
Food Insecurity Is Associated with Cognitive Function: A Systematic Review of Findings across the Life Course

 ,
, 

Abstract
:1. Introduction
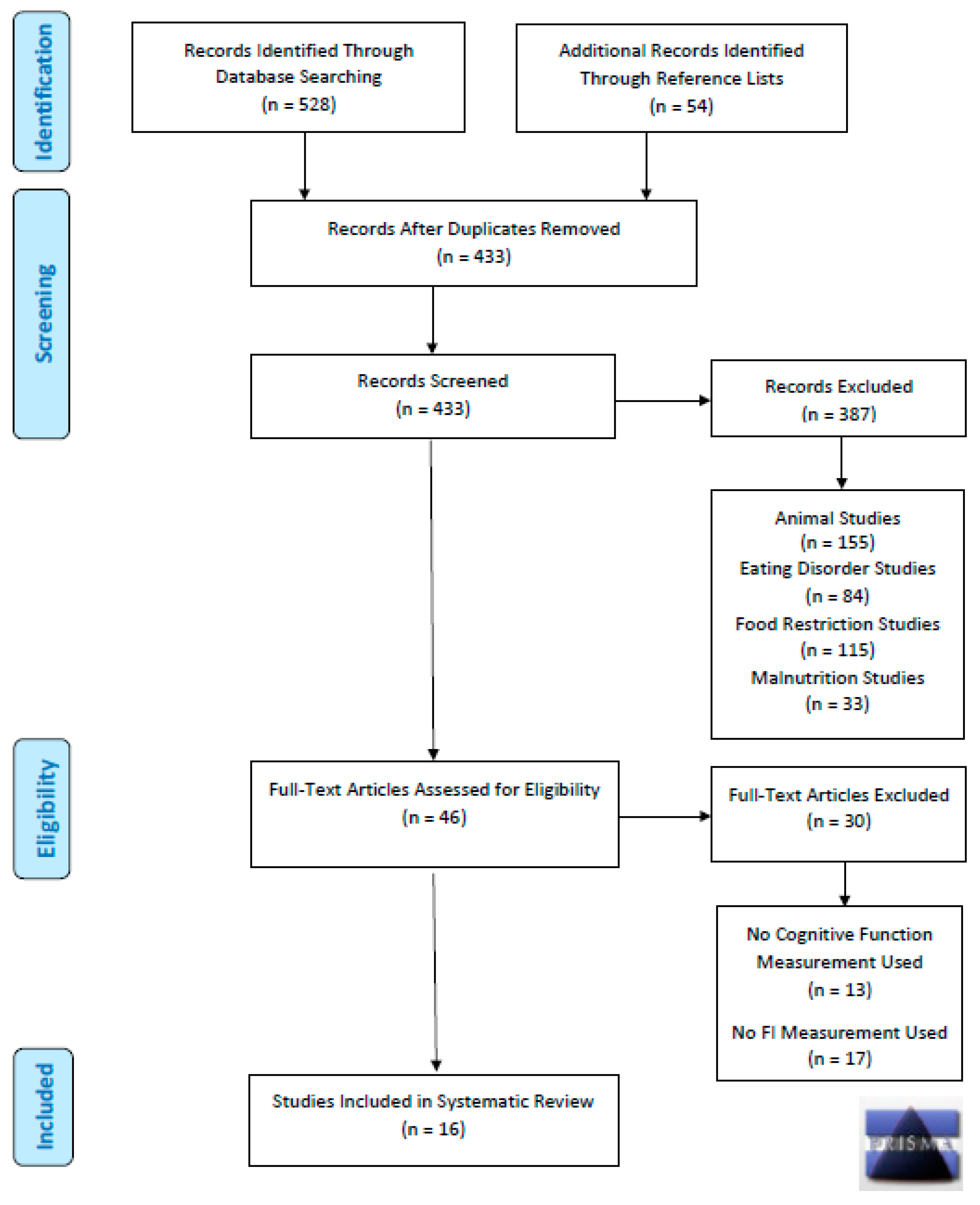
2. Materials and Methods
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United States Department of Agriculture (USDA)—Economic Research Service. Definitions of Food Security. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security.aspx (accessed on 1 September 2021).
- Coleman Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2019; United States Department of Agriculture: Washington, DC, USA, 2020; p. 47.
