Abstract
Background: Given the aging of the overall U.S. population, the resulting changes in healthcare needs especially among veterans, and the high prevalence of traumatic brain injury (TBI) among older adults, additional research is needed on community participation after TBI in older veterans. The current study examined predictors of community participation trajectories over the 5 years after TBI in veterans who were 55 years of age or older upon injury. Method: This study included data from 185 participants in the U.S. Department of Veterans Affairs TBI Model System national study who had sustained a TBI at age 55 or older and had completed at least one of each Participation Assessment with Recombined Tools-Objective (PART-O) subscale scores at one or more follow-up time points (1, 2, and 5 years post-TBI). Results: PART-O Productivity, Social, and Out and About scores remained constant over time. Lower PART-O Productivity trajectories were seen among participants who were unemployed at the time of injury (p = 0.023). Lower PART-O Social trajectories were seen among participants who had a lower education level (p = 0.021), were unmarried at injury (p < 0.001), and had private insurance coverage (p < 0.033). Conclusion: These findings add to the growing body of literature on TBI and community participation by focusing on an older adult veteran population. There is an urgency to understand the needs of this group, many of whom are aging with service-connected disabilities including TBI. Veterans with characteristics identified herein as being associated with lower community participation trajectories would be prime candidates for interventions that aim to increase community and social engagement after later-life TBI.
1. Introduction
The older population in the United States (U.S.) is rapidly growing; the number of Americans aged 65 and over reached 55.8 million or 16.8% of the population in 2020 [1]. This group is projected to nearly double from 56 million in 2020 to 94.7 million by 2060, by which point they will comprise 23% of the U.S. population [2]. This increase is partially driven by the aging of the baby boomer generation, which has accelerated since 2011, when the first baby boomers turned 65 years old [1]. Rising life expectancy at older ages also contributes to the growth of the aging population. Average life expectancy at birth increased from 73.7 to 78.7 between 1980 and 2018 [3]. In 2021, there were approximately 9 million veterans enrolled in the Department of Veterans Affairs (VA) health system, with adults aged 65 years and older constituting almost half of the veteran enrollee population [4]. The VA is anticipating an increasing aging population with service-connected disabilities and long-term care needs [5]. Compared to the general population, the aging veteran population has a higher prevalence of multiple health conditions and disabilities, necessitating more complex care provided through the VA system [6,7,8]. From 2017 through 2037, spending for long-term care is projected to increase from 64% to 79%, and spending for care provision associated with service-connected disabilities is projected to increase 156% from USD 4.4 billion to USD 11.3 billion [5].
Traumatic brain injury (TBI) is common in older adults, who experience higher rates of mortality, morbidity, and hospitalizations from TBI [9,10,11]. Between 2002 and 2017, the rate of emergency department visits for TBI increased by 78% among adults aged 65 years and older [12]. The rate of TBI-related trauma admissions exceeded population growth among older adults aged 75 and over between 2007 and 2010 [13]. In 2019, more than 40% of TBI-related deaths occurred among adults aged 65 and older [14]. Older adults are more vulnerable to the effects of TBI and tend to have poorer post-TBI outcomes compared to younger adults [15,16,17,18,19]. TBI in older adults is associated with prolonged recovery [20,21] and significant functional impairment and disability [17,22,23,24]. Risk factors for TBI in older adults include reduced physiologic reserve related to aging [25], polypharmacy [26], and pre-existing conditions such as stroke, depression, and activity of daily living impairment [27]. Older adults with TBI tend to experience less favorable rehabilitation outcomes compared to younger adults with similar injury severity [28,29,30]. Neurobehavioral symptoms [31,32] and worsened cognitive functioning are prevalent among older adults after TBI [31,33,34,35,36,37,38,39]. Older adults are also at an increased risk for psychological disorders after TBI [39] such as depression [40,41,42,43] and anxiety [44,45,46]. Poor psychosocial functioning has been associated with poor recovery from TBI in older adults [47].
Multi-domain functional impairments commonly observed after TBI in older adults can individually and additively impact community participation, which is an outcome of central importance to people living with TBI and their families [48]. In the International Classification of Functioning and Disability (ICF) framework, participation is defined as “involvement in a life situation” [49] (p. 127), which takes place across the social domains of domestic life, interpersonal interactions and relationships, major life areas, and community, social, and civil life [49]. TBI not only adversely affects social relationships [50], but it also restricts participation in social activities, resulting in reduced quality of life [51,52,53]. Older age at the time of injury was a predictor of decreased levels of participation and progressively declining frequency of participation over the first 5 years following TBI [54]. In one study, adults aged 65 and over reported the lowest frequency of participation in the areas of productivity and social relations [55].
Given the aging of the overall U.S. population [1], the high prevalence of TBI among older adults [14], and older veterans’ more complex care needs [6], additional research is needed focusing on community participation after TBI in older veterans. As such, the objective of the current study was to examine the predictors of community participation trajectories over the 5 years after TBI in veterans who were 55 years of age or older upon injury. Because this was an exploratory study, there were no specific hypotheses about which predictors would emerge as most significant.
2. Method
2.1. Procedure and Participants
Secondary analyses were conducted with data from the VA TBI Model Systems (TBIMS) study [56], which collects longitudinal data about veterans admitted to one of the five VA polytrauma rehabilitation centers (PRCs) for inpatient rehabilitation post-TBI. This study is one of the largest longitudinal studies of veterans with TBI in the world and therefore is uniquely equipped to shed light on the possibly unique recovery trajectories of older veterans. The five PRCs are located in different regions of the U.S., resulting in a strong geographic representation of the sample. Data are collected over the span of many years with a standardized interview protocol, therefore increasing the generalizability of findings to veterans from different military service eras. Data were collected through a combination of in-person interviews, electronic and mailed interviews, and phone interviews. Institutional Review Board approval was obtained for study design and procedures from each of the PRCs.
