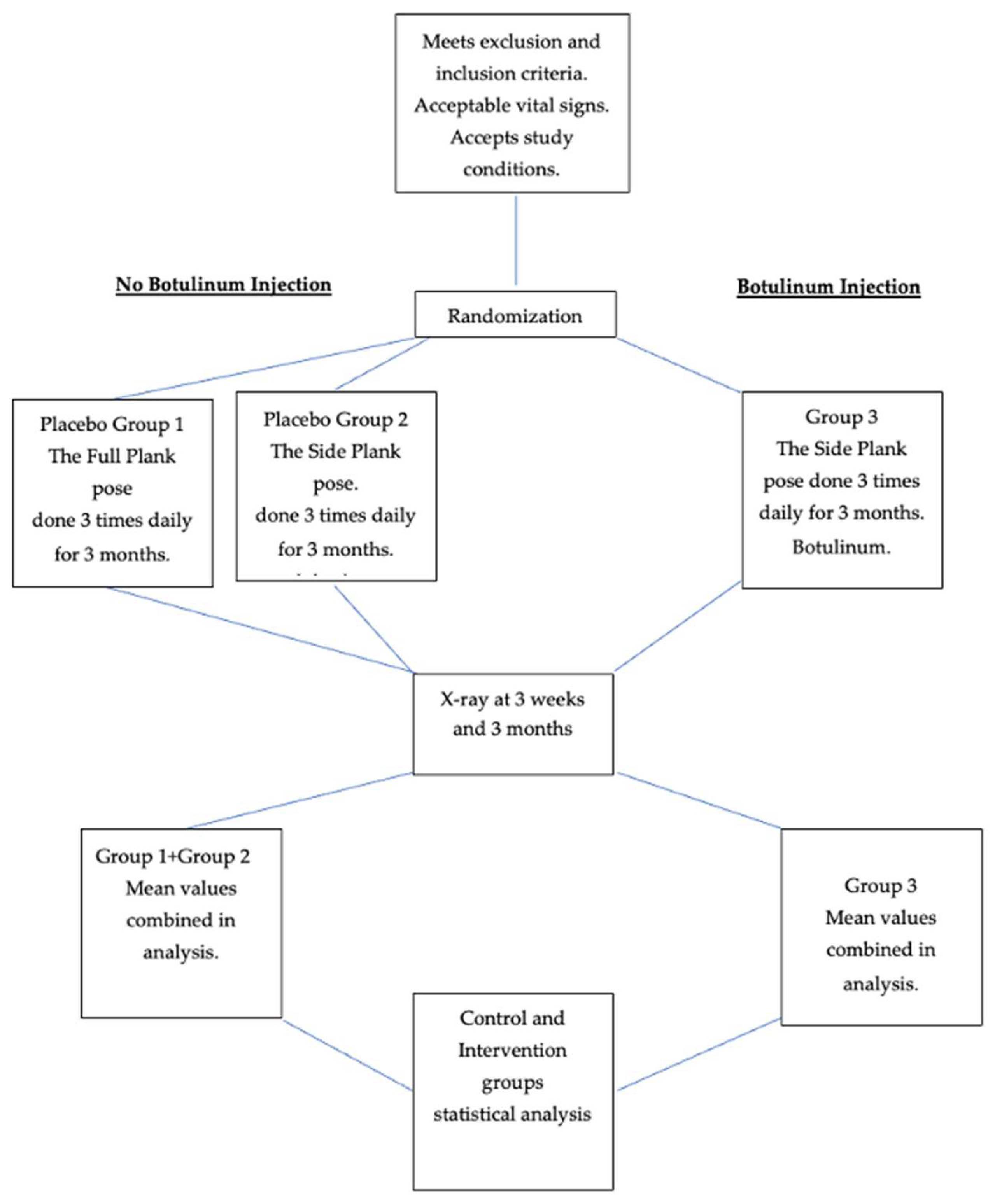
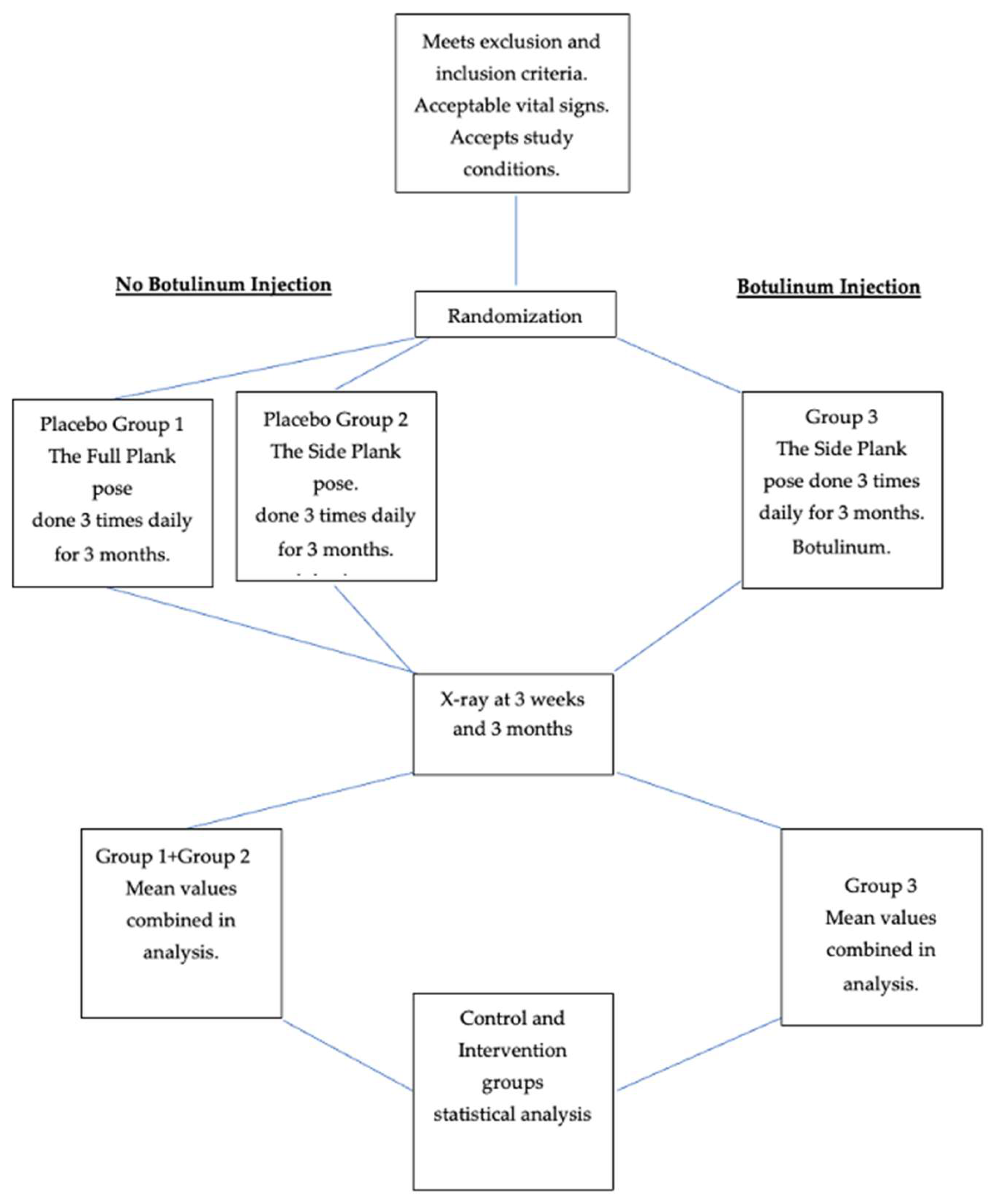
3.1. Eligibility
3.1.1. Inclusion Criteria
- Age 12–18 years.
- Lumbar or thoracolumbar curve of 25 degrees or more.
- Willingness to perform one yoga pose for as long as possible three times daily for three months.
- Parental or guardian agreement.
