
FLOating-Window Projective Separator (FloWPS) Machine Learning Approach to Predict Individual Clinical Efficiency of Cancer Drugs †





Abstract
:1. Background
2. Methods
2.1. Clinically Annotated Molecular Datasets
- −
- at least 40 gene expression profiles present;
- −
- data obtained for the same cancer type and using the same experimental platform;
- −
- every profile is linked with the case clinical history;
- −
- all cancers treated with at least one common drug or chemotherapy regimen;
- −
- treatment outcomes are available, enabling the classification of every case as either responder or non-responder.
2.2. Machine Learning (ML) Application with and without FloWPS
3. Results and Discussion
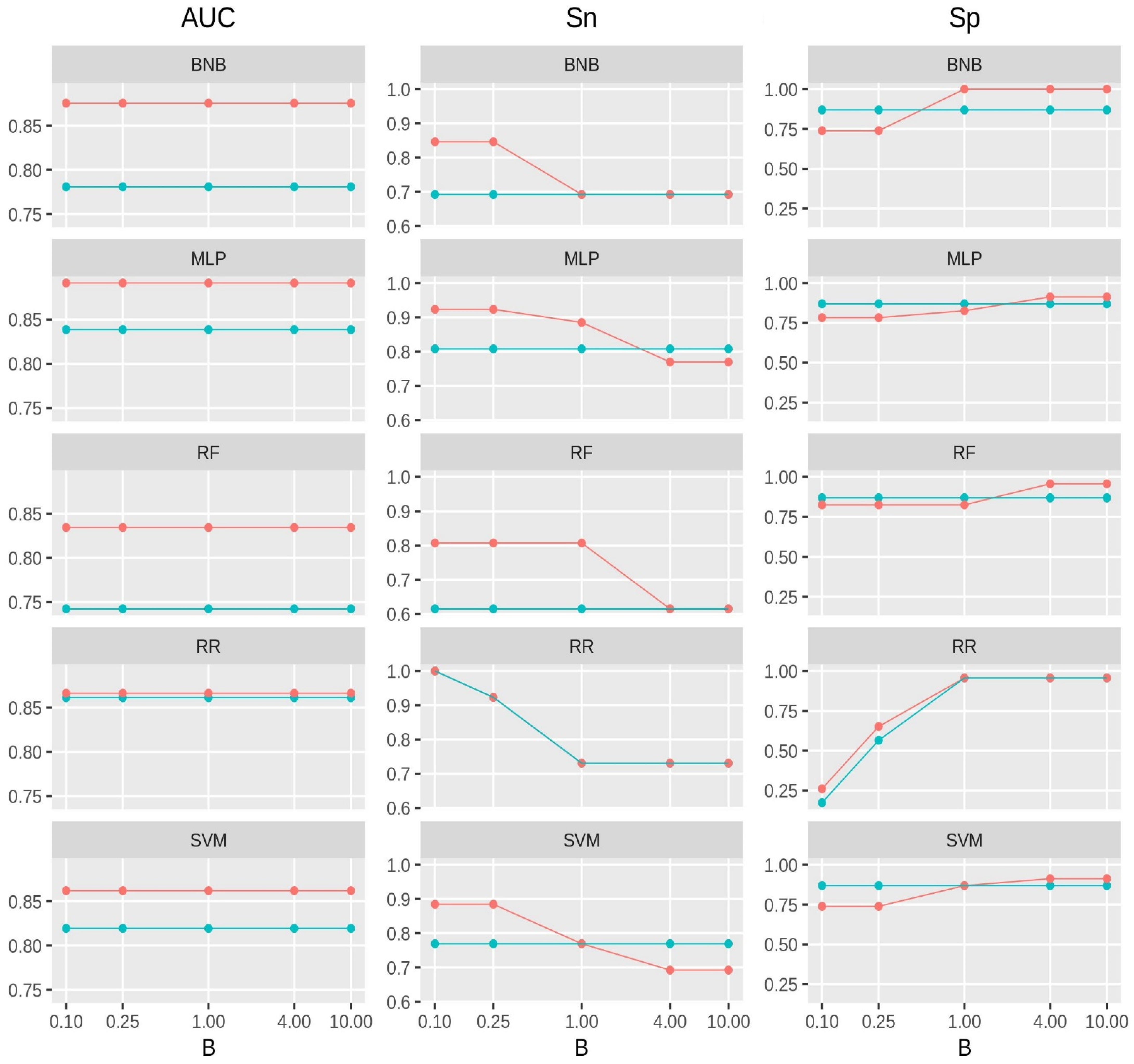
3.1. Performance of FloWPS with Different Balance Factors for False Positive vs. False Negative Errors
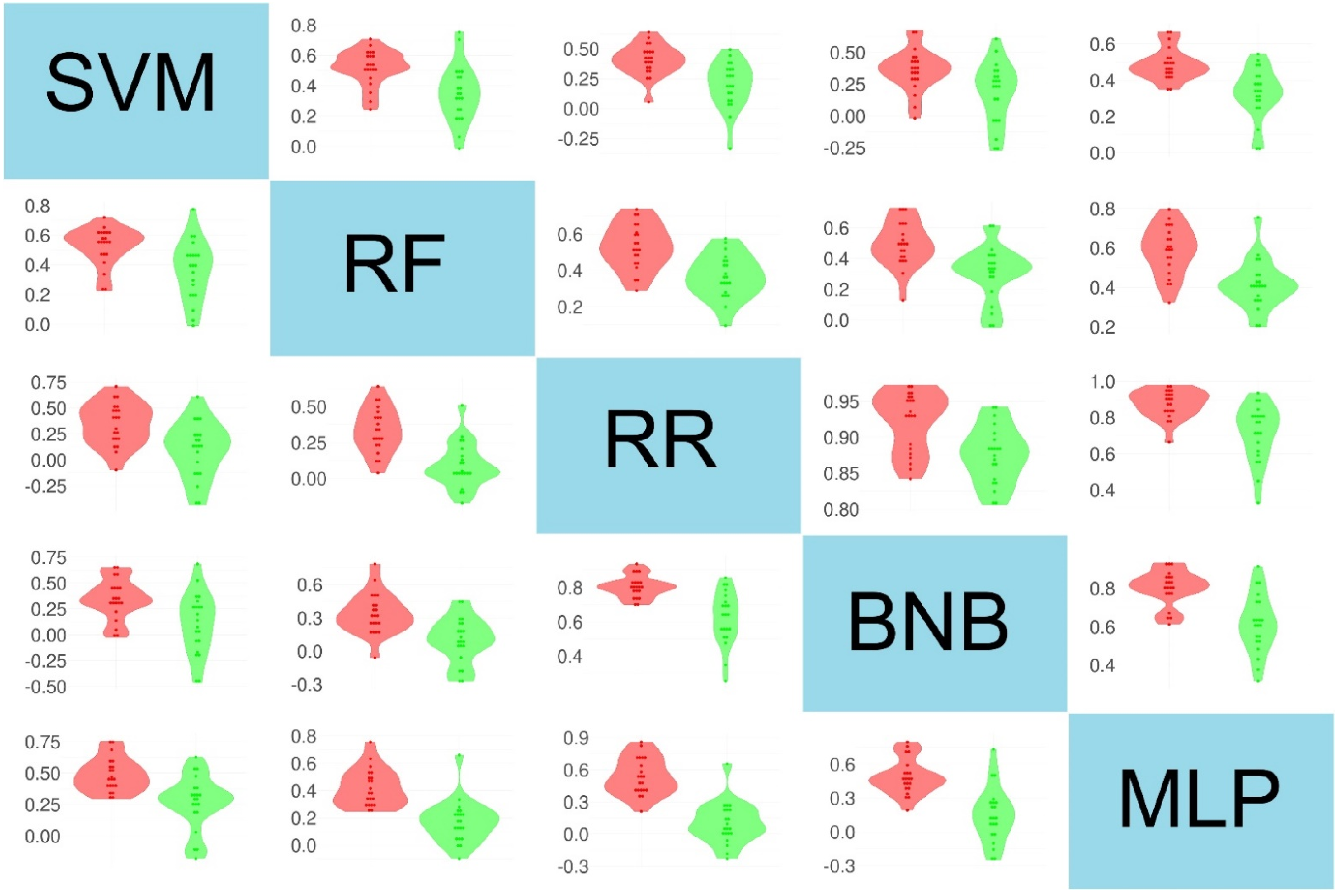
3.2. Correlation Study between Different ML Methods at the Level of Feature Importance
3.3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buzdin, A.; Sorokin, M.; Poddubskaya, E.; Borisov, N. High-Throughput Mutation Data Now Complement Transcriptomic Profiling: Advances in Molecular Pathway Activation Analysis Approach in Cancer Biology. Cancer Inform. 2019, 18, 117693511983884. [Google Scholar] [CrossRef] [PubMed]
- Tkachev, V.; Sorokin, M.; Mescheryakov, A.; Simonov, A.; Garazha, A.; Buzdin, A.; Muchnik, I.; Borisov, N. Floating-Window Projective Separator (FloWPS): A Data Trimming Tool for Support Vector Machines (SVM) to Improve Robustness of the Classifier. Front. Genet. 2019, 9, 717. [Google Scholar] [CrossRef] [PubMed]
- Borisov, N.; Sorokin, M.; Tkachev, V.; Garazha, A.; Buzdin, A. Cancer gene expression profiles associated with clinical outcomes to chemotherapy treatments. BMC Med. Genom. 2020, 13, 111. [Google Scholar] [CrossRef] [PubMed]
- Tkachev, V.; Sorokin, M.; Borisov, C.; Garazha, A.; Buzdin, A.; Borisov, N. Flexible Data Trimming Improves Performance of Global Machine Learning Methods in Omics-Based Personalized Oncology. Int. J. Mol. Sci. 2020, 21, 713. [Google Scholar] [CrossRef]
- Borisov, N.; Sergeeva, A.; Suntsova, M.; Raevskiy, M.; Gaifullin, N.; Mendeleeva, L.; Gudkov, A.; Nareiko, M.; Garazha, A.; Tkachev, V.; et al. Machine Learning Applicability for Classification of PAD/VCD Chemotherapy Response Using 53 Multiple Myeloma RNA Sequencing Profiles. Front. Oncol. 2021, 11, 652063. [Google Scholar] [CrossRef]
- Chadaga, K.; Prabhu, S.; Umakanth, S.; Bhat, K.; Sampathila, N.; Chadaga, R. COVID-19 Mortality Prediction among Patients using Epidemiological parameters: An Ensemble Machine Learning Approach. Eng. Sci. 2021, 16, 221–233. [Google Scholar] [CrossRef]
- Musunuri, B.; Shetty, S.; Shetty, D.K.; Vanahalli, M.K.; Pradhan, A.; Naik, N.; Paul, R. Acute-on-Chronic Liver Failure Mortality Prediction using an Artificial Neural Network. Eng. Sci. 2021, 15, 187–196. [Google Scholar] [CrossRef]
- Khalsan, M.; Machado, L.R.; Al-Shamery, E.S.; Ajit, S.; Anthony, K.; Mu, M.; Agyeman, M.O. A Survey of Machine Learning Approaches Applied to Gene Expression Analysis for Cancer Prediction. IEEE Access 2022, 10, 27522–27534. [Google Scholar] [CrossRef]
