
Group-Based Physical Activity Interventions Targeting Enjoyment in Older Adults: A Systematic Review




Abstract
:1. Introduction
1.1. Physical Activity for Older Adults
1.2. Enjoyment as a Predictor of Physical Activity
1.3. Behaviour Change and Maintenance
1.4. Aim of This Review
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis
3. Results
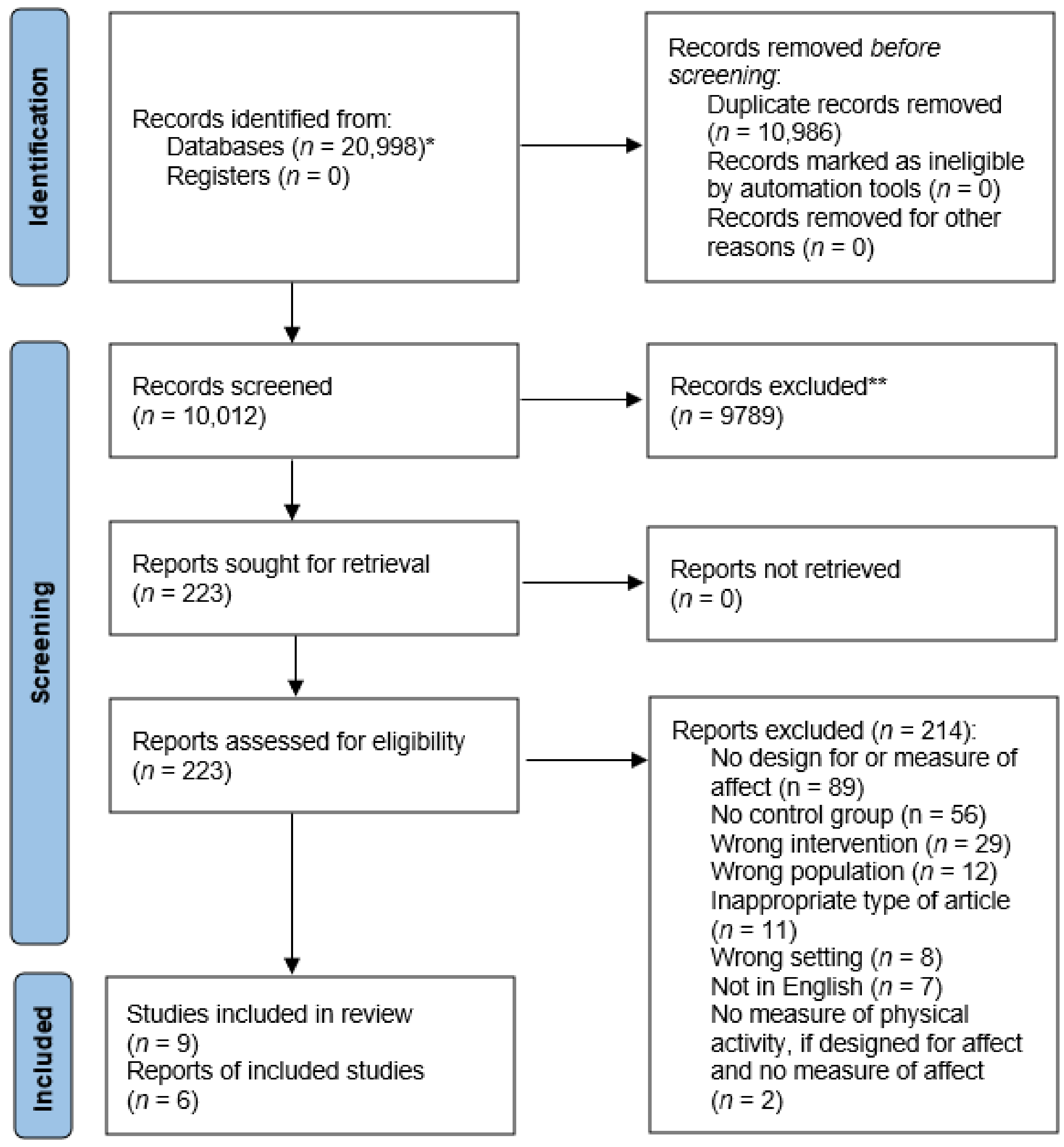
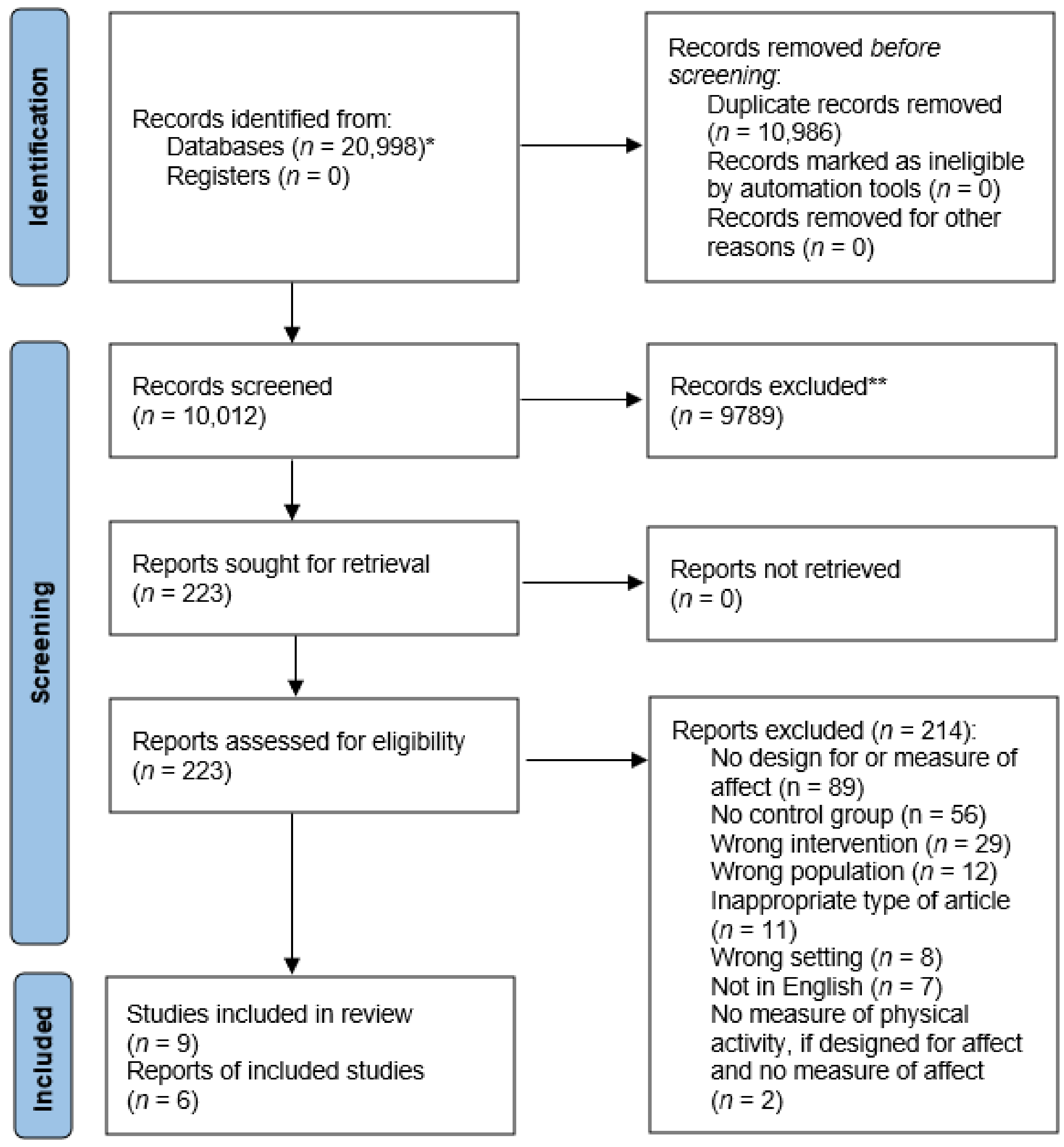
3.1. Study Selection
3.2. Study Characteristics
3.3. Intervention Descriptions
3.3.1. Behaviour Change Techniques
3.3.2. Behaviour Change Theory
3.4. Results of Individual Studies
3.4.1. Quantitative Findings
Enjoyment Outcome Measures
Physical Activity Outcome Measures
Adherence Outcome Measures
3.4.2. Qualitative Findings
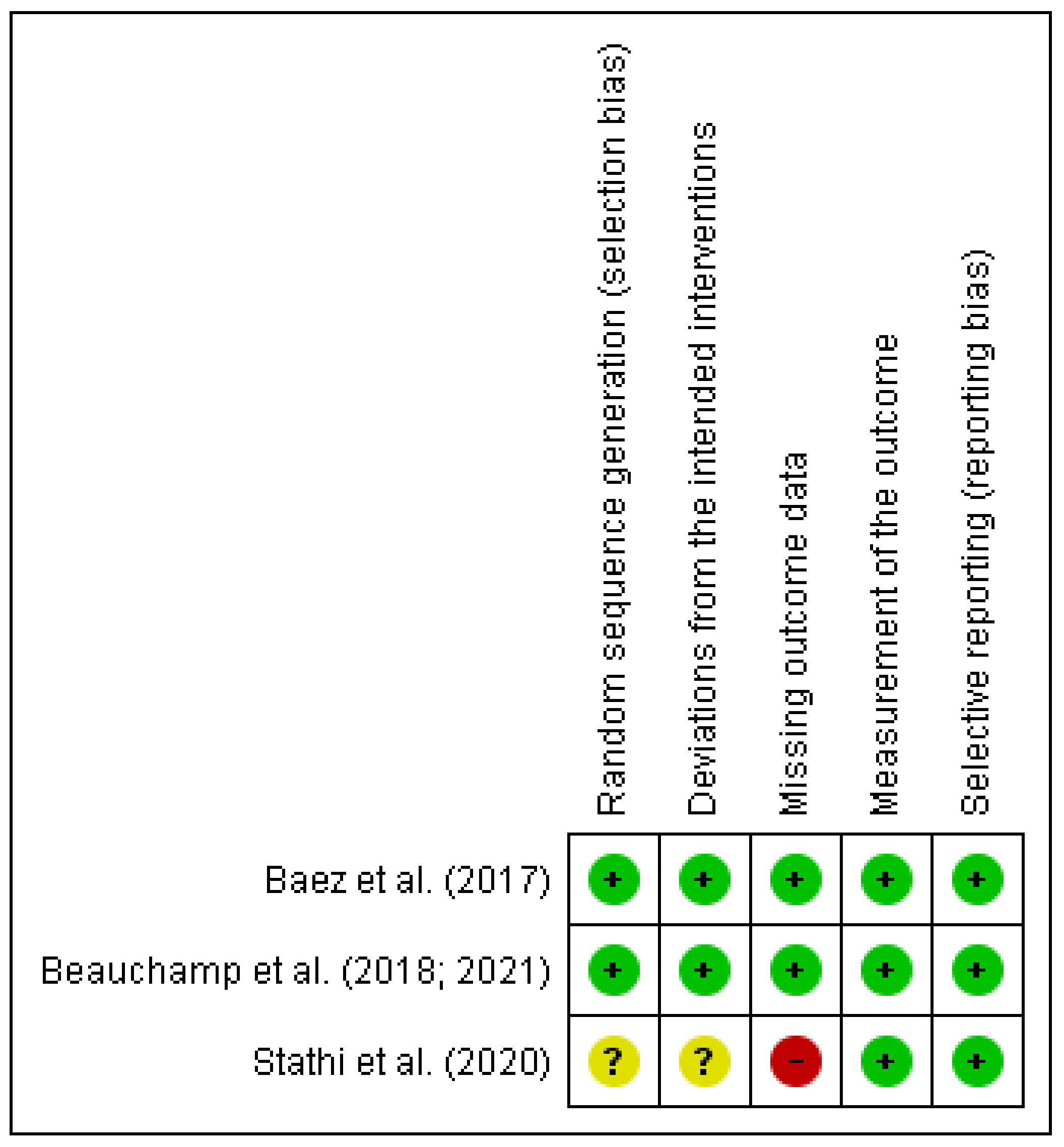
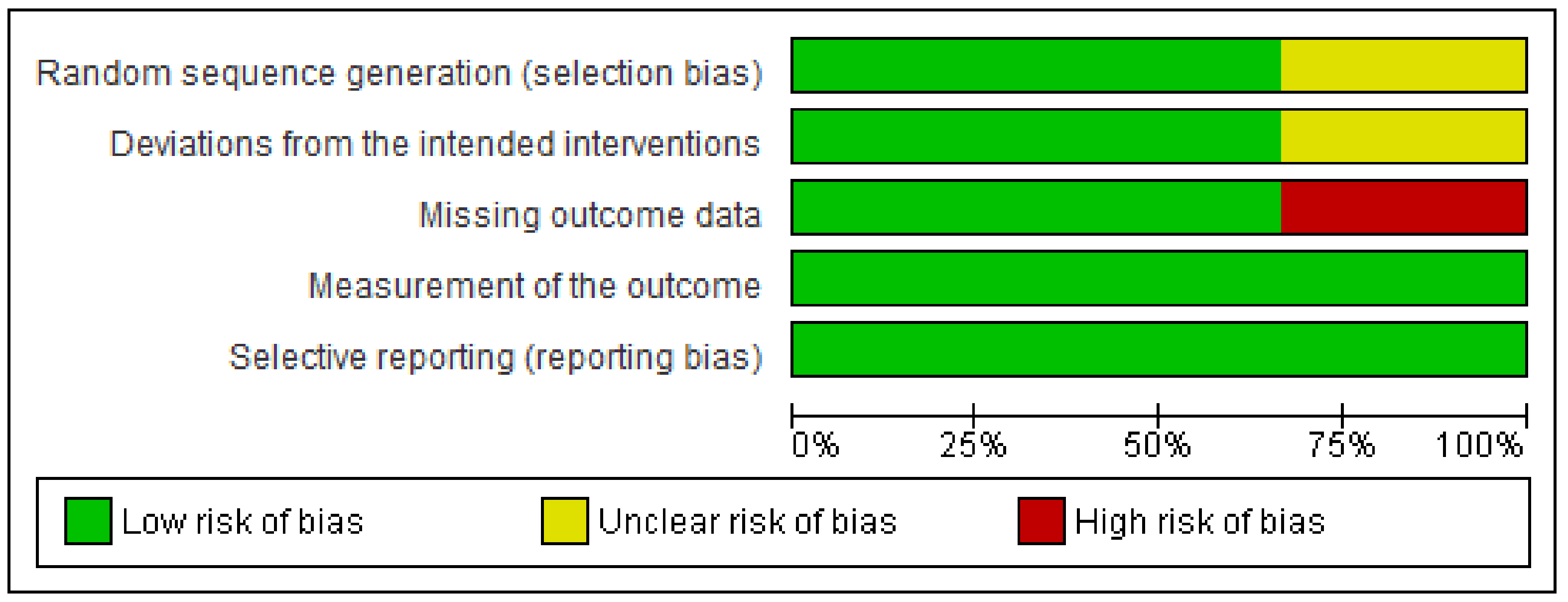
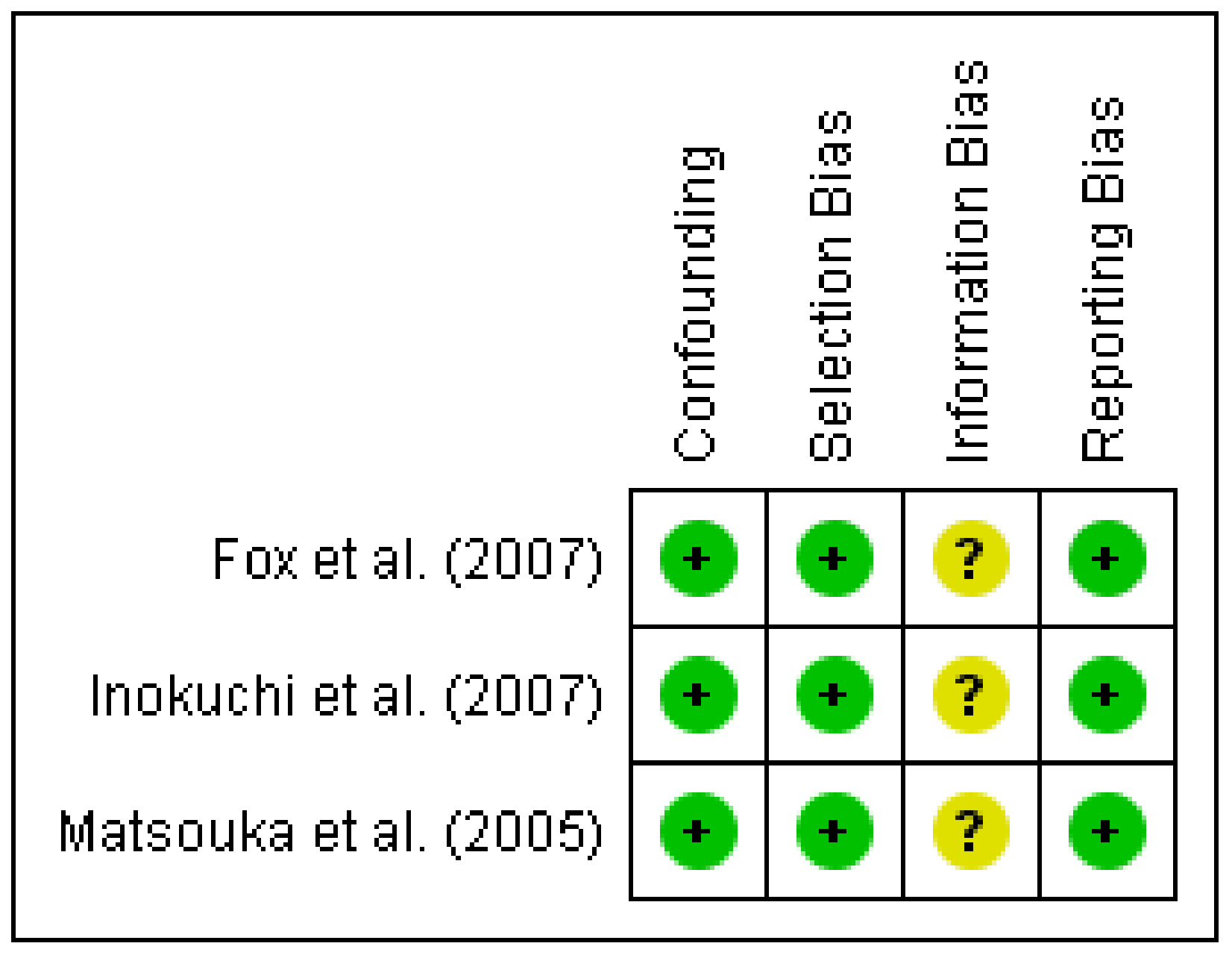
3.5. Risk of Bias
4. Discussion
4.1. Features of Enjoyable Group-Based Exercise
4.1.1. Identifying as Part of a Group That Exercises Together
4.1.2. Identifying as an Exerciser Who Meets in a Group
4.2. Limitations of Evidence
4.3. Implications for Practice, Policy and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bangsbo, J.; Blackwell, J.; Evans, A.B.; Gliemann, L.; Lundbye-Jensen, J.; Hellsten, Y.; Boraxbekk, C.J.; Caserotti, P.; Troelsen, J.; Dela, F.; et al. Copenhagen Consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Agostino, D.; Daskalopoulou, C.; Wu, Y.-T.; Koukounari, A.; Haro, J.M.; Tyrovolas, S.; Panagiotakos, D.B.; Prince, M.; Prina, A.M. The impact of physical activity on healthy ageing trajectories: Evidence from eight cohort studies. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, P.L.; Abdurahman, A.; Gabay, A.S.; Drew, D.; Tamm, M.; Husain, M.; Apps, M.A.J. Aging Increases Prosocial Motivation for Effort. Psychol. Sci. 2021, 32, 668–681. [Google Scholar] [CrossRef]
- Piggin, J. What Is Physical Activity? A Holistic Definition for Teachers, Researchers and Policy Makers. Front. Sports Act. Living 2020, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ekkekakis, P.; Hargreaves, E.A.; Parfitt, G. Invited Guest Editorial: Envisioning the next fifty years of research on the exercise–affect relationship. Psychol. Sport Exerc. 2013, 14, 751–758. [Google Scholar] [CrossRef]
