1. Introduction
Rabies is a lethal viral zoonotic disease that results in death for approximately 59,000 people per year in many countries in Africa and Asia [
1]. Because of the lack of specific and effective medical care for individuals with clinical rabies [
2,
3], many countries have taken various measures to prevent and control rabies in animals. In Africa and Asia, human rabies is contracted primarily from rabid dogs. However, several wild animal species, including bats and foxes, are carriers and vectors for rabies and related viruses in the genus Lyssavirus [
1,
3]. Rabies is almost always fatal and is one of the most painful forms of death from any infectious disease. It is also almost always preventable if properly managed according to the World Health Organization (WHO) guidelines. However, if untreated or managed incorrectly, the disease assumes horrific features that invariably kill the victim, as there is no treatment currently available for this disease.
In Pakistan, the problem of dog bites and, consequently, rabies has been an extremely contentious and neglected issue. The lack of epidemiological data on rabies has been previously noted by Iqbal et al., 2019 [
4] and Ahmad et al., 2021 [
5]. However, in Karachi alone, over 20,000 new cases of dog bite victims are treated annually [
6,
7]. In other provinces, new cases of dog bites each year range from approximately 10,000 to over 200,000 per year. In particular, this issue affects children (below the age of 15 years), as they play in the streets and are unable to run away from or defend themselves against an attacking animal. Some of the bites are severe and disfiguring if the victim is bitten on the head, face, or neck. It is also possible for multiple dogs to attack small children. Many families have been devastated by the loss of a child or a working family member. Within both the medical community and the general community, information, attitudes, and prevention practices against rabies are extremely poor.
It is well known that rabies awareness in most developing countries, including Pakistan, is inadequate [
1,
8]. Most victims do not wash bite wounds with soap and water, and most do not report bites to a health center. In healthcare centers, medical professionals do not assess wound severity correctly and, as a result, do not make the correct decisions about the use of vaccines and rabies immune globulin (RIG). Consequently, there is much mismanagement of animal bites both within the community as well as at the professional level, resulting in deaths from rabies. An important component of rabies awareness is the vaccination of dogs in public areas [
9]; however, in Pakistan, canine vaccination rates are not recorded despite the fact that the vaccination is recommended for pet dogs. In some provinces, such as Punjab, vaccines are available free of charge at public vaccination clinics. Despite this, these clinics are not available in all areas, including the study area. Additionally, there have been no studies evaluating the connection between dogs and humans in ecological settings in Pakistan [
10,
11]. Other efforts to reduce human exposure include governmental and private sector education programs, including the celebration of World Rabies Day. The goal of these programs is to educate the public on wound care and post-exposure human vaccination.
Rabies is a neglected and potentially underreported disease [
12]. In places where there is no organized control or surveillance, data are weak [
9]. Poor surveillance, underreporting, frequent misdiagnosis, and a lack of coordination between concerned departments are likely to lead to an underestimated calculation of incidence [
13,
14]. In the absence of specific data, a clustering of countries based on epidemiological, socioeconomic, and geographical criteria has been used to extrapolate estimates. Despite this, better surveillance and strengthened regional and global reporting systems would increase the accuracy of estimates and the impact of control programs. Country-specific studies of the burden and better surveillance are encouraged to obtain more reliable global estimates. In Pakistan, specifically, there have been few if any national rabies investigations on serology molecular epidemiology to support rabies prevention efforts [
5]. A robust One Health approach has been proposed to address the issue of dog bite cases and rabies around the world [
8]. Priorities for the One Health approach would include increased mass dog vaccination, access to human rabies vaccination, and community engagement.
In Pakistan, prior to 2021, there was no comprehensive surveillance system for dog-bite cases, and those cases were reported to the District Health Information System (DHIS) of the Ministry of National Health Services, Regulation and Coordination (MoNHSR&C). This system had several drawbacks, including delayed reporting and incomplete data collection. With this in mind, the reporting of dog bite cases was included in Integrated Disease Surveillance and Response System (IDSR) in 2021. To fill the gap in dog bite surveillance before 2021, the NIH started a pilot project of the World Veterinary Service (WVS) application for the real-time reporting of dog bite cases.