3.1.2. Exclusion Criteria
- Neuromuscular or musculoskeletal disease, e.g., cerebral palsy, Guillain–Barre syndrome, Marfan’s syndrome.
- Current use of brace.
- Previous spinal surgery.
- Previous exposure to botulinum toxin type A.
- Positive pregnancy test.
3.1.3. Particulars of the Study
4. Discussion
- (1)
- (2)
- The botulinum weakens the strong (concave) side of the lumbar curve, enabling the actin and myosin fibers of the weak (convex) side to slide further together, increasing the number of cross bridges, and proportionately increasing their power to contract [40], in addition to the continual strengthening the yoga pose provides during the latter part of the three-month period. These considerations must be viewed as hypotheses at this point, needing further confirmation or contradiction.
- (3)
5. Limitations of the Study
- (1)
- Although it reached statistical significance, this randomized controlled study is based on a small sample. Larger, randomized controlled trials are clearly necessary to demonstrate the efficacy of the botulinum-plus-yoga treatment more reliably.
- (2)
- A single blinded radiological opinion was utilized throughout this study. A second and even a third blinded radiologist (for non-unanimous assessments) would improve the objectivity in these studies.
- (3)
- The opposite limitation is also present: the ranges of the patients’ Risser numbers, ages and curve sizes are too large. Some researchers find that a combination of bracing and exercise is differentially effective in AIS at different Risser numbers and this type of variability may apply to botulinum as well [4,5,6].
- (4)
- Studies have found that bracing plus exercise substantially improve curves in AIS [41]. Studies using bracing and exercise, including the side plank and botulinum toxin injections, might further advance and enhance conservative treatment.
- (5)
- Further study design can also raise the level of objectivity regarding harms, e.g., by measuring activities of daily living [42]. More specific considerations mentioned by leaders in the field may also be relevant, including aesthetics, quality of life, disability, back pain, psychological well-being, self-esteem, body image and embarrassment in high school [13,14].
- (6)
- Longer follow-up is also necessary to demonstrate the value of the treatment. Two- or three-year follow-up or more would be desirable.
- (7)
- This study injected the minimal effective doses of botulinum. Dosages up to 1.67 times greater are patently safe [43]. It is possible that a proportionately greater effect would be seen with larger doses of incobotulinum. This study does not answer that important question.
- (8)
- One may additionally ask about whether the most relevant muscles have been treated. The iliocostalis, longissimus, semispinalis and spinalis muscles, as well as the external and internal intercostals and obliques, the superior and inferior serratus posterior, the subcostal, the quadratus lumborum, the latissimus dorsi and trapezius, the transversus abdominis, the rectus abdominis and the diaphragm itself might all function to laterally flex and/or rotate the spine. These muscles should be studied, both with different yoga poses and other types of exertion vis à vis strengthening them, and for appropriate dosages of botulinum toxin for weaking their contralateral counterparts.
