INTRODUCTION
Deviations in muscle tone are among the neuromuscular impairments presumed to accompany and perhaps influence motor control deficits in select forms of dysarthria and dysphagia (Darley, Aronson, & Brown, 1975;
Duffy, 2005;
Logemann, 1998). Muscle tone can be defined
physiologically as a state of steady involuntary contraction or tension in a relaxed muscle, contributing to the
clinical definition of tone, which is the resistance a relaxed muscle offers to passive stretch (Benarroch, Westmoreland, Daube, Reagan, & Sandok, 1999). Muscle tone is regulated by peripheral reflexes and by central influences on peripheral reflexes (
Benarroch et al., 1999). Pathologically heightened muscle tone (hypertonia) leads to stiffness that may vary according to the speed of movement or extent of displacement. Hypertonia typically results from lesions within the central nervous system and is thought to underlie spasticity and rigidity in spastic and hypokinetic dysarthria, respectively (
Duffy, 2005). Abnormally decreased tone (hypotonia) causes muscles to be flaccid or “floppy” and is typically associated with lesions to the peripheral nervous system. Less frequently, damage to the cerebellar control circuit may also cause hypotonia (Fine, Ionita, & Lohr, 2002). Flaccid and ataxic dysarthria are associated with reduced muscle tone (
Duffy, 2005).
The contribution of tone deviations to dysarthria has been grossly understudied. Nonetheless, interventions developed in physical medicine and rehabilitation to address tone deviations in the limb musculature have been adopted by speech-language pathologists (
Clark, 2003). These treatments are intended to alleviate tone deviations and/or to prevent the development or exacerbation of tone deviations in patients experiencing neuromuscular impairments. Two such interventions were selected for study in the current project.
The use of therapeutic vibration has a long history in physical rehabilitation. Vibration influences muscle tone by stimulating the muscle spindle, causing contraction of the stimulated muscle as well as inhibiting contraction in the antagonist. Through this mechanism, vibration may be applied directly to a hypotonic muscle in order to increase tone (
Bishop, 1975). Because not all skeletal muscles possess muscle spindles or spindle-mediated reflexes, therapeutic vibration would not be expected to have uniform effects across all muscle groups (
Clark, 2003).
Cryotherapy, or the application of cold, also has known effects on neuromuscular function. Pertinent to the current study is that cold helps ameliorate spasticity by reducing nerve conduction velocities and thereby the effects of peripheral reflexes on muscle tone (
Gracies, 2001;
Katz, 1988;
McGown, 1967;
Michlovitz, 1986;
Miglietta, 1973). Because the effect of icing does not rely on muscle spindle action, this intervention would be predicted to reduce tone in muscles regardless of the presence of muscle spindles or muscle spindle reflexes (
Clark, 2003).
No published studies have expressly examined how therapeutic interventions influence tone of any of the muscles of the speech mechanism. One likely contributing factor to this void is that methods for assessing muscle tone in the orofacial system are not generally available. Subjective assessment of muscle tone in the limb musculature involves the examiner moving a relaxed limb through its range of movement and judging the degree of resistance offered across a joint (Sloan, Sinclair, Thompson, Taylor, & Pentland, 1992). Variations of this method have been proposed for assessing tone of the lips and tongue (
Beckman, 1988;
Dworkin & Culatta, 1996) although these applications have not been empirically investigated. Several objective measures of muscle tone have been reported for the limb musculature (
Bizzini & Mannion, 2003; Boiteau, Maloulin, & Richards, 1995;
Leonard et al., 2003;
Mendelson, 1984; Pisano, Miscio, Colombo, & Pinelli, 1996) but, with one known exception, (Hunker, Abbs, & Barlow, 1982), similar tools have only recently been applied to the muscles used for speech and swallowing. Studies have examined tissue stiffness of the perioral region (Chu, Barlow, & Lee, 2009), tongue (
Solomon & Clark, 2010; Veldi, Vasar, Hion, Vain, & Kull, 2002; Veldi, Vasar, Vain, & Kull, 2004), cheeks (
Solomon & Clark, 2010), and soft palate (
Veldi et al., 2004).
A primary objective of this pilot study was to explore the utility of the Myotonometer™ (Neurogenic Technologies, Missoula, MT) for providing objective measures of muscle tone in the orofacial system for research as well as clinical purposes. The Myotonometer™ is a handheld instrument that applies force across a flat 1-cm diameter probe positioned on the skin overlying the muscle of interest. It measures tissue compliance by recording tissue displacement at each of eight incremental forces ranging from 0 to 1 kg. Tissue compliance at rest reflects muscle tone as well as the stiffness of nonmuscular tissue, and is the measure most pertinent to the current study. Tissue compliance during a maximum voluntary contraction (MVC) is associated with muscle strength (
Leonard et al., 2003); the difference in compliance between the two contraction states has been suggested to be predictive of overall level of muscle impairment (Leonard, Stephens, & Stroppel, 2001).
