
Creatine Supplementation Improves Muscular Performance without Additional Impact on the Cardiovascular System in Trained Women

 ,
, 
Abstract
1. Introduction
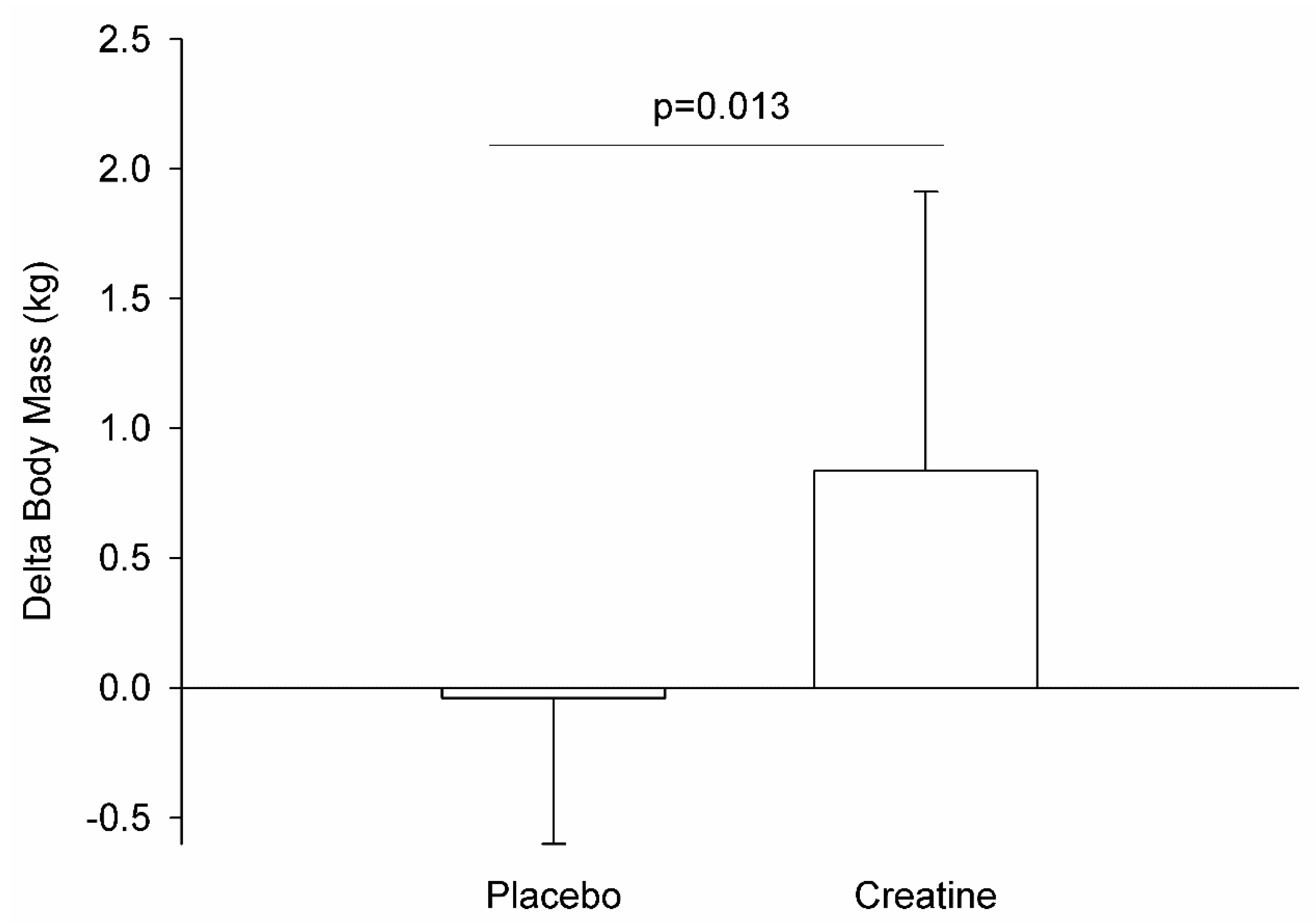
2. Results
3. Discussion
4. Materials and Methods
4.1. Experimental Approach to the Problem
4.2. Subjects
4.3. Procedures
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Machek, S.B.; Bagley, J.R. Creatine Monohydrate Supplementation. Strength Cond. J. 2018, 40, 82–93. Available online: http://journals.lww.com/00126548-201804000-00007 (accessed on 4 November 2020). [CrossRef]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Wallimann, T.; Tokarska-Schlattner, M.; Schlattner, U. The creatine kinase system and pleiotropic effects of creatine. Amino Acids 2011, 40, 1271–1296. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21448658 (accessed on 14 May 2022). [CrossRef] [PubMed]
- Branch, J.D. Effect of creatine supplementation on body composition and performance: A meta-analysis. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 198–226. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12945830 (accessed on 14 May 2022). [CrossRef] [PubMed]
- Dickinson, H.; Bain, E.; Wilkinson, D.; Middleton, P.; Crowther, C.A.; Walker, D.W. Creatine for women in pregnancy for neuroprotection of the fetus. Cochrane Database Syst. Rev. 2014, 19, CD010846. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25523279 (accessed on 14 May 2022). [CrossRef]
- Dickinson, J.M.; D’Lugos, A.C.; Naymik, M.A.; Siniard, A.L.; Wolfe, A.J.; Curtis, D.R. Transcriptome response of human skeletal muscle to divergent exercise stimuli. J. Appl. Physiol. 2018, 124, 1529–1540. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29543133 (accessed on 14 May 2022). [CrossRef]
- Borchio, L.; Machek, S.B.; Machado, M. Supplemental creatine monohydrate loading improves cognitive function in experienced mountain bikers. J. Sports Med. Phys. Fitness 2020, 60, 1168–1170. Available online: https://www.minervamedica.it/index2.php?show=R40Y2020N08A1168 (accessed on 14 October 2020). [CrossRef]
