Abstract
Background/Objectives: Arterial stiffness is an independent cardiovascular risk factor, and arterial velocity pulse index (AVI) and arterial pressure–volume index (API) are practical oscillometric markers. Shigin, a traditional Japanese vocal recitation practice characterised by abdominal breathing, has limited physiological evidence. This cross-sectional exploratory study examined the association between long-term shigin practice and arterial stiffness in older adults. Methods: Community-dwelling adults aged ≥60 years were classified into shigin practitioners (≥10 years), physically active non-practitioners, and inactive non-practitioners. AVI and API were measured using an upper-arm oscillometric device. Blood pressure, heart rate, salivary α-amylase (morning, standardised conditions), and peak expiratory flow were assessed. Results: Both shigin practitioners and active non-practitioners showed lower AVI and API, lower blood pressure, higher peak expiratory flow, and lower salivary α-amylase than inactive non-practitioners (p < 0.01). These associations remained significant after adjustment for blood pressure, heart rate, and sex. Conclusions: Long-term shigin practice was associated with arterial stiffness indices comparable to those of physically active older adults, without implying causality.
1. Introduction
Cardiovascular disease (CVD) is a leading cause of death in many developed countries, accounting for an estimated 32% of global deaths (approximately 19.8 million individuals) in 2022 [1]. In Japan, the mortality rate due to heart disease has increased since 1995 [2]. Increased arterial stiffness often precedes CVD events by several years [3]. Therefore, prevention of increased arterial stiffness is necessary to reduce CVD events.
Pulse wave velocity (PWV) and the cardio-ankle vascular index (CAVI) are widely used as representative methods for assessing arterial stiffness [3]. However, previously reported measurements require time and expertise, and the burden on patients—such as wearing limb cuffs and neck and thigh sensors—is a significant issue [4,5]. These requirements compromise the practicality of regular, large-scale screening. In recent years, arterial velocity pulse index (AVI) and arterial pressure–volume index (API) have gained attention as new indicators for assessing arterial stiffness. Developed through collaborative research between the National Institute of Advanced Industrial Science and Technology and the Institute of Physical and Chemical Research, AVI and API are based on the upper-arm oscillometric method and can be measured within approximately 2 min without requiring specialised procedures. Both are significantly correlated with PWV, CAVI, and blood pressure (BP) [6,7,8,9,10,11]. Furthermore, increased AVI and API may be independently associated with CVD risk [7,12,13]. For example, Sasaki-Nakashima et al. (2017) reported that API was independently associated with the Framingham and Suita risk scores [14]. Therefore, exploring interventions to maintain and improve AVI and API, which are new indicators of arterial stiffness, holds substantial preventive medical importance.
Numerous studies have suggested that behaviours involving breathing and vocalisation exert may be related to beneficial effects on circulatory function. Regular physical activity (especially aerobic exercise) strengthens the respiratory muscles and reduces in PWV, AVI, API, and BP [15,16]. Raj et al. (2023) reported that yoga practitioners had a significantly lower PWV than non-practitioners [17]. Similarly, a systematic review on breathing techniques and BP also suggested that breathing techniques significantly reduce systolic BP (SBP) and diastolic BP (DBP) [18]. In addition, breathing-based interventions are well established for reducing anxiety and stress, potentially involving neuroendocrine pathways including cortisol-related mechanisms, and respiratory training has a long history of lowering blood pressure [19]. These established effects provide a mechanistic framework linking breathing/vocalization practices to autonomic regulation and vascular function. Meanwhile, older individuals who have continued choral activities for over 10 years have higher subjective health perceptions than non-participants [20]. Furthermore, the BP in practitioners of traditional Tibetan Buddhist meditation was significantly lower than that in the general population, with an approximately 38% lower prevalence of hypertension [21]. These findings suggest that breathing- and vocalisation-based training reduces arterial stiffness. Traditional religious chanting (for example, Catholic Ave Maria and Buddhist mantras) also improves heart rate (HR) variability and circulatory indicators [22,23]. In Japan, shigin—a traditional performing art characterised by unique intonation and recitation style—emerged over 1000 years ago. Shigin is a traditional Japanese performing art characterised by unique recitation and breathing techniques, and is particularly sustained over long periods among older people. Thus, shigin gained widespread popularity in the early modern period and has recently been re-evaluated for its potential health benefits.
Physiologically, the combination of regular breathing rhythm, prolonged exhalation, and stable voice production may influence the autonomic nervous system and circulatory dynamics, similar to the effects observed in other forms of chanting. Therefore, long-term practitioners of shigin may experience beneficial effects on arterial stiffness through repetitive vocalisation and abdominal breathing. However, although chanting practices worldwide have been physiologically validated, shigin remains confined mainly to anecdotal, educational, or cultural contexts, with limited objective scientific investigation using physiological indicators.
Accordingly, the purpose of this study was to compare AVI and API between shigin practitioners and non-practitioners cross-sectionally. Non-practitioners were further divided into inactive and active groups, based on physical activity levels. This grouping was used to contextualize arterial stiffness indices in shigin practitioners relative to both low-activity and physically active reference groups, thereby partially disentangling shigin practice from habitual physical activity as a potential correlate of AVI/API.
2. Results
2.1. Participant Characteristics
Table 1 presents the participants’ physical and demographic characteristics. A total of 104 participants were included in the final analysis and categorised into the shigin practitioner group (n = 35), the active non-practitioner group (n = 35), and the inactive non-practitioner group (n = 34). There were no significant differences among the three groups in terms of sex, age, height, body weight, BMI, sleep duration, postmenopausal status, smoking history, or medication use. No participants reported physician-diagnosed primary cardiovascular disease, current smoking, or the use of antihypertensive, lipid-lowering, or antidiabetic medications, which reduces (but does not eliminate) concern that treatment status drove between-group differences in blood pressure-related variables.

Table 1.
Participant characteristics.
2.2. Arterial Stiffness
Figure 1 illustrates the AVI and API values. Both the poetry recitation practitioner group and active group had significantly lower AVI (Figure 1A) and API (Figure 1B) than the inactive group (both p < 0.01). These differences remained significant after adjusting for SBP, sex and HR as covariates via ANCOVA.