The muscles studied in the current project are those located in the submental region, which includes the anterior belly of the digastric, genioglossus, geniohyoid, hyoglossus, mylohyoid, and the platysma. All but the last muscle are primarily responsible for jaw movement and laryngeal elevation, but are also active during anterior tongue elevation (Jaffe, McCulloch, Palmer, & Luschei, 1997). The platysma does not act directly on any structures, but contributes to the tone of the superficial neck and lower face. These muscles are believed to possess muscle spindles, but corresponding reflex responses are poorly described and do not clearly mimic muscle spindle reflexes in the limbs (
Bowman, 1971;
Bowman & Combs, 1968; Neilson, Andrews, Guitar, & Quinn, 1979; Ostry, Gribble, Levin, & Feldman, 1997;
Weber & Smith, 1987).
The purpose of this study was to assess changes in compliance of the submental tissue in relaxed and contracted muscle states, and following application of vibration and icing, using the MyotonometerTM. We hypothesized that compliance would be greater at rest than during an MVC because contraction should stiffen the muscles. This result would serve as validation that the Myotonometer™ is indeed able to detect changes in submental muscle stiffness. Further, we hypothesized that vibration would not alter the resting or active compliance of the targeted muscles because they lack typical muscle spindle reflexes. Icing, which is purported to decrease nerve conduction velocities, was predicted to increase muscle compliance at rest (i.e., reduce muscle tone) and during MVC (i.e., reduce muscle strength) because its effects are not dependent on the presence of muscle spindle reflexes.
METHOD
Participants. The use of human subjects was approved by the Institutional Review Board of the participating university. Participants included 16 women (age range 22 – 24 years) without reported history of neurologic, orofacial, or speech/language impairments. All participants exhibited grossly normal orofacial structure and function as judged by the examiner and adequate hearing and language capabilities for completing the experimental tasks.
Procedures. Each participant completed two experimental sessions. The interval between the two sessions ranged from 24–72 hours. During each session, compliance of submental tissue was recorded before and after the application of a therapeutic intervention. At all recording times, compliance was measured at rest and during MVC. To promote muscle relaxation, resting measures were always recorded prior to active measures (
Leonard et al., 2003). The MVC task involved raising the tongue as hard as possible against an air-filled bulb positioned along the hard palate. The Iowa Oral Performance Instrument (IOPI, IOPI Medical LLC), which was coupled to the airfilled bulb, displayed pressure exerted on the bulb, allowing the examiner to ensure that the target movement was produced during the MVC task.
Following the pre-intervention compliance measures, one of the interventions was applied. Vibration was applied using a hand-held massager that provided a low-amplitude 200 Hz vibration. Icing was applied using a “Blue Ice” first-aid cold pack wrapped in a single layer of cotton fabric. In both the vibration and icing conditions, stimulation was applied directly over the target muscle group (i.e., submandibularly) for two minutes. Repeat measures of resting and active compliance, in that order, were recorded immediately following the application of the intervention. The order of interventions was counterbalanced across participants, with half of the participants receiving the icing intervention during the first session and the other half receiving vibration during the first session.