- Drennen, C.R.; Coleman, S.M.; de Cuba, S.E.; Frank, D.A.; Chilton, M.; Cook, J.T.; Cutts, D.B.; Heeren, T.; Casey, P.H.; Black, M.M. Food Insecurity, Health, and Development in Children Under Age Four Years. Pediatrics 2019, 144, e20190824. [Google Scholar] [CrossRef] [Green Version]
- Frongillo, E. Advancing Knowledge of How and Why Food Insecurity Is Associated with Poor Well-Being in Families and Individuals across the Life Course. J. Acad. Nutr. Diet. 2019, 119, 1621–1622. [Google Scholar] [CrossRef]
- Phojanakong, P.; Brown-Weida, E.; Grimaldi, G.; Lê-Scherban, F.; Chilton, M. Experiences of Racial and Ethnic Discrimination Are Associated with Food Insecurity and Poor Health. Int. J. Environ. Res. Public Health 2019, 16, 4369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gundersen, C.; Ziliak, J.P. Food insecurity and health outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gundersen, C.; Kreider, B. Bounding the effects of food insecurity on children’s health outcomes. J. Health Econ. 2009, 28, 971–983. [Google Scholar] [CrossRef] [PubMed]
- Ashiabi, G. Household food insecurity and children’s school engagement. J. Child. Poverty 2005, 11, 3–17. [Google Scholar] [CrossRef]
- Whitaker, R.C.; Phillips, S.M.; Orzol, S.M. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics 2006, 118, e859–e868. [Google Scholar] [CrossRef]
- McIntyre, L.; Williams, J.V.; Lavorato, D.H.; Patten, S. Depression and suicide ideation in late adolescence and early adulthood are an outcome of child hunger. J. Affect. Disord. 2013, 150, 123–129. [Google Scholar] [CrossRef]
- Huang, J.; Matta Oshima, K.M.; Kim, Y. Does food insecurity affect parental characteristics and child behavior? Testing mediation effects. Soc. Serv. Rev. 2010, 84, 381–401. [Google Scholar] [CrossRef] [Green Version]
- Jyoti, D.F.; Frongillo, E.A.; Jones, S.J. Food insecurity affects school children’s academic performance, weight gain, and social skills. J. Nutr. 2005, 135, 2831–2839. [Google Scholar] [CrossRef]
- Esfandiari, S.; Omidvar, N.; Eini-Zinab, H.; Doustmohammadian, A.; Amirhamidi, Z. Associations Among Food Insecurity, Academic Performance, and Weight Status in Primary Schoolchildren in Tehran, Iran: A Cross-sectional Study. J. Nutr. Educ. Behav. 2018, 50, 109–117. [Google Scholar] [CrossRef]
- Winicki, J.; Jemison, K. Food insecurity and hunger in the kindergarten classroom: Its effect on learning and growth. Contemp. Econ. Policy 2003, 21, 145–157. [Google Scholar] [CrossRef]
- Vozoris, N.T.; Tarasuk, V.S. Household food insufficiency is associated with poorer health. J. Nutr. 2003, 133, 120–126. [Google Scholar] [CrossRef]
- Seligman, H.K.; Laraia, B.A.; Kushel, M.B. Food insecurity is associated with chronic disease among low-income NHANES participants. J. Nutr. 2009, 140, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, M.; Keiley, M.K.; Garza, K.B.; Duffy, P.A.; Zizza, C.A. Food insecurity is associated with poor sleep outcomes among US adults. J. Nutr. 2014, 145, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Maddocks, E.; Chen, Y.; Gilman, S.; Colman, I. Food insecurity and mental illness: Disproportionate impacts in the context of perceived stress and social isolation. Public Health 2016, 132, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Chaudry, A.; Wimer, C. Poverty is not just an indicator: The relationship between income, poverty, and child well-being. Acad. Pediatr. 2016, 16, S23–S29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durao, S.; Visser, M.E.; Ramokolo, V.; Oliveira, J.M.; Schmidt, B.-M.; Balakrishna, Y.; Brand, A.; Kristjansson, E.; Schoonees, A. Community-level interventions for improving access to food in low-and middle-income countries. Cochrane Database Syst. Rev. 2020, 7, CD011504. [Google Scholar] [CrossRef] [Green Version]
- Champakam, S.; Srikantia, S.; Gopalan, C. Kwashiorkor and mental development. Am. J. Clin. Nutr. 1968, 21, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Hoorweg, J.C. Protein-Energy Malnutrition and Intellectual Abilities: A Study of Teen-Age Ugandan Children; Walter de Gruyter GmbH & Co KG: Berlin, Germany, 2019; Volume 5. [Google Scholar]
- Galler, J.R.; Ramsey, F. A follow-up study of the influence of early malnutrition on development: V. Delayed development of conservation (Piaget). J. Am. Acad. Child Adolesc. Psychiatry 1987, 26, 23–27. [Google Scholar] [CrossRef]
- Upadhyay, S.; Agarwal, D.; Shastri, J.; Agarwal, K. Persistence of soft neurological signs in chronic undernourished children. Nutr. Res. 1995, 15, 193–199. [Google Scholar] [CrossRef]
- Martorell, R. Undernutrition during pregnancy and early childhood and its consequences for cognitive and behavioral development. Early Child Dev. Investig. Our Child. Future 1997, 39–83. [Google Scholar]
- Mendez, M.A.; Adair, L.S. Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. J. Nutr. 1999, 129, 1555–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kar, B.R.; Rao, S.L.; Chandramouli, B. Cognitive development in children with chronic protein energy malnutrition. Behav. Brain Funct. 2008, 4, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rooij, S.R.; Wouters, H.; Yonker, J.E.; Painter, R.C.; Roseboom, T.J. Prenatal undernutrition and cognitive function in late adulthood. Proc. Natl. Acad. Sci. USA 2010, 107, 16881–16886. [Google Scholar] [CrossRef] [Green Version]
- Misra, U.; Kalital, J.; Kumar, S.; Poptani, H.; Agarwal, D.; Agarwal, K. Brain MRI and cognitive evoked potentials in rural chronically undernourished children. Nutr. Res. 1996, 16, 1147–1151. [Google Scholar] [CrossRef]
- Agarwal, K.; Das, D.; Agarwal, D.; Upadhyay, S.; Mishra, S. Soft neurological signs and EEG pattern in rural malnourished children. Acta Pædiatr. 1989, 78, 873–878. [Google Scholar] [CrossRef]
- Benı́tez-Bribiesca, L.; De la Rosa-Alvarez, I.; Mansilla-Olivares, A. Dendritic spine pathology in infants with severe protein-calorie malnutrition. Pediatrics 1999, 104, e21. [Google Scholar] [CrossRef] [Green Version]