Inclusion criteria for the VA TBIMS database are: (a) TBI diagnosis (i.e., mild, complicated mild, or moderate-to-severe) and associated admission to a PRC rehabilitation program, (b) 16 years of age or older at injury, and (c) informed consent by patient or a legally authorized representative. The present study had two specific exclusion criteria: (a) TBI sustained before age 55, and (b) not having at least one of each of the three Participation Assessment with Recombined Tools-Objective (PART-O) [57] subscales at one or more follow-up time points (data were collected at 1, 2, and 5 years post-TBI). In the current sample, 185 older veterans met these inclusion criteria. See Table 1 for participant demographic and injury-related data.

Table 1.
Sample characteristics.
2.2. Measures
2.2.1. Sociodemographic Characteristics
Age (in years) and sex (reported as male or female) were recorded at the time of injury. Race/ethnicity was dichotomized as White vs. Other due to the low representation of non-White participants in the dataset. Years of education was recorded as a continuous variable. Participants were considered married if they reported being married at the time of injury. Insurance was categorized as either private (including Tri-Care, worker’s compensation, and medical through auto insurance) or other (including Medicare, self or private pay, state or county, and VA, among others). Employment status was recorded for the month before injury, and participants were considered employed at injury if they were competitively employed; they were considered not competitively employed if they were a student, unemployed, caregiver, volunteer, or any other category. Pre-injury substance use history was dichotomized into categories including those who did and did not report a history of pre-injury substance use disorder. Potential pre-injury restrictions on activities were assessed by questions (yes/no) about the difficulties related to thinking skills, activities of daily living, independence outside the home, and working. Pre-injury participation in mental health services was also assessed (yes/no).
2.2.2. Injury Characteristics
Injury severity was characterized by duration (in days) of posttraumatic amnesia (PTA). Emergence from PTA was based on documented evidence provided in the acute care medical record or tracked prospectively through standardized measures upon admission to inpatient rehabilitation. PTA duration informed injury severity groupings defined as mild (0–1 days), moderate (2–7 days), and severe (8+ days). Participants with missing PTA were still included in the current study based on the approaches to handling missing data noted below. Combat status was dichotomized as yes/no regarding whether the participants had been deployed in combat zone at any point. Participants were categorized into those with a violent cause of injury and those without a violent cause of injury.
2.2.3. Participation Assessment with Recombined Tools-Objective (PART-O)
Community participation across the 5 years after TBI was measured using the PART-O [58,59], a 17-item self-report or proxy-report measure of post-TBI community engagement through three domains: (a) Productivity, which accounts for time spent working, attending school, or managing household tasks; (b) Social Relationships, reflecting time spent with family, friends, offering emotional support, and online interactions; and (c) Being Out and About in One’s Community, referred to as time spent outside the home engaging in leisure, shopping, or other activities. Domain scores range from 0 to 5, where higher scores indicate greater levels of community participation.
2.3. Data Analyses
All analyses were conducted using IBM SPSS Statistics version 27 (IBM, Armonk, NY, USA). Since many participants were missing data over the 5-year follow-up period, Little’s missing completely at random (MCAR) test was performed. Full information maximum likelihood (FIML) estimation was used to account for missing values, allowing retention of all participants meeting inclusion criteria. Dichotomous variables were given a reference point of 0, and continuous variables were centered around their means to reduce multicollinearity.
To examine trajectories of the PART-O subscales across the 5 years after TBI, several series of hierarchical linear models (HLMs) were run, one series for each of the three outcome variables. For each series, an unconditional growth model was run first with the successive addition of time2 to determine whether linear or quadratic models best depicted PART-O movement over time. Then -2 log-likelihoods (-2LLs) were calculated and compared for each model, with a drop of 3.84 chi-squared points reflecting a statistically significant improvement over the previous model.
HLM was then used to examine baseline predictors of PART-O subscale trajectories among older veterans across 1, 2, and 5 years after TBI. Predictors were entered simultaneously as fixed effects after being centered or given a reference point of 0, along with time (and with time2 as applicable). Each HLM determined whether linear outcome trajectories across years 1, 2, and 5 after TBI were predicted by baseline sociodemographic and injury severity characteristics of time; age; sex; race/ethnicity; education level; marital status; insurance type; employment status at time of injury; history of substance use disorder; pre-TBI functional limitations in cognitive abilities, activities of daily living, working, or independence outside of the home; history of mental health treatment; days in posttraumatic amnesia; deployment in a combat zone; and violent cause of injury. To test potential differential effects of the predictors over time (e.g., differences in slope as a function of the predictor), follow-up HLMs included each of the previously significant predictors from the first full model, time (and with time2 as applicable), and the interaction terms between time terms and the previously significant predictor. To avoid biasing figures by only graphing the outcome scores of participants with data present, the expectation-maximization algorithm was used to impute missing values that then were used to calculate overall means to be presented in the figures. For parsimony, only statistically significant main or interaction effects were graphed.
3. Results
3.1. Little’s MCAR Tests
Little’s MCAR test was statistically significant, χ2 (69) = 95.03, p = 0.021, suggesting that the three PART-O subscales were not MCAR. FIML was used to account for missing data in the trajectory analyses. For the degree of missingness of the three PART-O subscales at follow-up time points, see Table 2. Missingness at follow-ups occurred for a variety of reasons, including loss-to-follow-up, death, a participant not having yet entered a follow-up data collection window, and study withdrawal.
Table 2.
Percentage of data present at each follow-up time point.