- Clarke, H.; Hickner, R.C.; Ormsbee, M.J. The Potential Role of Creatine in Vascular Health. Nutrients 2021, 13, 857. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33807747 (accessed on 14 May 2022). [CrossRef]
- Dickinson, H.; Ellery, S.; Ireland, Z.; LaRosa, D.; Snow, R.; Walker, D.W. Creatine supplementation during pregnancy: Summary of experimental studies suggesting a treatment to improve fetal and neonatal morbidity and reduce mortality in high-risk human pregnancy. BMC Pregnancy Childbirth 2014, 14, 150. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24766646 (accessed on 14 May 2022). [CrossRef]
- Balestrino, M. Role of Creatine in the Heart: Health and Disease. Nutrients 2021, 13, 1215. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33917009 (accessed on 14 May 2022). [CrossRef]
- Blaustein, M.P.; Zhang, J.; Chen, L.; Hamilton, B.P. How does salt retention raise blood pressure? Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R514–R523. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16467498 (accessed on 14 May 2022). [CrossRef]
- Ribeiro, A.S.; Avelar, A.; Kassiano, W.; Nunes, J.P.; Schoenfeld, B.J.; Aguiar, A.F.; Trindade, M.C.; Silva, A.M.; Sardinha, L.B.; Cyrino, E.S. Creatine Supplementation Does Not Influence the Ratio Between Intracellular Water and Skeletal Muscle Mass in Resistance-Trained Men. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 405–411. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32916658 (accessed on 14 May 2022). [CrossRef]
- Carvalho, A.P.P.F.; Rassi, S.; Fontana, K.E.; Correa, K.d.S.; Feitosa, R.H.F. Influence of creatine supplementation on the functional capacity of patients with heart failure. Arq. Bras. Cardiol. 2012, 99, 623–629. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22735863 (accessed on 14 May 2022). [CrossRef]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN exercise & sports nutrition review update: Research & recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 38. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30068354 (accessed on 20 October 2021).