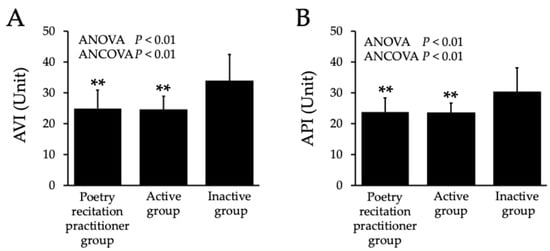
Figure 1.
AVI (A) and API (B) in both groups. Values are mean ± standard deviation (SD). AVI: arterial velocity pulse index, API: arterial pressure volume index. ** p < 0.01 vs. inactive group. Adjusted analyses were additionally performed using ANCOVA including SBP, sex, and HR as a covariate, yielding consistent results (p < 0.01).
2.3. Blood Pressure and Heart Rate
Brachial SBP, MBP, DBP, and CSBP were significantly lower in both the poetry recitation practitioner group and active group compared to the inactive group (Table 2; all p < 0.05). No significant differences were found among the groups in PP and HR. Additionally, no differences in BP or HR were observed between the poetry recitation practitioner group and the active group.
Table 2.
Secondary outcomes.
2.4. Salivary α-Amylase
Table 2 presents the results for salivary α-amylase activity. Both the poetry recitation practitioner group and active group showed significantly lower levels than the inactive group (p < 0.01). No significant difference was found between the poetry recitation practitioner group and the active group.
2.5. Peak Expiratory Flow
Table 2 shows the results for PEF. Both the poetry recitation practitioner group and active group had significantly higher PEF than the inactive group (p < 0.01). There was no significant difference in PEF between the poetry recitation practitioner group and the active group.
2.6. Correlation Between Arterial Stiffness and Peak Expiratory Flow
Figure 2 illustrates the correlations among physiological measures. PEF showed a significant negative correlation with AVI (r = −0.50, p < 0.05; Figure 2A) and with API (r = −0.40, p < 0.05; Figure 2B).
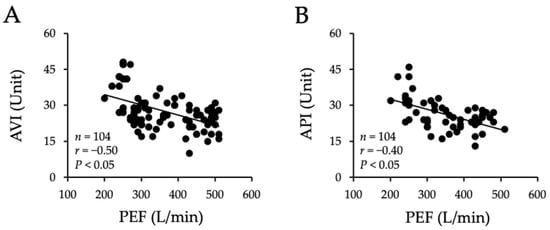
Figure 2.
Correlation between AVI (A), API (B), and PEF in both groups. Values are mean ± standard deviation (SD). AVI: arterial velocity pulse index, API: arterial pressure volume index, PEF: peak expiratory flow.
3. Discussion
This study found that, compared with the inactive group from the same age cohort and region, the poetry recitation practitioner group exhibited significantly lower AVI and API values. Furthermore, the poetry recitation practitioner group showed significantly higher PEF and significantly lower salivary α-amylase activity than the inactive group. Moreover, AVI and API values in the poetry recitation practitioner group were comparable with those in the active group. These findings indicate that shigin practice, which involves specific breathing and vocalization techniques, was associated with lower arterial stiffness indices and more favorable respiratory/stress-related profiles, comparable to those observed in physically active individuals. Overall, these findings suggest that long-term training in the breathing and vocalization techniques used in shigin is associated with physiological characteristics such as respiratory function and arterial stiffness indices, rather than demonstrating a causal effect. In the present study, the distribution of males and females was comparable across groups, and additional sex-adjusted and sex-stratified analyses did not materially alter the observed associations between group status and arterial stiffness indices. Although the present study was not specifically powered to detect subtle sex-specific effects, these findings reduce the likelihood that biological sex primarily accounted for the observed group differences.
Shigin is a traditional Japanese performing art characterized by unique recitation and breathing techniques, and is particularly sustained over long periods by older people. However, the population of shigin practitioners has declined in recent years, raising concerns about the preservation of Japan’s performing arts culture [24]. Although the present cross-sectional design limits causal inference, a physiological approach was implemented. In this study, the AVI and API of the poetry recitation practitioner group were significantly lower than those in the inactive group and comparable with those in the active group. Regular physical activity (predominantly aerobic exercises such as walking or running) suppresses age-related increases in arterial stiffness [25,26]. For example, an association has been demonstrated between the IPAQ score, which is an indicator of physical activity level, and CAVI [27]. In previous studies, individuals with exercise habits exhibited lower AVI and API than those without [16]. Among the Japanese population, increased physical activity levels are associated with reduced brachial-ankle pulse wave velocity [28]. Furthermore, in older persons, aerobic exercise performed four to five times per week reduces carotid-femoral pulse wave velocity [29]. In this study, the AVI and API of shigin practitioners were significantly lower than those in the inactive group and equivalent to those in the active group. In a previous study, an 8-week aerobic exercise program (30 min/session, 65% of reserve heart rate, bicycle ergometer) for older adults reduced API from 31.9 ± 4.0 before intervention to 24.1 ± 1.9 (mean ± SD) after intervention [30]. This post-intervention API value was equivalent to that of the poetry recitation practitioner and active group in this study. Therefore, shigin may be associated with vascular adaptations similar to those observed during physical activity, through a moderate physiological load associated with breathing and vocalisation. Furthermore, the AVI and API values of the shigin practitioners in this study tended to be lower than those of Japanese individuals with major adverse cardiac events (+) in a previous study (AVI: 29.0 ± 7.9, API: 35.6 ± 8.4) [14]. In the respiratory domain, a systematic review and meta-analysis of yoga, breathing techniques, and meditation suggested reductions in SBP and arterial stiffness [31]. Furthermore, a 6-week program of inspiratory muscle training lowers SBP by approximately nine mmHg [32], and regular yoga practitioners exhibited lower arterial stiffness than non-practitioners [33]. Interestingly, long-term practices of prayer (the Roman Catholic Ave Maria) and mantra chanting (Indian mantras) stabilise cardiovascular function [22,23]. Considering the above, the finding that the poetry recitation practitioner group had significantly lower AVI and API than the inactive group, significantly higher PEF, and results equivalent to those of the active group is consistent with the possibility that respiratory function–related factors are associated with differences in arterial stiffness.