- Hay, P.J.; Sachdev, P. Brain dysfunction in anorexia nervosa: Cause or consequence of under-nutrition? Curr. Opin. Psychiatry 2011, 24, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Sarrar, L.; Holzhausen, M.; Warschburger, P.; Pfeiffer, E.; Lehmkuhl, U.; Schneider, N. Cognitive function in adolescent patients with anorexia nervosa and unipolar affective disorders. Eur. Eat. Disord. Rev. 2016, 24, 232–240. [Google Scholar] [CrossRef]
- Jones, B.P.; Duncan, C.C.; Brouwers, P.; Mirsky, A.F. Cognition in eating disorders. J. Clin. Exp. Neuropsychol. 1991, 13, 711–728. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Anton, S.D.; Han, H.; York-Crowe, E.; Redman, L.M.; Ravussin, E.; Williamson, D.A. Examination of cognitive function during six months of calorie restriction: Results of a randomized controlled trial. Rejuvenation Res. 2007, 10, 179–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solianik, R.; Sujeta, A.; Čekanauskaitė, A. Effects of 2-day calorie restriction on cardiovascular autonomic response, mood, and cognitive and motor functions in obese young adult women. Exp. Brain Res. 2018, 236, 2299–2308. [Google Scholar] [CrossRef]
- Green, M.W.; Elliman, N.A.; Rogers, P.J. The effects of food deprivation and incentive motivation on blood glucose levels and cognitive function. Psychopharmacology 1997, 134, 88–94. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Caruso, C.M.; Niro, P.J.; Adam, G.E.; Kellogg, M.D.; Nindl, B.C.; Kramer, F.M. A double-blind, placebo-controlled test of 2 d of calorie deprivation: Effects on cognition, activity, sleep, and interstitial glucose concentrations. Am. J. Clin. Nutr. 2008, 88, 667–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, G.E.; Mahoney, C.R.; Caruso, C.; Bukhari, A.S.; Smith, T.J.; Pasiakos, S.M.; McClung, J.P.; Lieberman, H.R. Two days of calorie deprivation impairs high level cognitive processes, mood, and self-reported exertion during aerobic exercise: A randomized double-blind, placebo-controlled study. Brain Cogn. 2019, 132, 33–40. [Google Scholar] [CrossRef]
- Witte, A.; Fobker, M.; Gellner, R.; Knecht, S.; Flöel, A. Caloric restriction improves memory in elderly humans. Proc. Natl. Acad. Sci. USA 2009, 106, 1255–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benau, E.M.; Orloff, N.C.; Janke, E.A.; Serpell, L.; Timko, C.A. A systematic review of the effects of experimental fasting on cognition. Appetite 2014, 77, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef]
- Subramanian, S.; Kawachi, I.; Smith, G.D. Income inequality and the double burden of under-and overnutrition in India. J. Epidemiol. Community Health 2007, 61, 802–809. [Google Scholar] [CrossRef] [Green Version]
- Dabelea, D.; Harrod, C.S. Role of developmental overnutrition in pediatric obesity and type 2 diabetes. Nutr. Rev. 2013, 71, S62–S67. [Google Scholar] [CrossRef]
- Samartı́n, S.; Chandra, R.K. Obesity, overnutrition and the immune system. Nutr. Res. 2001, 21, 243–262. [Google Scholar] [CrossRef]
- Gupta, D.; Krueger, C.B.; Lastra, G. Over-nutrition, obesity and insulin resistance in the development of β-cell dysfunction. Curr. Diabetes Rev. 2012, 8, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Fleischhacker, S.; Andrés, J.R. Prioritizing nutrition security in the US. JAMA 2021, 325, 1605–1606. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.T.; Shuval, K.; Bertmann, F.; Yaroch, A.L. The Supplemental Nutrition Assistance Program, food insecurity, dietary quality, and obesity among US adults. Am. J. Public Health 2015, 105, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in US adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Robaina, K.A.; Martin, K.S. Food insecurity, poor diet quality, and obesity among food pantry participants in Hartford, CT. J. Nutr. Educ. Behav. 2013, 45, 159–164. [Google Scholar] [CrossRef]
- Moradi, S.; Mirzababaei, A.; Dadfarma, A.; Rezaei, S.; Mohammadi, H.; Jannat, B.; Mirzaei, K. Food insecurity and adult weight abnormality risk: A systematic review and meta-analysis. Eur. J. Nutr. 2019, 58, 45–61. [Google Scholar] [CrossRef]
- Min, J.; Zhao, Y.; Slivka, L.; Wang, Y. Double burden of diseases worldwide: Coexistence of undernutrition and overnutrition-related non-communicable chronic diseases. Obes. Rev. 2018, 19, 49–61. [Google Scholar] [CrossRef]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 4, 479–489. [Google Scholar] [CrossRef]
- Hossain, S.; Beydoun, M.A.; Weiss, J.; Kuczmarski, M.F.; Evans, M.K.; Zonderman, A.B. Longitudinal associations between dietary quality and Alzheimer’s Disease genetic risk on cognitive performance among African American adults. Br. J. Nutr. 2020, 124, 1264–1276. [Google Scholar] [CrossRef] [Green Version]
- Sarker, G.; Peleg-Raibstein, D. Maternal overnutrition induces long-term cognitive deficits across several generations. Nutrients 2019, 11, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, R.A.; Gunstad, J.; Gustafson, D.R.; Heymsfield, S.B.; Launer, L.J.; Kral, J.G.; Penninger, J.; Phillips, D.I.; Scarmeas, N. The paradox of overnutrition in aging and cognition. Ann. N. Y. Acad. Sci. 2013, 1287, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinour, L.M.; Bergen, D.; Yeh, M.-C. The food insecurity–obesity paradox: A review of the literature and the role food stamps may play. J. Am. Diet. Assoc. 2007, 107, 1952–1961. [Google Scholar] [CrossRef]
- Hernandez, D.C.; Reesor, L.; Murillo, R. Gender disparities in the food insecurity–overweight and food insecurity–obesity paradox among low-income older adults. J. Acad. Nutr. Diet. 2017, 117, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Life Course Approach to Health. Available online: https://www.who.int/ageing/publications/lifecourse/alc_lifecourse_training_en.pdf (accessed on 1 September 2021).