- Devereux-Fitzgerald, A.; Powell, R.; Dewhurst, A.; French, D.P. The acceptability of physical activity interventions to older adults: A systematic review and meta-synthesis. Soc. Sci. Med. 2016, 158, 14–23. [Google Scholar] [CrossRef]
- Stevens, C.J.; Baldwin, A.S.; Bryan, A.D.; Conner, M.; Rhodes, R.E.; Williams, D.M. Affective Determinants of Physical Activity: A Conceptual Framework and Narrative Review. Front. Psychol. 2020, 11, 1–19. [Google Scholar] [CrossRef]
- Michie, S.; Wood, C.E.; Johnston, M.; Abraham, C.; Francis, J.J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol. Assess. 2015, 19, 1–188. [Google Scholar]
- Marcus, B.H.; King, T.K.; Clark, M.M.; Pinto, B.M.; Bock, B.C. Theories and techniques for promoting physical activity behaviours. Sports Med. 1996, 22, 321–331. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Martin, A.D.; Taunton, J.E.; Rhodes, E.C.; Donnelly, M.; Elliot, J. Factors associated with exercise adherence among older adults—An individual perspective. Sports Med. 1999, 28, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Van Stralen, M.M.; De Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. Determinants of initiation and maintenance of physical activity among older adults: A literature review. Health Psychol. Rev. 2009, 3, 147–207. [Google Scholar] [CrossRef]
- McGowan, L.J.; Devereux-Fitzgerald, A.; Powell, R.; French, D.P. How acceptable do older adults find the concept of being physically active? A systematic review and meta-synthesis. Int. Rev. Sport Exerc. Psychol. 2018, 11, 1–24. [Google Scholar] [CrossRef]
- Wiersma, L.D. Conceptualization and development of the sources of enjoyment in youth sport questionnaire. Meas. Phys. Educ. Exerc. Sci. 2001, 5, 153–177. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Elbers, R.G.; Blencowe, N.S.; Cheng, H.Y.; McAleenan, A.; Tilling, K.; Whiting, P.F.; Higgins, J.P.T.; Reeves, B.C.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman Andrew, D.; Vist Gunn, E.; Regina, K.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann Holger, J. Rating Quality of Evidence and Strength of Recommendations: GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ Br. Med. J. 