Breathing-focused practices have been consistently associated with reductions in anxiety and perceived stress, and physiological pathways involving hypothalamic–pituitary–adrenal axis activity (including cortisol-related mechanisms) have been proposed. Moreover, respiratory training has a well-established track record of lowering blood pressure [33], which may, at least in part, contribute to more favorable vascular profiles in habitual practitioners. Although this study does not verify the underlying mechanisms, several plausible explanations exist. The API reflects the gradient of the cuff pressure–volume relationship (the compliance component of the pressure–volume curve), making it sensitive to peripheral arterial elasticity (including resistance vessels) and vascular tone [12,16]. Regular diaphragmatic breathing may enhance baroreflex sensitivity, suppress sympathetic output [34,35], and activate the nitric oxide (NO) pathway via shear stress [36]. The YOGINI Study (“Additional Improvement of Respiratory Technique on Vascular Function in Hypertensive Postmenopausal Women Following Yoga or Stretching Video Classes”) reported similar findings. Previous studies have suggested that 12 weeks of Baduanjin (a light exercise or qigong-like movement pattern involving breathing) significantly improved peripheral and CSBP, as well as sympathetic activity [37]. Thus, BP and sympathetic activity may be related to the low AVI and API values observed in the poetry recitation practitioner group. However, in this study, the between-group differences in AVI and API persisted even after adjusting for SBP and HR as covariates. In addition, because arterial stiffness indices are known to differ by biological sex, supplementary analyses were conducted using ANCOVA with sex included as an additional covariate. In these models, sex showed a statistically significant main effect on both AVI and API; however, the main effect of group remained significant after adjustment for sex, SBP, and heart rate. These findings indicate that the observed group differences in arterial stiffness indices were not explained by sex distribution and were robust to adjustment for biological sex. This pattern is compatible with alterations in vascular structure or function that cannot be fully explained by BP alone. Sympathetic nervous activity (SNA) is recognised as a key contributor to atherosclerosis by altering arterial smooth muscle tone [38]. Studies on healthy individuals have demonstrated a correlation between myogenic sympathetic nerve activity and AVI [39]. A study involving 10 years of yoga mantra chanting reported that vocalised breathing techniques influence autonomic nervous system rhythms [22]. Furthermore, anthroposophic speech therapy, a guided rhythmic speech practice that incorporates poetry, affects heart rate variability (HRV) [40]. Studies on deep breathing, meditation, yoga, and breathing exercises have repeatedly reported significant changes in the frequency components of HRV, even when HR remains constant [41]. Notably, the coordination between voice production and respiratory control has been extensively investigated in neurological and neurorehabilitative contexts, including disorders affecting speech motor control, respiration–phonation coupling, and autonomic regulation [42]. Beyond neurological applications, vocalization and respiratory control may also have relevance in internal medicine, particularly in cardiovascular and systemic conditions characterized by autonomic imbalance, vascular dysfunction, and stress-related pathophysiology. From this perspective, breathing–voice coordination may represent a broader physiological modulator rather than a phenomenon limited to speech or neurological rehabilitation. Although this study did not perform comprehensive HRV measurements, the poetry recitation practitioner group showed significantly lower salivary α-amylase activity than the inactive group. Therefore, the mechanical load from sustained vocalisation and abdominal breathing during poetry recitation may be associated with autonomic regulation, which could be reflected in lower API values and a shift toward compliance in the pressure–volume curve. AVI is an indicator that reflects the strength and timing of pulse wave propagation and its reflection from the heart to the periphery, representing the dynamic interaction between central and peripheral arteries [7]. The aorta is particularly rich in elastin, and its elasticity markedly decreases with aging [43]. Previous studies using animal models to analyse vascular endothelial function have suggested that age-related increases in arterial stiffness may be attributable to impaired vascular endothelial function [44]. In this study, no significant difference in CSBP was observed among the poetry recitation practitioner group. Therefore, the low AVI values may be associated with reduced peripheral vascular resistance. Specifically, the lower salivary α-amylase levels observed in the poetry recitation practitioner group than in those in the inactive group support the possibility that poetry recitation is associated with lower sympathetic arousal. Therefore, reduced sympathetic tone and peripheral vascular tension may contribute to the observed differences in arterial stiffness indices. Furthermore, the increase in PEF among the poetry recitation practitioner group may reflect improved respiratory muscle performance owing to diaphragmatic breathing and repeated sustained vocalisations. Improved respiratory function reduces peripheral vascular resistance by normalising intrathoracic pressure amplitude and promoting venous circulation [45]. These combined mechanisms may be associated with the lower API and AVI observed in the poetry recitation practitioner group. However, the effects of poetry recitation on the autonomic nervous system and hemodynamics may differ from those of general aerobic exercise. This study demonstrated that the AVI and API of the poetry recitation practitioner group were equivalent to those of the active group. This indicates that the vocalisation and breathing training inherent in poetry recitation is associated with favorable arterial stiffness indices. However, arterial adaptation to the unique autonomic nervous system stimulation of poetry recitation may also be involved. Therefore, clarifying the relative contributions of each factor remains a challenge and requires confirmation in longitudinal and interventional studies. However, the effects of poetry recitation on the autonomic nervous system and hemodynamics may differ from those of general aerobic exercise. This study demonstrated that the AVI and API of the poetry recitation practitioner group were equivalent to those of the active group. This indicates that the vocalisation and breathing training inherent in poetry recitation is associated with favorable arterial stiffness indices. However, arterial adaptation to the unique autonomic nervous system stimulation of poetry recitation may also be involved. Therefore, clarifying the relative contributions of each factor remains a challenge and requires confirmation in longitudinal and interventional studies [46,47]. Moreover, breathing exercises have been suggested to influence endothelial nitric oxide synthase (eNOS) and NO production, which play central roles in vascular health [48]. In contrast, aerobic or resistance exercise has been well documented to rapidly improve vascular endothelial function through increased blood flow and shear stress, which stimulate NO release and upregulate eNOS expression [49,50]. Notably, even relatively short-term aerobic training interventions (for example, 12 weeks) have demonstrated significant improvements in flow-mediated dilation (FMD) and arterial stiffness [51]. Given that shigin and other breathing-based interventions generate lower levels of hemodynamic shear stress than physical exercise does [52], their capacity to stimulate acute endothelial responses may be limited in the short term. Furthermore, vascular structural adaptations—such as outward remodeling or changes in wall-to-lumen ratio—typically require sustained mechanical stimuli over extended periods, which may not be adequately provided by low-intensity breathing practices alone. In addition, if participants already exhibited relatively preserved vascular function at baseline, the margin for detectable improvement may have been minimal, further reducing the likelihood of observing short-term changes through shigin. The stress-relieving and anti-inflammatory effects of shigin are cumulative, with effects emerging gradually over prolonged engagement. Some studies have proposed that slow and controlled breathing can produce vagal nerve stimulation-like effects, thereby modulating the neuroimmune communication pathways that indirectly support vascular homeostasis [53]. Collectively, these findings support the hypothesis that, although physical exercise offers a more potent and immediate stimulus for improving vascular function, long-term shigin practice may be associated with comparable vascular indices in some individuals. Therefore, the comparable AVI values observed in this study between long-term shigin practitioners and physically trained individuals may reflect cumulative adaptation or selection effects in the former group. In contrast, individuals who have recently initiated shigin training may exhibit smaller improvements in vascular indices relative to their exercise-trained counterparts. Future longitudinal studies assessing novice shigin practitioners at multiple time points—with concurrent measurements of endothelial function (e.g., FMD), arterial stiffness, inflammatory markers, and autonomic indicators—are warranted to validate this hypothesis and further clarify the physiological mechanisms underlying the vascular effects of shigin.
