
Perspectives on Wider Integration of the Health-Assistive Smart Home

 , ,
, ,
Abstract
:1. Introduction
1.1. Health-Smart Home
1.2. Accelerating the Integration of the Health Smart Home
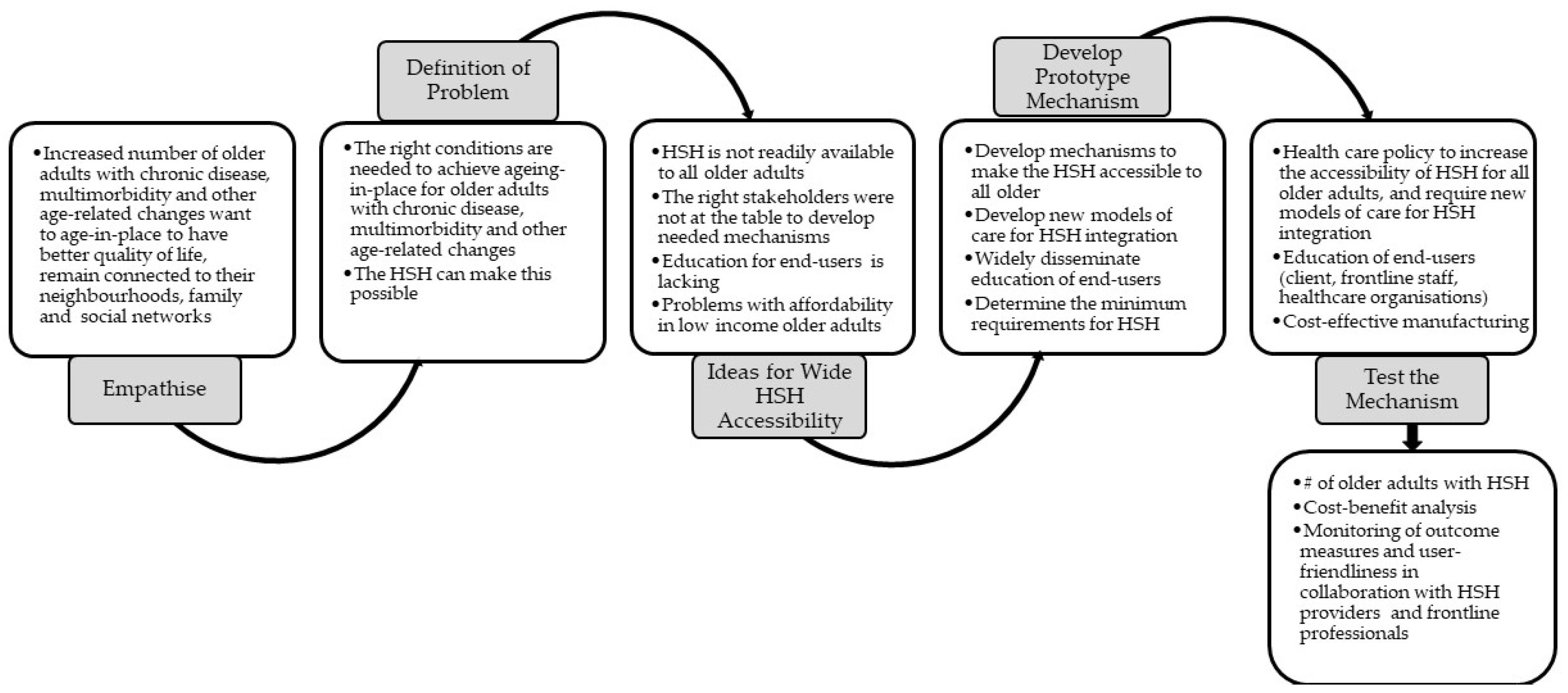
2. Design Thinking
3. Stakeholder Groups
3.1. Older Adult, Family Caregivers & Frontline Healthcare Professionals
3.2. Multidisciplinary Research and Academic or Educator Roles
3.3. Social Workers
3.4. Health Care Organizations
3.5. Aged Care Industry
3.6. Computer Science & Electrical Engineering Teams
3.7. Companies and Start-Ups
3.8. Healthcare Policy Makers and Special Interest Groups
3.9. Master System Integrator
4. Implications for Design Thinking for Real-World Integration of the HSH
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Healthy Ageing and the Sustainable Development Goals. Available online: http://www.who.int/ageing/sdgs/en/ (accessed on 10 March 2021).
- American Advisors Group. Importance of Home Survey. 2021. Available online: https://www.aag.com/homesurvey/p/1 (accessed on 3 May 2022).