3.2. PART-O Productivity
The -2LL of the initial model with linear time was 625.90, and the -2LL of the model with the addition of quadratic time was 625.15. The successive addition of a time product term did not result in a -2LL decrease of more than 3.84 chi-square points from the previous models, which suggested that linear (straight line) movement of PART-O Productivity trajectories was the best fit for the data.
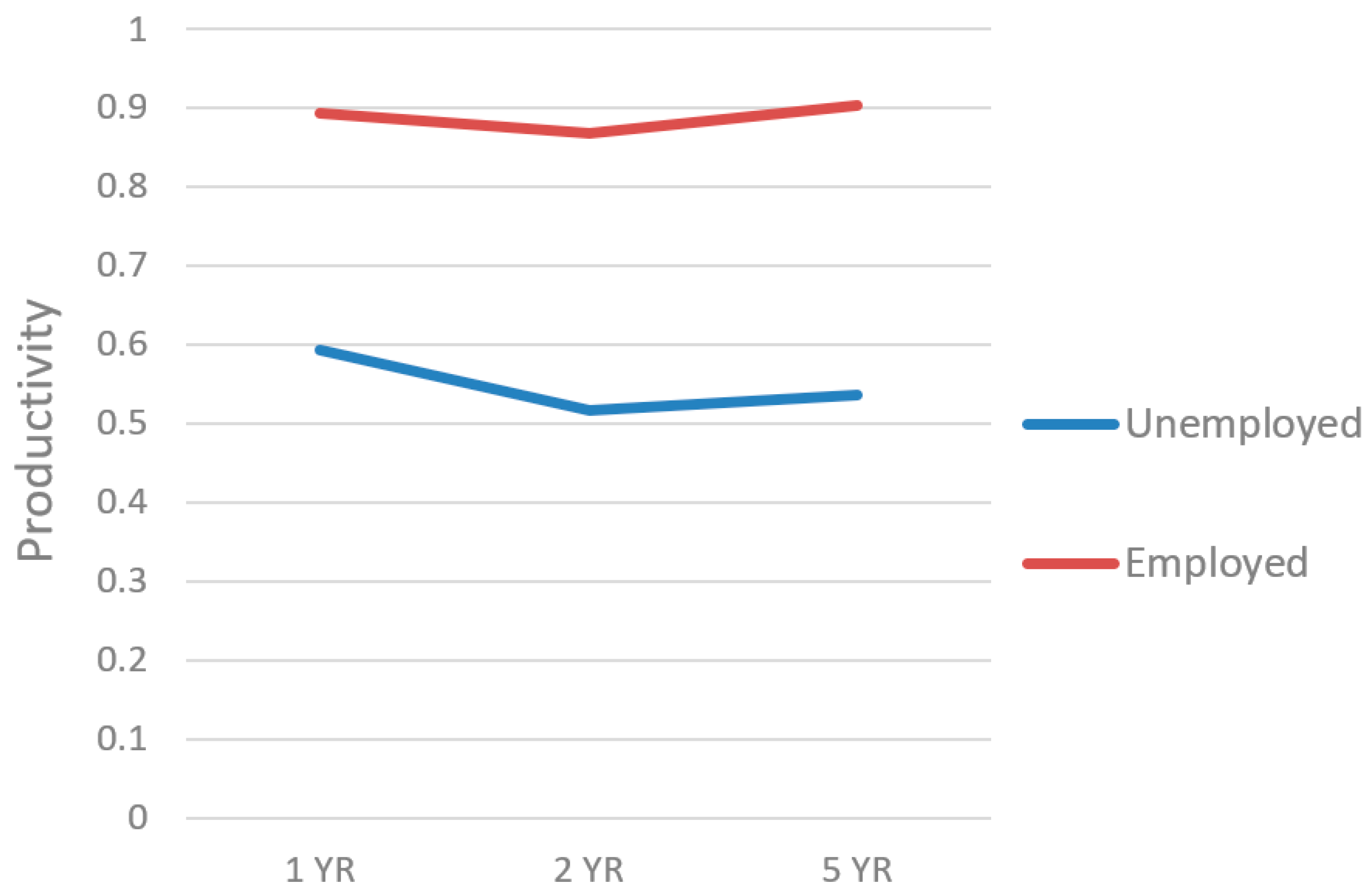
In the main HLM, PART-O Productivity scores remained constant over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. Lower PART-O Productivity trajectories (i.e., lower scores over time) were seen among participants who were unemployed at the time of injury (p = 0.023; Figure 1). No other predictors were statistically significant. A follow-up HLM examined whether linear trajectories of PART-O Productivity could be predicted by employment at injury and its interaction with time (Table 4). This time*employed at injury interaction was not statistically significant, suggesting that the slopes of the PART-O Productivity trajectory were similar for those who were both employed and unemployed at injury.
Table 3.
Fixed effects.
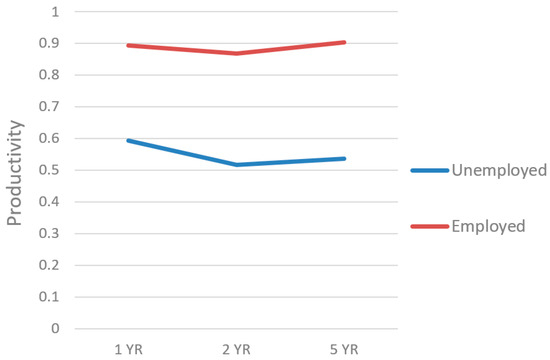
Figure 1.
Main effect of pre-injury employment on productivity trajectories.
Table 4.
Interactions in significant predictors over time.
3.3. PART-O Social
The -2LL of the initial model with linear time was 813.59, and the -2LL of the model with the addition of quadratic time was 812.94. The successive addition of a time product term did not result in a -2LL decrease of more than 3.84 chi-square points from the previous models, which suggested that linear (straight line) movement of PART-O Social trajectories was the best fit for the data.
