
Associations between Traumatic Experience and Resilience in Adolescent Refugees: A Scoping Review
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility
- (i)
- Traumatic experience was the independent variable of the study,
- (ii)
- Resilience was an outcome variable of the study,
- (iii)
- Relationship between traumatic experience and resilience was reported,
- (iv)
- Articles had to be peer-reviewed and published in English based on primary data. Articles were published between 1 January 2010, and 20 January 2022. This period is selected because it is called the world refugee crisis time, and most people are unprecedentedly displaced from their country of origin all over the world.
- (v)
- Participants of the study included adolescent refugees or asylum seekers. Adolescents aged between 12–18 of all genders were included in this review.
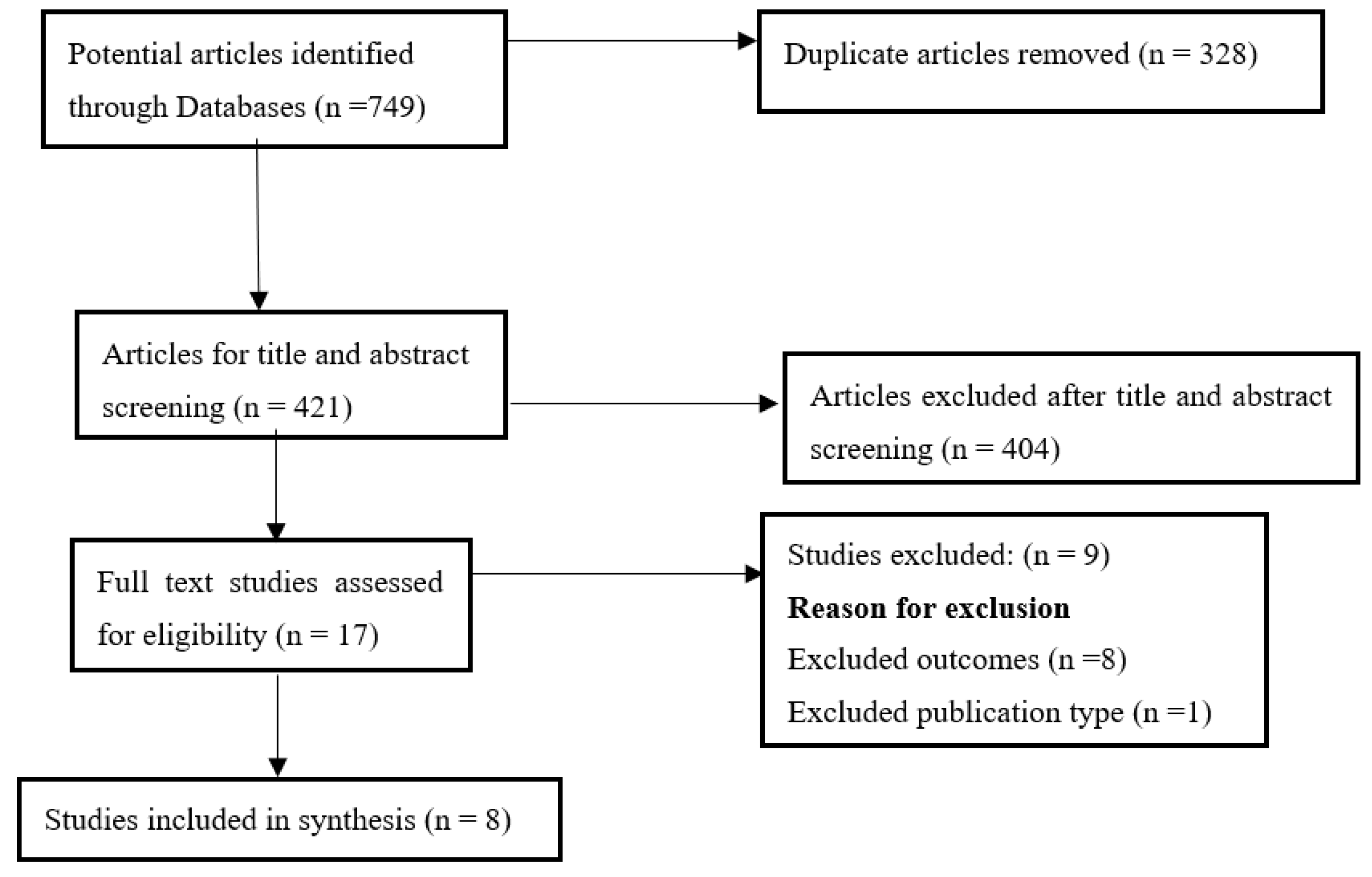
2.2. Search Strategy
2.3. Data Extraction
2.4. Data Synthesis
3. Results
3.1. Determinants of Resilience Factors in Adolescent Refugees
3.2. Relationship between Traumatic Experience and Resilience
4. Discussion
5. Strengths and Limitations
6. Recommendations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anagnostopoulos, D.C.; Heberbrand, J.; Eliez, S.; Doyle, M.B.; Klasen, H.; Crommen, S.F.C.; Pejovic-Milovancevic, M.; Herreros, O.; Minderaa, R.; Karwautz, A.; et al. European Society of Child Adolescent Psychiatry: Position statement on mental health of child and adolescent refugees. Eur. Child Adolesc. Psychiatry 2016, 25, 673–676. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bean, T.; Derluyn, I.; Eurelings-Bontekoe, E.; Broekaert, E.; Spinhoven, P. Comparing psychological distress, traumatic stress reactions, and experiences of unaccompanied refugee minors with experiences of adolescents accompanied by parents. J. Nerv. Ment. Disease 2007, 195, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Sapmaz, Ş.Y.; Tanrıverdi, B.U.; Öztürk, M.; Gözaçanlar, Ö.; Ülker, G.Y.; Özkan, Y. Neuropsychiatric Disease and Treatment Dovepress immigration-related mental health disorders in refugees 5–18 years old living in Turkey. Neuropsychiatr. Dis. Treat. 2017, 13, 2813–2821. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.P. When immigration is trauma: Guidelines for the individual and family clinician. Am. J. Orthopsychiatry 2001, 71, 153–170. [Google Scholar] [CrossRef] [PubMed]