From a clinical rehabilitation and public health perspective, shigin may represent a low-cost, culturally embedded, and sustainable approach, particularly when contrasted with supervised exercise programs or rehabilitation strategies that require specialized facilities, equipment, or ongoing professional support. The comparable outcomes between the poetry recitation practitioner group and the active groups suggest that shigin practice may be associated with favorable profiles, even among individuals with limited mobility or exercise intolerance; however, interventional studies are required to determine its effectiveness. As cardiovascular disease (CVD) remains a global health burden—particularly among aging populations—the dissemination of alternative, culturally acceptable preventive and rehabilitative strategies is urgently needed. From a scientific and methodological standpoint, this study advances the field by incorporating novel indices of arterial stiffness (AVI and API), respiratory function (PEF), and a stress biomarker (salivary α-amylase) to characterize the physiological profile associated with traditional vocal practice comprehensively. These findings open new avenues for interdisciplinary research at the intersection of cardiovascular physiology, respiratory therapy, neuroautonomic regulation, and behavioral rehabilitation. Importantly, this study provides a rare example of evidence-based cultural preservation. In an era in which traditional performing arts are rapidly declining, our findings support the hypothesis that practices such as shigin may possess both intangible cultural value and tangible physiological benefits. By validating the health-promoting properties of such traditions using modern biomedical tools, this study contributes to the global movement toward culturally sensitive, community-based rehabilitation and health promotion. Thus, this study serves as both a scientific contribution and a public health innovation rooted in cultural heritage.
Because this study employed a cross-sectional, observational design, the direction of the observed associations cannot be determined; the findings may reflect reverse causation and/or residual confounding (e.g., unmeasured lifestyle, diet, socioeconomic status, or health selection into shigin practice), and thus should not be interpreted as evidence that shigin causes improvements in vascular health. Moreover, the physiological evidence directly supporting the proposed mechanisms linking vocalization, breathing coordination, and arterial stiffness remains limited. Although several plausible pathways have been suggested based on respiratory and autonomic physiology, the underlying mechanisms cannot be conclusively established from this exploratory, cross-sectional study and should be interpreted with appropriate caution.
This study had some limitations. The cross-sectional design precludes causal inference, and dosage information such as shigin frequency, cumulative sessions, vocal volume, or tempo was not collected. In addition, important lifestyle-related factors (e.g., dietary patterns, socioeconomic status, and engagement in other physical, cultural, or meditative activities) were not comprehensively assessed and may have contributed to residual confounding. Although sex-stratified and sex-adjusted analyses were conducted, the study was not specifically powered to detect sex-specific associations; therefore, subtle biological sex differences cannot be fully excluded. In addition, other arterial stiffness indicators (PWV, CAVI, FMD, and Augmentation Index) were not compared. Future randomized controlled trials and longitudinal studies should analyze in more detail the relationship between breathing patterns and hemodynamics to clarify the physiological mechanisms quantitatively.
4. Materials and Methods
4.1. Study Design and Ethics
This study used a cross-sectional observational design. All participants received verbal and written explanations of the study purpose, procedures, anticipated benefits, and potential risks, and provided written informed consent. This study complied with the Declaration of Helsinki and was approved by the Ethics Review Committee of Teikyo University of Science (Approval No. 24A071). This study was registered with the University Hospital Medical Information Network Center (UMIN000059866). This manuscript was prepared in accordance with the STROBE statement for cross-sectional studies. Participants were instructed to refrain from caffeine intake before measurement, wait ≥60 min after breakfast, and avoid exercise on the day of testing. Measurements were performed in the morning after adequate rest in a quiet environment at 24–26 °C. Outcome assessments were performed by trained staff using standardised procedures; assessors were not blinded to group assignment, but AVI/API and blood pressure values were automatically computed by the device to minimise observer influence.