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, S.; Chae, H.W.; Lee, H.S.; Kim, S.; Kwon, J.-W.; Lee, S.-B.; Moon, S.-H.; Lee, H.-M.; Lee, B.H. Incidence and Surgery Rate of Idiopathic Scoliosis: A Nationwide Database Study. Int. J. Environ. Res. Public Health 2021, 18, 8152. [Google Scholar] [CrossRef] [PubMed]
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idio pathic scoliosis. J. Child. Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Longworth, B.; Fary, R.; Hopper, D. Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers. Arch. Phys. Med. Rehabil. 2014, 95, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.-K.; Tan, J. The natural history of adolescent idiopathic scoliosis. Indian J. Orthop. 2010, 44, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ragborg, L. Long term curve progression in idiopathic scoliosis: 40-year follow-up. In Proceedings of the Scoliosis Research Society (SRS) 57th Annual Meeting, Stockholm, Sweden, 14–17 September 2022. [Google Scholar]
- Stirling, A.J.; Howel, D.; Millner, P.A.; Sadiq, S.; Sharples, D.; Dickson, R.A. Late-onset idiopathic scoliosis in children six to fourteen years old: A cross-sectional prevalence study. J. Bone Joint Surg. Am. 1996, 78, 1330–1342. [Google Scholar] [CrossRef] [PubMed]
- Nachemson, A.L.; Peterson, L.E. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis: A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J. Bone Joint Surg. Am. 1995, 77, 815–882. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.D.; Villagrasa, M.; Gallo, D. A specific scoliosis classification correlating with brace treatment: Description and reliability. Scoliosis 2010, 5, 1. [Google Scholar] [CrossRef]
- Coillard, C.; Circo, A.B.; Rivard, C.H. A prospective randomized controlled trial of the natural history of idiopathic scoliosis versus treatment with the SpineCor brace. Sosort Award 2011 winner. Eur. J. Phys. Rehabil. Med. 2014, 50, 479–487. [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef]
- Aulisa, A.G.; Guzzanti, V.; Falciglia, F.; Giordano, M.; Marzetti, E.; Aulisa, L. Lyon bracing in adolescent females with thoracic idiopathic scoliosis: A prospective study based on SRS and SOSORT criteria. BMC Musculoskelet. Disord. 2015, 16, 316. [Google Scholar] [CrossRef]
- Negrini, S.; Marchini, G. Efficacy of the symmetric, patient-oriented, rigid, three-dimensional, active (SPoRT) concept of bracing for scoliosis: A prospective study of the Sforzesco versus Lyon brace. Eura Medicophys. 2007, 43, 171–184. [Google Scholar]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; De Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Schwieger, T.; Campo, S.; Weinstein, S.L.; Dolan, L.A.; Ashida, S.; Steuber, K.R. Body Image and Quality-of-Life in Untreated Versus Brace-Treated Females With Adolescent Idiopathic Scoliosis. Spine 2016, 41, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Sun, Y.; Guo, X.; Cao, J.; Lu, H.; Chen, W.; Chen, J.; Zhu, Q.; Zhang, C.; Zhang, M.; et al. The efficacy of 3D personalized insoles in moderate adolescent idiopathic scoliosis: A randomized controlled trial. BMC Musculoskelet. Disord. 2022, 23, 983. [Google Scholar] [CrossRef] [PubMed]
- Yagci, G.; Yakut, Y. Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment. Prosthet. Orthot. Int. 2019, 43, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Parent, E.C.; Hedden, D.M.; Moreau, M.; Hill, D.; Lou, E. Effect of Schroth exercises on curve characteristics and clinical outcomes in adolescent idiopathic scoliosis: Protocol for a multicentre randomised controlled trial. J. Physiother. 2014, 60, 234. [Google Scholar] [CrossRef]
- Tian, G.; Shen, M.R.; Jiang, W.G.; Xie, F.R.; Wei, W.W. Case-control study on spinal leveraging manipulation and medicine for the treatment of degenerative scoliosis. Zhongguo Gu Shang 2015, 28, 508–511. [Google Scholar] [PubMed]
- Kocaman, H.; Bek, N.; Kaya, M.H.; Büyükturan, B.; Yetiş, M.; Büyükturan, Ö. The effectiveness of two different exercise approaches in adolescent idiopathic scoliosis: A single-blind, randomized-controlled trial. PLoS ONE 2021, 16, e0249492. [Google Scholar] [CrossRef]