- James, A.; Rowley, S.; Stone, W.; Parkinsson, S.; Spinney, A.; Ryenolds, M. Older Australians and the Housing Aspirations Gap: Housing Aspirations and Constraints for Lower Income Australians. Australian and Housing Research Institute. Available online: https://www.ahuri.edu.au/sites/default/files/migration/documents/AHURI-Final-Report-317-Older-Australians-and-the-housing-aspirations-gap.pdf (accessed on 3 May 2022).
- McGilton, K.S.; Vellani, S.; Yeung, L.; Chishtie, J.; Commisso, E.; Ploeg, J.; Andrew, M.K.; Ayala, A.P.; Gray, M.; Morgan, D.; et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: A scoping review. BMC Geriatr. 2018, 18, 231. [Google Scholar] [CrossRef] [PubMed]
- Rohrmann, S. Epidemiology of Frailty in Older People. Adv. Exp. Med. Biol. 2020, 1216, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-J.; Jung, S.-W.; Kim, Y.-E.; Go, D.-S.; Yoon, S.-J. Assessing the Impact of Aging on Burden of Disease. Iran. J. Public Health 2018, 47, 33–38. [Google Scholar] [PubMed]
- Australian Institute of Health and Welfare. The Desire to Age in Place among Older Australians. pp. 1–20. Available online: https://www.aihw.gov.au/getmedia/69a6b0b9-6f86-411c-b15d-943144296250/15141.pdf (accessed on 4 May 2022).
- National Institute on Aging. Aging Well in the 21st Century: Strategic Directions for Research on Aging. Goal C: Develop Effective Interventions to Maintain Health, Well-Being, and Function and Prevent or Reduce the Burden of Age-Related Diseases, Disorders, and Disabilities. Available online: https://www.nia.nih.gov/about/aging-strategic-directions-research (accessed on 3 April 2020).
- National Aged Care Alliance. Ensuring Equity of Access & Outcomes in the Future Aged Care System. Available online: https://naca.asn.au/wp-content/uploads/2018/11/Equity-of-Access-and-Outcomes-Statement-of-Principles_Landscape-1.pdf (accessed on 4 March 2019).
- European Comission. Making Ageing Better: Service Design Can Innovate Senior Care. Available online: https://ec.europa.eu/regional_policy/en/projects/finland/making-ageing-better-service-design-can-innovate-senior-care (accessed on 3 January 2021).
- Australian Bureau of Statistics. Population Projections, 2012 (Bases) to 2101. Available online: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/3222.0main+features32012%20(base)%20to%202101 (accessed on 3 January 2019).
- Carnemolla, P. Ageing in place and the internet of things—How smart home technologies, the built environment and caregiving intersect. Vis. Eng. 2018, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Sponselee, A.; Schouten, B.; Bouwhuis, D.; Willems, C. Smart Home Technology for the Elderly: Perceptions of Multidisciplinary Stakeholders. In Constructing Ambient Intelligence; Mühlhäuser, M., Ferscha, A., Aitenbichler, E., Eds.; Springer: Berlin, Germany, 2007; Volume 11, pp. 314–326. [Google Scholar]
- Bennett, J.; Rokas, O.; Chen, L. Healthcare in the Smart Home: A Study of Past, Present and Future. Sustainability 2017, 9, 840. [Google Scholar] [CrossRef] [Green Version]
- Cook, D.J.; Crandall, A.S.; Thomas, B.L.; Krishnan, N.C. CASAS: A Smart Home in a Box. Computer 2013, 46, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Fritz, R.L.; Dermody, G. A nurse-driven method for developing artificial intelligence in “smart” homes for aging-in-place. Nurs. Outlook 2019, 67, 140–153. [Google Scholar] [CrossRef]
- Fritz, R.L.; Wilson, M.; Dermody, G.; Schmitter-Edgecombe, M.; Cook, D.J. Automated Smart Home Assessment to Support Pain Management: Multiple Methods Analysis. J. Med. Internet Res. 2020, 22, e23943. [Google Scholar] [CrossRef]
- Bae, I.-H. An ontology-based approach to ADL recognition in smart homes. Future Gener. Comput. Syst. 2014, 33, 32–41. [Google Scholar] [CrossRef]
- Williams, J.A.; Cook, D.J. Forecasting behavior in smart homes based on sleep and wake patterns. Technol. Health Care 2017, 25, 89–110. [Google Scholar] [CrossRef] [Green Version]
- Nawaz, A.; Helbostad, J.L.; Skjæret, N.; Vereijken, B.; Bourke, A.; Dahl, Y.; Mellone, S. Designing Smart Home Technology for Fall Prevention in Older People. In HCI International 2014—Posters’ Extended Abstracts; Springer: Cham, Switzerland, 2014; pp. 485–490. [Google Scholar]
- InteliCare Worry Less, Care More. Available online: https://intelicare.com.au/ (accessed on 2 May 2022).