- Charlson, F.; van Ommeren, M.; Flaxman, A.; Cornett, J.; Whiteford, H.; Saxena, S. New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. Lancet 2019, 394, 240–248. [Google Scholar] [CrossRef]
- De Jong, J.T.V.M.; Komproe, I.H.; Van Ommeren, M. Common mental disorders in post conflict settings. Lancet 2003, 361, 2128–2130. [Google Scholar] [CrossRef]
- Nickerson, A.; Liddell, B.; Asnaani, A.; Carlsson, J.; Fazel, M.; Knaevelsrud, C.; Morina, N.; Neuner, F.; Newnham, E.; Rasmussen, A. Trauma and Mental Health in Forcibly Displaced Populations. Int. Soc. Trauma. Stress Stud. 2017, 1–37. Available online: https://www.istss.org/getattachment/Education-Research/Briefing-Papers/Trauma-and-Mental-Health-in-Forcibly-Displaced-Pop/Displaced-Populations-Briefing-Paper (accessed on 1 March 2022).
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; Van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef]
- Vossoughi, N.; Jackson, Y.; Gusler, S.; Stone, K. Mental Health Outcomes for Youth Living in Refugee Camps: A Review. Trauma Violence Abus. 2018, 19, 528–542. [Google Scholar] [CrossRef]
- Zimmerman, C.; Kiss, L.; Hossain, M. Migration and Health: A Framework for 21st Century Policy-Making. PLoS Med. 2011, 8, e1001034. [Google Scholar] [CrossRef]
- Lau, W.; Thomas, T. Research into the psychological well-being of young refugees. Int. Psychiatry 2008, 5, 60–62. [Google Scholar] [CrossRef]
- Fairbank, J.A.; Fairbank, D.W. Epidemiology of child traumatic stress. Curr. Psychiatry Rep. 2009, 11, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.; Ford, K.; Hardcastle, K.; Hopkins, J.; Hughes, K.; Bellis, M.A. Adverse Childhood Experiences in Child Refugee and Asylum-Seeking Populations. 2020. Available online: https://www.wmsmp.org.uk/wp-content/uploads/ACEs-in-Child-Refugee-and-Asylum-Seekers-Report-English-final.pdf (accessed on 30 September 2022).