4.2. Participants and Group Definitions
Participants were recruited through local public media from the same region. Inclusion criteria were community-dwelling adults aged ≥60 years who were able to complete all measurements. Exclusion criteria included a self-reported history of significant cardiovascular disease (e.g., myocardial infarction, stroke, or heart failure) based on a medical history questionnaire. Comorbidities (hypertension, hyperlipidemia, and diabetes), smoking status, and medication use were assessed by questionnaire. Shigin practitioners were defined a priori as individuals who (i) had continuous registration with an officially recognised shigin federation/school for ≥10 years, (ii) practiced ≥1 session/week for ≥5 of the past 10 years, and (iii) held at least an intermediate certificate (kyu/dan or equivalent) or had on-record participation in certified recitation events. Federation-issued documents (membership/qualification records and event participation logs) were inspected in person by study staff and cross-checked against federation rosters; inspections were recorded in a verification log (date, verifier IDs, source, items confirmed). A supervising master provided a signed attestation of ongoing practice for each practitioner. Non-practitioners were individuals without a history of shigin practice and were classified by physical activity level using the International Physical Activity Questionnaire (IPAQ). The “active” non-practitioner group met IPAQ criteria for moderate-to-high physical activity and reported regular aerobic exercise training. The “inactive” non-practitioner group met IPAQ criteria for low physical activity. IPAQ additionally screened shigin practitioners to confirm the absence of other regular exercise programmes, enabling interpretation relative to both low-activity and physically active reference groups (Table 1).
4.3. Sample Size Calculation
The required sample size was estimated using G*Power (version 3.1.9.7, Heinrich-Heine-University Düsseldorf, Germany), assuming a one-way analysis of variance (ANOVA) to compare arterial stiffness indices across three groups. Based on the study design and previous research, a medium-to-large effect size (f = 0.31) was assumed. With α = 0.05 and power (1-β) = 0.80, the required total sample size was estimated at 102 participants (34 per group). The final analysed sample and group sizes are reported in the Section 3.
4.4. Outcomes (Primary and Secondary)
Primary outcomes were AVI and API. Secondary outcomes were brachial blood pressure indices (SBP, DBP, MBP, PP), heart rate (HR), estimated central SBP (CSBP), salivary α-amylase activity, and peak expiratory flow (PEF). These variables were selected to characterise arterial stiffness indices together with plausible correlates related to autonomic/stress-related physiology and respiratory function.
4.5. Measurement Procedures
4.5.1. Arterial Stiffness (AVI and API)
AVI and API were measured based on previously reported methods [6,7]. AVI reflects systemic arterial stiffness, and API reflects peripheral arterial stiffness. Measurements were performed using the PASESA AVE-2000 medical electronic sphygmomanometer (Shisei Data Co., Ltd., Tokyo, Japan). BP and pulse wave data were simultaneously acquired using an oscillometric sensor attached to the left upper arm. AVI and API were calculated from the time series of cuff pressure and pulse wave amplitude data. The AVI was determined from the peak-to-peak amplitude of the differential waveform, whereas the API was derived based on changes in arterial volume. The calculation principles and formulas followed those previously published. Measurements were performed by trained researchers with participants seated in a resting position. The validity and reliability of AVI and API have been confirmed in previous studies. The coefficient of variation (CV) for this measurement was 3 ± 1% for both AVI and API.
4.5.2. Blood Pressure and Heart Rate
SBP, DBP, mean blood pressure (MBP), pulse pressure (PP), and HR in the brachial artery were measured using the PASESA AVE-2000 medical electronic sphygmomanometer (Shisei Datam Co., Ltd., Tokyo, Japan). These were evaluated from the arterial pressure waveforms measured by an oscillometric sensor [6,7]. Central SBP (CSBP) was estimated using the device-embedded algorithm of a cuff-based vascular function analyzer (PASESA AVE-2000, Win Horizon Limited, Hong Kong, China), which computes CSBP from concurrently measured brachial BP, arterial stiffness indices (AVI and API), and age.
4.5.3. Stress Level (Salivary α-Amylase)
Salivary α-amylase activity was evaluated as a physiological indicator of stress response [54]. Because salivary α-amylase shows diurnal variation, all samples were collected during a fixed morning window (e.g., 09:00–11:00) under standardized conditions. Participants were asked to avoid eating, drinking (except water), tooth brushing, and smoking for at least 60 min before saliva collection. Saliva collection and measurement were performed using a Salivary Amylase Monitor (Nipro Corporation, Osaka, Japan) based on a dry chemistry method. A dedicated test strip was placed under the tongue for 30 s and then inserted into the device; the result was displayed within approximately 1 min. The device has been previously evaluated for performance/validity in assessing salivary α-amylase activity [54]. Given the known diurnal fluctuations of this biomarker, the measurement procedure and collection time window are described explicitly to improve interpretability. The CV for this measurement was 5 ± 1%.
4.5.4. Respiratory Function (PEF)
Respiratory function was assessed using PEF, measured with a Mini Lite Peak Flow Meter MY-0010S (Matsuyoshi Medical Instruments Co., Ltd., Tokyo, Japan). Participants were instructed to stand upright, inhale maximally, and exhale forcefully and rapidly. After one to three practice trials to familiarise participants with the PEF meter, measurements were obtained based on the American Lung Association [55]. The CV for this measurement was 5 ± 3%.
4.6. Statistical Analysis
All data are presented as mean ± standard deviation (SD). Normality of continuous variables was assessed using the Shapiro–Wilk test (and visual inspection of Q–Q plots). Group differences were evaluated using one-way analysis of variance (ANOVA) to compare variables among the poetry recitation practitioner, inactive, and active groups, followed by a Bonferroni post hoc correction for multiple comparisons. For the primary outcomes (AVI and API), adjusted estimates were obtained using analysis of covariance (ANCOVA) with SBP, HR, and biological sex as covariates. In addition, exploratory group × sex interaction terms were tested to examine whether the associations between group status and arterial stiffness indices differed by sex. Associations between AVI/API and PEF were evaluated using Pearson’s correlation coefficient. The significance level was set at p < 0.05. Statistical analyses were performed using IBM SPSS Statistics Version 31 (IBM, Armonk, NY, USA).
5. Conclusions
This study provides preliminary evidence that middle-aged and older adults who engaged in long-term poetry recitation exhibited significantly lower arterial stiffness indices (AVI and API) in this investigated population and significantly higher PEF compared to their age-matched peers in the inactive group. These preliminary findings indicate that long-term practice of poetry recitation is associated with enhanced respiratory function and reduced vascular stiffness indices. However, given the cross-sectional design, these findings should be interpreted as associative rather than causal. They should not be construed as evidence that shigin leads to or results in improvements in vascular health.