- Tarnopolsky, M.A.; MacLennan, D.P. Creatine Monohydrate Supplementation Enhances High-Intensity Exercise Performance in Males and Females. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 452–463. Available online: https://journals.humankinetics.com/view/journals/ijsnem/10/4/article-p452.xml (accessed on 8 October 2020). [CrossRef]
- Almeida, D.; Colombini, A.; Machado, M. Creatine supplementation improves performance, but is it safe? Double-blind placebo-controlled study. J. Sports Med. Phys. Fit. 2020, 60, 1034–1039. [Google Scholar]
- Amdi, C.H.; Cleather, D.J.; Tallent, J. Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females. Sports 2021, 9, 157. Available online: http://www.ncbi.nlm.nih.gov/pubmed/34822356 (accessed on 14 May 2022). [CrossRef]
- Machek, S.B.; Hwang, P.S.; Cardaci, T.D.; Wilburn, D.T.; Bagley, J.R.; Blake, D.T.; Galpin, A.J.; Willoughby, D.S. Myosin Heavy Chain Composition, Creatine Analogues, and the Relationship of Muscle Creatine Content and Fast-Twitch Proportion to Wilks Coefficient in Powerlifters. J. Strength Cond. Res. 2020, 34, 3022–3030. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33105350 (accessed on 14 May 2022). [CrossRef]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-based differences in skeletal muscle kinetics and fiber-type composition. Physiology 2015, 30, 30–39. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25559153 (accessed on 14 May 2022). [CrossRef]
- Staron, R.S.; Hagerman, F.C.; Hikida, R.S.; Murray, T.F.; Hostler, D.P.; Crill, M.T.; Ragg, K.E.; Toma, K. Fiber type composition of the vastus lateralis muscle of young men and women. J. Histochem. Cytochem. 2000, 48, 623–629. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10769046 (accessed on 14 May 2022). [CrossRef]
- Ellery, S.J.; Walker, D.W.; Dickinson, H. Creatine for women: A review of the relationship between creatine and the reproductive cycle and female-specific benefits of creatine therapy. Amino Acids 2016, 48, 1807–1817. [Google Scholar] [CrossRef] [PubMed]
- Mihic, S.; MacDonald, J.R.; McKenzie, S.; Tarnopolsky, M.A. Acute creatine loading increases fat-free mass, but does not affect blood pressure, plasma creatinine, or CK activity in men and women. Med. Sci. Sport Exerc. 2000, 32, 291. Available online: http://journals.lww.com/00005768-200002000-00007 (accessed on 8 October 2020). [CrossRef] [PubMed]
- Smith-Ryan, A.E.; Cabre, H.E.; Eckerson, J.M.; Candow, D.G. Creatine Supplementation in Women’s Health: A Lifespan Perspective. Nutrients 2021, 13, 877. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33800439 (accessed on 5 November 2021). [CrossRef] [PubMed]
- Powers, M.E.; Arnold, B.L.; Weltman, A.L.; Perrin, D.H.; Mistry, D.; Kahler, D.M.; Kraemer, W.; Volek, J. Creatine Supplementation Increases Total Body Water Without Altering Fluid Distribution. J. Athl. Train. 2003, 38, 44–50. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12937471 (accessed on 14 May 2022).
- Sartorio, A.; Malavolti, M.; Agosti, F.; Marinone, P.G.; Caiti, O.; Battistini, N. Body water distribution in severe obesity and its assessment from eight-polar bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2005, 59, 155–160. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15340370 (accessed on 14 May 2022). [CrossRef]
- Miller, R.M.; Chambers, T.L.; Burns, S.P.; Godard, M.P. Validating InBody® 570 Multi-frequency Bioelectrical Impedance Analyzer versus DXA for Body Fat Percentage Analysis. J. Exerc. Physiol. 2016, 19, 71–78. Available online: https://www.asep.org/asep/asep/JEPonlineOCTOBER2016_Miller.pdf (accessed on 14 May 2022). [CrossRef]
- Haun, C.T.; Vann, C.G.; Roberts, B.M.; Vigotsky, A.D.; Schoenfeld, B.J.; Roberts, M.D. A Critical Evaluation of the Biological Construct Skeletal Muscle Hypertrophy: Size Matters but So Does the Measurement. Front. Physiol. 2019, 10, 247. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30930796 (accessed on 14 May 2022). [CrossRef]
- Hultman, E.; Söderlund, K.; Timmons, J.A.; Cederblad, G.; Greenhaff, P.L. Muscle creatine loading in men. J. Appl. Physiol. 1996, 81, 232–237. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8828669 (accessed on 14 May 2022). [CrossRef]
- Rawson, E.S.; Persky, A.M.; Price, T.B.; Clarkson, P.M. Effects of repeated creatine supplementation on muscle, plasma, and urine creatine levels. J. Strength Cond. Res. 2004, 18, 162–167. Available online: http://www.ncbi.nlm.nih.gov/pubmed/14971966 (accessed on 14 May 2022).
