
Short-Term Effects of Eccentric Strength Training on Hematology and Muscle Ultrasound in University Students

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
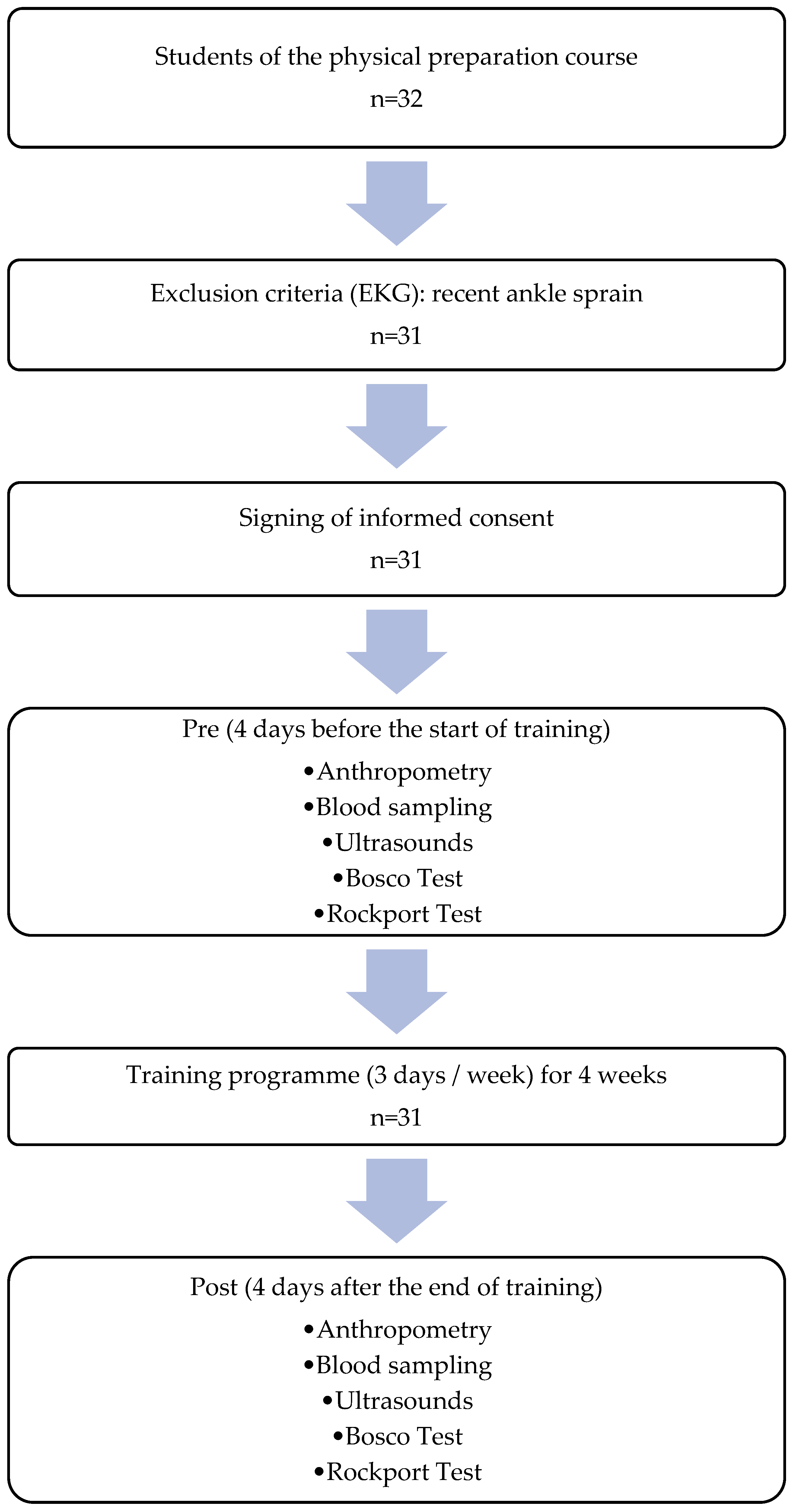
2.1. Participants
2.2. Procedure
2.3. Training Protocol
2.4. Laboratory Test
2.5. Quantitative Ultrasound
2.6. Vertical Jump Tests
2.7. Aerobic Power Test
2.8. Statistical Analysis
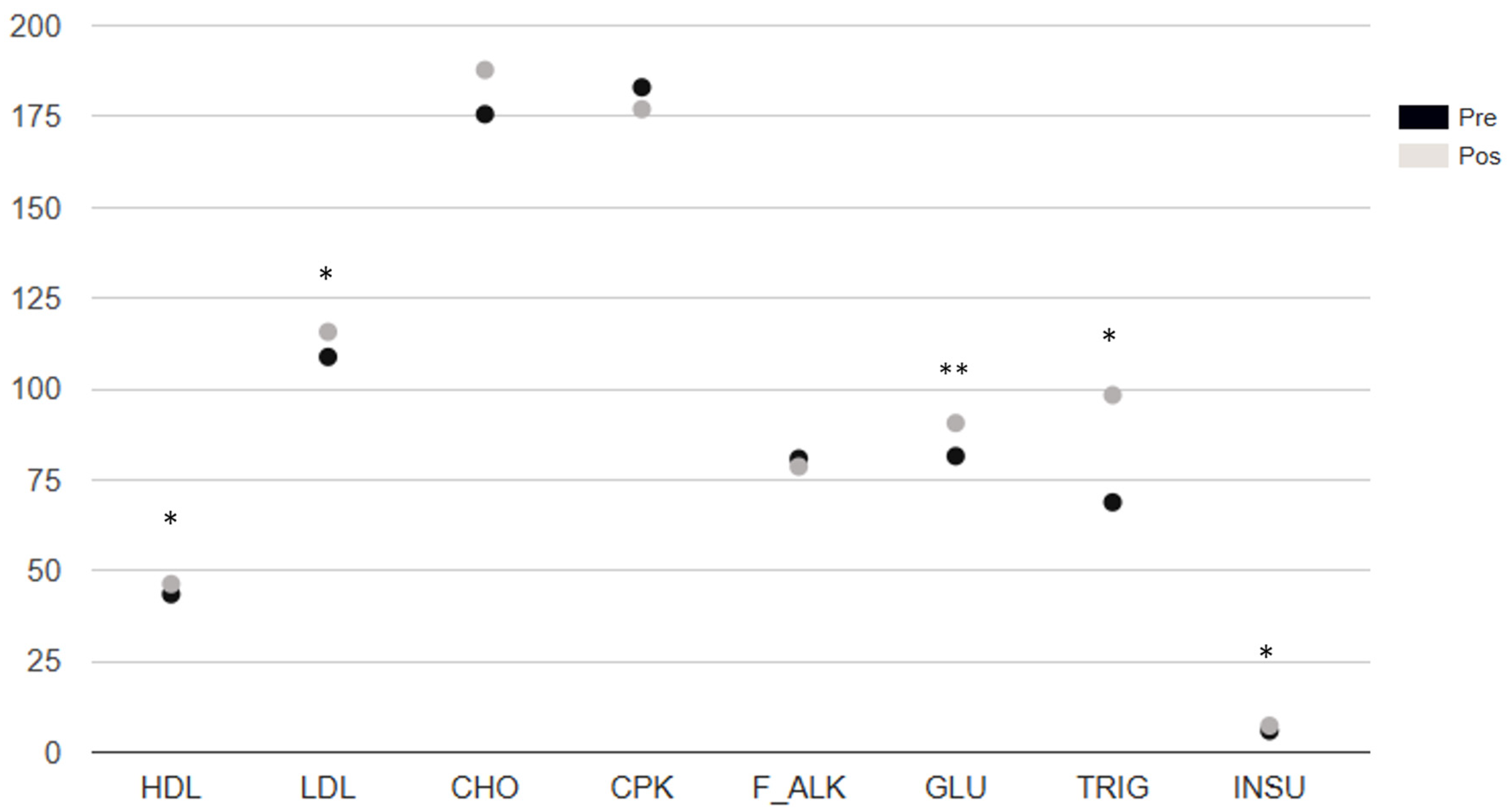
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 1RM | One-repetition maximum |
| A-VIT | Vastus intermedius thickness in the anterior region |
| AEI-SFT | Echo intensity of anterior subcutaneous fat tissue |
| ASFT | Anterior subcutaneous fat tissue thickness |
| ATT | Anterior total thickness |
| Band | Band neutrophils (immature neutrophils) |
| BAS | Basophils |
| BAS_CIT | Citrated basophils |
| BMI | Body mass index |
| CBC | Complete blood count |
| CHO | Total cholesterol |
| CHr | Hemoglobin reticulocytes (CHr) |
| CMJ | Counter movement jump |
| CMJP | Countermovement jump power |
| CMJPR | Relative countermovement jump power |
| CPK | Creatine phosphokinase |
| CRE | Creatinine |
| DAM | Median absolute deviation |
| Dif1 | Anterior fat EI minus RF EI |
| Dif2 | Anterior fat EI minus anterior VI EI |
| Dif3 | Anterior fat EI minus average of RF EI and anterior VI EI |
| Dif4 | Lateral fat EI minus VL EI |
| Dif5 | Anterior fat EI minus lateral VI EI |
| Dif6 | Lateral fat EI minus average of VL EI and lateral VI EI |
| EI | Echo-intensity |
| EI-A-VI | Echo intensity of the vastus intermedius in the anterior region |
| EI-L-VI | Echo intensity of the vastus intermedius in the lateral region |
| EI-RF | Echo intensity of the rectus femoris |
| EI-VL | Echo intensity of the vastus lateralis |