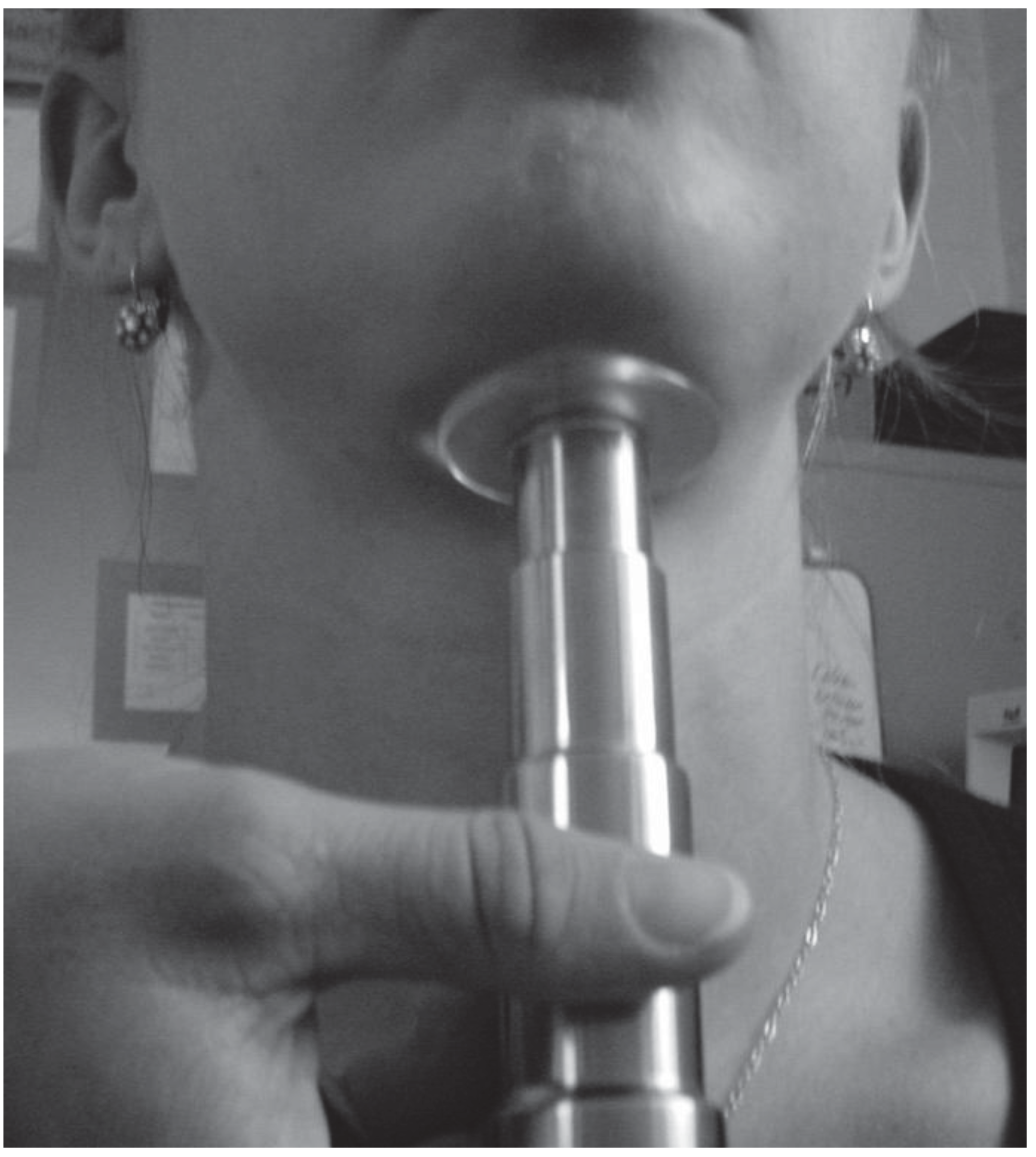
To measure submental tissue compliance, the Myotonometer™ was held below the chin with the probe deflecting upward toward the target musculature. The probe was positioned medially midway between the posterior border of the chin and the anterior border of the hyoid bone. During resting compliance measures, participants were instructed to completely relax. The examiner then applied upward pressure on the probe (
Figure 1). The Myotonometer™ yields a data set for each trial that includes the tissue displacement at each
force level as well as “area under the curve” (AUC), which is a composite measure reflecting the extent of displacement across all force increments. Four trials were performed sequentially for each condition, in approximately 1 second intervals. The average AUC served as the dependent variable for statistical analysis.
The experiment involved two conditions of muscle state (rest and MVC), two measurement points (pre- and post-intervention), and two intervention conditions (vibration and icing). Experimental hypotheses were tested using a 2x2x2 repeated-measures ANOVA.
RESULTS
Test-Retest Reliability. Pre-intervention measures of muscle compliance were obtained during both experimental sessions.
Table 1 lists resting and active compliance for each participant during the first and second sessions. The mean change across sessions was 7.2% for resting compliance and 4.3% for active compliance. Eleven of the 16
participants’ AUC results (69%) agreed within 9% for resting compliance and 15% for active compliance; 13 participants’ data (81%) agreed within 15% for resting compliance and 17% for active compliance. These agreements indicate reasonable test-retest reliability for most participants. Disagreements, however, were as great as 35% and 47% for passive and active compliance, respectively.
Effects of Contraction and Intervention. ANOVA revealed a significant main effect of muscle state [F(1, 15) = 89.35; p<.001] but no main effects of either measurement point [F(1, 15) – 2.78; p = .234] or intervention [F(1, 15) = .587; p = .455]. A significant interaction between measurement point and muscle state [F(1, 15) – 14.32; p = .002] was observed.
As illustrated in
Figure 2, the magnitude of the difference in compliance between resting and contracted muscle was greater prior to the interventions. The lack of significant interaction among measurement point, muscle state, and intervention condition [F(1, 15) = .089;
p = .769] indicates that this difference was similar for both interventions.