The National Institutes of Health of Pakistan produces equine rabies immunoglobulins (eRIG) and vero-cell culture rabies vaccine and provide these products to all public sector hospitals across the country [
15]. Moreover, different cell culture rabies vaccines and human rabies immunoglobulins (hRIG) are available in the open market. As there was no real-time data available before 2021 on the incidence of rabies in Islamabad, to address this need, a pilot project was initiated by the National Institute of Health (NIH) in collaboration with Health Security Partners (HSP) to establish dog bite case surveillance in all public sector secondary care hospitals of Islamabad by collecting information on every patient who visits a secondary care hospital with a history of dog bite and is categorized as per World Health Organization protocols [
16]. Moreover, open access to an application named WVS (world veterinary service for rabies) was given to strengthen surveillance of dog bite cases. This study aims to analyze different characteristics of dog bite case data, identify the gaps in dog bite data surveillance information, and recommend suggestions to improve and strengthen the dog bite surveillance system.
2. Materials and Methods
From December 2019 to July 2020, the study team relied on a convenience sample to enroll as many people as possible using a descriptive cross-sectional study approach. All people who visited the Federal Government Polyclinic Hospital or the Federal General Hospital and presented with a history of dog bites were considered as a case and enrolled in this study. Individuals who were afflicted with dog bites were categorized into Category