Author Contributions
R.K., S.S., K.N. and H.N. designed the study; R.K., S.S., K.N. and H.N. collected the data and performed the study; R.K. and H.N. performed the statistical analyses; R.K. drafted the manuscript; H.N. critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in compliance with the Declaration of Helsinki, based on ethical principles, human rights, and the protection of participants’ personal information. Ethical approval for this study was obtained from the Ethics Committee of Teikyo University of Science (Approval Number 24A071, date 12 April 2025).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon request.
Acknowledgments
This study was conducted with the kind cooperation of the Tama City Shigin Federation. We are deeply grateful to all community participants, research assistants, and students who supported the data collection. We also thank the staff who helped with instrumentation and venue coordination.
Conflicts of Interest
The authors declare no conflicts of interest. No individual or organisation exerted any undue influence on the study design, data collection and analysis, manuscript preparation, or the decision to publish.
References
- Mensah, G.A.; Fuster, V.; Murray, C.J.L.; Roth, G.A. Global Burden of Cardiovascular Diseases and Risks Collaborators, Global Burden of Cardiovascular Diseases and Risks, 1990–2022. J. Am. Coll. Cardiol. 2023, 82, 2350–2473. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Eguchi, E.; Hayashi, F.; Kinuta, M.; Imano, H. Epidemiology of cardiovascular disease in Japan: An overview study. J. Cardiol. 2024, 83, 191–200. [Google Scholar] [CrossRef]
- Hametner, B.; Wassertheurer, S.; Mayer, C.C.; Danninger, K.; Binder, R.K.; Weber, T. Aortic Pulse Wave Velocity Predicts Cardiovascular Events and Mortality in Patients Undergoing Coronary Angiography: A Comparison of Invasive Measurements and Noninvasive Estimates. Hypertension 2021, 77, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Ohishi, M.; Takagi, T.; Terai, M.; Shiota, A.; Hayashi, N.; Rakugi, H.; Ogihara, T. Clinical usefulness and limitations of brachial-ankle pulse wave velocity in the evaluation of cardiovascular complications in hypertensive patients. Hypertens. Res. 2006, 29, 989–995. [Google Scholar] [CrossRef]
- Spronck, B.; Terentes-Printzios, D.; Avolio, A.P.; Boutouyrie, P.; Guala, A.; Jerončić, A.; Laurent, S.; Barbosa, E.C.D.; Baulmann, J.; Chen, C.-H.; et al. Association for Research into Arterial Structure and Physiology (ARTERY), the European Society of Hypertension Working Group on Large Arteries, European Cooperation in Science and Technology (COST) Action VascAgeNet, North American Artery Society, ARTERY LATAM, Pulse of Asia, and Society for Arterial Stiffness—Germany-Austria-Switzerland (DeGAG), 2024 Recommendations for Validation of Noninvasive Arterial Pulse Wave Velocity Measurement Devices. Hypertension 2024, 81, 183–192. [Google Scholar] [CrossRef]
- Komine, H.; Asai, Y.; Yokoi, T.; Yoshizawa, M. Non-invasive assessment of arterial stiffness using oscillometric blood pressure measurement. Biomed. Eng. Online 2012, 11, 6. [Google Scholar] [CrossRef]
- Okamoto, M.; Nakamura, F.; Musha, T.; Kobayashi, Y. Association between novel arterial stiffness indices and risk factors of cardiovascular disease. BMC Cardiovasc. Disord. 2016, 16, 211. [Google Scholar] [CrossRef]
- Ueda, T.; Miura, S.-I.; Suematsu, Y.; Shiga, Y.; Kuwano, T.; Sugihara, M.; Ike, A.; Iwata, A.; Nishikawa, H.; Fujimi, K.; et al. Association of Arterial Pressure Volume Index With the Presence of Significantly Stenosed Coronary Vessels. J. Clin. Med. Res. 2016, 8, 598–604. [Google Scholar] [CrossRef]
- Komatsu, S.; Tomiyama, H.; Kimura, K.; Matsumoto, C.; Shiina, K.; Yamashina, A. Comparison of the clinical significance of single cuff-based arterial stiffness parameters with that of the commonly used parameters. J. Cardiol. 2017, 69, 678–683. [Google Scholar] [CrossRef][Green Version]
- Zhang, Y.; Yin, P.; Xu, Z.; Xie, Y.; Wang, C.; Fan, Y.; Liang, F.; Yin, Z. Non-Invasive Assessment of Early Atherosclerosis Based on New Arterial Stiffness Indices Measured with an Upper-Arm Oscillometric Device. Tohoku J. Exp. Med. 2017, 241, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Jiang, Y.; Liang, F.; Lu, J. Threshold values of brachial cuff-measured arterial stiffness indices determined by comparisons with the brachial-ankle pulse wave velocity: A cross-sectional study in the Chinese population. Front. Cardiovasc. Med. 2023, 10, 1131962. [Google Scholar] [CrossRef]
- Jin, L.; Zhang, M.; Sha, L.; Cao, M.; Tong, L.; Chen, Q.; Shen, C.; Du, L.; Liu, L.; Li, Z. Increased arterial pressure volume index and cardiovascular risk score in China. BMC Cardiovasc. Disord. 2023, 23, 22. [Google Scholar] [CrossRef]
- Jin, L.; Tong, L.; Shen, C.; Du, L.; Mao, J.; Liu, L.; Li, Z. Association of Arterial Stiffness Indices with Framingham Cardiovascular Disease Risk Score. Rev. Cardiovasc. Med. 2022, 23, 287. [Google Scholar] [CrossRef]
- Sasaki-Nakashima, R.; Kino, T.; Chen, L.; Doi, H.; Minegishi, S.; Abe, K.; Sugano, T.; Taguri, M.; Ishigami, T. Successful prediction of cardiovascular risk by new non-invasive vascular indexes using suprasystolic cuff oscillometric waveform analysis. J. Cardiol. 2017, 69, 30–37. [Google Scholar] [CrossRef]