- World Health Organization. Global Strategy on Digital Health 2020–2025. 2021, pp. 1–60. Available online: https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf (accessed on 2 April 2021).
- Dermody, G.; Fritz, R.; Glass, C.; Dunham, M.; Whitehead, L. Factors influencing community-dwelling older adults’ readiness to adopt smart home technology: A qualitative exploratory study. J. Adv. Nurs. 2021, 77, 4847–4861. [Google Scholar] [CrossRef] [PubMed]
- Auernhammer, J.; Roth, B. The origin and evolution of Stanford University’s design thinking: From product design to design thinking in innovation management. J. Prod. Innov. Manag. 2021, 38, 623–644. [Google Scholar] [CrossRef]
- Nedeltcheva, G.N.; Shoikova, E. Coupling Design Thinking, User Experience Design and Agile: Towards Cooperation Framework. In Proceedings of the International Conference on Big Data and Internet of Thing, London, UK, 20–22 December 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 225–229. [Google Scholar]
- Martins, F.; Almeida, M.; Calili, R.; Oliveira, A. Design Thinking Applied to Smart Home Projects: A User-Centric and Sustainable Perspective. Sustainability 2020, 12, 10031. [Google Scholar] [CrossRef]
- Kim, M.J.; Cho, M.E.; Jun, H.J. Developing Design Solutions for Smart Homes Through User-Centered Scenarios. Front. Psychol. 2020, 11, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, M.; Wu, Y. Smart home for elderly care: Development and challenges in China. BMC Geriatr. 2020, 20, 318. [Google Scholar] [CrossRef]
- Sumner, J.; Chong, L.S.; Bundele, A.; Lim, Y.W. Co-Designing Technology for Aging in Place: A Systematic Review. Gerontol. 2020, 61, e395–e409. [Google Scholar] [CrossRef]
- Ellis, G.; Sevdalis, N. Understanding and improving multidisciplinary team working in geriatric medicine. Age Ageing 2019, 48, 498–505. [Google Scholar] [CrossRef]
- Fisk, A.D.; Rogers, W.A.; Charness, N.; Czaja, S.J.; Sharit, J. Designing for Older Adults-Principles and Creative Human Factor Approaches, 2nd ed.; CRC Press Taylor and Francis Group: Boca Raton, FL, USA, 2010. [Google Scholar]
- Reeder, B.; Meyer, E.; Lazar, A.; Chaudhuri, S.; Thompson, H.J.; Demiris, G. Framing the evidence for health smart homes and home-based consumer health technologies as a public health intervention for independent aging: A systematic review. Int. J. Med. Inform. 2013, 82, 565–579. [Google Scholar] [CrossRef] [Green Version]
- Yale School of Nursing Gallup: Nurses Are Most Trusted Profession for 20th Straight Year. Available online: https://nursing.yale.edu/news/gallup-nurses-are-most-trusted-profession-20th-straight-year (accessed on 4 May 2022).