I, II, and III depending on the type of exposure. Those with Category I exposure were defined as any patient presenting with an animal lick on intact skin, whereas Category II exposure were those patients with minor scratches or abrasions without bleeding, while Category III exposure patients were those who present with transdermal bite or scratches, contamination of mucus membrane or broken skin with saliva from animal licks, and exposure due to direct contact with bats. The following stakeholders were involved and engaged in the data collection for this research study:
- (a)
National Institute of Health, Islamabad (focal point for dog bite surveillance);
- (b)
Federal Government Polyclinic Hospital, Islamabad (focal point for data collection);
- (c)
Federal General Hospital, Chak Shahzad, Islamabad (focal point for data collection).
Orientation meetings were held with the hospital and research authorities to brief them on the project objectives and to develop cross-site protocols. Based on the meetings, a focal person was nominated from each emergency department staff. The designated focal person was engaged in all data collection activities and was trained in data entry using the WVS mobile-based application. Data collected included demographic information, level, and site of dog bite with category and treatment status.
Statistical Analysis
Data analysis was conducted at NIH, Islamabad. Data collected at each hospital were viewed using the WVS mobile application and analyzed using epi-info 2007 (Center for Disease Control & Prevention, Atlanta, GA, USA). Variables such as male-to-female ratio, age range, common site of bite and exposure level, and type of treatment were examined and compared, while the chai square test and independent t-test were calculated with p-value ≤ 0.005 for statistical analysis