- Betancourt, T.S.; Khan, K.T. The mental health of children affected by armed conflict: Protective processes and pathways to resilience. Int. Rev. Psychiatry 2008, 20, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Klasen, F.; Oettingen, G.; Daniels, J.; Post, M.; Hoyer, C.; Adam, H. Posttraumatic resilience in former Ugandan child soldiers. Child Dev. 2010, 81, 1096–1113. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S.; Tellegen, A. Resilience in developmental psychopathology: Of the Project Competence Longitudinal Study. Dev. Psychopathol. 2012, 24, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Pieloch, K.A.; McCullough, M.B.; Marks, A.K. Resilience of children with refugee statuses: A research review. Can. Psychol. 2016, 57, 330–339. [Google Scholar] [CrossRef]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 25338. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Dev. Psychopathol. 2011, 23, 493–506. [Google Scholar] [CrossRef]
- Rutter, M. Resilience concepts and findings: Implications for family therapy. J. Fam. Ther. 1999, 21, 119–144. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Masten, A.S.; Hubbard, J.J.; Gest, S.D.; Tellegen, A.; Garmezy, N.; Ramirez, M. Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Dev. Psychopathol. 1999, 11, 143–169. [Google Scholar] [CrossRef] [PubMed]
- Fergus, S.; Zimmerman, M.A. Adolescent resilience: A framework for understanding healthy development in the face of risk. Annu. Rev. Pub. Health 2005, 26, 399–419. [Google Scholar] [CrossRef]
- Barankin, T.; Khanlou, N. Growing Up Resilient: Ways to Build Resilience in Children and Youth. 2007. Available online: https://www.camh.ca/-/media/files/guides-and-publications/2887-growupresil_ins-pdf.pdf (accessed on 30 September 2022).
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- United Nations High Commissioner for Refugees. Trends at a Glance: Global Trends Forced Displacement in 2019. 2020. Available online: https://www.unhcr.org/5ee200e37.pdf (accessed on 2 March 2022).
- Beiser, M.; Dion, R.; Gotowiec, A.; Hyman, I.; Vu, N. Immigrant and refugee children in Canada. Can. J. Psychiatry 1995, 40, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Ziaian, T.; de Anstiss, H.; Antoniou, G.; Baghurst, P.; Sawyer, M. Resilience and Its Association with Depression, Emotional and Behavioural Problems, and Mental Health Service Utilisation among Refugee Adolescents Living in South Australia. Int. J. Popul. Res. 2012, 1–9. [Google Scholar] [CrossRef]
- Murad, K.; Thabet, A.A. The Relationship between Traumatic Experience, Posttraumatic Stress Disorder, Resilience, and Posttraumatic Growth among Adolescents in Gaza Strip. Glob. J. Intellect. Dev. Disabil. 2017, 3, 73–82. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Dehnel, R.; Dalky, H.; Sudarsan, S.; Al-Delaimy, W.K. Resilience and Mental Health Among Syrian Refugee Children in Jordan. J. Immigr. Minor. Health 2022, 24, 420–429. [Google Scholar] [CrossRef]
- Guido, V.; Alessandro, P.; Francesca, G. Child Psychological Adjustment to War and Displacement: A Discriminant Analysis of Resilience and Trauma in Syrian Refugee Children. J. Child Fam. Stud. 2021, 30, 2575–2588. [Google Scholar]
- Kim, Y.J.; Cho, Y.A.; Kim, H.A. A Mediation Effect of Ego Resiliency Between Stresses and Mental Health of North Korean Refugee Youth in South Korea. Child Adolesc. Soc. Work J. 2015, 32, 481–490. [Google Scholar] [CrossRef]
- Mahamid, F.A. Collective Trauma, Quality of Life and Resilience in Narratives of Third Generation Palestinian Refugee Children. Child Indic. Res. 2020, 13, 2181–2204. [Google Scholar] [CrossRef]
- O’connor, K.; Seager, J. Displacement, violence, and mental health: Evidence from rohingya adolescents in cox’s bazar, Bangladesh. Int. J. Environ. Res. Pub. Health 2021, 18, 5318. [Google Scholar] [CrossRef] [PubMed]