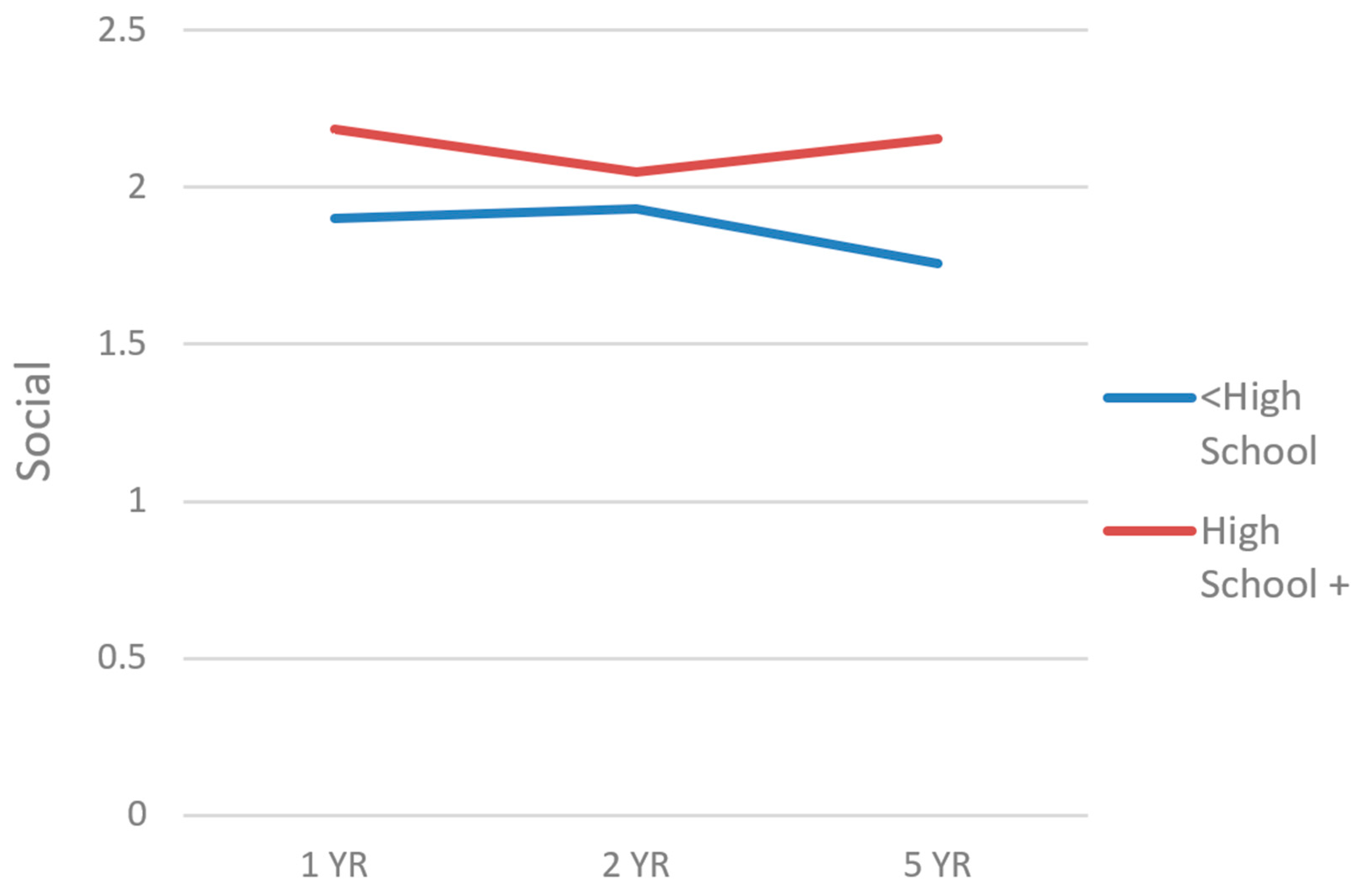
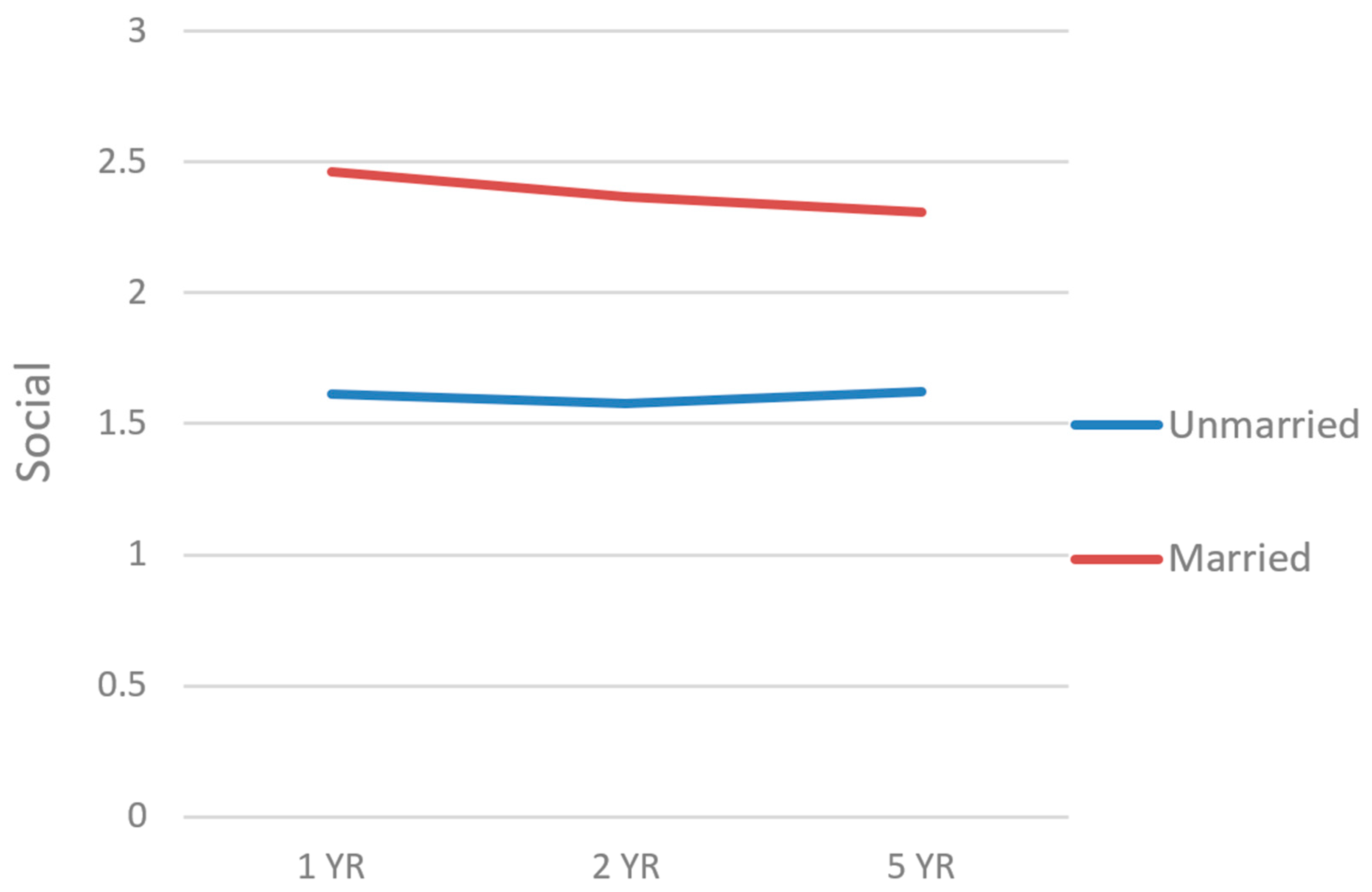
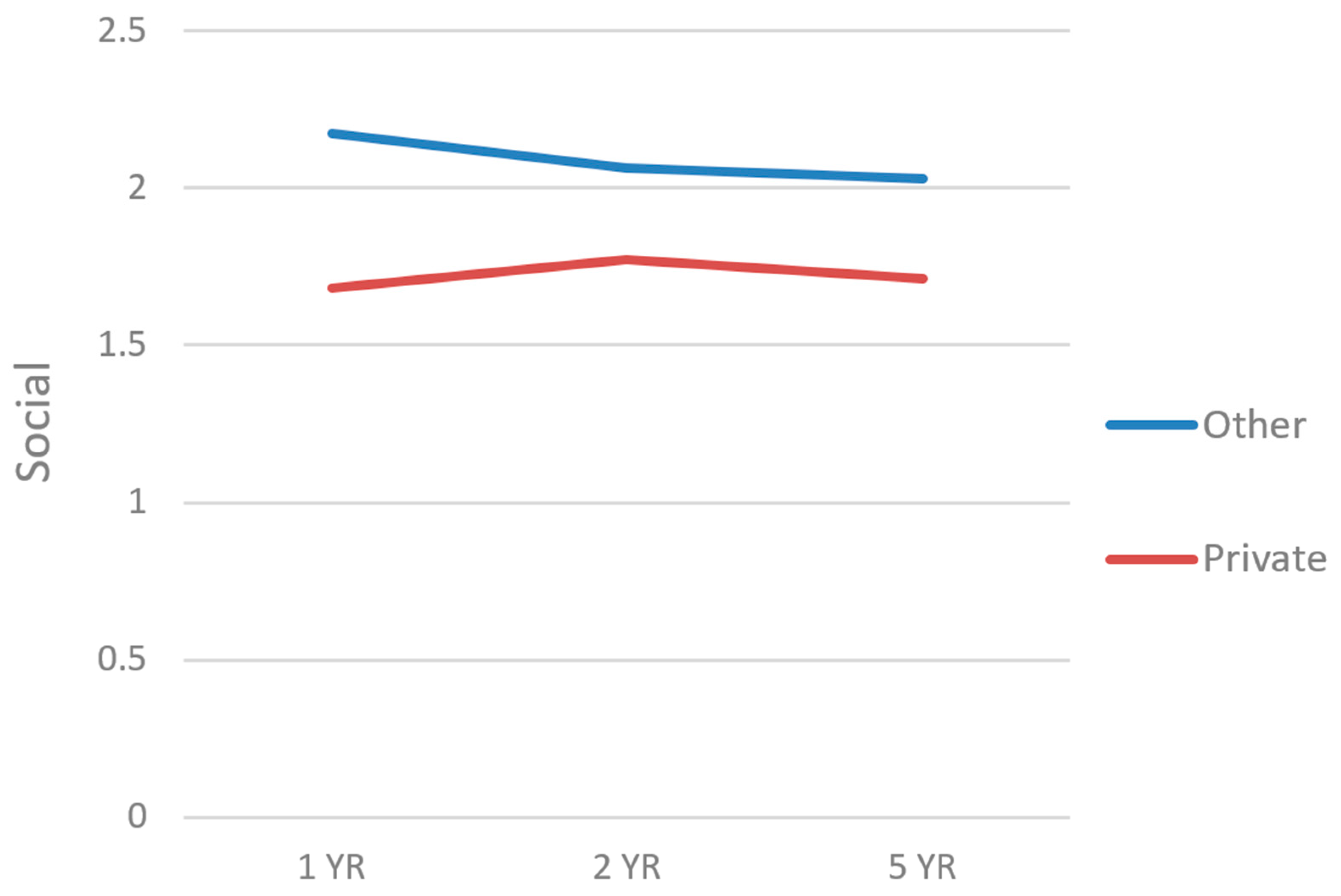
In the main HLM, PART-O Social scores remained constant over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. Lower PART-O Social trajectories were seen among participants who had a lower education level (p = 0.021; Figure 2), were unmarried at injury (p < 0.001; Figure 3), and among those who had private insurance coverage (p < 0.033; Figure 4). The b-weight for age was negative and its corresponding p-value barely achieved statistical significance, initially suggesting that individuals who were older at the time of injury had lower PART-O Social trajectories. When this effect was graphed, the opposite trend emerged such that younger individuals had slightly higher social trajectories, with the main difference only at 1 year. This reversal of findings suggests that this just-significant effect may have been due to low-to-moderate multicollinearity among the predictors and therefore was a statistical suppressor effect devoid of substantive interpretation [60], and/or a function of the necessary different methods for handling missing data in the analysis (FIML) vs. in graphing (expectation maximization); either way, this effect will not be interpreted further. Follow-up HLMs examined whether linear trajectories of PART-O Social could be predicted by the previously significant predictors and their interactions with time (Table 4). None of these interaction terms were statistically significant, suggesting that the slopes of PART-O Social trajectories were similar based on these demographic and injury characteristics.