3. Results
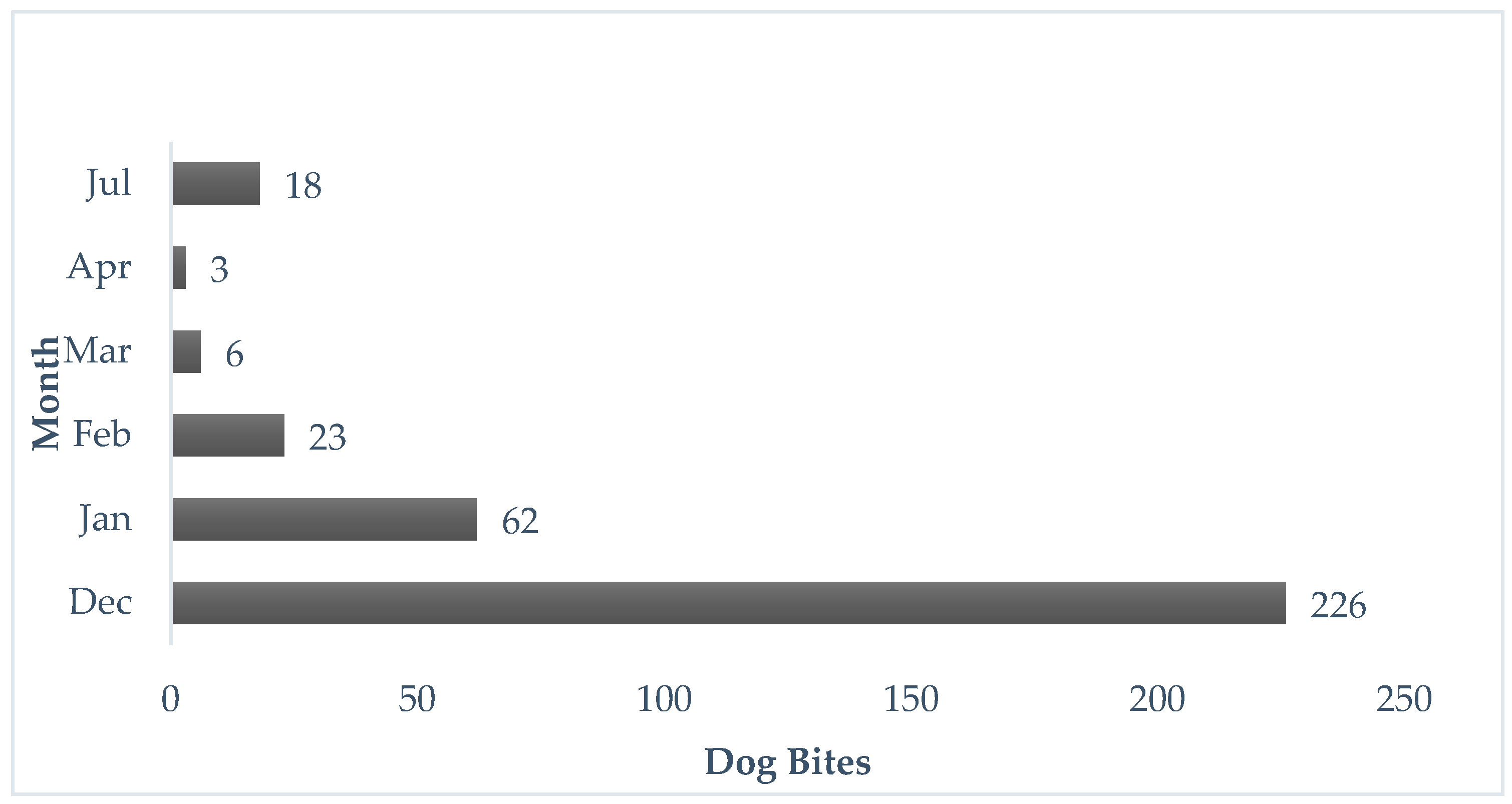
In this study, we observed 338 dog bite cases between December 2019 and July 2020. The distribution of dog bite cases by month is depicted in
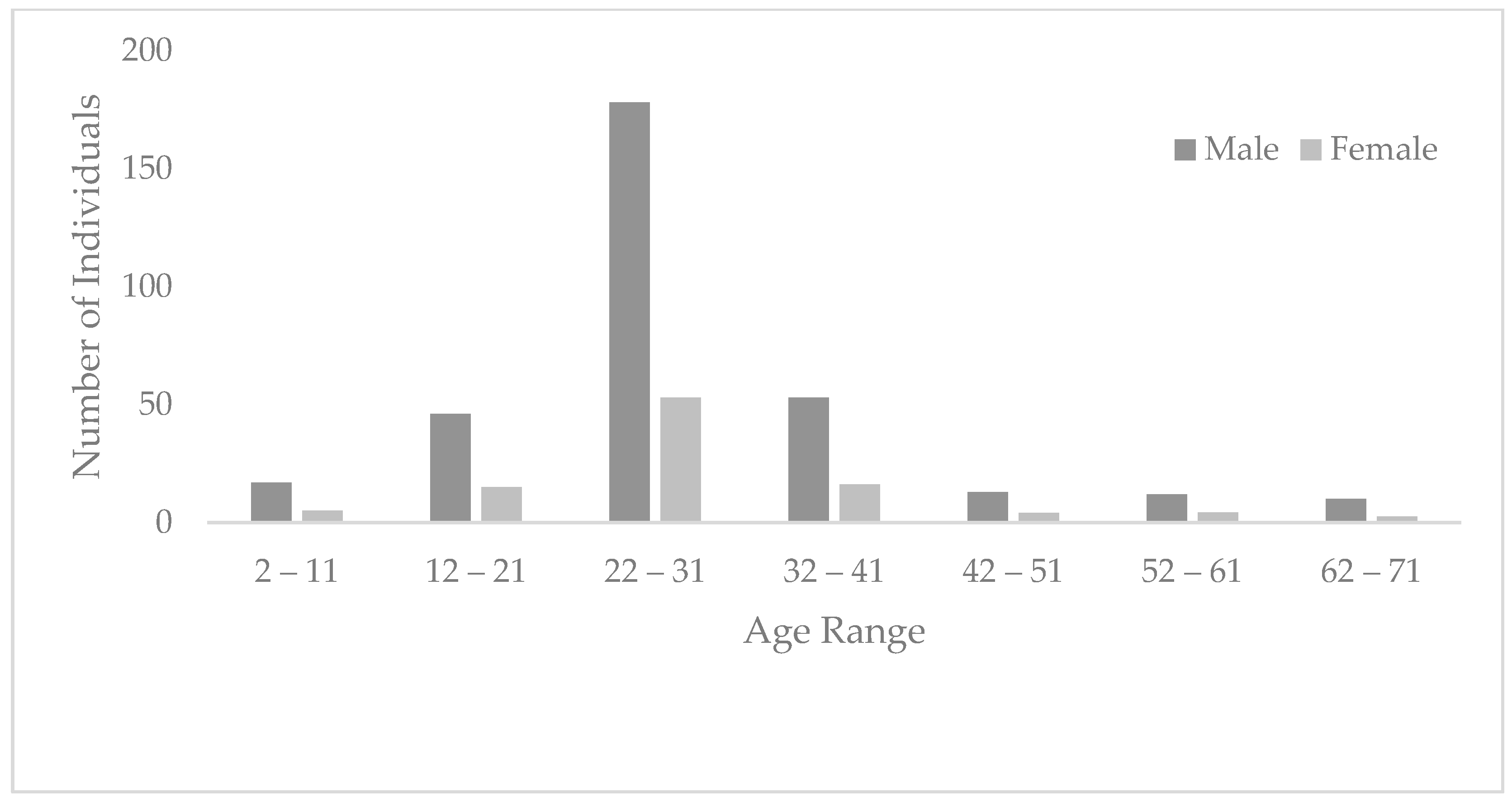
Figure 1; 233 bites occurred in males (69%), while 105 occurred in females (31%), with a male-to-female ratio of (2:1). The age range among dog bite cases was between 2 and 71 years, and the frequency of age is depicted in
Figure 2. The majority of the cases occurred in individuals aged 22 to 31 (n = 178), followed by 32 to 41 years of age (n = 53) and 12 to 21 years (n = 46). The age group least affected was aged 62–71 (n = 10), followed by 52 to 61 years of age (n = 12). An independent t-test was applied, and it showed a significant relationship between age and gender among dog bite cases (t = 2.027, df = 336, 95% CI = 0.084, 5.535,
p-value = 0.04). Similarly, a Chi-Square test showed a significant association between age groups and category of wound (χ
2 = 32.614, df = 8,
p-value ≤ 0.001). Also, there was a strong association of dog bite cases with gender (χ
2 = 6.251, df = 2,
p-value = 0.044).
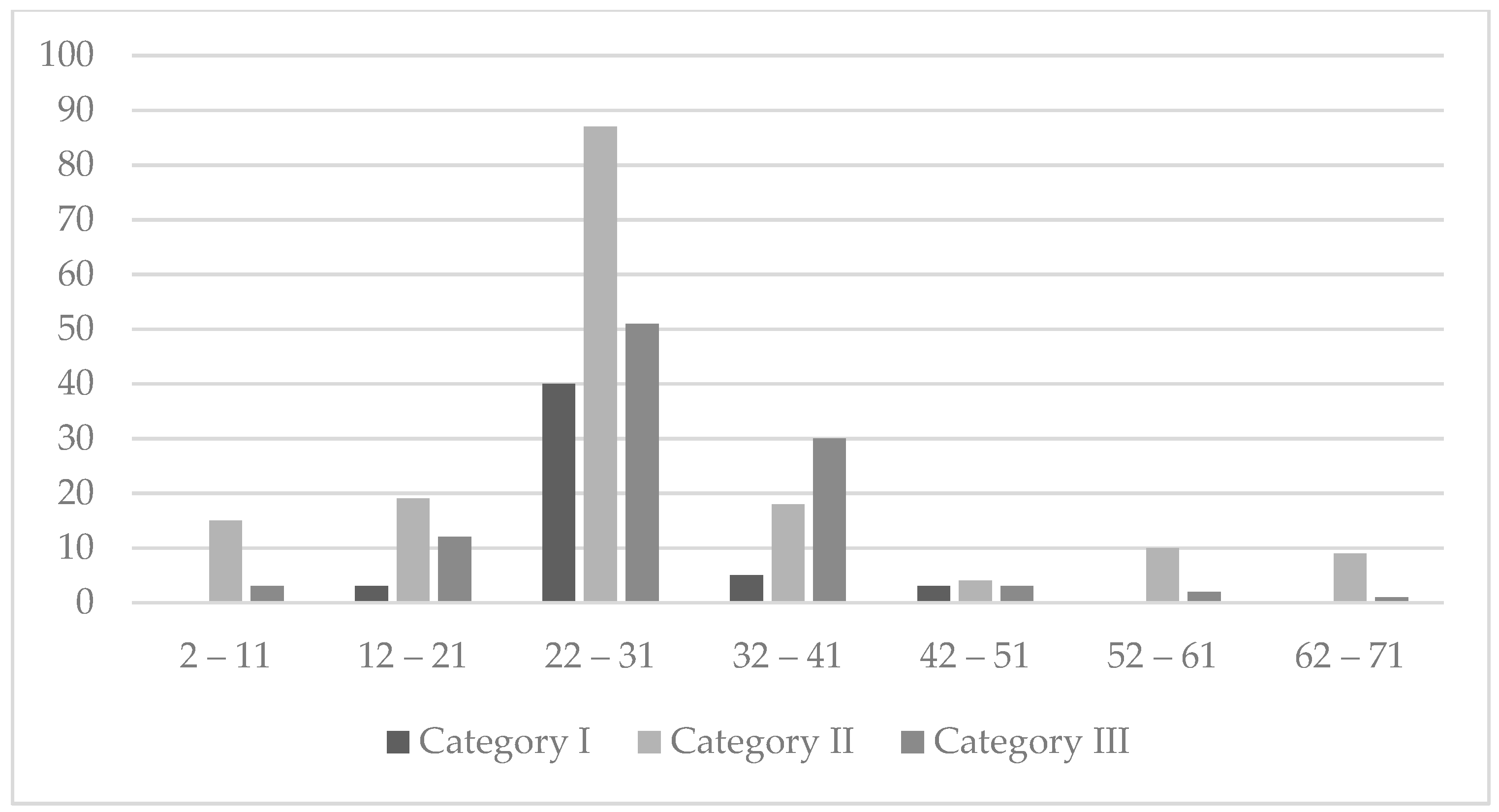
More than 51% of the dog bite cases had Category II exposure (n = 174) and 32% presented with Category III exposure (n = 106). Only 18% of people had a presentation of Category I exposure with a total of 58 cases. It was also observed that a Category II wound was common in individuals younger than 40 years of age. Category I of the wound was only noted prominently in the 22–31-year age groups (