| EOS | Eosinophils |
| F_ALK | Alkaline phosphatase (also abbreviated as ALP) |
| GGT | Gamma-glutamyl transferase |
| GLU | Glucose |
| GRATOX | Toxic granulations |
| HCT | Hematocrit |
| HDL | High-density lipoprotein cholesterol |
| HGB | Hemoglobin |
| HR | Heart rate |
| IMM_GRAN | Immature granulocytes |
| INSU | Insulin |
| L-VIT | Vastus intermedius thickness in the lateral region |
| LDL | Low-density lipoprotein cholesterol |
| LEI-SFT | Echo intensity of the lateral subcutaneous fat tissue |
| LSFT | Lateral subcutaneous fat thickness |
| LTT | Lateral total thickness |
| LYM | Lymphocytes |
| MCH | Mean corpuscular hemoglobin |
| MCHC | Mean corpuscular hemoglobin concentration |
| MCV | Mean corpuscular volume |
| MON | Monocytes |
| MOR_PLA | Abnormal platelet morphology |
| MPV | Mean platelet volume |
| MT | Muscle thickness |
| n | Sample size |
| NEU | Neutrophils |
| NRBC | Nucleated red blood cells |
| P-LCR | Platelet large cell ratio |
| PA | Physical activity |
| PA-RF | Pennation angle of the rectus femoris |
| PA-VL | Pennation angle of the vastus lateralis |
| PBAS | Basal protein |
| PCT | Plateletcrit |
| PDW | Platelet distribution width |
| PLCR | Platelet large cell ratio (dup. of ANS) |
| PLT | Platelets |
| RBC | Red blood cells |
| RDW | Red cell distribution width |
| RDW-SD | Red cell distribution width—standard deviation |
| RET-PLT | Reticulated platelets |
| RET# | Reticulocyte count (absolute) |
| RET% | Reticulocyte percentage |
| RF | Rectus femoris |
| RFT | Rectus femoris thickness |
| SD | Standard deviation |
| SJ | Squat jump |
| SJP | Power of the squat jump |
| SJPR | Relative squat jump power |
| TRIG | Triglycerides |
| TUT | Total time under tension |
| US | Ultrasound |