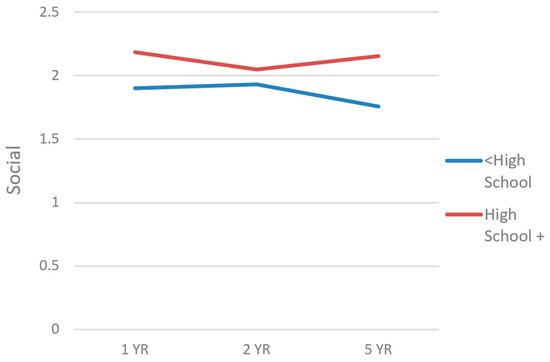
Figure 2.
Main effect of education on PART-O Social trajectories.
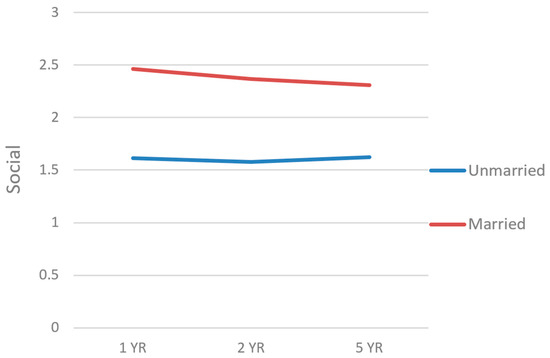
Figure 3.
Main effect of marital status on PART-O Social trajectories.
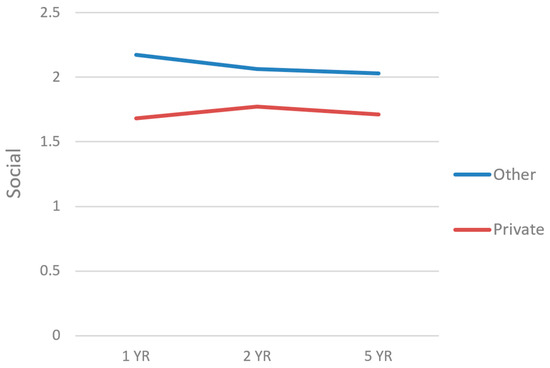
Figure 4.
Main effect of type of insurance on PART-O Social trajectories.
3.4. PART-O Out and About
The -2LL of the initial model with linear time was 700.49, and the -2LL of the model with the addition of quadratic time was 699.33. The successive addition of a time product term did not result in a -2LL decrease of more than 3.84 chi-square points from the previous models, which suggested that linear (straight line) movement of PART-O Out and About trajectories was the best fit for the data.
In the main HLM, PART-O Out and About scores remained constant over time. The unstandardized b-weights and p-values for this HLM appear in Table 3. There were no statistically significant fixed effects in the model.
4. Discussion
This study examined whether demographic, pre-injury, and injury characteristics among older (55+ years) veterans with TBI predicted community participation trajectories from 1 to 5 years after TBI in three community participation domains (productivity, social relationship, and being out and about in one’s community). PART-O Productivity, Social, and Out and About scores remained constant over time. Lower PART-O Productivity trajectories emerged among participants who had been unemployed at the time of injury. Lower PART-O Social trajectories emerged among participants who had a lower education level, had been unmarried at injury, and had private insurance coverage.
These findings are important in the context of the previous literature, which has shown that older age at the time of injury was a predictor of lower levels of participation and declining trajectories of participation after TBI [54]. However, in the current study of veterans who sustained a TBI over age 55, age at injury was not a significant predictor of community participation trajectories; this may suggest that previously documented age effects primarily emerge when comparing younger adults to older adults. Indeed, in studies examining participation across the lifespan, older adults have had the lowest participation frequency [55,61]. In the current study, the constant levels over time of community participation in all three domains contrasts somewhat with these previous studies but is likely due to the relatively younger classification of older adults in the current study (age 55+) as well as the shorter follow-up span of data collection across years 1–5.