- Na, M.; Dou, N.; Ji, N.; Xie, D.; Huang, J.; Tucker, K.L.; Gao, X. Food insecurity and cognitive function in middle to older adulthood: A systematic review. Adv. Nutr. 2020, 11, 667–676. [Google Scholar] [CrossRef]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk factors for malnutrition in older adults: A systematic review of the literature based on longitudinal data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef]
- Smith, K.E.; Mason, T.B.; Johnson, J.S.; Lavender, J.M.; Wonderlich, S.A. A systematic review of reviews of neurocognitive functioning in eating disorders: The state-of-the-literature and future directions. Int. J. Eat. Disord. 2018, 51, 798–821. [Google Scholar] [CrossRef]
- Siervo, M.; Arnold, R.; Wells, J.; Tagliabue, A.; Colantuoni, A.; Albanese, E.; Brayne, C.; Stephan, B. Intentional weight loss in overweight and obese individuals and cognitive function: A systematic review and meta-analysis. Obes. Rev. 2011, 12, 968–983. [Google Scholar] [CrossRef] [Green Version]
- Weerahandi, S. Generalized confidence intervals. In Exact Statistical Methods for Data Analysis; Springer: Berlin/Heidelberg, Germany, 1995; pp. 143–168. [Google Scholar]
- Viswanathan, M.; Patnode, C.D.; Berkman, N.D.; Bass, E.B.; Chang, S.; Hartling, L.; Murad, M.H.; Treadwell, J.R.; Kane, R.L. Assessing the Risk of Bias in Systematic Reviews of Health Care Interventions. Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet]. 2017. Available online: https://www.ncbi.nlm.nih.gov/sites/books/NBK519366/ (accessed on 13 August 2021).
- Jarde, A.; Losilla, J.-M.; Vives, J.; Rodrigo, M.F. Q-Coh: A tool to screen the methodological quality of cohort studies in systematic reviews and meta-analyses. Int. J. Clin. Health Psychol. 2013, 13, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Owens, D.K.; Lohr, K.N.; Atkins, D.; Treadwell, J.R.; Reston, J.T.; Bass, E.B.; Chang, S.; Helfand, M. Grading the strength of a body of evidence when comparing medical interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet]; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2009. [Google Scholar]
- Lohr, K.N.; Carey, T.S. Assessing “best evidence”: Issues in grading the quality of studies for systematic reviews. Jt. Comm. J. Qual. Improv. 1999, 25, 470–479. [Google Scholar] [CrossRef]
- Hernandez, D.C.; Jacknowitz, A. Transient, but not persistent, adult food insecurity influences toddler development. J. Nutr. 2009, 139, 1517–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frith, E.; Loprinzi, P.D. Food insecurity and cognitive function in older adults: Brief report. Clin. Nutr. 2018, 37, 1765–1768. [Google Scholar] [CrossRef]
- Hobkirk, A.L.; Towe, S.L.; Patel, P.; Meade, C.S. Food insecurity is associated with cognitive deficits among hiv-positive, but not hiv-negative, individuals in a united states sample. AIDS Behav. 2017, 21, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Grineski, S.E.; Morales, D.X.; Collins, T.W.; Rubio, R. Transitional dynamics of household food insecurity impact children’s developmental outcomes. J. Dev. Behav. Pediatr. JDBP 2018, 39, 715. [Google Scholar] [CrossRef]
- Alaimo, K.; Olson, C.M.; Frongillo, E.A. Food insufficiency and American school-aged children’s cognitive, academic, and psychosocial development. Pediatrics 2001, 108, 44–53. [Google Scholar] [PubMed]
- Gao, X.; Scott, T.; Falcon, L.M.; Wilde, P.E.; Tucker, K.L. Food insecurity and cognitive function in Puerto Rican adults. Am. J. Clin. Nutr. 2009, 89, 1197–1203. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, S.; King, C. The unequal impact of food insecurity on cognitive and behavioral outcomes among 5-year-old urban children. J. Nutr. Educ. Behav. 2018, 50, 687–694. [Google Scholar] [CrossRef]
- Koyanagi, A.; Veronese, N.; Stubbs, B.; Vancampfort, D.; Stickley, A.; Oh, H.; Shin, J.I.; Jackson, S.; Smith, L.; Lara, E. Food insecurity is associated with mild cognitive impairment among middle-aged and older adults in South Africa: Findings from a nationally representative survey. Nutrients 2019, 11, 749. [Google Scholar] [CrossRef] [Green Version]
- Mayston, R.; Patel, V.; Abas, M.; Korgaonkar, P.; Paranjape, R.; Rodrigues, S.; Prince, M. Determinants of common mental disorder, alcohol use disorder and cognitive morbidity among people coming for HIV testing in Goa, India. Trop. Med. Int. Health 2015, 20, 397–406. [Google Scholar] [CrossRef]
- Momtaz, Y.A.; Haron, S.A.; Hamid, T.A.; Ibrahim, R.; Masud, J. Does food insufficiency in childhood contribute to dementia in later life? Clin. Interv. Aging 2015, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Onadja, Y.; Atchessi, N.; Soura, B.A.; Rossier, C.; Zunzunegui, M.-V. Gender differences in cognitive impairment and mobility disability in old age: A cross-sectional study in Ouagadougou, Burkina Faso. Arch. Gerontol. Geriatr. 2013, 57, 311–318. [Google Scholar] [CrossRef]
- Portela-Parra, E.T.; Leung, C.W. Food Insecurity Is Associated with Lower Cognitive Functioning in a National Sample of Older Adults. J. Nutr. 2019, 149, 1812–1817. [Google Scholar] [CrossRef]
- Tong, M.; Tieu, L.; Lee, C.; Ponath, C.; Guzman, D.; Kushel, M. Factors associated with food insecurity among older homeless adults: Results from the HOPE HOME study. J. Public Health 2019, 41, 240–249. [Google Scholar] [CrossRef]
- Wong, J.C.; Scott, T.; Wilde, P.; Li, Y.-G.; Tucker, K.L.; Gao, X. Food insecurity is associated with subsequent cognitive decline in the Boston Puerto Rican Health Study. J. Nutr. 2016, 146, 1740–1745. [Google Scholar] [CrossRef] [Green Version]
- Barnes, L.L.; Wilson, R.S.; Everson-Rose, S.A.; Hayward, M.D.; Evans, D.A.; De Leon, C.F.M. Effects of early-life adversity on cognitive decline in older African Americans and whites. Neurology 2012, 79, 2321–2327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn-Schwartz, E.; Weinstein, G. Early-life food deprivation and cognitive performance among older Europeans. Maturitas 2020, 141, 26–32. [Google Scholar] [CrossRef]
- Tan, J.Y.; Sheira, L.A.; Frongillo, E.A.; Adimora, A.A.; Tien, P.C.; Konkle-Parker, D.; Golub, E.T.; Merenstein, D.; Levin, S.; Cohen, M. Food insecurity and neurocognitive function among women living with or at risk for HIV in the United States. Am. J. Clin. Nutr. 2020, 112, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture (USDA)—Economic Research Service. U.S. Household Food Security Survey Module: Three-Stage Design, with Screeners. Available online: https://www.ers.usda.gov/media/8271/hh2012.pdf (accessed on 1 September 2021).