- Cong, Y.; Shintani, M.; Imanari, F.; Osada, N.; Endo, T. A New Approach to Drug Repurposing with Two-Stage Prediction, Machine Learning, and Unsupervised Clustering of Gene Expression. OMICS J. Integr. Biol. 2022, 26, 339–347. [Google Scholar] [CrossRef]
- Azarkhalili, B.; Saberi, A.; Chitsaz, H.; Sharifi-Zarchi, A. DeePathology: Deep Multi-Task Learning for Inferring Molecular Pathology from Cancer Transcriptome. Sci. Rep. 2019, 9, 16526. [Google Scholar] [CrossRef]
- Turki, T.; Wang, J.T.L. Clinical intelligence: New machine learning techniques for predicting clinical drug response. Comput. Biol. Med. 2019, 107, 302–322. [Google Scholar] [CrossRef] [PubMed]
- Turki, T.; Wei, Z. A link prediction approach to cancer drug sensitivity prediction. BMC Syst. Biol. 2017, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Turki, T.; Wei, Z. Learning approaches to improve prediction of drug sensitivity in breast cancer patients. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3314–3320. [Google Scholar]
- Turki, T.; Wei, Z.; Wang, J.T.L. Transfer Learning Approaches to Improve Drug Sensitivity Prediction in Multiple Myeloma Patients. IEEE Access 2017, 5, 7381–7393. [Google Scholar] [CrossRef]
- Turki, T.; Wei, Z.; Wang, J.T.L. A transfer learning approach via procrustes analysis and mean shift for cancer drug sensitivity prediction. J. Bioinform. Comput. Biol. 2018, 16, 1840014. [Google Scholar] [CrossRef] [PubMed]
- Borisov, N.; Tkachev, V.; Suntsova, M.; Kovalchuk, O.; Zhavoronkov, A.; Muchnik, I.; Buzdin, A. A method of gene expression data transfer from cell lines to cancer patients for machine-learning prediction of drug efficiency. Cell Cycle 2018, 17, 486–491. [Google Scholar] [CrossRef]
- Borisov, N.; Buzdin, A. New Paradigm of Machine Learning (ML) in Personalized Oncology: Data Trimming for Squeezing More Biomarkers From Clinical Datasets. Front. Oncol. 2019, 9, 658. [Google Scholar] [CrossRef]
- Arimoto, R.; Prasad, M.-A.; Gifford, E.M. Development of CYP3A4 inhibition models: Comparisons of machine-learning techniques and molecular descriptors. J. Biomol. Screen. 2005, 10, 197–205. [Google Scholar] [CrossRef]
- Balabin, R.M.; Lomakina, E.I. Support vector machine regression (LS-SVM): An alternative to artificial neural networks (ANNs) for the analysis of quantum chemistry data? Phys. Chem. Chem. Phys. 2011, 13, 11710–11718. [Google Scholar] [CrossRef]
- Balabin, R.M.; Smirnov, S.V. Interpolation and extrapolation problems of multivariate regression in analytical chemistry: Benchmarking the robustness on near-infrared (NIR) spectroscopy data. Analyst 2012, 137, 1604–1610. [Google Scholar] [CrossRef]
- Betrie, G.D.; Tesfamariam, S.; Morin, K.A.; Sadiq, R. Predicting copper concentrations in acid mine drainage: A comparative analysis of five machine learning techniques. Environ. Monit. Assess. 2013, 185, 4171–4182. [Google Scholar] [CrossRef]