When examining predictors, the finding that participation in the Productivity domain was lower for those who had been unemployed at the time of injury may be in part due to hours spent working being a component of the PART-O Productivity subscale. Older adults are more likely to experience changes in their employment after TBI [23], and the ability to return to work is an important factor in maintaining community participation, with employment pre-injury being a strong predictor of employment post-injury [62]. Previous studies have found a positive relationship between pre-injury employment and productivity but with older individuals having less productivity over time [63,64]. Individuals who are injured at an older age are more likely to retire than stay in the workforce [63]. Further, previous research has shown that individuals who are unemployed at the time of TBI are extremely unlikely to become employed at years 1, 2, or 5 after injury and only approximately 30% likely to be employed at 10 years after TBI [65]. This suggests that an underlying mechanism for this association in the current study is that unemployed older adults who sustain a TBI may have very little focus on rehabilitation of productive activity, favoring instead on maintenance approaches rather than rigorous vocational rehabilitation. Therefore, in addition to considering retirement options, rehabilitation providers should promote vocational opportunities that allow older veterans to return to work and increase community participation. Providers might also consider other factors that reduce motivation for older veterans to engage in productive community participation, such as the confluence of internalized ableism and internalized ageism. If older veterans with TBI are in fact unable to work, VA providers can help veterans explore whether they are eligible for disability benefits if they can prove their injury was service-connected, especially given the VA’s close attention paid to the residual effects of TBI [66].
The finding that higher trajectories were observed in the Social domain for those who had been married at injury may similarly be partially attributable to marital status factoring into the PART-O Social score, but it is also in line with the previous literature finding that living with others is linked to higher participation [54]. Older adults who are married at injury may have added social opportunities created by their spouse and their spouse’s social network vs. an older adult who sustains a TBI and is unmarried. Conversely, married people may socialize less outside the dyad than their unmarried counterparts, so it is unclear whether this finding is due to romantic partnership being a component of how social participation is conceptualized in the PART-O. Regardless of injury, older adults are more likely to have reduced social participation and spend more time at home than younger adults [67], and being married may provide older adults with more constant and increased social support and opportunities for social engagement than those who are unmarried, allowing them to maintain a higher level of social participation.
Lower levels of social participation were also observed for those with lower educational attainment. This may reflect broader patterns of inequality due to socioeconomic status that reduce the ability of older adults to participate in their community [68]. Lower educational attainment may lead to reduced income, thereby limiting social engagement in activities that cost money or that are dependent on reliable private transportation. Lower levels of participation in the Social domain were also observed for older adults with private insurance. This is an unexpected finding given that those with private insurance are more likely to be discharged to rehabilitation, and thus have access to more specialized rehabilitation opportunities aimed at increasing participation [69,70]. This finding is particularly important because older adults are less likely to be referred to neurorehabilitation, regardless of insurance status [71]. However, the finding may reflect the sense of camaraderie and identity that many veterans experience when receiving care in the VA Health Care System (coded as “other” and therefore not “private” insurance in the current study) and being able to interact with other veterans. Rehabilitation professions can focus on improving older veterans’ community participation via their social relationships and engagement outside the home. Many older veterans enjoy socialization with other veterans due to their unique culture and experiences. The emergence of veteran self-help communities has been shown to increase community engagement and promote overall well-being [72]. Similar approaches can be adapted for older veterans with TBI.
Limitations and Future Directions
The current study had several limitations that reflect opportunities for future research. Although the PART-O is a validated measure of participation after TBI, it may not comprehensively capture participatory life activities in older veterans with TBI. For example, the measure considers only participation level (i.e., frequency of an activity) and even if frequency is maintained consistently, there could have been important changes in the quality or personal meaningfulness of participation (i.e., satisfaction the person derives from participating) [73]. Some research suggests that for older adults in particular, satisfaction with participation may be a more useful indicator than frequency [55,74,75]. Thus, multidimensional approaches to characterizing older veterans’ participation after TBI may be important in future studies [74]. Some of the current study’s predictor variables were relatively coarse indicators of health-related factors (e.g., pre-injury mental health treatment as a reflection of mental health history) and may not have been sensitive enough to capture differences in community participation levels. And while we did find an effect of employment at injury on productivity, it is unknown whether certain types of competitive employment confer more advantages than others. Approximately three-quarters of the veterans in the current sample identified as White, with several other groups represented in the remainder, precluding an ability to examine nuanced racial/ethnic differences in participation. Because cultural and environmental factors can influence participation patterns, studies with more diverse older veteran samples are warranted [76]. Relatedly, the current sample was limited to older veterans receiving care at VA polytrauma rehabilitation centers. The sampling approach may impact variables such as type of insurance, cause of TBI, and employment at the time of injury. Future research may utilize purposive sampling to ensure equal distribution among the variables of interest. Finally, the study’s statistical methods for handling missing longitudinal data (FIML) are generally seen as the most state-of-the-art modern approach for minimizing bias in parameter estimates. Despite nearly three-quarters of participants having data at 1 or 2 years after injury, slightly less than half of participants had data at 5 years after injury. This could have been for a variety of reasons (e.g., death, loss to follow up, drop out, or a participant simply not coming up yet on their 5-year data collection window), so some small degree of bias could still have been introduced into the analyses due to differential attrition. Findings should therefore be interpreted with an appropriate degree of caution. Attrition is difficult to avoid in complex populations such as older adults with TBI, but larger sample sizes in future studies that continue to employ FIML for handling missing data may be able to help mitigate this problem.
5. Conclusions
The present study adds to the growing body of literature on TBI and community participation by focusing on an older adult veteran population. There is an urgency to understand the needs of this group, particularly as post-9/11 veterans, many of whom are living with service-connected disabilities including TBI, age into older adulthood. This study found that being currently unemployed, and other personal characteristics like lower education, being unmarried, and having private insurance are related to reduced participation among older veterans living with TBI. Veterans with these characteristics would be prime candidates for interventions that aim to increase community and social engagement after TBI. Interventions may include support groups for this specific population administered by VA PRCs, connecting with community stakeholders to increase outreach to older veterans not connected to the wider veteran community, and providing transportation for older veterans to participate in community events. Future research may examine what modes of community and social engagement are perceived as fulfilling by older veterans, barriers to community and social engagement for older veterans, and how community and social engagement impacts other health indicators in older veterans with TBI.