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, M.R.; Harden, S.M.; Wolf, S.A.; Rhodes, R.E.; Liu, Y.; Dunlop, W.L.; Schmader, T.; Sheel, A.W.; Zumbo, B.D.; Estabrooks, P.A. Group based physical Activity for oLder adults (GOAL) randomized controlled trial: Study protocol. BMC Public Health 2015, 15, 592. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, M.R.; Ruissen, G.R.; Dunlop, W.L.; Estabrooks, P.A.; Harden, S.M.; Wolf, S.A.; Liu, Y.; Schmader, T.; Puterman, E.; Sheel, A.W. Group-based physical activity for older adults (GOAL) randomized controlled trial: Exercise adherence outcomes. Health Psychol. 2018, 37, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.R.; Liu, Y.; Dunlop, W.L.; Ruissen, G.R.; Schmader, T.; Harden, S.M.; Wolf, S.A.; Puterman, E.; Sheel, A.W.; Rhodes, R.E. Psychological mediators of exercise adherence among older adults in a group-based randomized trial. Health Psychol. 2021, 40, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Bennett, E.V.; Clarke, L.H.; Wolf, S.A.; Dunlop, W.L.; Harden, S.M.; Liu, Y.; Estabrooks, P.A.; Rhodes, R.E.; Beauchamp, M.R. Older adults’ experiences of group-based physical activity: A qualitative study from the ‘GOAL’ randomized controlled trial. Psychol. Sport Exerc. 2018, 39, 184–192. [Google Scholar] [CrossRef]
- Matsouka, O.; Kabitsis, C.; Harahousou, Y.; Trigonis, I. Mood alterations following an indoor and outdoor exercise program in healthy elderly women. Percept. Mot. Ski. 2005, 100, 707–715. [Google Scholar] [CrossRef]
- Stathi, A.; Withall, J.; Thompson, J.L.; Davis, M.G.; Gray, S.; de Koning, J.; Parkhurst, G.; Lloyd, L.; Greaves, C.; Laventure, R. Feasibility Trial Evaluation of a Peer Volunteering Active Aging Intervention: ACE (Active, Connected, Engaged). Gerontologist 2020, 60, 571–582. [Google Scholar] [CrossRef]
- Inokuchi, S.; Matsusaka, N.; Hayashi, T.; Shindo, H. Feasibilty and effectiveness of a nurse-led community exercise programme for prevention of falls among frail elderly people: A multi-centre controlled trial. J. Rehabil. Med. 2007, 39, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Fox, K.; Stathi, A.; McKenna, J.; Davis, M. Physical activity and mental well-being in older people participating in the Better Ageing Project. Eur. J. Appl. Physiol. 2007, 100, 591–602. [Google Scholar] [CrossRef]