- Xi, H.; Du, L.; Li, G.; Zhang, S.; Li, X.; Lv, Y.; Feng, L.; Yu, L. Effects of exercise on pulse wave velocity in hypertensive and prehypertensive patients: A systematic review and meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 2025, 12, 1504632. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, R.; Iwanuma, S.; Ohashi, N.; Hashiguchi, T. New indices of arterial stiffness measured with an upper-arm oscillometric device in active versus inactive women. Physiol. Rep. 2018, 6, e13574. [Google Scholar] [CrossRef] [PubMed]
- Raj, T.; Elliot, C.A.; Stoner, L.; Higgins, S.; Paterson, C.; Hamlin, M.J. Association between Yoga Participation and Arterial Stiffness: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 5852. [Google Scholar] [CrossRef]
- Garg, P.; Mendiratta, A.; Banga, A.; Bucharles, A.; Victoria, P.; Kamaraj, B.; Qasba, R.K.; Bansal, V.; Thimmapuram, J.; Pargament, R.; et al. Effect of breathing exercises on blood pressure and heart rate: A systematic review and meta-analysis. Int. J. Cardiol. Cardiovasc. Risk Prev. 2024, 20, 200232. [Google Scholar] [CrossRef]
- Kowalski, T.; Obmiński, Z.; Waleriańczyk, W.; Klusiewicz, A. The Acute Effect of Respiratory Muscle Training on Cortisol, Testosterone, and Testosterone-to-Cortisol Ratio in Well-Trained Triathletes-Exploratory Study. Respir. Physiol. Neurobiol. 2025, 331, 104353. [Google Scholar] [CrossRef] [PubMed]
- Pentikäinen, E.; Pitkäniemi, A.; Siponkoski, S.-T.; Jansson, M.; Louhivuori, J.; Johnson, J.K.; Paajanen, T.; Särkämö, T. Beneficial effects of choir singing on cognition and well-being of older adults: Evidence from a cross-sectional study. PLoS ONE 2021, 16, e0245666. [Google Scholar] [CrossRef]
- Meng, Q.; Xu, Y.; Shi, R.; Zhang, X.; Wang, S.; Liu, K.; Chen, X. Effect of religion on hypertension in adult Buddhists and residents in China: A cross-sectional study. Sci. Rep. 2018, 8, 8203. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Sleight, P.; Bandinelli, G.; Cencetti, S.; Fattorini, L.; Wdowczyc-Szulc, J.; Lagi, A. Effect of rosary prayer and yoga mantras on autonomic cardiovascular rhythms: Comparative study. BMJ 2001, 323, 1446–1449. [Google Scholar] [CrossRef]
- Tseng, A.A. Scientific Evidence of Health Benefits by Practicing Mantra Meditation: Narrative Review. Int. J. Yoga 2022, 15, 89–95. [Google Scholar] [CrossRef]
- Nihon Ginkenshibu Shinkōkai (Japan Ginkenshibu Promotion Foundation), FY2025 Project Plan and Budget. n.d. Available online: https://www.ginken.or.jp/wordpress/wp-content/uploads/2025/03/%E4%BB%A4%E5%92%8C%EF%BC (accessed on 20 September 2025).
- Liu, H.; Shivgulam, M.E.; Schwartz, B.D.; Kimmerly, D.S.; O’Brien, M.W. Impact of exercise training on pulse wave velocity in healthy and clinical populations: A systematic review of systematic reviews. Am. J. Physiol. Heart Circ. Physiol. 2023, 325, H933–H948. [Google Scholar] [CrossRef]
- Pierce, D.R.; Doma, K.; Leicht, A.S. Acute Effects of Exercise Mode on Arterial Stiffness and Wave Reflection in Healthy Young Adults: A Systematic Review and Meta-Analysis. Front. Physiol. 2018, 9, 73. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, T.; Amiya, E.; Ando, J.; Watanabe, M.; Murasawa, T.; Komuro, I. Different Contributions of Physical Activity on Arterial Stiffness between Diabetics and Non-Diabetics. PLoS ONE 2016, 11, e0160632. [Google Scholar] [CrossRef]
- Inomoto, A.; Deguchi, J.; Fukuda, R.; Yotsumoto, T.; Toyonaga, T. Age-Specific Determinants of Brachial-Ankle Pulse Wave Velocity among Male Japanese Workers. Tohoku J. Exp. Med. 2021, 253, 135–141. [Google Scholar] [CrossRef]
- Shibata, S.; Fujimoto, N.; Hastings, J.L.; Carrick-Ranson, G.; Bhella, P.S.; Hearon, C.M.; Levine, B.D. The effect of lifelong exercise frequency on arterial stiffness. J. Physiol. 2018, 596, 2783–2795. [Google Scholar] [CrossRef]
- Kobayashi, R.; Kasahara, Y.; Ikeo, T.; Asaki, K.; Sato, K.; Matsui, T.; Iwanuma, S.; Ohashi, N.; Hashiguchi, T. Effects of different intensities and durations of aerobic exercise training on arterial stiffness. J. Phys. Ther. Sci. 2020, 32, 104–109. [Google Scholar] [CrossRef]
- Patil, S.G.; Biradar, M.S.; Khode, V.; Vadiraja, H.S.; Patil, N.G.; Raghavendra, R.M. Effectiveness of yoga on arterial stiffness: A systematic review. Complement. Ther. Med. 2020, 52, 102484. [Google Scholar] [CrossRef] [PubMed]
- Craighead, D.H.; Heinbockel, T.C.; Freeberg, K.A.; Rossman, M.J.; Jackman, R.A.; Jankowski, L.R.; Hamilton, M.N.; Ziemba, B.P.; Reisz, J.A.; D’Alessandro, A.; et al. Time-Efficient Inspiratory Muscle Strength Training Lowers Blood Pressure and Improves Endothelial Function, NO Bioavailability, and Oxidative Stress in Midlife/Older Adults With Above-Normal Blood Pressure. J. Am. Heart Assoc. 2021, 10, e020980. [Google Scholar] [CrossRef]
- Duren, C.M.; Cress, M.E.; McCully, K.K. The influence of physical activity and yoga on central arterial stiffness. Dyn. Med. 2008, 7, 2. [Google Scholar] [CrossRef]
- Ferreira, J.B.; Plentz, R.D.M.; Stein, C.; Casali, K.R.; Arena, R.; Lago, P.D. Inspiratory Muscle Training Reduces Blood Pressure and Sympathetic Activity in Hypertensive Patients: A Randomized Controlled Trial. Int. J. Cardiol. 2013, 166, 61–67. [Google Scholar] [CrossRef]