- Rantz, M.J.; Skubic, M.; Popescu, M.; Galambos, C.; Koopman, R.J.; Alexander, G.L.; Phillips, L.J.; Musterman, K.; Back, J.; Miller, S.J. A New Paradigm of Technology-Enabled ‘Vital Signs’ for Early Detection of Health Change for Older Adults. Gerontology 2015, 61, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Dermody, G.; Fritz, R. A conceptual framework for clinicians working with artificial intelligence and health-assistive Smart Homes. Nurs. Inq. 2018, 26, e12267. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demiris, G.; Rantz, M.J.; A Aud, M.; Marek, K.D.; Tyrer, H.W.; Skubic, M.; A Hussam, A. Older adults’ attitudes towards and perceptions of ‘smart home’ technologies: A pilot study. Med. Inform. Internet Med. 2004, 29, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Arthanat, S.; Wilcox, J.; Macuch, M. Profiles and Predictors of Smart Home Technology Adoption by Older Adults. OTJR Occup. Particip. Health 2018, 39, 247–256. [Google Scholar] [CrossRef] [PubMed]
- A Lindeman, D.; Kim, K.K.; Gladstone, C.; Apesoa-Varano, E.C. Technology and Caregiving: Emerging Interventions and Directions for Research. Gerontologist 2020, 60, S41–S49. [Google Scholar] [CrossRef] [PubMed]
- Berridge, C.; Wetle, T.F. Why Older Adults and Their Children Disagree about In-Home Surveillance Technology, Sensors, and Tracking. Gerontologist 2020, 60, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Risling, T. Educating the nurses of 2025: Technology trends of the next decade. Nurse Educ. Pract. 2017, 22, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.; Bardach, S.H.; Pope, N.D. COVID-19 and the Digital Divide: Will Social Workers Help Bridge the Gap? J. Gerontol. Soc. Work 2020, 63, 671–673. [Google Scholar] [CrossRef]
- Ginter, P.M.; Duncan, W.J.; Swayne, L.E. The Strategic Management of Health Care Organizations; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Benjamin, K.; Potts, H.W.J.D.H. Digital transformation in government: Lessons for digital health? Digital Health 2018, 4, 2055207618759168. [Google Scholar] [CrossRef] [Green Version]
- Research Report World. Global Aged Care Services Market Report. Available online: https://www.researchreportsworld.com/-global-aged-care-services-market-17229184 (accessed on 3 January 2021).
- Manchester, H. Co-designing technologies for care: Spaces of co-habitation. In Socio-Gerontechnology; Routledge: London, UK, 2021; pp. 213–227. [Google Scholar]
- Barnett, K.; Livingstone, A.; Margelis, G.; Tomlins, G.; Gould, G.; Capamagian, L.; Alexander, G.; Mason, C.; Young, R. Innovation Driving Care Systems Capability: Final Report; Aged Care Industry IT Company: Murarrie, QLD, Australia, 2020. [Google Scholar]
- Topol, E. Preparing the Healthcare Workforce to Deliver the Digital Future. pp. 1–53. Available online: https://topol.hee.nhs.uk/wp-content/uploads/HEE-Topol-Review-2019.pdf (accessed on 6 April 2021).
- Rantz, M.J.; Porter, R.T.; Cheshier, D.; Otto, D.; Servey, C.H., 3rd; Johnson, R.A.; Aud, M.; Skubic, M.; Tyrer, H.; He, Z.; et al. TigerPlace, a State-Academic-Private Project to Revolutionize Traditional Long-Term Care. J. Hous. Elder. 2008, 22, 66–85. [Google Scholar] [CrossRef] [Green Version]
- Franck, E.; Nauta, J.; de Haan, R. Business Case for Smart Homes. In Handbook of Smart Homes, Health Care and Well-Being; van Hoof, J., Demiris, G., Wouters, E.J.M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 413–426. [Google Scholar]
- Ghods, A.; Caffrey, K.; Lin, B.; Fraga, K.; Fritz, R.; Schmitter-Edgecombe, M.; Hundhausen, C.; Cook, D.J. Iterative Design of Visual Analytics for a Clinician-in-the-Loop Smart Home. IEEE J. Biomed. Health Inform. 2018, 23, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Campos, P.A.; Reich, M.R. Political Analysis for Health Policy Implementation. Health Syst. Reform 2019, 5, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Vanus, J.; Koziorek, J.; Hercík, R. Design of a smart building control with view to the senior citizens’ needs. IFAC Proc. Vol. 2013, 46, 422–427. [Google Scholar] [CrossRef]
- Barker, O. Realizing the Promise of the Internet of Things in Smart Buildings. Computer 2020, 53, 76–79. [Google Scholar] [CrossRef]
- Demiris, G.; Hensel, B.K.; Skubic, M.; Rantz, M. Senior residents’ perceived need of and preferences for “smart home” sensor technologies. Int. J. Technol. Assess. Health Care 2008, 24, 120–124. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Stakeholder Group | Requirements for HSH Integration | Contribution to HSH Integration |
|---|---|---|
| Microsystem | ||
| Older adult & family caregivers (critical at each phase) | Knowledge of the HSH, benefits, and potential challenges How the HSH can meet the goals/needs of an older adult and family caregivers Funding mechanism that addresses initial HSH cost and ongoing service/maintenance fees Offering different levels of HSH that can change with the worsening of chronic conditions | Can be early adopters to test the user-friendliness of the HSH and to determine the aspects still needed to meet their needs |
| Frontline healthcare professionals (critical at idea generation, developing the prototype, testing the mechanism phases) | Education for older adults and their family caregivers Clinical workforce readiness to use HSH in care delivery | Trusted professions, prescribing/gatekeeping role Monitoring of health outcomes Contribute to workforce readiness |