- Seki, S.; Iwasaki, M.; Makino, H.; Yahara, Y.; Kondo, M.; Kamei, K.; Futakawa, H.; Nogami, M.; Watanabe, K.; Tran Canh Tung, N.; et al. Association of Ligamentum Flavum Hypertrophy with Adolescent Idiopathic Scoliosis Progression—Comparative Microarray Gene Expression Analysis. Int. J. Mol. Sci. 2022, 23, 5038. [Google Scholar] [CrossRef]
- Lin, M.-R.; Chou, P.-H.; Huang, K.-J.; Ting, J.; Liu, C.-Y.; Chou, W.-H.; Lin, G.-H.; Chang, J.-G.; Ikegawa, S.; Wang, S.-T.; et al. Whole-Exome Sequencing Identifies Genetic Variants for Severe Adolescent Idiopathic Scoliosis in a Taiwanese Population. J. Pers. Med. 2023, 13, 32. [Google Scholar] [CrossRef]
- Cortés-Pérez, I.; Salamanca-Montilla, L.; Gámiz-Bermúdez, F.; Obrero-Gaitán, E.; Ibáñez-Vera, A.J.; Lomas-Vega, R. Vestibular Morphological Alterations in Adolescent Idiopathic Scoliosis: A Systematic Review of Observational Studies. Children 2023, 10, 35. [Google Scholar] [CrossRef]
- Montemurro, N.; Ricciardi, L.; Scerrati, A.; Ippolito, G.; Lofrese, G.; Trungu, S.; Stoccoro, A. The Potential Role of Dysregulated miRNAs in Adolescent Idiopathic Scoliosis and 22q11.2 Deletion Syndrome. J. Pers. Med. 2022, 12, 1925. [Google Scholar] [CrossRef] [PubMed]
- Seleviciene, V.; Cesnaviciute, A.; Strukcinskiene, B.; Marcinowicz, L.; Strazdiene, N.; Genowska, A. Physiotherapeutic Scoliosis-Specific Exercise Methodologies Used for Conservative Treatment of Adolescent Idiopathic Scoliosis, and Their Effectiveness: An Extended Literature Review of Current Research and Practice. Int. J. Environ. Res. Public Health 2022, 19, 9240. [Google Scholar] [CrossRef] [PubMed]
- Hausmann, O.N.; Böni, T.; Pfirrmann, C.W.; Curt, A.; Min, K. Preoperative radiological and electrophysiological evaluation in 100 adolescent idiopathic scoliosis patients. Eur. Spine J. 2003, 12, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Skibinska, I.; Tomaszewski, M.; Andrusiewicz, M.; Urbaniak, P.; Czarnecka-Klos, R.; Shadi, M.; Kotwicki, T.; Kotwicka, M. Expression of Estrogen Receptor Coactivator Proline-, Glutamic Acid- and Leucine-Rich Protein 1 within Paraspinal Muscles in Adolescents with Idiopathic Scoliosis. PLoS ONE 2016, 11, e0152286. [Google Scholar] [CrossRef] [PubMed]
- Fishman, L.M.; Groessl, E.J.; Sherman, K.J. Serial case reporting yoga for idiopathic and degenerative scoliosis. Glob. Adv. Health Med. 2014, 3, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Fishman, L.M.; Groessl, E.J.; Bernstein, P. Two Isometric Yoga Poses Reduce the Curves in Degenerative and Adolescent Idiopathic Scoliosis. Top. Geriatr. Rehabil. 2017, 33, 231–237. [Google Scholar] [CrossRef]
- Zang, J.; Li, L. Analysis of Treatments of Adolescent Idiopathic Scoliosis. In Proceedings of the 2021 4th International Conference on Humanities Education and Social Sciences (ICHESS 2021), Xishuangbanna, China, 29–31 October 2021; Advances in Social Science, Education and Humanities Research. Springer Nature: Berlin/Heidelberg, Germany, 2021; Volume 615. [Google Scholar]
- Sarkisova, N.; Andras, L.M.; Yang, J.; Zaslow, T.L.; Edison, B.R.; Tolo, V.T.; Skaggs, D.L. Side Plank Pose Exercises for Adolescent Idiopathic Scoliosis Patients. Glob. Adv. Health Med. 2019, 8, 2164956119887720. [Google Scholar] [CrossRef]
- Fishman, L.M. Side Plank Pose Exercises for Adolescent Idiopathic Scoliosis Patients-Some Concerns about a Randomized Controlled Trial. Glob. Adv. Health Med. 2021, 10, 21649561211019372. [Google Scholar] [CrossRef]
- Junqueira, D.R.; Zorzela, L.; Golder, S.; Loke, Y.; Gagnier, J.J.; Julious, S.A.; Li, T.; Mayo-Wilson, E.; Pham, B.; Phillips, R.; et al. CONSORT Harms 2022 statement, explanation, and elaboration: Updated guideline for the reporting of harms in randomised trials. BMJ 2023, 381, e073725. [Google Scholar] [CrossRef]
- Dysport ® as an Adjunctive Treatment to Bracing in the Management of Adolescent Idiopathic Scoliosis. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT03935295 (accessed on 20 September 2023).