- Dangmann, C.; Solberg, Ø.; Myhrene Steffenak, A.K.; Høye, S.; Andersen, P.N. Syrian Refugee Youth Resettled in Norway: Mechanisms of Resilience Influencing Health-Related Quality of Life and Mental Distress. Front. Public Health 2021, 9, 711451. [Google Scholar] [CrossRef] [PubMed]
- Sleijpen, M.; Mooren, T.; Kleber, R.J.; Boeije, H.R. Lives on hold: A qualitative study of young refugees’ resilience strategies. Childhood 2017, 24, 348–365. [Google Scholar] [CrossRef] [PubMed]
- Uysal, B.; Yanik, M.; Tastekne, F.; Tuzgen, E.; Altinisik, E.; Acarturk, C. Psychological problems and resilience among Syrian adolescents exposed to war. Eur. J. Trauma Dissociation 2022, 6, 100258. [Google Scholar] [CrossRef]
- Santrock, J.W. Adolescence, 15th ed.; Mc Graw-Hill: New York, NY, USA, 2013. [Google Scholar]
- United Nations High Commissioner Refugees. Figures at a Glance. 2019. Available online: https://www.unhcr.org/figures-at-a-glance.html (accessed on 2 March 2022).
- Jensen, T.K.; Fjermestad, K.W.; Granly, L.; Wilhelmsen, N.H. Stressful life experiences and mental health problems among unaccompanied asylum-seeking children. Clin. Child Psychol. Psychiatry 2015, 20, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Lustig, S.L.; Kia-Keating, M.; Knight, W.G.; Geltman, P.; Ellis, H.; Kinzie, J.D.; Keane, T.; Saxe, G.N. Review of child and adolescent refugee mental health. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 24–36. [Google Scholar] [CrossRef]
- Dumont, M.; Provost, M.A. Resilience in adolescents: Protective role of social, coping strategies, self-esteem, and social activities on experience of stress and depression. J. Youth Adolesc. 1999, 28, 343–363. [Google Scholar] [CrossRef]
- Reed, R.V.; Fazel, M.; Jones, L.; Panter-Brick, C.; Stein, A. Mental health of displaced and refugee children resettled in low-income and middle-income countries: Risk and protective factors. Lancet 2012, 379, 250–265. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607. [Google Scholar] [CrossRef]
- Ungar, M. Designing resilience research: Using multiple methods to investigate risk exposure, promotive and protective processes, and contextually relevant outcomes for children and youth. Child Abus. Negl. 2019, 96, 104098. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.; Vann, B. Gender-based violence in refugee settings. Lancet 2002, 360, 13–14. [Google Scholar] [CrossRef] [PubMed]
- Lugova, H.; Samad, N.; Haque, M. Sexual and gender-based violence among refugees and internally displaced persons in the democratic republic of the congo: Post-conflict scenario. Risk Manag. Health Care Policy 2020, 13, 2937. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author(s) | Country | Study Design | Participant Characteristics and Origin | Sample Size and Sampling Technique |
|---|---|---|---|---|
| Dehnel et al. [32] | Jordan | Cross-sectional | Syrian refugee children. Mean age of 13.4 years, range 10–17. Male (25.7%) and female (74.3%). | N = 339, Non-random sampling |
| Guido et al. [33] | Jordan | Cross-sectional | Syrian children living in Jordanian refugee camps. Mean age 10.5 years, range 7–14. Male (49.8%) and female (50.2%). | N = 311 Random sampling |
| Kim et al. [34] | South Korea | Cross-sectional | North Korean refugee youth. Mean age 18.2 years, range 13–21. Male (51.4%) and female (48.6%). | N = 144, Non-random sampling |
| Mahamid [35] | Palestine (West Bank) | Case study | Palestine adolescent refugees. Mean age 14.8 years, range 14–16. Male (43.3%) and female (n = 56.7%). | N = 30, Snowball sampling |
| O’connor & Seager [36] | Bangladesh | Cross-sectional | Rohingya adolescents living in camps. Mean age 16 years, range 15–18. Male (49%) and female (51%). | N = 361 Random sampling |