- Wechsler, D. Wechsler Adult Intelligence Scale, 3rd ed.; Yonago Acta Medica: Yonago, Japan, 1997.
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Chichester, UK, 2016. [Google Scholar]
- Jaeger, J. Digit symbol substitution test: The case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharmacol. 2018, 38, 513. [Google Scholar] [CrossRef]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Kemp, S.; Benito-León, J.; Reuber, M. The influence of cognitive impairment on health-related quality of life in neurological disease. Acta Neuropsychiatr. 2010, 22, 2–13. [Google Scholar] [CrossRef]
- Bishop, N.A.; Lu, T.; Yankner, B.A. Neural mechanisms of ageing and cognitive decline. Nature 2010, 464, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Deary, I.J.; Corley, J.; Gow, A.J.; Harris, S.E.; Houlihan, L.M.; Marioni, R.E.; Penke, L.; Rafnsson, S.B.; Starr, J.M. Age-associated cognitive decline. Br. Med. Bull. 2009, 92, 135–152. [Google Scholar] [CrossRef]
- Cheng, E.R.; Palta, M.; Kotelchuck, M.; Poehlmann, J.; Witt, W.P. Cognitive delay and behavior problems prior to school age. Pediatrics 2014, 134, e749–e757. [Google Scholar] [CrossRef] [Green Version]
- Perez-Escamilla, F.; de Toledo Vianna, R.P. Food Insecurity and the Behavioral and Intellectual Development of Children: A Review of the Evidence. J. Appl. Res. Child. 2012, 3, 9. [Google Scholar]
- Shankar, P.; Chung, R.; Frank, D.A. Association of food insecurity with children’s behavioral, emotional, and academic outcomes: A systematic review. J. Dev. Behav. Pediatr. 2017, 38, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Slopen, N.; Fitzmaurice, G.; Williams, D.R.; Gilman, S.E. Poverty, food insecurity, and the behavior for childhood internalizing and externalizing disorders. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 444–452. [Google Scholar]
- Kleinman, R.E.; Murphy, J.M.; Little, M.; Pagano, M.; Wehler, C.A.; Regal, K.; Jellinek, M.S. Hunger in children in the United States: Potential behavioral and emotional correlates. Pediatrics 1998, 101, e3. [Google Scholar] [CrossRef] [Green Version]
- Banich, M.T.; Compton, R.J. Cognitive Neuroscience; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Alloway, T.P.; Alloway, R.G. Investigating the predictive roles of working memory and IQ in academic attainment. J. Exp. Child Psychol. 2010, 106, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnsten, A.F. Stress signalling pathways that impair prefrontal cortex structure and function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar] [CrossRef]
- Shansky, R.M.; Lipps, J. Stress-induced cognitive dysfunction: Hormone-neurotransmitter interactions in the prefrontal cortex. Front. Hum. Neurosci. 2013, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, E.K.; Cohen, J.D. An integrative theory of prefrontal cortex function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, B.B.; Schoen, L.S.; Badia, P. Predictable and unpredictable shock: Behavioral measures of aversion and physiological measures of stress. Psychol. Bull. 1984, 96, 45. [Google Scholar] [CrossRef]
- Jackson, D.B.; Chilton, M.; Johnson, K.R.; Vaughn, M.G. Adverse childhood experiences and household food insecurity: Findings from the 2016 National Survey of Children’s Health. Am. J. Prev. Med. 2019, 57, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Knowles, M.; Patel, F.; Frank, D.A.; Heeren, T.C.; Chilton, M. Childhood adversity and adult reports of food insecurity among households with children. Am. J. Prev. Med. 2016, 50, 561–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J. The Aerobic and Cognitive Exercise Study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef]
- Hawkins, M.A.; Layman, H.M.; Ganson, K.T.; Tabler, J.; Ciciolla, L.; Tsotsoros, C.E.; Nagata, J.M. Adverse childhood events and cognitive function among young adults: Prospective results from the national longitudinal study of adolescent to adult health. Child Abus. Negl. 2021, 115, 105008. [Google Scholar] [CrossRef]
- Bowen, S.; Elliott, S.; Hardison-Moody, A. The structural roots of food insecurity: How racism is a fundamental cause of food insecurity. Sociol. Compass 2021, 15, e12846. [Google Scholar] [CrossRef]
- Odoms-Young, A.M. Examining the impact of structural racism on food insecurity: Implications for addressing racial/ethnic disparities. Fam. Community Health 2018, 41, S3. [Google Scholar] [CrossRef]
- Coogan, P.; Schon, K.; Li, S.; Cozier, Y.; Bethea, T.; Rosenberg, L. Experiences of racism and subjective cognitive function in African American women. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12067. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | Study Design | Year of Data Collection | Country | Sample Size | Participant Demographics | Food Insecurity Measures | Cognitive Function Measures 1 | Food Insecurity and Cognitive Function Findings 2 |
|---|---|---|---|---|---|---|---|---|
| Alaimo et al. (2001) [73] | Observational, cross-sectional, secondary data | 1988–1994 | USA | 5349 | Children; aged 6–11 years old Adolescents; aged 12–16 years old | NHANES III: ‘Sometimes or often not enough food’ | WISC-R: Block design and digit span tasks | Food insecurity and executive function/visuospatial abilities: (null) |