- Fuller, B. Nine Chains to the Moon; Dover: New York, NY, USA, 2020; Available online: http://www.rwgrayprojects.com/rbfnotes/fpapers/tensegrity/tenseg01.html (accessed on 20 September 2023).
- Kim, Y.J.; Lim, O.K.; Choi, W.J. Are There Differences Between Intradermal and Intramuscular Injections of Botulinum Toxin on the Forehead? Dermatol. Surg. 2020, 46, e126–e131. [Google Scholar] [CrossRef] [PubMed]
- Sitnikova, V.; Kämppi, A.; Teronen, O.; Kemppainen, P. Effect of Botulinum Toxin Injection on EMG Activity and Bite Force in Masticatory Muscle Disorder: A Randomized Clinical Trial. Toxins 2022, 14, 545. [Google Scholar] [CrossRef] [PubMed]
- Mitsikostas, D.D.; Dekundy, A.; Hanschmann, A.; Althaus, M.; Scheschonka, A.; Pagan, F.; Jankovic, J. Duration and onset of effect of incobotulinumtoxinA for the treatment of blepharospasm in botulinum toxin-naïve subjects. Curr. Med. Res. Opin. 2021, 37, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.C.; Hsieh, L.F.; Chi, W.C.; Lou, S.M. Effect of intramuscular botulinum toxin injection on upper limb spasticity in stroke patients. Am. J. Phys. Med. Rehabil. 2002, 81, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Hexsel, D.; Valente-Bezerra, I.; Mosena, G.; Oakim Mourao, M.A.; Fabris, V.C. Subjective and Objective Measurements of the Facial Effects of Microdoses of Botulinum Toxin. Dermatol. Pract. Concept. 2023, 13, e2023168. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, R.J.; Gai, C.M.; Aguilar, D.; Bove, D.; Dolan, J.; Vargas, A.; Couvillion, K.; Jenkins, N.D.; Campbell, B.I. Training Volume, Not Frequency, Indicative of Maximal Strength Adaptations to Resistance Training. J. Strength Cond. Res. 2018, 32, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- da Silveira, G.E.; Andrade, R.M.; Guilhermino, G.G.; Schmidt, A.V.; Neves, L.M.; Ribeiro, A.P. The Effects of Short- and Long-Term Spinal Brace Use with and without Exercise on Spine, Balance, and Gait in Adolescents with Idiopathic Scoliosis. Medicina 2022, 58, 1024. [Google Scholar] [CrossRef]
- A Critical Review of Scales of Activities of Daily Living. Available online: https://database.cosmin.nl/catalog/234 (accessed on 21 September 2023).