- Hatzis, C.; Pusztai, L.; Valero, V.; Booser, D.J.; Esserman, L.; Lluch, A.; Vidaurre, T.; Holmes, F.; Souchon, E.; Wang, H.; et al. A genomic predictor of response and survival following taxane-anthracycline chemotherapy for invasive breast cancer. JAMA 2011, 305, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Itoh, M.; Iwamoto, T.; Matsuoka, J.; Nogami, T.; Motoki, T.; Shien, T.; Taira, N.; Niikura, N.; Hayashi, N.; Ohtani, S.; et al. Estrogen receptor (ER) mRNA expression and molecular subtype distribution in ER-negative/progesterone receptor-positive breast cancers. Breast Cancer Res. Treat. 2014, 143, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Horak, C.E.; Pusztai, L.; Xing, G.; Trifan, O.C.; Saura, C.; Tseng, L.-M.; Chan, S.; Welcher, R.; Liu, D. Biomarker analysis of neoadjuvant doxorubicin/cyclophosphamide followed by ixabepilone or Paclitaxel in early-stage breast cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, G.; Mitsiades, C.; Bryant, B.; Zhan, F.; Chng, W.J.; Roels, S.; Koenig, E.; Fergus, A.; Huang, Y.; Richardson, P.; et al. Gene expression profiling and correlation with outcome in clinical trials of the proteasome inhibitor bortezomib. Blood 2007, 109, 3177–3188. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, D.; Tian, Z.; Nicholson, B.; Kumar, K.G.S.; Zhou, B.; Carrasco, R.; McDermott, J.L.; Leach, C.A.; Fulcinniti, M.; Kodrasov, M.P.; et al. A small molecule inhibitor of ubiquitin-specific protease-7 induces apoptosis in multiple myeloma cells and overcomes bortezomib resistance. Cancer Cell 2012, 22, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Terragna, C.; Remondini, D.; Martello, M.; Zamagni, E.; Pantani, L.; Patriarca, F.; Pezzi, A.; Levi, G.; Offidani, M.; Proserpio, I.; et al. The genetic and genomic background of multiple myeloma patients achieving complete response after induction therapy with bortezomib, thalidomide and dexamethasone (VTD). Oncotarget 2016, 7, 9666–9679. [Google Scholar] [CrossRef]
- Amin, S.B.; Yip, W.K.; Minvielle, S.; Broyl, A.; Li, Y.; Hanlon, B.; Swanson, D.; Shah, P.K.; Moreau, P.; Van Der Holt, B.; et al. Gene expression profile alone is inadequate in predicting complete response in multiple myeloma. Leukemia 2014, 28, 2229–2234. [Google Scholar] [CrossRef]
- Ubels, J.; Sonneveld, P.; van Beers, E.H.; Broijl, A.; van Vliet, M.H.; de Ridder, J. Predicting treatment benefit in multiple myeloma through simulation of alternative treatment effects. Nat. Commun. 2018, 9, 2943. [Google Scholar] [CrossRef]
- Broyl, A.; Hose, D.; Lokhorst, H.; de Knegt, Y.; Peeters, J.; Jauch, A.; Bertsch, U.; Buijs, A.; Stevens-Kroef, M.; Beverloo, H.B.; et al. Gene expression profiling for molecular classification of multiple myeloma in newly diagnosed patients. Blood 2010, 116, 2543–2553. [Google Scholar] [CrossRef]
- Zhan, F.; Huang, Y.; Colla, S.; Stewart, J.P.; Hanamura, I.; Gupta, S.; Epstein, J.; Yaccoby, S.; Sawyer, J.; Burington, B.; et al. The molecular classification of multiple myeloma. Blood 2006, 108, 2020–2028. [Google Scholar] [CrossRef]
- Goldman, M.; Craft, B.; Swatloski, T.; Cline, M.; Morozova, O.; Diekhans, M.; Haussler, D.; Zhu, J. The UCSC Cancer Genomics Browser: Update 2015. Nucleic Acids Res. 2015, 43, D812–D817. [Google Scholar] [CrossRef] [PubMed]