- Baez, M.; Far, I.K.; Ibarra, F.; Ferron, M.; Didino, D.; Casati, F. Effects of online group exercises for older adults on physical, psychological and social wellbeing: A randomized pilot trial. PeerJ 2017, 5, e3150. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Facilitating Optimal Motivation and Psychological Well-Being Across Life’s Domains. Can. Psychol. Psychol. Can. 2008, 49, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.C.; Hogg, M.A.; Oakes, P.J.; Reicher, S.D.; Wetherell, M.S. Rediscovering the Social Group: A Self-Categorization Theory; Basil Blackwell: Cambridge, MA, USA, 1987; p. 239. [Google Scholar]
- Greaves, C. Supporting health behaviour change in general practice. In Psychology and Diabetes Care; Barnard, K.D., Lloyd, C.E., Eds.; Springer: London, UK, 2012. [Google Scholar]
- Netz, Y.; Wu, M.J.; Becker, B.J.; Tenenbaum, G. Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychol. Aging 2005, 20, 272–284. [Google Scholar] [CrossRef] [Green Version]
- Gellert, P.; Ziegelmann, J.P.; Schwarzer, R. Affective and health-related outcome expectancies for physical activity in older adults. Psychol. Health 2012, 27, 816–828. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268. [Google Scholar] [CrossRef] [PubMed]
- Bethancourt, H.J.; Rosenberg, D.E.; Beatty, T.; Arterburn, D.E. Barriers to and facilitators of physical activity program use among older adults. Clin. Med. Res. 2014, 12, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEwan, D.; Bennett, E.V.; Rhodes, R.E. Collaboration behaviors within interactive exercise groups. Psychol. Health 2020, 36, 1066–1087. [Google Scholar] [CrossRef]
- Burke, S.; Carron, A.; Eys, M.; Ntoumanis, N.; Estabrooks, P. Group versus Individual Approach? A Meta-Analysis of the Effectiveness of Interventions to promote physical activity. Sport Exer. Psychol. Rev. 2005, 2, 19–35. [Google Scholar]
- Olanrewaju, O.; Kelly, S.; Cowan, A.; Brayne, C.; Lafortune, L. Physical Activity in Community Dwelling Older People: A Systematic Review of Reviews of Interventions and Context. PLoS ONE 2016, 11, e0168614. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977; p. 247. [Google Scholar]