| VL | Vastus lateralis |
| VLT | Vastus lateralis thickness |
| VO2max | Maximum oxygen consumption |
| WBC | White blood cells |
References
- Anand, M., Vaithianathan, K., Saran, K. S., & Prasanna, T. A. (2019). Effect of game specific circuit training and plyometrics on selected physiological and hematological variables of handball players. Indian Journal of Public Health Research & Development, 10(7), 365. [Google Scholar] [CrossRef]
- Benavides-Villanueva, J., & Ramirez-Campillo, R. (2022). Entrenamiento con sobrecarga, duración de la repetición e hipertrofia: Una revisión de la literatura. Revista Ciencias de La Actividad Física, 23(1), 1–13. [Google Scholar] [CrossRef]
- Beqa Ahmeti, G., Idrizovic, K., Elezi, A., Zenic, N., & Ostojic, L. (2020). Endurance training vs. circuit resistance training: Effects on lipid profile and anthropometric/body composition status in healthy young adult women. International Journal of Environmental Research and Public Health, 17(4), 1222. [Google Scholar] [CrossRef]
- Bompa, T., & Buzzichelli, C. (2015). Periodization training for sports (3rd ed.). Human kinetics. [Google Scholar]
- Calderón, J. (2007). Fisiología aplicada al deporte. Editorial Tébar. [Google Scholar]
- Carbone, S., Kirkman, D. L., Garten, R. S., Rodriguez-Miguelez, P., Artero, E. G., Lee, D. C., & Lavie, C. J. (2020). Muscular strength and cardiovascular disease. Journal of Cardiopulmonary Rehabilitation and Prevention, 40(5), 302–309. [Google Scholar] [CrossRef]
- Chalapud Narváez, L. M., & Molano Tobar, N. J. (2021). Nivel de actividad física en universitarios de Popayán. Revista Cubana de Investigaciones Biomédicas, 40(4). Available online: https://revibiomedica.sld.cu/index.php/ibi/article/view/1083 (accessed on 3 July 2025).