| Barnes et al. (2012) [83] | Observational, longitudinal, primary data | 1993–2009 | USA | 6105 | Adults; mean 74.9 years old; 61.8% Black; 60.7% female | One item asking how often participants went without enough food to eat during childhood | MMSE | Food insecurity and general cognition: = −0.197 p < 0.001 |
| Cohn-Schwartz & Weinstein (2020) [84] | Observational, longitudinal, secondary Data | 2009–2013 | Europe (Multi-Country) | 2131 | Adults; mean 76.2 years old; 50% female | Two items: one asking whether the participant ever experienced hunger; one asking when the hunger period occurred | RAVLT; SHARE immediate and delayed word recall; animal naming task; serial sevens test | Food insecurity and impaired general cognition OR = 0.97 95% CI = 0.94–0.99 and verbal memory = −1.23 p = 0.04 |
| Frith and Loprinzi (2018) [70] | Observational, cross-sectional, secondary data | 1999–2002 | USA | 1851 | Adults; 60–85 years old | USDA 18-item Household Food Security Survey Module | DSST | Food insecurity and general cognition: = −14.4; 95% CI = −22.3, −0.3 |
| Gao et al. (2009) [74] | Observational, cross-sectional, primary data | 2004–2009 | USA | 1358 | Adults; 45–75 years old; 70% female | USDA 10-item Household Food Security Scale | MMSE; verbal memory test; digit span test | Food insecurity and executive function = −0.21 p = 0.003 and verbal memory = 22.7 p = 0.04 |
| Grineski et al. (2018) [72] | Observational, cross-sectional, secondary data | 2010–2012 | USA | 11958 | Children; 5–9 years old; 52% White, 13% Black, 25% Hispanic, 4% Asian, 6% other | USDA 18-item Household Food Security Survey Module | Numbers reversed test; 2-step dimensional change card sort test | Food insecurity and executive function: = −5.20 p ≤ 0.05 |
| Hernandez and Jacknowitz (2009) [69] | Observational, cross-sectional, secondary data | 2001–2006 | USA | 7900 | Children; 9–24 months old | USDA 18-item Household Food Security Survey Module | BSF-R mental scale | Food insecurity and general cognition: = −1.62 p < 0.05 |
| Hobbs and King (2018) [75] | Observational, cross-sectional, secondary data | 1998–2000 | USA | 2046 | Children; 5 years old; 22.5% White; 52.6% Black; 21.6% Hispanic; 3.3% other | USDA 18-item Household Food Security Survey Module | Peabody: PVT-R; W-J letter–word | Food insecurity and general cognition: = −0.19 95% CI = −0.33, −0.04 |
| Hobkirk et al. (2017) [71] | Observational, cross-sectional, primary data | 2010–2014 | USA | 97 | Adults; mean 45 years old; 85% Black; 35% female | HFIAS for Measurement of Food Access: Indicator Guide Version 3 | WAIS-III; HVLT; BVMT-R; Stroop test; trail-making test; PASAT-100; NAB digits test; FAS; grooved pegboard test | Food insecurity and general cognition/executive function: (null) |
| Koyanagi et al. (2019) [76] | Observational, cross-sectional, secondary data | 2007–2008 | South Africa | 3672 | Adults; mean 61.4 years old; 74.2% Black, 8.2% White, 16.5% other; 56% female | Two items adapted from NHANES | CERAD; WAIS-III; Animal Naming Task | Food insecurity and impaired general cognition: OR = 2.41 95% CI = 1.63, 3.87 |
| Mayston et al. (2015) [77] | Observational, cross-sectional, primary data | 2008–2010 | India | 1934 | Adults; mean 35 years old; 53% female | One item asking if participants had ‘ever experienced hunger due to a lack of money’ | Word-list learning memory task; animal naming verbal fluency task | Food insecurity and impaired verbal memory: OR = 1.41 95% CI = 1.05, 1.88 |
| Momtaz et al. (2015) [78] | Observational, cross-sectional, secondary data | 2003–2005 | Malaysia | 2745 | Adults; 60+ years old | One item asking if participants had ‘enough food to eat’ | GMS-AGECAT: Malaysian-adapted | Food insecurity & impaired general cognition: OR = 1.81 95% CI = 1.13, 2.92 |
| Onadja et al. (2013) [79] | Observational, cross-sectional, secondary data | 2010 | Burkina Faso | 981 | Adults; 50+ years old; 52.6% female | Measure examining ‘food availability uncertainty,’ ‘food intake reduction,’ and ‘totally lacking food’ | LCT | Food insecurity and impaired general cognition: OR = 1.80 95% CI = 1.06, 3.06 |
| Portela-Parra and Leung (2019) [80] | Observational, cross-sectional, secondary data | 2011–2014 | USA | 1823 | Adults; 60+ years old; 54% female; 42.7% Non-Hispanic White, 22.9% Non-Hispanic Black; 25.8% Hispanic, 8.6% Non-Hispanic other | USDA 10-item Adult Food Security Survey Module | CERAD: word learning subtest, delayed word cecall; AFT, DSST | Food insecurity and general cognition = −0.24 95% CI = −0.33, −0.15, executive function = −0.13 95% CI = −0.25, −0.002, and verbal memory: = −0.14 95% CI = −0.26, −0.01 |
| Tan et al. (2020) [85] | Observational, cross-sectional, secondary data | 2013–2015 | USA | 1346 | Adults; median 49.6 years old; 68.1% Black, 10.9% White, 16.4% Hispanic; 4.6% other | USDA 18-item Household Food Security Survey Module | Letter–number span task, Stroop test, symbol digit modalities test, trail-making test Part B, HVLT, COWAT | Food insecurity & executive bunction: = −1.45 p ≤ 0.01 |
| Tong et al. (2018) [81] | Observational, cross-sectional, secondary data | 2013–2014 | USA | 250 | Adults; mean 58 years old; 79.7% Black, 10.9% White, 4.6% Hispanic/Latino; 22.9% female | USDA Household Food Security Survey Module 6-item Short Form | MMSE | Food insecurity and impaired general cognition: OR = 2.21 95% CI = 1.12, 4.35 |