- Walz, A.L.; Ooms, A.; Gadd, S.; Gerhard, D.S.; Smith, M.A.; Guidry Auvil, J.M.; Meerzaman, D.; Chen, Q.-R.; Hsu, C.H.; Yan, C.; et al. Recurrent DGCR8, DROSHA, and SIX Homeodomain Mutations in Favorable Histology Wilms Tumors. Cancer Cell 2015, 27, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Tricoli, J.V.; Blair, D.G.; Anders, C.K.; Bleyer, W.A.; Boardman, L.A.; Khan, J.; Kummar, S.; Hayes-Lattin, B.; Hunger, S.P.; Merchant, M.; et al. Biologic and clinical characteristics of adolescent and young adult cancers: Acute lymphoblastic leukemia, colorectal cancer, breast cancer, melanoma, and sarcoma: Biology of AYA Cancers. Cancer 2016, 122, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Korde, L.A.; Lusa, L.; McShane, L.; Lebowitz, P.F.; Lukes, L.; Camphausen, K.; Parker, J.S.; Swain, S.M.; Hunter, K.; Zujewski, J.A. Gene expression pathway analysis to predict response to neoadjuvant docetaxel and capecitabine for breast cancer. Breast Cancer Res. Treat. 2010, 119, 685–699. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Larionov, A. Changes in expression of oestrogen regulated and proliferation genes with neoadjuvant treatment highlight heterogeneity of clinical resistance to the aromatase inhibitor, letrozole. Breast Cancer Res. BCR 2010, 12, R52. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Larionov, A.; Anderson, T.J.; Evans, D.B.; Dixon, J.M. Sequential changes in gene expression profiles in breast cancers during treatment with the aromatase inhibitor, letrozole. Pharm. J. 2012, 12, 10–21. [Google Scholar] [CrossRef]
- Popovici, V.; Chen, W.; Gallas, B.G.; Hatzis, C.; Shi, W.; Samuelson, F.W.; Nikolsky, Y.; Tsyganova, M.; Ishkin, A.; Nikolskaya, T.; et al. Effect of training-sample size and classification difficulty on the accuracy of genomic predictors. Breast Cancer Res. BCR 2010, 12, R5. [Google Scholar] [CrossRef]
- Iwamoto, T.; Bianchini, G.; Booser, D.; Qi, Y.; Coutant, C.; Shiang, C.Y.-H.; Santarpia, L.; Matsuoka, J.; Hortobagyi, G.N.; Symmans, W.F.; et al. Gene pathways associated with prognosis and chemotherapy sensitivity in molecular subtypes of breast cancer. J. Natl. Cancer Inst. 2011, 103, 264–272. [Google Scholar] [CrossRef]
- Miyake, T.; Nakayama, T.; Naoi, Y.; Yamamoto, N.; Otani, Y.; Kim, S.J.; Shimazu, K.; Shimomura, A.; Maruyama, N.; Tamaki, Y.; et al. GSTP1 expression predicts poor pathological complete response to neoadjuvant chemotherapy in ER-negative breast cancer. Cancer Sci. 2012, 103, 913–920. [Google Scholar] [CrossRef]
- Liu, J.C.; Voisin, V.; Bader, G.D.; Deng, T.; Pusztai, L.; Symmans, W.F.; Esteva, F.J.; Egan, S.E.; Zacksenhaus, E. Seventeen-gene signature from enriched Her2/Neu mammary tumor-initiating cells predicts clinical outcome for human HER2+:ERα- breast cancer. Proc. Natl. Acad. Sci. USA 2012, 109, 5832–5837. [Google Scholar] [CrossRef]
- Shen, K.; Qi, Y.; Song, N.; Tian, C.; Rice, S.D.; Gabrin, M.J.; Brower, S.L.; Symmans, W.F.; O’Shaughnessy, J.A.; Holmes, F.A.; et al. Cell line derived multi-gene predictor of pathologic response to neoadjuvant chemotherapy in breast cancer: A validation study on US Oncology 02-103 clinical trial. BMC Med. Genom. 2012, 5, 51. [Google Scholar] [CrossRef] [PubMed]