Figure 3).
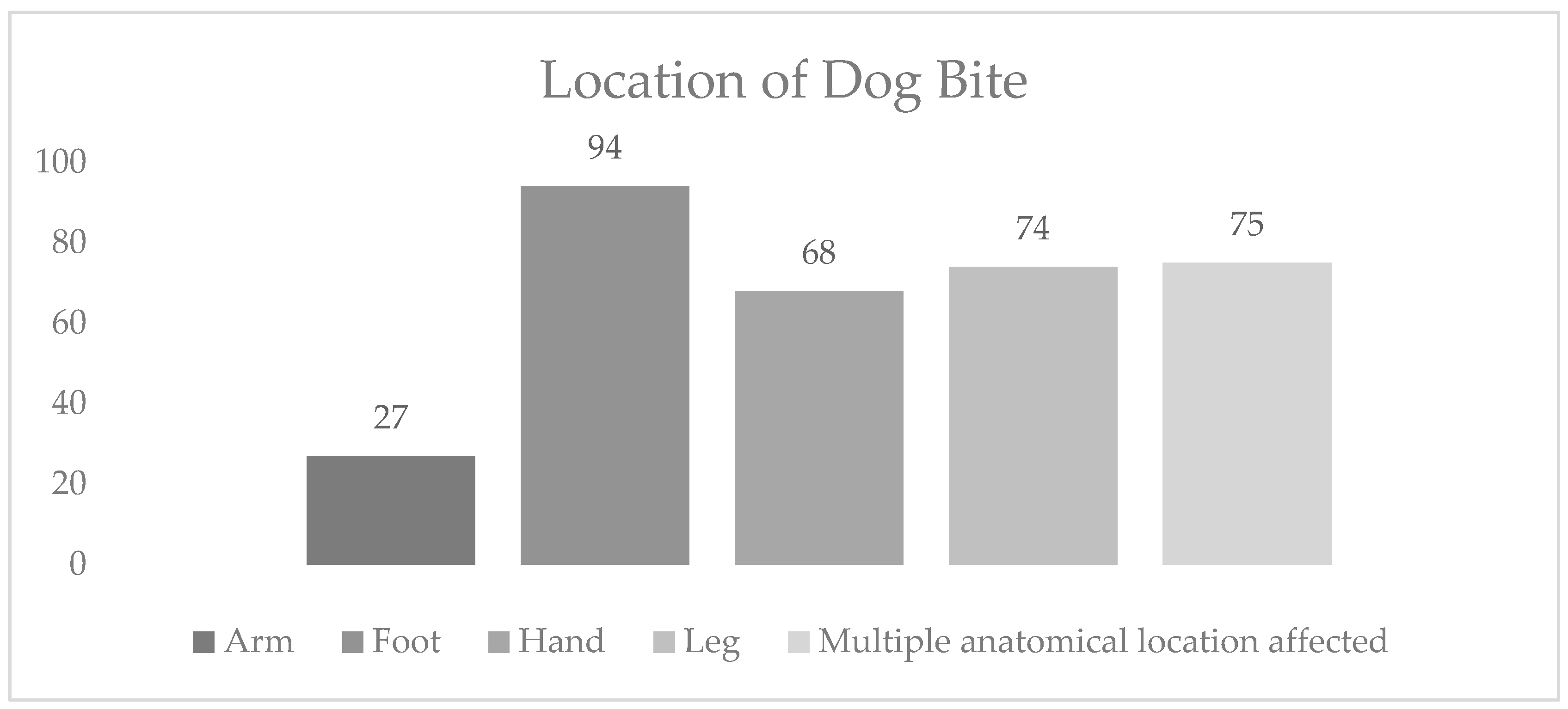
At the hospital, the anatomical location of each person’s wound was also recorded. Depending on the area affected, the wound of each person was categorized with presentation as a single anatomical location and multiple anatomical locations (
Figure 4). About 78% of people (n = 263) presented with a single anatomical location involved, while the most commonly affected location was the foot (28%), followed by the leg (22%), and the hand (20%). The area least affected area was the arm (8%). Out of the 22% of individuals indicating multiple anatomical locations, a head–neck wound was most often the case for those individuals (7%), followed by trunk–torso–buttock in (6%) of the bite cases (
Figure 4). No individuals with single or multiple anatomical locations were referred to other hospitals for further case management.
4. Discussion
Rabies is known as the oldest infectious disease to affect all mammals. The causative agent belongs to the genus
Lyssavirus and the family
Rhabdoviridae is transmitted from the saliva of an already infected (rabid) animal to other animals or humans through a bite as it does not transmit through intact skin [
17,
18,
19]. Although some data are available at the province level in Pakistan, there are no data on dog bite incidence in Islamabad prior to this study. To address this need, our pilot project was initiated by the NIH to collect dog bite case data. It was observed in the data that the most common age group (>68%) among dog bite cases was 22–41 years. Similarly, data from the Central Park Medical College, Lahore, were utilized by the University of Lahore to determine public services available for dog bite victims in district Lahore, in which the most common age group was found ranging from 16 to 60 years [
20]. The most likely reason for exposure in this group might be that in Pakistan, this age group is often outside the home for various activities such as business, prayer early in the morning, travel, and many other activities. Similar to other studies, we found that a higher number of dog bites occurred in males compared to females. A hospital-based survey was conducted in Bhutan among dog-bite-affected people, and it was found that males are more vulnerable to dog bites than females; another study conducted between June 2018 and May 2019 in Karachi also reflected such findings [
6,
21].
In many studies, it has been found that children less than 15 years of age are at high risk for dog bite attacks due to their outdoor activities [
22]. Our findings are somewhat contrary as we found the greatest incidence of bites in an older age group. Despite this, other studies have also found median age values of approximately 20 years, indicating that other interactions with dog populations may be important, such as pedestrian behavior or occupational hazards [
9].
Although in this study, a large increase in the number of dog bites was observed during the month of December, it is not clear whether this trend is a result of increased outdoor activity or increased human activity. In January 2020, the coronavirus pandemic began spreading across the world and human behavior changed significantly. In future studies, dog bite rates should be recorded throughout the year to evaluate seasonal patterns.