- Fishman, L.M.; Schmidhofer, S.B. Botulinum toxin in the treatment of piriformis syndrome. In Manual of Botulinum Toxin Therapy, 3rd ed.; Truong, D., Dressler, D., Hallett, M., Zachary, C., Pathak, M., Eds.; Cambridge University Press: Cambridge, UK, 2023; Chapter 30; pp. 259–268. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Group | # | M * | Age (SD) | Weight (SD) | Risser # | T1 | T2 | T3 |
|---|---|---|---|---|---|---|---|---|
| Group 1 | 6 | 1 | 16.8 (1.3) | 123.6 (18.25) | 3.25 (1.26) | 35.75 (17.25) | 37 (15.32) | 37.5 (13.89) |
| Group 2 | 5 | 0 | 14.7 (2.1) | 116 (15.92) | 3.7 (1.27) | 38 (13.04) | 33.40 (11.46) | 33.40 (12.16) |
| Group 3 | 13 | 4 | 15.9 (1.75) | 123.85 (11.95) | 3.6 (0.96) | 41.9 (16.2) | 33.15 (13.95) | 29.46 (12.59) |
| Group 1 + 2 | 11 | 1 | 15.3 (2.2) | 121.4 (25.1) | 3.4 (1.24) | 37.91 (12.78) | 35.73 (11.38) | 35.82 (11.12) |
| Group | T1 | T2 | T2-T1 | T3 | T3-T2 | T3-T1 |
|---|---|---|---|---|---|---|
| 1 | 35.75 (17.25) | 37 (15.34) | 1.25 | 37.5 (13.89) | 0.5 | 1.75 |
| 2 | 35.25 (13.28) | 33.40 (12.46) | 7.25 | 33.16 | 0 | −4.6 |
| 1 + 2 | 37.92 (12.78) | 35.73 (11.38) | −2.19 | 35.88 (11.12) | 0.15 | −2.4 |
| 3 | 41.85 (16.20) | 33.15 (13.95) | −8.7 | 29.46 (12.59) | −3.69 | −12.39 |
| Mean values | ||||||
| ( ) = Standard deviation |
| Groups | Delta | t-Value | p | df | Confid Levels | S.E. |
|---|---|---|---|---|---|---|
| Groups 1 vs. 2 | ||||||
| T2-T1 | −5.9 | 2.0114 | 0.0971 | 8 | −0.77 to 11.27 | 2.61 |
| T3-T1 | 1.75 | 0.4093 | 0.6867 | 16 | −8.75 to 12.73 | 5.108 |
| T3-T2 | 0.5 | 0.1832 | 0.8607 | 6 | −28.71 to24.71 | 10.92 |
| Groups 1 vs. 3 | ||||||
| T2-T1 | −6.35 | 3.865 | 0.0015 | 15 | 6.56 to 22.71 | 3.786 |
| T3-T1 | −10 | 4.4055 | 0.0005 | 15 | 5.91 to 16.98 | 2.597 |
| T3-T2 | −4.2 | 1.2178 | 0.2421 | 16 | −3.15 to 11.53 | 3.443 |
| Groups 2 vs. 3 | ||||||
| T2-T1 | −5.9 | 2.0147 | 0.0611 | 16 | −0.271 to 10.66 | 2.577 |
| T3-T1 | −7.76 | 2.2827 | 0.0365 | 16 | −0.54 to 14.63 | 3.323 |
| T3-T2 | −3.7 | 1.2178 | 0.2421 | 15 | −3.15 to 11.53 | 3.443 |
| Groups 1 + 2 vs. 3 | ||||||
| T2-T1 | −6.5 | 3.3096 | 0.0031 | 23 | −10.31 to −2.38 | 2.039 |
| T3-T1 | −10.4 | 4.4393 | 0.0002 | 23 | −8.57 to 12.75 | 2.358 |
| T3-T2 | −3.85 | 2.2057 | 0.0382 | 22 | 0.24 to 7.94 | 1.855 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fishman, L. Incobotulinumtoxin A and Yoga-like Isometric Exercise in Adolescent Idiopathic Lumbar Scoliosis—A Randomized Pilot Study. Muscles 2024, 3, 28-39. https://doi.org/10.3390/muscles3010004
Fishman L. Incobotulinumtoxin A and Yoga-like Isometric Exercise in Adolescent Idiopathic Lumbar Scoliosis—A Randomized Pilot Study. Muscles. 2024; 3(1):28-39. https://doi.org/10.3390/muscles3010004
Chicago/Turabian StyleFishman, Loren. 2024. "Incobotulinumtoxin A and Yoga-like Isometric Exercise in Adolescent Idiopathic Lumbar Scoliosis—A Randomized Pilot Study" Muscles 3, no. 1: 28-39. https://doi.org/10.3390/muscles3010004
APA StyleFishman, L. (2024). Incobotulinumtoxin A and Yoga-like Isometric Exercise in Adolescent Idiopathic Lumbar Scoliosis—A Randomized Pilot Study. Muscles, 3(1), 28-39. https://doi.org/10.3390/muscles3010004