- Dolgener, F. A., Hensley, L. D., Marsh, J. J., & Fjelstul, J. K. (1994). Validation of the rockport fitness walking test in college males and females. Research Quarterly for Exercise and Sport, 65(2), 152–158. [Google Scholar] [CrossRef]
- Franchi, M. V., Reeves, N. D., & Narici, M. V. (2017). Skeletal muscle remodeling in response to eccentric vs. concentric loading: Morphological, molecular, and mesolic adaptations. Frontiers in Physiology, 8, 447. [Google Scholar] [CrossRef]
- Gentil, P., Soares, S., & Bottaro, M. (2015). Single vs. multi-joint resistance exercises: Effects on muscle strength and hypertrophy. Asian Journal of Sports Medicine, 6(1). [Google Scholar] [CrossRef]
- Harput, G., Toprak, U., Colakoglu, F. F., Temel, E., Saylisoy, S., & Baltaci, G. (2023). Effects of plyometric training on sonographic characteristics of quadriceps muscle and patellar tendon, quadriceps strength, and jump height in adolescent female volleyball players. International Journal of Athletic Therapy and Training, 28(2), 89–96. [Google Scholar] [CrossRef]
- He, M., Hu, S., Wang, J., Wang, J., Găman, M. A., Hariri, Z., & Tian, Y. (2023). Effect of resistance training on lipid profile in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. European Journal of Obstetrics & Gynecology and Reproductive Biology, 288, 18–28. [Google Scholar] [CrossRef]
- Ibis, S., Hazar, S., & Demirci, I. (2012). The effect of plyometric training on hematological parameters in alpine skiers. Age (Years), 12(17). Available online: https://sportspa.ftos.untz.ba/index.php/sportspa/article/view/87/80 (accessed on 3 July 2025).
- Kleinberg, C. R., Ryan, E. D., Tweedell, A. J., Barnette, T. J., & Wagoner, C. W. (2016). Influence of lower extremity muscle size and quality on stair-climb performance in career firefighters. Journal of Strength and Conditioning Research, 30(6), 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa-Nowak, D., Nowakowska, A., Zwierko, T., Rybak, M., & Nowak, R. (2020). The influence of a health-related fitness training program on motor performance as well as hematological and biochemical parameters. International Journal of Environmental Research and Public Health, 17(2), 578. [Google Scholar] [CrossRef]
- Kraemer, W. J., & Ratamess, N. A. (2004). Fundamentals of resistance training: Progression and exercise prescription. Medicine & Science in Sports & Exercise, 36(4), 674–688. [Google Scholar] [CrossRef]
- Kudo, S., Sato, T., & Miyashita, T. (2020). Effect of plyometric training on the fascicle length of the gastrocnemius medialis muscle. Journal of Physical Therapy Science, 32(4), 277–280. [Google Scholar] [CrossRef]
- Küçük Yetgin, M., Agopyan, A., Küçükler, F. K., Gedikbaşı, A., Yetgin, S., Çelik Kayapınar, F., Özbar, N., Biçer, B., & Çotuk, H. B. (2020). The effects of resistance and aerobic exercises on adiponectin, insulin resistance, lipid profile and body composition in adolescent boys with obesity. Istanbul Medical Journal, 21(3), 182–189. [Google Scholar] [CrossRef]
- Lakićević, N. (2019). The effects of alcohol consumption on recovery following resistance exercise: A systematic review. Journal of Functional Morphology and Kinesiology, 4(3), 41. [Google Scholar] [CrossRef]
- Lorenzo, L. R., Del Olmo, M. F., Molina, J. S., & Acero, R. M. (2020). Criterios observables para la ejecución de pruebas de salto vertical: SJ, CMJ, CMJA, 1RJA. Revista de Entrenamiento Deportivo [Internet], 34. Available online: https://portalinvestigacion.udc.gal/documentos/608ca9d8af765575d40b1fb8 (accessed on 3 July 2025).