The wounds of 34 individuals with Category I wound were cleaned at home or at the hospital, while 24 did not treat their wounds. Only 84 persons with Category II exposure were evaluated by healthcare providers. Though all people with Category I, II, and III exposure were given the first dose of the anti-rabies vaccine, the rest of the doses had to be arranged by patients at their own cost. As per national and international guidelines, it is recommended that Category I patients should not be given the anti-rabies vaccine [
15]. However, the common practice in Pakistan is that healthcare providers at tertiary care hospitals will administer one dose of the anti-rabies vaccine to all dog bite patients, including Category I wound patients, as noted in previous studies [
9,
23]. None of the patients with Category II or III wounds were treated with rabies immunoglobulins at hospitals. To do this, they had to buy the immunoglobulins from a private pharmacy. The medications were very expensive, and patients were not provided with further hospital treatment.
In Pakistan and other developing countries, rabies is a neglected viral disease [
7]. The incidence of the disease is much lower compared to other viral diseases, and the subsequent load of patients with rabies infection is very low. Therefore, rabies patients are not managed properly as recommended by World Health Organization (WHO) or the Centers for Disease Control and Prevention (CDC) at hospitals.
The World Health Organization recommends rabies immunoglobulins for Category III exposures if an individual has not been immunized previously [
16]. The Centers for Disease Control and Prevention (CDC) has provided guidelines for the management of Category III dog bites, including recommendations for patient exposures and antibiotics for patients apart from rabies immunoglobulins and vaccination [
24]. In 2014, a study conducted on the management of dog bites by frontline service providers in primary healthcare facilities in the Greater Accra Region of Ghana concluded that knowledge and practices among frontline service providers are poor. This study recommended capacity-building training in the management of dog bites and relevant susceptible potential rabies infection [
25]. Poor dog bite management skills and practices were also evident in our study. Here, we describe poor wound management at the hospital level in most cases of Categories II and III dog bites [
9]. Often, these wounds were not cleaned or managed well. Even with Category III exposure, immunoglobulins were not administered to the patient due to the unavailability of immunoglobulins.
Since the beginning of the COVID-19 pandemic, all essential medical services to patients have been compromised [
1,
6,
16,
26,
27]. All outpatient services were limited to COVID-19 suspected patients. This challenge was faced not only by developing countries but also by each developed country as they reserved medical and emergency services to treat COVID-19 [
28]. The lockdown was imposed in the last week of March or the first week of April 2020 throughout the whole country [
29]. The public was directed to avoid unnecessary outside activity. However, these restrictions were not applicable to the health sector, pharmacies, and patients visiting emergency departments [
30]. Although dedicated rabies clinics were not available in Islamabad, dog bite cases were managed by the emergency departments of public and private sector hospitals. The anti-rabies vaccine was available in the hospitals and public sector hospitals as per policy, and they provided the first dose of the anti-rabies vaccine free of cost. The anti-rabies vaccine was also available in private hospitals and pharmacies for purchase. Despite the lockdown and work-from-home policies, the NIH-Pakistan produced and supplied anti-rabies vaccines to government hospitals and dispensaries throughout the pandemic. From March to June 2020, only 26 dog bite cases were reported in this pilot project. This project was limited as a result of resource reallocation due to the COVID-19 pandemic as, ideally, rabies surveillance would include additional months of surveillance and evaluation of patient outcomes.
This study represents the first report of incidence data from Islamabad, and from the data, it is clear that real-time dog bite data can be collected easily, and that surveillance can be conducted at a facility level and potentially at district or state levels. At the hospital level, immunoglobulins are not provided, which requires patients to purchase these medications out of pocket or skip treatment if their bite is categorized as Category III. This increases the chances for patients of developing a rabies infection and its complications and may result in the death of the patient if the cost of immunoglobulins is out of reach. A limitation of this study is that it focused only on the surveillance of human bites. There is a veterinary component to the spread of rabies in Pakistan that should also be examined in order to further prevention and control efforts. Future research should include a One Health strategy to incorporate an examination of the spread of this deadly pathogen in humans, animals, and the environment.
It is recommended that immunoglobulins be provided free of cost at the facility level to minimize the burden on patients and, consequently, lower the chances of carrying rabies infection. There should be multi-stakeholder engagement in rabies surveillance using a One Health approach involving political commitment, as it will empower surveillance mechanisms from local administrations to the ministerial level. Additionally, the management of dog populations should be managed by municipal administration to control, neutralize, and vaccinate stray dogs rather than kill them.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}