- Raponi, M.; Harousseau, J.-L.; Lancet, J.E.; Löwenberg, B.; Stone, R.; Zhang, Y.; Rackoff, W.; Wang, Y.; Atkins, D. Identification of molecular predictors of response in a study of tipifarnib treatment in relapsed and refractory acute myelogenous leukemia. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2007, 13, 2254–2260. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, A.K.; Arthur, L.M.; Renshaw, L.; Larionov, A.A.; Kay, C.; Dunbier, A.K.; Thomas, J.S.; Dowsett, M.; Sims, A.H.; Dixon, J.M. Accurate Prediction and Validation of Response to Endocrine Therapy in Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 2270–2278. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, K.; Czerwi?ska, P.; Wiznerowicz, M. The Cancer Genome Atlas (TCGA): An immeasurable source of knowledge. Contemp. Oncol. Pozn. Pol. 2015, 19, A68–A77. [Google Scholar] [CrossRef]
- Yuan, Y.; Shi, Y.; Li, C.; Kim, J.; Cai, W.; Han, Z.; Feng, D.D. DeepGene: An advanced cancer type classifier based on deep learning and somatic point mutations. BMC Bioinform. 2016, 17, 476. [Google Scholar] [CrossRef]
- Yuan, Y.; Shi, Y.; Su, X.; Zou, X.; Luo, Q.; Feng, D.D.; Cai, W.; Han, Z.-G. Cancer type prediction based on copy number aberration and chromatin 3D structure with convolutional neural networks. BMC Genom. 2018, 19, 565. [Google Scholar] [CrossRef]
- Huang, Z.; Johnson, T.S.; Han, Z.; Helm, B.; Cao, S.; Zhang, C.; Salama, P.; Rizkalla, M.; Yu, C.Y.; Cheng, J.; et al. Deep learning-based cancer survival prognosis from RNA-seq data: Approaches and evaluations. BMC Med. Genom. 2020, 13, 41. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Bartlett, P.; Shawe-taylor, J. Generalization Performance of Support Vector Machines and Other Pattern Classifiers. Adv. Kernel Methods Support Vector Learn. 1999, 43–54. [Google Scholar]
- Vapnik, V.; Chapelle, O. Bounds on Error Expectation for Support Vector Machines. Neural Comput. 2000, 12, 2013–2036. [Google Scholar] [CrossRef]
- Altman, N.S. An Introduction to Kernel and Nearest-Neighbor Nonparametric Regression. Am. Stat. 1992, 46, 175–185. [Google Scholar] [CrossRef]
- Toloşi, L.; Lengauer, T. Classification with correlated features: Unreliability of feature ranking and solutions. Bioinformatics 2011, 27, 1986–1994. [Google Scholar] [CrossRef] [PubMed]
- Tikhonov, A.; Yakovlevich Arsenin, V. Solutions of Ill-Posed Problems; Springer: Berlin/Heidelberg, Germany, 1977. [Google Scholar]
- Webb, G.I.; Boughton, J.R.; Wang, Z. Not So Naive Bayes: Aggregating One-Dependence Estimators. Mach. Learn. 2005, 58, 5–24. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, H.; Wu, Z.; Wang, T.; Li, W.; Tang, Y.; Liu, G. In Silico Prediction of Blood-Brain Barrier Permeability of Compounds by Machine Learning and Resampling Methods. ChemMedChem 2018, 13, 2189–2201. [Google Scholar] [CrossRef] [PubMed]
- Yosipof, A.; Guedes, R.C.; García-Sosa, A.T. Data Mining and Machine Learning Models for Predicting Drug Likeness and Their Disease or Organ Category. Front. Chem. 2018, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Prados, J.; Kalousis, A.; Sanchez, J.-C.; Allard, L.; Carrette, O.; Hilario, M. Mining mass spectra for diagnosis and biomarker discovery of cerebral accidents. Proteomics 2004, 4, 2320–2332. [Google Scholar] [CrossRef]
- Marvin, M.; Seymour, A. Papert Perceptrons—Expanded Edition: An Introduction to Computational Geometry; MIT Press: Boston, MA, USA, 1987. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Lisacek, F.; Sanchez, J.-C.; Müller, M. Bioinformatics for protein biomarker panel classification: What is needed to bring biomarker panels into in vitro diagnostics? Expert Rev. Proteom. 2009, 6, 675–689. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Müller, A.; Nothman, J.; Louppe, G.; et al. Scikit-learn: Machine Learning in Python. arXiv 2012, arXiv:12010490 Cs. [Google Scholar]