- López Chicharro, J. L., & Mojares, L. M. L. (2008). Fisiología Clínica del Ejercicio. Editorial Médica Panamericana. [Google Scholar]
- Lum, D., Tan, F., Pang, J., & Barbosa, T. M. (2019). Effects of intermittent sprint and plyometric training on endurance running performance. Journal of Sport and Health Science, 8(5), 471–477. [Google Scholar] [CrossRef]
- Makaruk, H., Winchester, J. B., Sadowski, J., Czaplicki, A., & Sacewicz, T. (2011). Effects of unilateral and bilateral plyometric training on power and jumping ability in women. Journal of Strength and Conditioning Research, 25(12), 3311–3318. [Google Scholar] [CrossRef]
- Mangine, G. T., Fukuda, D. H., LaMonica, M. B., Wells, A. J., Townsend, J. R., Jajtner, A. R., Fragala, M. S., Stout, J. R., & Hoffman, J. R. (2014). Influence of gender and muscle architecture asymmetry on jump and sprint performance. Journal of Sports Science & Medicine, 13(4), 904–911. [Google Scholar]
- Marcon, M., Ciritsis, B., Laux, C., Nanz, D., Nguyen-Kim, T. D. L., Fischer, M. A., Andreisek, G., & Ulbrich, E. J. (2015). Cross-sectional area measurements versus volumetric assessment of the quadriceps femoris muscle in patients with anterior cruciate ligament reconstructions. European Radiology, 25(2), 290–298. [Google Scholar] [CrossRef] [PubMed]
- Marušič, J., Vatovec, R., Marković, G., & Šarabon, N. (2020). Effects of eccentric training at long-muscle length on architectural and functional characteristics of the hamstrings. Scandinavian Journal of Medicine & Science in Sports, 30(11), 2130–2142. [Google Scholar] [CrossRef]
- Mazzetti, S. A., Kraemer, W. J., Volek, J. S., Duncan, N. D., Ratamess, N. A., Gómez, A. L., Newton, R. U., Hakkinen, K., & Fleck, S. J. (2000). The influence of direct supervision of resistance training on strength performance. Medicine & Science in Sports & Exercise, 32(6), 1175–1184. [Google Scholar] [CrossRef]
- Menon, M. K., Houchen, L., Harrison, S., Singh, S. J., Morgan, M. D., & Steiner, M. C. (2012). Ultrasound assessment of lower limb muscle mass in response to resistance training in COPD. Respiratory Research, 13(1), 119. [Google Scholar] [CrossRef]
- Monti, E., Franchi, M. V., Badiali, F., Quinlan, J. I., Longo, S., & Narici, M. V. (2020). The time-course of changes in muscle mass, architecture and power during 6 weeks of plyometric training. Frontiers in Physiology, 11, 946. [Google Scholar] [CrossRef]
- Mota, J. A., Stock, M. S., & Thompson, B. J. (2017). Vastus lateralis and rectus femoris echo intensity fail to reflect knee extensor specific tension in middle-school boys. Physiological Measurement, 38(8), 1529–1541. [Google Scholar] [CrossRef]
- Murray, C. J. L., Lauer, J. A., Hutubessy, R. C. W., Niessen, L., Tomijima, N., Rodgers, A., Lawes, C. M. M., & Evans, D. B. (2003). Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: A global and regional analysis on reduction of cardiovascular-disease risk. The Lancet, 361(9359), 717–725. [Google Scholar] [CrossRef]
- Nourshahi, M., Rostami, S., & Nazari, N. (2024). The impact of alcohol consumption on resistance training-induced muscle hypertrophy and alcohol-induced cardiomyopathy. Journal of Sport and Exercise Physiology, 17(2), 109–129. [Google Scholar]
- Proske, U., & Morgan, D. L. (2001). Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. The Journal of Physiology, 537(2), 333–345. [Google Scholar] [CrossRef]