| Dangmann et al. [37] | Norway | Cross-sectional | Syrian Refugee youth. The mean age was 18 years, range 12–24. Male (62.5%) and female (37.5%). | N = 161 Strategic sampling |
| Sleijpen et al. [38] | Netherlands | Case study | Treatment-seeking refugee youth originating from the Middle East, Africa, Eastern Europe, and Asia. Mean age 16.7 years, range 13–21. Male (50%) and female (50%). | N = 16 Non-random sampling |
| Uysal et al. [39] | Turkey | Cross-sectional | Syrian adolescent refugees. Mean age 15.5 years, range 12–18. Male (44%) and female (56%). | N = 430 Random sampling |
| Author(s) | Resilience Factors Measured | Relationship between Traumatic Experience and Resilience |
|---|---|---|
| Dangmann et al. [37] | Individual, relational and contextual dimensions. | Potential traumatic events were negatively correlated with resilience (r = −0.20, p < 0.05). |
| Dehnel et al. [32] | Individual (personal and social skills), relational (such as child’s social support) and contextual factors (spirituality and environmental influences). | Traumatic life events were not significantly correlated with resilience. |
| Guido et al. [33] | Personal skills, social resources and contextual factors. | Higher levels of trauma exposure were correlated with lower resilience (r = −0.213, p< 0.001). |
| Kim et al. [34] | Individual resiliency (e.g., hardiness, intimacy and clear sense of goals). | Trauma exposure was not significantly associated with ego resiliency (R = 0.02) |
| Mahamid [35] | Individual resiliency (e.g., positive self-efficacy, effective coping, psychological hardness and responsibility). | Children in the sample group expressed high levels of resiliency in dealing with traumatic and painful experiences. |
| O’connor & Seager [36] | Individual, relational, communal and cultural. | Exposure to traumatic events was positively and significantly associated with resilience |
| Sleijpen et al. [38] | Individual and social contexts factors such as (1) acting autonomously, (2) performing at school, (3) perceiving support from peers and parents and (4) participating in the new society | Resilience helped young refugees strengthen their sense of power and control, give them some distraction, and support or sustain their spirit within the family unit and the new society. Almost all of them (n = 15) found that they had psychologically matured: they had become stronger and more independent through their hardships. |
| Uysal et al. [39] | Individual, relational, communal and cultural. | Resilience was negatively correlated with occurrence of traumatic events (r = −0.34, p < 0.001) and negative appraisal of trauma (r = −0.26, p < 0.01). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danga, S.D.; Adebiyi, B.O.; Koegler, E.; Joseph, C.; Roman, N.V. Associations between Traumatic Experience and Resilience in Adolescent Refugees: A Scoping Review. Youth 2022, 2, 681-690. https://doi.org/10.3390/youth2040048
Danga SD, Adebiyi BO, Koegler E, Joseph C, Roman NV. Associations between Traumatic Experience and Resilience in Adolescent Refugees: A Scoping Review. Youth. 2022; 2(4):681-690. https://doi.org/10.3390/youth2040048
Chicago/Turabian StyleDanga, Solomon D., Babatope O. Adebiyi, Erica Koegler, Conran Joseph, and Nicolette V. Roman. 2022. "Associations between Traumatic Experience and Resilience in Adolescent Refugees: A Scoping Review" Youth 2, no. 4: 681-690. https://doi.org/10.3390/youth2040048
APA StyleDanga, S. D., Adebiyi, B. O., Koegler, E., Joseph, C., & Roman, N. V. (2022). Associations between Traumatic Experience and Resilience in Adolescent Refugees: A Scoping Review. Youth, 2(4), 681-690. https://doi.org/10.3390/youth2040048