- Vandenberghe, K.; Goris, M.; Van Hecke, P.; Van Leemputte, M.; Vangerven, L.; Hespel, P. Long-term creatine intake is beneficial to muscle performance during resistance training. J. Appl. Physiol. 1997, 83, 2055–2063. Available online: http://www.ncbi.nlm.nih.gov/pubmed/9390981 (accessed on 14 May 2022). [CrossRef]
- Mackay, K.; González, C.; Zbinden-Foncea, H.; Peñailillo, L. Effects of oral contraceptive use on female sexual salivary hormones and indirect markers of muscle damage following eccentric cycling in women. Eur. J. Appl. Physiol. 2019, 119, 2733–2744. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31686212 (accessed on 14 May 2022). [CrossRef]
- Anderson, L.J.; Baker, L.L.; Schroeder, E.T. Blunted Myoglobin and Quadriceps Soreness After Electrical Stimulation During the Luteal Phase or Oral Contraception. Res. Q. Exerc. Sport 2017, 88, 193–202. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28388333 (accessed on 14 May 2022). [CrossRef]
- Kraemer, W.J.; Fry, A.C. Strength testing: Development and evaluation of methodology. In Physiological Assessment of Human Fitness; Maud, P., Foster, C., Eds.; Human Kinetics: Champaign, IL, USA, 1995; pp. 115–138. [Google Scholar]
- Kraemer, W.J.; Adams, K.; Cafarelli, E.; A Dudley, G.; Dooly, C.; Feigenbaum, M.S.; Fleck, S.J.; Franklin, B.; Fry, A.C.; Hoffman, J.; et al. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar]
- Arney, B.E.; Glover, R.; Fusco, A.; Cortis, C.; de Koning, J.J.; van Erp, T.; Jaime, S.; Mikat, R.P.; Porcari, J.P.; Foster, C. Comparison of RPE (Rating of Perceived Exertion) Scales for Session RPE. Int. J. Sports Physiol. Perform. 2019, 14, 994–996. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30569764 (accessed on 14 May 2022). [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. Available online: http://doi.apa.org/getdoi.cfm?doi=10.1037/0033-2909.86.2.420 (accessed on 8 October 2020). [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge, Lawrence Erlbaum: Hillsdale, NJ, USA, 1998; 567p. [Google Scholar]
- O’Connor, K.; Stip, E.; Pélissier, M.-C.; Aardema, F.; Guay, S.; Gaudette, G.; van Haaster, I.; Robillard, S.; Grenier, S.; Careau, Y.; et al. Treating delusional disorder: A comparison of cognitive-behavioural therapy and attention placebo control. Can. J. Psychiatry 2007, 52, 182–190. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17479527 (accessed on 14 May 2022). [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. Available online: http://journal.frontiersin.org/article/10.3389/fpsyg.2013.00863/abstract (accessed on 14 May 2022). [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 14) | Creatine (n = 14) | p-Value | |
|---|---|---|---|
| Age (years) | 25.7 ± 5.6 | 25.4 ± 6.8 | 0.88 |
| Body Mass (kg) | 61.5 ± 4.2 | 57.9 ± 7.7 | 0.13 |
| Height (cm) | 163 ± 5 | 163 ± 6 | 0.90 |
| Experience (months) | 28 ± 14 | 28 ± 14 | 0.98 |
| Heart Rate (bpm) | 81.8 ± 11.4 | 80.0 ± 8.7 | 0.83 |
| SBP (mmHg) | 113.9 ± 10.7 | 112.9 ± 7.0 | 0.45 |
| DBP (mmHg) | 72.0 ± 10.2 | 72.7 ± 7.4 | 0.83 |