- Ramírez-delaCruz, M., Bravo-Sánchez, A., Esteban-García, P., Jiménez, F., & Abián-Vicén, J. (2022). Effects of plyometric training on lower body muscle architecture, tendon structure, stiffness and physical performance: A systematic review and meta-analysis. Sports Medicine-Open, 8(1), 40. [Google Scholar] [CrossRef] [PubMed]
- Reimers, K., Reimers, C. D., Wagner, S., Paetzke, I., & Pongratz, D. E. (1993). Skeletal muscle sonography: A correlative study of echogenicity and morphology. Journal of Ultrasound in Medicine, 12(2), 73–77. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, A., Cardona, D., & Ruiz, G. (2022). Programa de entrenamiento de la zona core en fútbol. In En Ciencias del deporte y de la actividad física (pp. 113–154). Kinesis. [Google Scholar]
- Santos, R., & Armada-da-Silva, P. A. S. (2017). Reproducibility of ultrasound-derived muscle thickness and echo-intensity for the entire quadriceps femoris muscle. Radiography, 23(3), e51–e61. [Google Scholar] [CrossRef] [PubMed]
- Saran, K. S., Vaithianathan, K., Anand, M., & Prasanna, T. A. (2019). Isolated and combined effect of plyometric and weight training on selected physical fitness and hematological variables of football players. Indian Journal of Public Health Research & Development, 10(7), 362. [Google Scholar] [CrossRef]
- Sarkar, S., Dasgupta, S., Meitei, K. K., Adhikari, S., Bandyopadhyay, A., & Dey, S. K. (2020). Effect of eccentric cycling and plyometric training on physiological and performance related parameters of trained junior track cyclists. Polish Journal of Sport and Tourism, 27(1), 14–20. [Google Scholar] [CrossRef]
- Sarto, F., Spörri, J., Fitze, D. P., Quinlan, J. I., Narici, M. V., & Franchi, M. V. (2021). Implementing ultrasound imaging for the assessment of muscle and tendon properties in elite sports: Practical aspects, methodological considerations and future directions. Sports Medicine, 51(6), 1151–1170. [Google Scholar] [CrossRef]
- Sayers, S. P., Harackiewicz, D. V., Harman, E. A., Frykman, P. N., & Rosenstein, M. T. (1999). Cross-validation of three jump power equations. Medicine & Science in Sports & Exercise, 31(4), 572–577. [Google Scholar] [CrossRef]
- Schobersberger, W., Tschann, M., Hasibeder, W., Steidl, M., Herold, M., Nachbauer, W., & Koller, A. (1990). Consequences of 6 weeks of strength training on red cell O2 transport and iron status. European Journal of Applied Physiology and Occupational Physiology, 60(3), 163–168. [Google Scholar] [CrossRef]
- Schoenfeld, B. J. (2010). The mechanisms of muscle hypertrophy and their application to resistance training. Journal of Strength and Conditioning Research, 24(10), 2857–2872. [Google Scholar] [CrossRef]
- Stock, M. S., & Thompson, B. J. (2021). Echo intensity as an indicator of skeletal muscle quality: Applications, methodology, and future directions. European Journal of Applied Physiology, 121(2), 369–380. [Google Scholar] [CrossRef]
- Tambalis, K., Panagiotakos, D. B., Kavouras, S. A., & Sidossis, L. S. (2009). Responses of blood lipids to aerobic, resistance, and combined aerobic with resistance exercise training: A systematic review of current evidence. Angiology, 60(5), 614–632. [Google Scholar] [CrossRef] [PubMed]
- Verkhoshansky, Y., & Siff, M. C. (2009). Supertraining. Verkhoshansky SSTM. [Google Scholar]