- Crozier, A.; Buckley, B.J.R.; Watson, P.M.; Porcellato, L. Facilitators and challenges in delivering a peer-support physical activity intervention for older adults: A qualitative study with multiple stakeholders. BMC Public Health 2020, 20, 1904. [Google Scholar] [CrossRef]
- O’Brien, N.; McDonald, S.; Araujo-Soares, V.; Lara, J.; Errington, L.; Godfrey, A.; Meyer, T.D.; Rochester, L.; Mathers, J.C.; White, M.; et al. The features of interventions associated with long-term effectiveness of physical activity interventions in adults aged 55–70 years: A systematic review and meta-analysis. Health Psychol. Rev. 2015, 9, 417–433. [Google Scholar] [CrossRef]
- Dunlop, W.L.; Falk, C.F.; Beauchamp, M.R. How dynamic are exercise group dynamics? Examining changes in cohesion within class-based exercise programs. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2013, 32, 1240–1243. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Age (Years) Mean (SD) | Sample Size | Gender (% Female) | Study Design | Control Group | Participants’ Characteristics | Enjoyment Aspect of Design | Enjoyment Related Outcome Measures | Measurement Timepoints |
|---|---|---|---|---|---|---|---|---|---|---|
| Baez, et al., (2017) [29] | Italy | 70.9 (5.7) | Total: 37; I = 20; C = 17 | 73% | Randomised pilot trial | Standard individual home-based training program | Ranging from non-frail to mild frailty level | Investigating the relationship between enjoyment in physical activity and adherence | PACES: 16 items (5 points per item) | Week 0 Week 10 |
| Beauchamp, et al., (2018, 2021) [22,23] | Canada | 71.57 (5.4) | Total: 627; I(SASG) = 236; I(SAMG) = 210; C(MAMG) = 181 | 71% | Randomised controlled trial | Standard exercise group composed of mixed age and gender | Health status mainly good–very good, married (50.6%), White (82.1%), retired (79.1%) | Affective attitudes towards physical activity predicted as mediators of adherence, in grouping similar identities together | Affective attitudes towards physical activity: three semantic differential items (7 points per item) | Week 12 Week 24 |