- Joseph, C.N.; Porta, C.; Casucci, G.; Casiraghi, N.; Maffeis, M.; Rossi, M.; Bernardi, L. Slow breathing improves arterial baroreflex sensitivity and decreases blood pressure in essential hypertension. Hypertension 2005, 46, 714–718. [Google Scholar] [CrossRef]
- Fetter, C.; Marques, J.R.; de Souza, L.A.; Dartora, D.R.; Eibel, B.; Boll, L.F.C.; Goldmeier, S.N.; Dias, D.; De Angelis, K.; Irigoyen, M.C. Additional Improvement of Respiratory Technique on Vascular Function in Hypertensive Postmenopausal Women Following Yoga or Stretching Video Classes: The YOGINI Study. Front. Physiol. 2020, 11, 898. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Huang, J.; Gao, D.; Zeng, S.; Tang, S.; Chang, Z.; Wen, C.; Zhang, M.; Hu, M.; Wei, G.-X. Effects of mind-body practice on arterial stiffness, central hemodynamic parameters and cardiac autonomic function of college students. Complement. Ther. Clin. Pract. 2021, 45, 101492. [Google Scholar] [CrossRef]
- Tanaka, H.; Dinenno, F.A.; Seals, D.R. Reductions in central arterial compliance with age are related to sympathetic vasoconstrictor nerve activity in healthy men. Hypertens. Res. 2017, 40, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, H.; Hamaoka, T.; Murai, H.; Hirai, T.; Mukai, Y.; Kusayama, T.; Takashima, S.; Kato, T.; Takata, S.; Usui, S.; et al. Relationships between muscle sympathetic nerve activity and novel indices of arterial stiffness using single oscillometric cuff in patients with hypertension. Physiol. Rep. 2022, 10, e15270. [Google Scholar] [CrossRef] [PubMed]
- Bettermann, H.; Von Bonin, D.; Frühwirth, M.; Cysarz, D.; Moser, M. Effects of speech therapy with poetry on heart rate rhythmicity and cardiorespiratory coordination. Int. J. Cardiol. 2002, 84, 77–88. [Google Scholar] [CrossRef]
- Libby, D.J.; Worhunsky, P.D.; Pilver, C.E.; Brewer, J.A. Meditation-induced changes in high-frequency heart rate variability predict smoking outcomes. Front. Hum. Neurosci. 2012, 6, 54. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Di Luciano, C.; Chiaramonte, I.; Serra, A.; Bonfiglio, M. Multi-disciplinary clinical protocol for the diagnosis of bulbar amyotrophic lateral sclerosisProtocolo clínico multi-disciplinar para el diagnóstico de la esclerosis lateral amiotrófica bulbar. Acta Otorrinolaringol. 2019, 70, 25–31. [Google Scholar] [CrossRef]
- Tsamis, A.; Krawiec, J.T.; Vorp, D.A. Elastin and collagen fibre microstructure of the human aorta in ageing and disease: A review. J. R. Soc. Interface 2013, 10, 20121004. [Google Scholar] [CrossRef]
- Wesley, C.D.; Neutel, C.H.G.; De Meyer, G.R.Y.; Martinet, W.; Guns, P.-J. Unravelling the impact of active and passive contributors to arterial stiffness in male mice and their role in vascular aging. Sci. Rep. 2024, 14, 18337. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Baker, S.E. Take a Deep, Resisted, Breath. J. Am. Heart Assoc. 2021, 10, e022203. [Google Scholar] [CrossRef]
- Gerritsen, R.J.S.; Band, G.P.H. Breath of Life: The Respiratory Vagal Stimulation Model of Contemplative Activity. Front. Hum. Neurosci. 2018, 12, 397. [Google Scholar] [CrossRef]
- Magnon, V.; Dutheil, F.; Vallet, G.T. Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Sci. Rep. 2021, 11, 19267. [Google Scholar] [CrossRef]
- Podder, A.; Nazim, S.; Sharma, A.; De, A.; Singh, V.; Kumar, J.; Kumar, D.; Varsha, C.S.; Jani, P. Impact of Regular Breathing Exercises on Blood Pressure Phenotypes and BMI in Young Male Individuals: A Narrative Review. Cureus 2025, 17, e90027. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Maiorana, A.; O’Driscoll, G.; Taylor, R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J. Physiol. 2004, 561, 1–25. [Google Scholar] [CrossRef]
- Niebauer, J.; Cooke, J.P. Cardiovascular effects of exercise: Role of endothelial shear stress. J. Am. Coll. Cardiol. 1996, 28, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Chen, Y.; Zhen, K.; Ren, S.; Lv, Y.; Yu, L. Effect of continuous aerobic exercise on endothelial function: A systematic review and meta-analysis of randomized controlled trials. Front. Physiol. 2023, 14, 1043108. [Google Scholar] [CrossRef]
- Tavoian, D.; Mazzone, J.L.; Craighead, D.H.; Bailey, E.F. Acute inspiratory resistance training enhances endothelium-dependent dilation and retrograde shear rate in healthy young adults. Physiol. Rep. 2024, 12, e15943. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Dong, J.; Wang, Y.; Liu, Y. Exploring the potential of vagus nerve stimulation in treating brain diseases: A review of immunologic benefits and neuroprotective efficacy. Eur. J. Med. Res. 2023, 28, 444. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Kanemori, T.; Kanemaru, M.; Takai, N.; Mizuno, Y.; Yoshida, H. Performance evaluation of salivary amylase activity monitor. Biosens. Bioelectron. 2004, 20, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Measuring Your Peak Flow Rate. 2025. Available online: https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/treatment/devices/peak-flow (accessed on 20 September 2025).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.