- Wernbom, M., Augustsson, J., & Thomeé, R. (2007). The influence of frequency, intensity, volume and mode of strength training on whole muscle cross-sectional area in humans. Sports Medicine, 37(3), 225–264. [Google Scholar] [CrossRef] [PubMed]
- Wilk, M., Gepfert, M., Krzysztofik, M., Golas, A., Mostowik, A., Maszczyk, A., & Zajac, A. (2019). The influence of grip width on training volume during the bench press with different movement tempos. Journal of Human Kinetics, 68(1), 49–57. [Google Scholar] [CrossRef] [PubMed]
- Wu, J. S., Darras, B. T., & Rutkove, S. B. (2010). Assessing spinal muscular atrophy with quantitative ultrasound. Neurology, 75(6), 526–531. [Google Scholar] [CrossRef]
- Yang, Y., Bay, P. B., Wang, Y. R., Huang, J., Teo, H. W. J., & Goh, J. (2018). Effects of consecutive versus non-consecutive days of resistance training on strength, body composition, and red blood cells. Frontiers in Physiology, 9, 725. [Google Scholar] [CrossRef]
- Young, H., Jenkins, N. T., Zhao, Q., & Mccully, K. K. (2015). Measurement of intramuscular fat by muscle echo intensity. Muscle & Nerve, 52(6), 963–971. [Google Scholar] [CrossRef]
- Zatsiorsky, V. M., Kraemer, W. J., & Fry, A. C. (2020). Science and practice of strength training. Human kinetics. [Google Scholar]
- Zhu, X.-Y., Shi, M.-Q., Jiang, Z.-M., Xiao-Li, Tian, J.-W., & Su, F.-F. (2025). Global, regional, and national burden of cardiovascular diseases attributable to metabolic risks across all age groups from 1990 to 2021: An analysis of the 2021 global burden of disease study data. BMC Public Health, 25, 1704. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Phase | Days | % 1RM | Sets | Repetitions | Reference |
|---|---|---|---|---|---|
| 1 | 1–6 | 60–70% | 4–5 | 10–12 | (Bompa & Buzzichelli, 2015) |
| 2 | 7–9 | 70–80% | 4–5 | 8–10 | (Schoenfeld, 2010) |
| 3 | 10–12 | 80–90% | 5–6 | 5–6 | (Zatsiorsky et al., 2020) |
| 4 | 13–18 * | 85–95% | 4–5 | 4–5 | (Verkhoshansky & Siff, 2009) |
| Description | Value |
|---|---|
| n | 31 |
| Age (years) (Mean ± SD) | 22.3 ± 4.14 |
| Height (metres) (Mean ± SD) | 1.73 ± 0.08 |
| Body Mass (kg) (Median ± MAD | 69 ± 13.64 |
| BMI (kg/mÂ2) (Median ± MAD) | 23.54 ± 3.34 |
| Ultrasound | Before | After | p-Value * | ES | ||
|---|---|---|---|---|---|---|
| M | MAD | M | MAD | |||
| ASFT | 5.12 | 3.05 | 5.69 | 3.56 | 0.8279 | 0.041 |
| RFT | 25.93 | 4.05 | 27.37 | 5.46 | 0.0044 ** | 0.500 |
| A-VIT | 20.45 | 2.94 | 21.00 | 3.46 | 0.1589 | 0.255 |
| ATT | 48.06 | 6.91 | 49.08 | 7.41 | 0.0059 ** | 0.484 |
| AEI-SFT | 155.22 | 17.01 | 157.16 | 11.97 | 0.1110 | 0.289 |
| EI-RF | 116.29 | 18.16 | 112.05 | 9.61 | 0.1821 | 0.243 |
| EI-A-VI | 90.05 | 15.88 | 90.38 | 13.67 | 0.9999 | 0 |
| PA-RF | 15.12 | 4.56 | 17.0 | 2.62 | 0.0552 | 0.345 |
| LSFT | 5.06 | 3.23 | 5.60 | 3.29 | 0.8129 | 0.044 |
| VLT | 24.32 | 4.18 | 25.12 | 4.04 | 0.0351 * | 0.377 |
| L-VIT | 20.40 | 4.63 | 19.51 | 4.37 | 0.8204 | 0.042 |
| LTT | 47.59 | 7.99 | 48.58 | 6.52 | 0.0032 ** | 0.516 |
| LEI-SFT | 151.59 | 10.90 | 155.48 | 9.98 | 0.1353 | 0.271 |
| EI-VL | 119.74 | 18.02 | 117.39 | 10.78 | 0.1574 | 0.257 |
| EI-L-VI | 78.47 | 14.62 | 80.03 | 19.12 | 0.3992 | 0.155 |
| PA-VL | 16.13 | 3.59 | 15.65 | 3.19 | 0.9615 | 0.011 |
| Dif1 | 33.0 | 15.54 | 41.17 | 18.32 | <0.0001 ** | 0.686 |
| Dif2 | 67.17 | 15.40 | 71.73 | 21.28 | 0.2241 | 0.222 |
| Dif3 | 49.11 | 14.06 | 55.63 | 13.73 | 0.0027 ** | 0.524 |
| Dif4 | 30.78 | 24.94 | 37.92 | 19.89 | 0.0012 ** | 0.560 |