| Fox, et al., (2007) [28] | Italy, France, England | 75.6 (3.9) | Total: 176; I = 112; C = 64 | 56% | Non-randomised controlled trial | No intervention: healthy younger adults aged 20–37 years (n = 45) | Majority with no serious conditions of ill health, at least secondary-level educated, married | Investigating the relationship between engagement in physical activity and mood | Enjoyment as a qualitative theme on the effect on participants well-being | Week 52 a 8–12 months post-intervention b |
| Inokuchi, et al., (2007) [27] | Japan | 80.8 (6.5) | Total: 268; I = 144; C = 124 | 84% | Multi-centre non-randomised controlled trial | Weekly social programmes in day centre | Criteria included 5 or more risk factors for falls | Recreational tea breaks were explicit in the design to encourage friendly relations | NR | NR |
| Matsouka, et al., (2005) [25] | Greece | 64.8 (4.7) | Total 55; I = 45; C = 10 | 100% | Non-randomised controlled trial | Non-exercisers (members of the Public Care Institutes for the Elderly) | Inactive female-exclusive criteria, members of Public Care Institutes for the Elderly (PCIE) | Groups were designed to meet 0, 1, 2, and 3 times per week, examining the effect of group exercise frequency on mood | Exercise-induced feeling inventory, positive engagement subscale: 12 items (5 points per item) | Week 0 Week 12 |
| Stathi, et al., (2020) [26] | UK | 73.8 (6.9) | Total: 39; EG = 22; CG = 17 | 44% | Feasibility randomised controlled trial | Waiting-list control group | Sedentary, retired, inactive c, capable of walking at least 200 m, and no diagnosis of dementia | Designed to support socially disengaged and inactive older adults to get out of the house and celebrate achievements | NR | NR |
| Author (Year) | Physical Aspect of Intervention | Social Aspect of Intervention | Basis of Exercise Program | Who Delivered the Intervention | Mode of Delivery | Setting | Length (Weeks) | No. Session per Week | Session Duration (Mins) | How Adherence Was Assessed | Adherence | Theory |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baez, et al. (2017) [29] | Muscle strengthening and balance retraining exercises | Virtual gym classes with messaging and persuasion features | OTAGO falls prevention programme | Training coach | Gym central trainee mobile app | Online | 8 | 2+ | 30–40 | 1. % of sessions attended 2. % length of exercise videos watched | 1. 85% sessions attended 2. Mean (SD) 91.75% (12.46) | NR |