| Wong et al. (2016) [82] | Observational, longitudinal, primary data | 2004–2009 | USA | 597 | Adults; 45-75 years old; 68.3% female | USDA 10-item Household Food Security Survey Module | MMSE, 16-word learning list, digit span test (forward and backward), Stroop test, verbal fluency test, clock drawing test, figure copying | Food insecurity and general cognition = −1.20 95% CI = −2.19, −0.20, executive function = −4.67 95% CI = −8.52, −0.85, and visuospatial abilities: = −6.18 95% CI = −8.92, −3.43 |
| Citation. | General Cognition: | Executive Functioning: (Working Memory, Cognitive Flexibility, Inhibition, Planning, Reasoning) | Visuospatial Abilities: (Perception, Construction) | Verbal Memory: (Short-Term, Long-Term) |
|---|---|---|---|---|
| Alaimo et al. (2001) [73] | WISC-R: digit span | WISC-R: block design | ||
| Barnes et al. (2012) [83] | MMSE ** | |||
| Cohn-Schwartz & Weinstein (2020) [84] | Serial sevens test * | Animal naming task | RAVLT immediate recall RAVLT delayed recall ** | |
| Frith and Loprinzi (2018) [70] | DSST *CI | |||
| Gao et al. (2009) [74] | MMSE * | Digit span backward ** Stroop test Letter fluency * | Figure copying test Clock drawing test | Digit span forward Word list learning * Word recognition Word percentage retention * |
| Grineski et al. (2018) [72] | Numbers reversed test *** 2-step dimensional change card sort test *** | |||
| Hernandez and Jacknowitz (2009) [69] | BSF-R: cognitive scale | |||
| Hobbs and King (2018) [75] | Peabody: PVT-R ** W-J: letter–word * | |||
| Hobkirk et al. (2019) [71] | WAIS-III: digit symbol PASAT-100 NAB digits forward/digits backward test | Stroop test Trail-making test Part B FAS: letter fluency FAS: category fluency | BVMT-R | HVLT |
| Koyanagi et al. (2019) [76] | MCI *** | WAIS-III: digit span forward and backward a Animal naming task a | CERAD: word learning a CERAD: delayed recall a | |
| Mayston et al. (2015) [77] | Animal naming task: memory | Word list learning: delayed recall * | ||
| Momtaz et al. (2015) [78] | GMS-AGECAT: Malaysian-adapted ** | |||
| Onadja et al. (2013) [79] | LCT *CI | |||
| Portela-Parra and Leung (2019) [80] | DSST * | AFT * | CERAD: word learning * CERAD: delayed recall | |
| Tan et al. (2020) [85] | Letter–number span taska Stroop test a Symbol digit modalities test a Trail-mMaking test Part B a | HVLT a COWAT a | ||
| Tong et al. (2018) [81] | MMSE *CI | |||
| Wong et al. (2016) [82] | MMSE *CI | Digit span backward Stroop test Letter fluency * | Figure copying test *** Clock drawing test | Digit span forward Word list learning Word recognition |
| Citation | Study Design | Methods to Adjust for Selection Bias | Validity of Measures [+/−] | Recall Bias (Yes/No) | Confidence Intervals (NA/Precise/Imprecise) | Analytical Methods to Adjust for Confounding |
|---|---|---|---|---|---|---|
| Alaimo et al. (2001) [73] | Observational, cross-sectional, secondary data | Oversampling of subgroups Representative sample Sampling weights | +/− | Yes | NA | Main effect linear and logistic models, adjusted for sociodemographics and health outcomes: blood lead concentration, family size, mother’s age at birth, presence of birth complications, low birth weight, prenatal smoke exposure, parental perceptions of child’s health status |
| Barnes et al. (2012) [83] | Observational, longitudinal, primary data | None | +/− | Yes | NA | Mixed-effect models, adjusted for sociodemographics, medical conditions, geographic region, age, race, sex, years of educational attainment, self-reported myocardial infarction, hypertension, stroke, diabetes, southern vs. other states |
| Cohn-Schwartz & Weinstein (2020) [84] | Observational, longitudinal, secondary data | Exclusion of data from participants with a history of brain disease and/or injury | +/− | Yes | Precise 95% CI = 0.94, 0.99 | Multivariable linear regression, adjusted for age; sex; education; body mass index; chronic health conditions; physical activity; smoking cigarettes; depressive symptoms; income; weekly frequency of fruits and vegetables, dairy, fish/chicken/legumes/eggs; previous stress; poor health and financial hardship |
| Frith and Loprinzi (2018) [70] | Observational, cross-sectional, secondary data | Representative sample Multistage probability | + | Yes | Imprecise 95% CI = −22.3, −0.3 | Multivariable linear regression, adjusted for age, race/ethnicity, sex, measured body mass index, c-reactive protein, self-reported smoking status, diabetes status, measured arterial pressure, self-reported physical activity, social support |
| Gao et al. (2009) [74] | Observational, cross-sectional, primary data | Stratified random sampling | + | Yes | Precise 95% CI = −1.6, −0.19 | GLM, adjusted for measured body mass index, measured blood pressure, hypertension, Type 2 diabetes, total homocysteine, age, education, household income, smoking, alcohol intake, poverty status, acculturation, depression |
| Grineski et al. (2018) [72] | Observational, cross-sectional, sedondary Data | Representative sample Sampling weights | + | Yes | NA | Hierarchical linear modeling, adjusted for sociodemographic factors impacting cognitive function: number of parents in the household, US-born parents, household size, teen mother, parental depression, parental health status, and socio-economic status |