| Dif5 | 79.52 | 13.80 | 84.10 | 23.02 | 0.8544 | 0.035 |
| Dif6 | 56.65 | 19.27 | 59.77 | 21.54 | 0.1574 | 0.257 |
| Complete Blood Count (CBC) | Before | After | p-Value * | ES | ||
|---|---|---|---|---|---|---|
| M | MAD | M | MAD | |||
| RBC | 5.3 | 0.44 | 5.4 | 0.30 | 0.0513 | 0.350 |
| HGB | 16.0 | 1.19 | 16.2 | 0.89 | 0.0656 | 0.331 |
| HCT | 46.6 | 3.11 | 48.0 | 2.52 | 0.0033 | 0.514 |
| MCV | 88.4 | 3.41 | 89.3 | 3.85 | 0.0015 | 0.549 |
| MCH | 30.0 | 1.33 | 29.9 | 1.33 | 0.9112 | 0.021 |
| MCHC | 33.6 | 0.74 | 33.5 | 0.74 | 0.0459 | 0.358 |
| RDW | 12.8 | 0.74 | 12.3 | 0.59 | 0.0344 | 0.378 |
| WBC | 6590 | 889.5 | 6610 | 1541.9 | 0.4588 | 0.136 |
| NEU | 3596 | 868.8 | 3320 | 948.8 | 0.0734 | 0.322 |
| BAND | 0 | 0 | 0 | 0 | 0.5000 | 0.254 |
| EOS | 170 | 103.8 | 190 | 118.6 | 0.1801 | 0.243 |
| BAS | 40 | 29.65 | 40 | 29.65 | 0.8776 | 0.030 |
| IMN_GRAN | 40 | 29.65 | 40 | 29.65 | 0.6716 | 0.078 |
| LYM | 2220 | 474.43 | 2320 | 548.56 | 0.0585 | 0.340 |
| MON | 510 | 163.09 | 490 | 148.26 | 0.3907 | 0.157 |
| NRBC | 0 | 0 | 0 | 0 | n.a | n.a |
| PLT | 259 | 34.10 | 251 | 32.62 | 0.4353 | 0.143 |
| MPV | 10.1 | 0.74 | 10.1 | 0.74 | 0.9345 | 0.016 |
| PDW | 11.5 | 1.33 | 11.5 | 1.63 | 0.5908 | 0.098 |
| P-LCR | 0 | 0 | 0 | 0 | 0.5000 | 0.254 |
| PCT | 0 | 0 | 0 | 0 | n.a | n.a |
| PLCR | 0 | 0 | 0 | 0 | 0.9999 | 0.104 |
| CRE | 0 | 0 | 0 | 0 | n.a | n.a |
| GGT | 0 | 0 | 0 | 0 | n.a | n.a |
| PBAS | 0 | 0 | 0 | 0 | 0.9999 | 0.180 |
| GRATOX | 0 | 0 | 0 | 0 | 0.9999 | 0.180 |
| BAS_CIT | 0 | 0 | 0 | 0 | 0.5000 | 0.254 |
| MOR_PLA | 0 | 0 | 0 | 0 | 0.9999 | 0 |
| RDW-SD | 41.1 | 1.78 | 40.5 | 1.78 | 0.3196 | 0.181 |
| RET% | 1.5 | 0.44 | 1.3 | 0.30 | 0.0539 | 0.346 |
| RET# | 83.6 | 23.72 | 76.6 | 21.79 | 0.1461 | 0.264 |
| CHr | 36.1 | 2.52 | 35.8 | 3.85 | 0.9999 | 0 |
| RET-plt | 2.8 | 1.33 | 3.0 | 1.19 | 0.0232 | 0.404 |
| Rockport | Before | After | p-Value * | ES | ||
|---|---|---|---|---|---|---|
| M | MAD | M | MAD | |||
| HR | 119 | 19.27 | 132 | 29.65 | 0.2827 | 0.196 |
| VO2max | 52.84 | 7.47 | 54.09 | 8.27 | 0.0167 | 0.426 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, J.C.G.; Echeverri Chica, J.; Campuzano Zuluaga, G.; Ruiz Rengifo, G.M.; Cardona Nieto, D.; Arango, J.C.A.; Ramos-Álvarez, O. Short-Term Effects of Eccentric Strength Training on Hematology and Muscle Ultrasound in University Students. Youth 2025, 5, 72. https://doi.org/10.3390/youth5030072
García JCG, Echeverri Chica J, Campuzano Zuluaga G, Ruiz Rengifo GM, Cardona Nieto D, Arango JCA, Ramos-Álvarez O. Short-Term Effects of Eccentric Strength Training on Hematology and Muscle Ultrasound in University Students. Youth. 2025; 5(3):72. https://doi.org/10.3390/youth5030072
Chicago/Turabian StyleGarcía, Juan Carlos Giraldo, Julián Echeverri Chica, German Campuzano Zuluaga, Gloria María Ruiz Rengifo, Donaldo Cardona Nieto, Juan Cancio Arcila Arango, and Oliver Ramos-Álvarez. 2025. "Short-Term Effects of Eccentric Strength Training on Hematology and Muscle Ultrasound in University Students" Youth 5, no. 3: 72. https://doi.org/10.3390/youth5030072
APA StyleGarcía, J. C. G., Echeverri Chica, J., Campuzano Zuluaga, G., Ruiz Rengifo, G. M., Cardona Nieto, D., Arango, J. C. A., & Ramos-Álvarez, O. (2025). Short-Term Effects of Eccentric Strength Training on Hematology and Muscle Ultrasound in University Students. Youth, 5(3), 72. https://doi.org/10.3390/youth5030072