| Beauchamp, et al., (2018, 2021) [22,23] | Moderate-intensity exercises | Exerciser t-shirts and post-workout gatherings, delivered by older adults | GOAL trial informed by Lively Lads case study | Peer facilitators | Face to face | YMCA centre | 24 | 3 | 50–60 | Electronic attendance records from access cards | Week 12: 52.2% a Week 24: 45.1% a | Self-categorization theory, social cognitive theory, theory of planned behaviour |
| Fox, et al., (2007) [28] | Aerobic exercise, machine-based strength training, Tai Chi, and flexibility exercise | Initial intensive support and social opportunities | Better Ageing Project | Researchers and exercise professionals | Face to face | University Campus Health and Wellness Clubs | 52 | Centre = 2; Home = 1 | 60–90 | Class register and home log | 93% attendance at exercise classes and 85% for home exercises | NR |
| Inokuchi, et al., (2007) [27] | Stretching and strengthening exercises against gravity and balance retraining exercises included stepping, tandem walking, and sideways walking | Recreational and tea breaks | Nurse-led falls prevention exercise programme | Nurse-led | Face to face | Community centre | 17 | Centre = 1 (supplemented by daily home exercises) | 120 | Class register and home log | 90.9% attendance at classes Home exercises: Mean = 4.3 days a week | NR |
| Matsouka, et al., (2005) [25] | Flexibility, strength, coordination (outdoor and indoor leisure activities, callisthenic exercises), aerobic (walking and aerobic exercises), flexibility, balance, agility, muscular coordination (games and recreational activities) | Focus on leisure and recreational activities | Training programme based on “Long-term Physical Activity Workshop” for isolated older adults | Trained exercise specialist | Face to face | Public Care Institutes for the Elderly | 11 | 1–3 | 45 | NR | NR | NR |