- Ioannidis, J.P.A.; Hozo, I.; Djulbegovic, B. Optimal type I and type II error pairs when the available sample size is fixed. J. Clin. Epidemiol. 2013, 66, 903–910. [Google Scholar] [CrossRef]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Type I and type II errors in statistical decision. Restor. Dent. Endod. 2015, 40, 249. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Qiu, Y.; Deng, A. A note on Type S/M errors in hypothesis testing. Br. J. Math. Stat. Psychol. 2019, 72, 1–17. [Google Scholar] [CrossRef]
- Cummins, R.O.; Hazinski, M.F. Guidelines based on fear of type II (false-negative) errors : Why we dropped the pulse check for lay rescuers. Circulation 2000, 102, I377–I379. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, P.; Maestre, Z.; Martinez-Madrid, M.; Reynoldson, T.B. Evaluating the Type II error rate in a sediment toxicity classification using the Reference Condition Approach. Aquat. Toxicol. 2011, 101, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Borisov, N.; Shabalina, I.; Tkachev, V.; Sorokin, M.; Garazha, A.; Pulin, A.; Eremin, I.I.; Buzdin, A. Shambhala: A platform-agnostic data harmonizer for gene expression data. BMC Bioinform. 2019, 20, 66. [Google Scholar] [CrossRef]
- Borisov, N.; Sorokin, M.; Zolotovskaya, M.; Borisov, C.; Buzdin, A. Shambhala-2: A Protocol for Uniformly Shaped Harmonization of Gene Expression Profiles of Various Formats. Curr. Protoc. 2022, 2, e444. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Dataset ID | Disease Type | Treatment | Experimental Platform | Number NC of Cases (R vs. NR) | Number S of Core Marker Genes |
|---|---|---|---|---|---|---|
| [22,23] | GSE25066 | Breast cancer with different hormonal and HER2 status | Neoadjuvant taxane + anthracycline | Affymetrix Human Genome U133 Array | 235 (118 R: Complete response + partial response; 117 NR: Residual disease + progressive disease) | 20 |
| [24] | GSE41998 | Breast cancer with different hormonal and HER2 status | Neoadjuvant doxorubicin + cyclophosphamide, followed by paclitaxel | Affymetrix Human Genome U133 Array | 68 (34 R: Complete response + partial response; 34 NR: Residual disease + progressive disease) | 11 |
| [25] | GSE9782 | Multiple myeloma | Bortezomib monotherapy | Affymetrix Human Genome U133 Array | 169 (85 R: Complete response + partial response; 84 NR: No change + progressive disease) | 18 |
| [26] | GSE39754 | Multiple myeloma | Vincristine + adriamycin + dexamethasone followed by autologous stem cell transplantation (ASCT) | Affymetrix Human Exon 1.0 ST Array | 124 (62 R: Complete, near-complete, and very good partial responders, 62 NR: Partial, minor, and worse) | 16 |
| [27] | GSE68871 | Multiple myeloma | Bortezomib-thalido-mide-dexamethasone | Affymetrix Human Genome U133 Plus | 98 (49 R: Complete, near-complete, and very good partial responders, 49 NR: Partial, minor, and worse) | 12 |
| [28] | GSE55145 | Multiple myeloma | Bortezomib followed by ASCT | Affymetrix Human Exon 1.0 ST Array | 56 (28 R: Complete, near-complete, and very good partial responders, 28 NR: Partial, minor. and worse) | 14 |