| 10 RM half-squat (kg) | 37.9 ± 10.7 | 42.2 ± 14.3 | 0.25 |
| 10 RM leg press (kg) | 163.6 ± 35.6 | 176.8 ± 40.6 | 0.37 |
| Session | Set | Placebo (n = 14) | Creatine (n = 14) | ||||
|---|---|---|---|---|---|---|---|
| HR | SBP | DBP | HR | SBP | DBP | ||
| 1 | 1st | 122 ± 21 | 144 ± 22 | 77 ± 13 | 119 ± 16 | 142 ± 15 | 77 ± 8 |
| 2nd | 121 ± 18 | 141 ± 10 | 77 ± 10 | 126 ± 22 | 143 ± 10 | 76 ± 12 | |
| 3rd | 121 ± 17 | 142 ± 15 | 76 ± 11 | 127 ± 23 | 140 ± 10 | 77 ± 8 | |
| 6 | 1st | 119 ± 19 | 136 ± 16 | 75 ± 10 | 122 ± 19 | 138 ± 14 | 74 ± 7 |
| 2nd | 122 ± 13 | 139 ± 12 | 77 ± 12 | 125 ± 18 | 134 ± 12 | 74 ± 7 | |
| 3rd | 121 ± 20 | 136 ± 8 | 73 ± 10 | 133 ± 19 | 130 ± 11 | 72 ± 8 | |
| 12 | 1st | 119 ± 15 | 140 ± 11 | 78 ± 12 | 120 ± 20 | 140 ± 9 | 74 ± 10 |
| 2nd | 124 ± 15 | 140 ± 14 | 74 ± 11 | 130 ± 31 | 139 ± 10 | 75 ± 9 | |
| 3rd | 126 ± 15 | 139 ± 14 | 75 ± 13 | 134 ± 26 | 137 ± 12 | 74 ± 11 | |
| Session | Set | Placebo (n = 14) | Creatine (n = 14) | ||||
|---|---|---|---|---|---|---|---|
| HR | SBP | DBP | HR | SBP | DBP | ||
| 1 | 1st | 121 ± 19 | 137 ± 13 | 72 ± 10 | 119 ± 26 | 139 ± 11 | 68 ± 7 |
| 2nd | 127 ± 14 | 137 ± 12 | 71 ± 8 | 125 ± 21 | 137 ± 9 | 72 ± 7 | |
| 3rd | 128 ± 17 | 136 ± 13 | 73 ± 11 | 124 ± 24 | 133 ± 9 | 68 ± 8 | |
| 6 | 1st | 117 ± 20 | 133 ± 10 | 66 ± 8 | 125 ± 21 | 135 ± 7 | 66 ± 7 |
| 2nd | 120 ± 17 | 134 ± 9 | 69 ± 7 | 129 ± 19 | 135 ± 9 | 68 ± 8 | |
| 3rd | 124 ± 15 | 135 ± 12 | 72 ± 11 | 133 ± 21 | 139 ± 11 | 69 ± 11 | |
| 12 | 1st | 120 ± 14 | 132 ± 8 | 73 ± 10 | 121 ± 23 | 131 ± 8 | 69 ± 7 |
| 2nd | 127 ± 9 | 133 ± 11 | 71 ± 11 | 123 ± 18 | 132 ± 8 | 70 ± 10 | |
| 3rd | 123 ± 19 | 134 ± 9 | 68 ± 11 | 126 ± 24 | 136 ± 8 | 72 ± 9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azevedo, K.S.; Machek, S.B.; Lewis, A.E.; Azevedo, W.J.S.; Willardson, J.M.; Pereira, R.; Machado, M. Creatine Supplementation Improves Muscular Performance without Additional Impact on the Cardiovascular System in Trained Women. Muscles 2022, 1, 121-132. https://doi.org/10.3390/muscles1030013
Azevedo KS, Machek SB, Lewis AE, Azevedo WJS, Willardson JM, Pereira R, Machado M. Creatine Supplementation Improves Muscular Performance without Additional Impact on the Cardiovascular System in Trained Women. Muscles. 2022; 1(3):121-132. https://doi.org/10.3390/muscles1030013
Chicago/Turabian StyleAzevedo, Katia S., Steven B. Machek, Abby E. Lewis, Warleyson J. S. Azevedo, Jeffrey M. Willardson, Rafael Pereira, and Marco Machado. 2022. "Creatine Supplementation Improves Muscular Performance without Additional Impact on the Cardiovascular System in Trained Women" Muscles 1, no. 3: 121-132. https://doi.org/10.3390/muscles1030013
APA StyleAzevedo, K. S., Machek, S. B., Lewis, A. E., Azevedo, W. J. S., Willardson, J. M., Pereira, R., & Machado, M. (2022). Creatine Supplementation Improves Muscular Performance without Additional Impact on the Cardiovascular System in Trained Women. Muscles, 1(3), 121-132. https://doi.org/10.3390/muscles1030013