| Stathi, et al., (2020) [26] | Promotion of a range of local physical and non-physical activity opportunities | Initial individual peer support and joint visits, two group social events | Active, Connected, Engaged (ACE) programme | Peer led by trained activators | Introduction to community face-to-face groups | Existing community groups | 24 | NR | NR | % of sessions with their activator attended | 100% | Self-determination theory |
| Affect | BCTs | Theory | |
|---|---|---|---|
| Environmental | Welcoming, supportive (instructor), providing opportunities to interact— exercise programme or externally | Adding objects to the environment (exercise aids); restructuring the social environment (online, tea-breaks, activity opportunities) | Self- categorization theory (group cohesion) Self- determination theory (social support—competence) |
| Social | Company—shared experience, perceived similarity, building a sense of community | Social support—messaging, post-workout, and social events | |
| Interpersonal | Courage—supporting, interacting, caring, expressing (laughing) | ||
| Individual | Competence—performance, achievement, Confidence—self-worth, knowledge, satisfaction (noticing and valuing effort and benefits for daily life) | Instruction and demonstration on how to perform behaviour (training tips, manual, handout, videos) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Creighton, R.M.; Paradis, K.F.; Blackburn, N.E.; Tully, M.A. Group-Based Physical Activity Interventions Targeting Enjoyment in Older Adults: A Systematic Review. J. Ageing Longev. 2022, 2, 113-129. https://doi.org/10.3390/jal2020011
Creighton RM, Paradis KF, Blackburn NE, Tully MA. Group-Based Physical Activity Interventions Targeting Enjoyment in Older Adults: A Systematic Review. Journal of Ageing and Longevity. 2022; 2(2):113-129. https://doi.org/10.3390/jal2020011
Chicago/Turabian StyleCreighton, Rachel M., Kyle F. Paradis, Nicole E. Blackburn, and Mark A. Tully. 2022. "Group-Based Physical Activity Interventions Targeting Enjoyment in Older Adults: A Systematic Review" Journal of Ageing and Longevity 2, no. 2: 113-129. https://doi.org/10.3390/jal2020011
APA StyleCreighton, R. M., Paradis, K. F., Blackburn, N. E., & Tully, M. A. (2022). Group-Based Physical Activity Interventions Targeting Enjoyment in Older Adults: A Systematic Review. Journal of Ageing and Longevity, 2(2), 113-129. https://doi.org/10.3390/jal2020011