| Social workers (critical at idea generation phase) | Opportunities to collaborate with governmental and non-governmental agencies, policies, or services Connect with HSH stakeholders to share knowledge that may impact the integration of the HSH | Determine the social complexities that impact aging-in-place of the older adult; connect older adult governmental and non-governmental agencies, policies, or services |
| Multidisciplinary research teams (critical at each phase) | Funding and supportive academic and clinical environments to conduct research Studies that show clinical effectiveness and cost-effectiveness of the HSH Studies that show that the HSH is meeting the needs/expectations of older adults and family caregivers and clinicians | Findings from pragmatic clinical trials on the clinical effectiveness of the HSH The impact of HSH on older adults and family caregivers’ needs/desires; and clinician end-user experiences/perceptions regarding the HSH and clinical decision-making Cost-benefit analysis |
| Academic or educator roles (critical at defining the problem, idea generation phases) | Increased digital literacy in health professional’s education standards Increased educational materials developed for the public about HSH and how it can support older adults and family caregivers | Development of curriculum for allied health professions; educational material for older adults and family caregivers, and education on the HSH |
| Mesosystem | ||
| Health care organizations (critical at defining the problem, idea, and testing phases) | New models of care delivery using HSH Enable prescriptions for HSH Robust technology infrastructure and supports | Development of new models of care Clinical policies and procedures |
| Aged-care organizations (critical at defining the problem, idea generation, and testing phases) | Clinical workforce readiness to use HSH in care delivery Data visualizations that make sense for clinicians, and integration into existing electronic health record systems need a mechanism by which equitable access to the HSH is available to all older adults including low/lower income | Early adopters of HSH in retirement villages/apartments. Provides a platform to provide education to the public, older adults, and family caregivers Collaborate with the multidisciplinary research team |
| HSH Companies: Computer science & electrical engineering teams, entrepreneurs, start-ups, companies (critical at all phases) | Clinical significance of monitored health behavior to refine machine learning Data visualizations that make sense for clinicians, and integration into existing electronic health record systems Privacy/data security Business development and strategies for scaling up | Development of algorithms & artificial intelligent agent Clinician dashboard Sensor development and further innovation (e.g., gait analysis in the home, accommodating for pets) Formation of start-up companies to advance the practical manufacturing of HSH with minimal cost and clinical effectiveness and user-friendliness for older adults, families, and the clinical workforce |
| Master system integrator (MSI) (critical at developing the prototype, and testing phases) | Collaboration with technicians and building experts | Balances the depth and breadth of knowledge required to design and manage smart building systems on a short and long-term basis Connects the multidisciplinary team members with trade contractors and coordinates trade teams for effective design, implementation, and evaluation |
| Macrosystem | ||
| Health care policymakers (critical at empathizing, defining a problem, testing phases) | Policies and standards for the HSH if covered by aged care packages public health funding Integration of HSH into aged care packages/ public funding Policies and standards developed for privacy and data management of HSH data | Development of health care policy with corresponding mechanisms for prescribers and payment, ensuring that all older adults have access to the HSH |
| Special interest groups/advocates (critical at Testing phase) | Knowledge and understanding of how the HSH can benefit | Advocacy, dissemination of education |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dermody, G.; Mikus, J.; Porock, D.; Sugarman, D.; Janjua, N.K.; How, C.; Fritz, R. Perspectives on Wider Integration of the Health-Assistive Smart Home. J. Ageing Longev. 2022, 2, 140-152. https://doi.org/10.3390/jal2020013
Dermody G, Mikus J, Porock D, Sugarman D, Janjua NK, How C, Fritz R. Perspectives on Wider Integration of the Health-Assistive Smart Home. Journal of Ageing and Longevity. 2022; 2(2):140-152. https://doi.org/10.3390/jal2020013
Chicago/Turabian StyleDermody, Gordana, Jenna Mikus, Davina Porock, Dov Sugarman, Naeem K. Janjua, Christopher How, and Roschelle Fritz. 2022. "Perspectives on Wider Integration of the Health-Assistive Smart Home" Journal of Ageing and Longevity 2, no. 2: 140-152. https://doi.org/10.3390/jal2020013
APA StyleDermody, G., Mikus, J., Porock, D., Sugarman, D., Janjua, N. K., How, C., & Fritz, R. (2022). Perspectives on Wider Integration of the Health-Assistive Smart Home. Journal of Ageing and Longevity, 2(2), 140-152. https://doi.org/10.3390/jal2020013