DISCUSSION
One purpose of the present study was to explore the feasibility of using the Myotonometer™ to measure submental tissue compliance. Two analyses addressed this issue: variability across sessions and the main effect of muscle activity. Consistency across sessions was generally quite good, with 11 participants varying less than 9% in the resting condition and less than 15% in the active condition. The greatest differences noted between sessions was 35% during relaxation and 47% during contraction. Large differences across sessions for the resting condition could reflect normal daily variations in muscle tone or strength, and in the active condition could reflect different degrees of contraction despite attempts to exert maximal effort. However, measurement error seems the more likely explanation. Because the inferior borders of the mandible are in close proximity to the target measurement site, slight variations in positioning or angle of the probe may have captured stiffness of tendon or other connective tissue. The sensitivity of the Myotonometer™ to measurement variations could be studied by systematically altering the submental probe position and depression angle. This may be particularly useful in future studies that seek to explore age- and sex-related variations in muscle compliance. The other analysis speaking to the feasibility of using the Myotonometer™ to assess submental muscle tone is whether changes in compliance were detected between resting and active contraction states.
Figure 2 clearly shows that large reductions in compliance were recorded during the active contraction state relative to rest. Thus, even though the muscles in the submental area are generally smaller than those most typically assessed with the Myotonometer™ (e.g., triceps, trapezius), the change in tissue compliance generated by contraction of these muscles was well within the measurement parameters of the Myotonometer™.
Of primary interest was the effect of intervention on resting muscle compliance, the index of muscle tone, as this physical parameter is often cited as an appropriate target for treatment. If the submental muscles demonstrated typical spindle reflexes in response to vibration, the resulting contraction would result in decreased tissue compliance. No changes in compliance were detected following vibration, thus our findings do not provide evidence for spindle reflexes in the submental musculature (
Bowman, 1971;
Bowman & Combs, 1968;
Neilson et al., 1979;
Ostry et al., 1997;
Weber & Smith, 1987).
Therapeutic icing is thought to influence muscle tone by decreasing nerve conduction velocities. We predicted that icing of the submental musculature would increase muscle tissue compliance at rest (indicating decreased muscle tone) and during maximum contraction (indicating decreased muscle strength). Neither of these predictions held true. One possible explanation is that the icing did not cool the muscles or nerves to the extent necessary to impact neuromuscular function. Subjects consistently reported that the stimulated tissue felt cold, but somatosensory effects may not predict the impact on the sensorimotor system. An alternative explanation is that icing affected tissue compliance by more than one mechanism. Specifically, in addition to reducing nerve conduction velocities, icing also decreases blood flow (Ho, Coel, Kagawa, & Richardson, 1994) and increases muscle stiffness (
Price & Lehmann, 1990), which may lead to decreased tissue compliance. Because the Myotonometer™ measures compliance of muscle and surrounding tissue, it cannot isolate nerve effects from perfusion effects.
The outcome measure of interest in the current study was muscle compliance before and after therapeutic interventions. Although we considered active and resting compliance as independent measures, previous studies have also considered the difference in compliance between active and resting states to be relevant to detection of changes in neuromuscular function (
Leonard et al., 2001). The significant interaction between muscle state and measurement point indicates that the difference in compliance between active and resting states was larger prior to intervention compared to after intervention. We might speculate that intervention-induced changes in neuromuscular function of the submental musculature is so subtle that neither resting nor active compliance in isolation is sufficient to detect it, but that the composite “compliance difference” measure is more sensitive to subtle changes. This hypothesis must be tested in a prospective study with the expected therapeutic mechanisms of any predicted effects clearly specified.
This pilot study was motivated by a desire to identify tools that quantify muscle tone in the orofacial musculature so such tools can be employed to examine the effects of interventions on muscle tone. The present findings suggest that the Myotonometer™ is sensitive to changes in submental compliance associated with muscle contraction. Although changes in compliance were not detected after intervention, a number of issues limit our ability to draw strong conclusions from these preliminary findings. First, changes in compliance that might have occurred may be too subtle to be detected by the Myotonometer™. Second, treatment effects on muscle compliance were assessed in healthy participants. Although the proposed therapeutic mechanisms should act on healthy tissue, the effects may be more dramatic in neuromuscular impairment. A related issue is that we intentionally selected a muscle group that was not predicted to respond to one of the interventions. Greater effects of vibration would be predicted in orofacial muscle groups with documented spindle reflexes (e.g., masseter). Further limiting our ability to detect changes as a result of intervention was the relatively small sample size. Finally, this pilot study was limited to the study of a single dose. The size of intervention effects, however, may be dose dependent. Although this pilot study was necessarily limited in scope, it generated these additional issues as potential topics for future investigations.



{kind=link}
{kind=link}