| Hernandez and Jacknowitz (2009) [69] | Observational; Cross-Sectional; Secondary Data | Over-sampling of subgroups Representative sample | + | Yes | NA | Ordinary least squares regression models, including 5 robustness checks; adjusted for child age, child sex, child race/ethnicity, number of times the family eats dinner together, previous food insecurity, birth order, maternal age at birth, maternal education, US-born status, employment status, marital status, income, geographic region, size of city, state-level poverty, percent of people within the sate with a bachelor’s degrees, state-level food stamp program participation, state-level WIC participation |
| Hobbs and King (2018) [75] | Observational, cross-sectional, sedondary Data | Over-sampling of subgroups with increased risk | + | Yes | Precise 95% CI = −0.33, −0.04 | Unconditional quantile regression; difference of means t-test, adjusted for mother’s race, low birthweight, maternal education, mother’s marital status, mother’s employment status, maternal smoking during pregnancy, parental history of substance abuse, US-born status, participation in the Supplemental Nutrition Assistance Program, maternal depression, social support, material hardship, parental stress |
| Hobkirk et al. (2017) [71] | Observational, cross-sectional, primary data | None | + | Yes | NA | ANCOVA, adjusted for premorbid verbal IQ, hepatitis C infection, income in the past 30 days, any history of homelessness, current health insurance, and HIV+ disease characteristics |
| Koyanagi et al. (2019) [76] | Observational, cross-sectional, sedondary Data | Representative sample Stratified multistage cluster sampling design | +/− | Yes | Precise 95% CI = 1.63, 3.87 | Multivariable logistic regression, adjusted for sex, age, education, income, race, physical activity, smoking use, alcohol use, depression in past 12 months, measured body mass index, stroke, diabetes, hypertension |
| Mayston et al. (2015) [77] | Observational, cross-sectional, primary data | None | +/− | Yes | Precise 95% CI = 1.05, 1.88 | Multivariate logistic regression, adjusted for sex, age, psychological comorbidity; hazardous drinking was adjusted for men only |
| Momtaz et al. (2015) [78] | Observational, cross-sectional, secondary data | Random sampling | +/− | Yes | Precise 95% CI = 1.13, 2.92 | Multiple logistic regression, adjusted for age, sex, marital status, educational attainment, ethnicity, and place of residence |
| Onadja et al. (2013) [79] | Observational, cross-sectional, secondary data | None | + | Yes | Precise 95% CI = 1.06, 3.06 | Linear regression, adjusted for age, sex, ethnicity, socioeconomic conditions in childhood, self-rated health during childhood, current socioeconomic status including marital status, body mass index, hypertension |
| Portela-Parra and Leung (2019) [80] | Observational, cross-sectional, secondary data | None | + | Yes | Precise 95% CI = −0.33, −0.15 95% CI = −0.25, −0.002 95% CI = −0.26, −0.01 | Multivariable linear regression, adjusted for age, sex, race/ethnicity, highest education level, marital status, income, smoking status |
| Tan et al. (2020) [85] | Observational, cross-sectional, secondary data | Recruitment of demographically similar control participants | + | Yes | NA | Multivariable linear regression, adjusted for income, employment status, illicit and non-illicit substance use, body mass index, depression, post-traumatic stress disorder |
| Tong et al. (2018) [81] | Observational, cross-sectional, secondary data | Random sampling | +/− | Yes | Precise 95% CI = 1.12, 4.35 | Logistic regression, adjusted for age, race/ethnicity, employment, residential history, health status, depressive symptoms, smoking status, alcohol use, illicit substance use, social support |
| Wong et al. (2016) [82] | Observational, longitudinal, primary data | Random sampling | + | Yes | Precise 95% CI = −2.19, −0.20 Imprecise 95% CI = −8.52, −0.85 95% CI = −8.92, −3.43 | Logistic regression, adjusted for age, sex, body mass index, education, physical activity score, poverty, acculturation score, smoking status, alcohol use, overall diet quality, presence of hypertension or diabetes, plasma homocysteine concentration, APOE status, depression, relevant baseline cognitive test score, time between assessments |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Royer, M.F.; Guerithault, N.; Braden, B.B.; Laska, M.N.; Bruening, M. Food Insecurity Is Associated with Cognitive Function: A Systematic Review of Findings across the Life Course. Int. J. Transl. Med. 2021, 1, 205-222. https://doi.org/10.3390/ijtm1030015
Royer MF, Guerithault N, Braden BB, Laska MN, Bruening M. Food Insecurity Is Associated with Cognitive Function: A Systematic Review of Findings across the Life Course. International Journal of Translational Medicine. 2021; 1(3):205-222. https://doi.org/10.3390/ijtm1030015
Chicago/Turabian StyleRoyer, Michael F., Nicolas Guerithault, B. Blair Braden, Melissa N. Laska, and Meg Bruening. 2021. "Food Insecurity Is Associated with Cognitive Function: A Systematic Review of Findings across the Life Course" International Journal of Translational Medicine 1, no. 3: 205-222. https://doi.org/10.3390/ijtm1030015
APA StyleRoyer, M. F., Guerithault, N., Braden, B. B., Laska, M. N., & Bruening, M. (2021). Food Insecurity Is Associated with Cognitive Function: A Systematic Review of Findings across the Life Course. International Journal of Translational Medicine, 1(3), 205-222. https://doi.org/10.3390/ijtm1030015