| [5] | https://www.frontiersin.org/articles/10.3389/fonc.2021.652063/full#supplementary-material (accessed on 17 November 2021) | Multiple myeloma | Bortezomib, doxorubicin, and dexamethasone (PAD), or bortezomib, cyclophospha-mide, and dexamethasone (VCD) | RNA sequencing, Illumina HiSeq 3000 | 53 (28 R: complete response + very good partial response; 25 NR: partial response + minimal response) | 8 |
| [29,30] | GSE19784_1 | Multiple myeloma, ISS stage I | Bortezomib, doxorubicin and dexamethasone (PAD) | Affymetrix Human Genome U133 Plus 2.0 Array | 61 (32 R, 29 NR) | 7 |
| [29,30] | GSE19784_2 | Multiple myeloma, ISS stage II | Bortezomib, doxorubicin and dexamethasone (PAD) | Affymetrix Human Genome U133 Plus 2.0 Array | 51 (33 R, 18 NR) | 12 |
| [29,30] | GSE19784_3 | Multiple myeloma, ISS stage III | Bortezomib, doxorubicin and dexamethasone (PAD) | Affymetrix Human Genome U133 Plus 2.0 Array | 41 (29 R, 12 NR) | 11 |
| [29,31] | GSE2658 | Multiple myeloma | Bortezomib, doxorubicin and dexamethasone (PAD) | Affymetrix Human Genome U133 Plus 2.0 Array | 208 (55 R, 153 NR) | 16 |
| [32,33] | TARGET-50 | Pediatric kidney Wilms tumor | Vincristine sulfate + cyclosporine, cytarabine, daunorubicin + conventional surgery + radiation therapy | Illumina HiSeq 2000 | 72 (36 R, 36 NR) | 14 |
| [32,34] | TARGET-10 | Pediatric acute lymphoblastic leukemia | Vincristine sulfate + carboplatin, cyclophosphamide, doxorubicin | Illumina HiSeq 2000 | 60 (30 R, 30 NR) | 14 |
| [32] | TARGET-20 | Pediatric acute myeloid leukemia | Non-target drugs (asparaginase, cyclosporine, cytarabine, daunorubicin, etoposide; methotrexate, mitoxantrone), including busulfan and cyclophosphamide | Illumina HiSeq 2000 | 46 (23 R, 23 NR) | 10 |
| [32] | TARGET-20 | Pediatric acute myeloid leukemia | Same non-target drugs, but excluding busulfan and cyclophosphamide | Illumina HiSeq 2000 | 124 (62 R, 62 NR) | 16 |
| [35] | GSE18728 | Breast cancer | Docetaxel, capecitabine | Affymetrix Human Genome U133 Plus 2.0 Array | 61 (23R: Complete response + partial response; 38 NR: Residual disease + progressive disease) | 16 |
| [36,37] | GSE20181 | Breast cancer | Letrozole | Affymetrix Human Genome U133A Array | 52 (37 R: Complete response + partial response; 15 NR: Residual disease + progressive disease) | 11 |
| [38] | GSE20194 | Breast cancer | Paclitaxel; (tri)fluoroacetyl chloride; 5-fluorouracil, epirubicin, cyclophosphamide | Affymetrix Human Genome U133A Array | 52 (11 R: Complete response + partial response; 41 NR: Residual disease + progressive disease) | 10 |
| [39] | GSE23988 | Breast cancer | Docetaxel, capecitabine | Affymetrix Human Genome U133A Array | 61 (20 R: Complete response + partial response; 41 NR: Residual disease + progressive disease) | 18 |
| [40] | GSE32646 | Breast cancer | Paclitaxel, 5-fluorouracil, epirubicin, cyclophosphamide | Affymetrix Human Genome U133 Plus 2.0 Array | 115 (27 R: Complete response + partial response; 88 NR: Residual disease + progressive disease) | 17 |
| [41] | GSE37946 | Breast cancer | Trastuzumab | Affymetrix Human Genome U133A Array | 50 (27 R: Complete response + partial response; 23 NR: Residual disease + progressive disease) | 14 |
| [42] | GSE42822 | Breast cancer | Docetaxel, 5-fluorouracil, epirubicin, cyclophosphamide, capecitabine | Affymetrix Human Genome U133A Array | 91 (38 R: Complete response + partial response; 53 NR: Residual disease + progressive disease) | 13 |
| [43] | GSE5122 | Acute myeloid leukemia | Tipifarnib | Affymetrix Human Genome U133A Array | 57 (13 R: Complete response + partial response + stable disease; 44 R: Progressive disease) | 10 |
| [44] | GSE59515 | Breast cancer | Letrozole | Illumina HumanHT-12 V4.0 expression beadchip | 75 (51 R: Complete response + partial response; 24 NR: Residual disease + progressive disease) | 15 |
| [45] | TCGA-LGG | Low-grade glioma | Temozolomide + (optionally) mibefradil | Illumina HiSeq 2000 | 131 (100 R: Complete response + partial response + stable disease; 31 NR: Progressive disease) | 9 |
| [45] | TCGA-LC | Lung cancer | Paclitaxel + (optionally),cisplatin/carboplatin, reolysin | Illumina HiSeq 2000 | 41 (24 R: Complete response + partial response + stable disease; 17 NR: Progressive disease) | 7 |
| ML Method | Method Type | Median AUC without FloWPS | Median AUC with FloWPS | Paired t-Test p-Value for AUC with-vs.-w/o FloWPS | Advantage of FloWPS | Median Sn at B = 4 | Median Sp at B = 0.25 |
|---|---|---|---|---|---|---|---|
| SVM | Global | 0.74 | 0.80 | 1.3 × 10−5 | Yes | 0.45 | 0.42 |
| kNN | Local | 0.76 | 0.75 | 0.53 | No | 0.25 | 0.34 |
| RF | Global | 0.74 | 0.82 | 1.3 × 10−5 | Yes | 0.45 | 0.42 |
| RR | Local | 0.80 | 0.79 | 0.16 | No | 0.36 | 0.41 |
| BNB | Global | 0.77 | 0.82 | 2.7 × 10−4 | Yes | 0.51 | 0.58 |
| ADA | Global | 0.70 | 0.76 | 2.4 × 10−4 | Yes | 0.32 | 0.41 |
| MLP | Global | 0.73 | 0.82 | 6.4 × 10−5 | Yes | 0.53 | 0.53 |
| SVM | RF | RR | BNB | MLP | |
|---|---|---|---|---|---|
| SVM | 1 | 0.53/0.34 | 0.40/0.19 | 0.37/0.24 | 0.46/0.33 |
| RF | 0.55/0.40 | 1 | 0.51/0.35 | 0.48/0.33 | 0.590.40 |
| RR | 0.39/0.14 | 0.32/0.04 | 1 | 0.93/0.88 | 0.89/0.76 |
| BNB | 0.34/0.14 | 0.31/0.09 | 0.79/0.64 | 1 | 0.81/0.61 |
| MLP | 0.46/0.30 | 0.38/0.17 | 0.52/0.06 | 0.46/0.12 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borisov, N.; Tkachev, V.; Sorokin, M.; Buzdin, A. FLOating-Window Projective Separator (FloWPS) Machine Learning Approach to Predict Individual Clinical Efficiency of Cancer Drugs. Biol. Life Sci. Forum 2021, 7, 23. https://doi.org/10.3390/ECB2021-10273
Borisov N, Tkachev V, Sorokin M, Buzdin A. FLOating-Window Projective Separator (FloWPS) Machine Learning Approach to Predict Individual Clinical Efficiency of Cancer Drugs. Biology and Life Sciences Forum. 2021; 7(1):23. https://doi.org/10.3390/ECB2021-10273
Chicago/Turabian StyleBorisov, Nicolas, Victor Tkachev, Maxim Sorokin, and Anton Buzdin. 2021. "FLOating-Window Projective Separator (FloWPS) Machine Learning Approach to Predict Individual Clinical Efficiency of Cancer Drugs" Biology and Life Sciences Forum 7, no. 1: 23. https://doi.org/10.3390/ECB2021-10273
APA StyleBorisov, N., Tkachev, V., Sorokin, M., & Buzdin, A. (2021). FLOating-Window Projective Separator (FloWPS) Machine Learning Approach to Predict Individual Clinical Efficiency of Cancer Drugs. Biology and Life Sciences Forum, 7(1), 23. https://doi.org/10.3390/ECB2021-10273