Author Contributions
Conceptualization, S.V. and P.B.P.; methodology, S.V. and P.B.P.; software, S.V. and P.B.P.; validation, S.V. and P.B.P.; formal analysis, S.V. and P.B.P.; investigation, S.V., D.W.K., M.E.D., B.X. and P.B.P.; resources, S.V. and P.B.P.; data curation, D.W.K., M.E.D., B.X. and P.B.P.; writing—original draft preparation, S.V., B.X., M.E.D., C.M.T., S.B.J., V.L.-J., K.G.T., R.G.K., U.M.V. and B.E.; writing—review and editing, P.B.P., S.V., D.W.K., K.D.-O. and R.G.K.; visualization S.V. and P.B.P.; supervision, P.B.P.; project administration, P.B.P. and D.W.K.; funding acquisition, P.B.P. and D.W.K. All authors have read and agreed to the published version of the manuscript.
Funding
This material is based upon work supported in part by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development. The contents of this publication were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) to TIRR Memorial Hermann (#90DPTB0025), Mount Sinai (#90DPTB0028), Virginia Commonwealth University (90DPTB0021), and Moss Rehabilitation Research Institute (#90DPTB0019).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Central Virginia Veterans Affairs Health Care System (W91YTZ13C0015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study or their legal proxy.
Data Availability Statement
The data presented in this article are not readily available because of patient confidentiality and data restrictions put in place by the U.S. Department of Veterans Affairs. Requests to access the datasets should be directed to perrin@virginia.edu.
Acknowledgments
NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this publication do not necessarily represent the policy of NIDILRR, ACL, or HHS, and are not necessarily endorsed by the Federal Government. The views expressed in this manuscript are those of the authors and do not necessarily represent the official policy or position of the Defense Health Agency, Department of Defense, or any other U.S. government agency. This work was prepared under Contract HT0014-22-C-0016 with DHA Contracting Office (CO-NCR) HT0014 and, therefore, is defined as U.S. Government work under Title 17 U.S.C.§101. Per Title 17 U.S.C.§105, copyright protection is not available for any work of the U.S. Government. For more information, please contact dha.TBICOEinfo@health.mil. UNCLASSIFIED.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- US Census Bureau. The Older Population: 2020; 2020 Census Brief C2020BR-07; US Census Bureau: Suitland, MD, USA, 2023. Available online: https://www.census.gov/library/publications/2023/decennial/c2020br-07.html (accessed on 28 March 2024).
- US Census Bureau. Table 2: Projected Age and Sex Composition of the Population: 2017–2060. Available online: https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.html (accessed on 28 March 2024).
- Arias, E.; Xu, J. United States Life Tables, 2018; National Vital Statistics Reports Vol 69, No 12; Centers for Disease Control and Prevention National Center for Health Statistics: Hyattsville, MD, USA, 2020. Available online: https://blogs.cdc.gov/nchs/2020/11/20/7035/ (accessed on 28 March 2024).
- Wang, J.; Cidade, M.; Larsen, M.; Pearman, G.; Schimpf, M.; Dhanireddy, P. Main Results Report, Prepared for S. A. S. (SAS) O. of S. P. and A. (OSPA) V. H. A. 2018 Survey of Veteran Enrollees’ Health and Use of Health Care; Department of Veterans Affairs: Rockville, MD, USA, 2019.
- US Government Accountability Office. VA Health Care: Veterans’ Use of Long-Term Care Is Increasing, and VA Faces Challenges in Meeting the Demand; GAO-20-284; US Government Accountability Office: Washington, DC, USA, 2020. Available online: https://www.gao.gov/assets/gao-20-284.pdf (accessed on 12 June 2023).
- Betancourt, J.A.; Granados, P.S.; Pacheco, G.J.; Reagan, J.; Shanmugam, R.; Topinka, J.B.; Beauvais, B.M.; Ramamonjiarivelo, Z.H.; Fulton, L.V. Exploring Health Outcomes for U.S. Veterans Compared to Non-Veterans from 2003 to 2019. Healthcare 2021, 9, 604. [Google Scholar] [CrossRef]
- Vinson, L.; Goodman, D.; Hutton, D.; Kuykendall, L. Report of the Caring for Behaviorally and Medically Complex Inpatients in VHA: Assessment of Program Needs and Models of Care. VHA Complex Patient Care Implementation Task Force; Department of Veterans Affairs: Washington, DC, USA, 2017.
- O’malley, K.A.; Vinson, L.; Pless Kaiser, A.; Sager, Z.; Hinrichs, K. Mental Health and Aging Veterans: How the Veterans Health Administration Meets the Needs of Aging Veterans. Public Policy Aging Rep. 2020, 30, 19–23. [Google Scholar] [CrossRef]
- Harvey, L.A.; Close, J.C.T. Traumatic Brain Injury in Older Adults: Characteristics, Causes and Consequences. Injury 2012, 43, 1821–1826. [Google Scholar] [CrossRef]
- Mosenthal, A.C.; Lavery, R.F.; Addis, M.; Kaul, S.; Ross, S.; Marburger, R.; Deitch, E.A.; Livingston, D.H. Isolated Traumatic Brain Injury: Age Is an Independent Predictor of Mortality and Early Outcome. J. Trauma Acute Care Surg. 2002, 52, 907. [Google Scholar] [CrossRef]
- Thompson, H.J.; McCormick, W.C.; Kagan, S.H. Traumatic Brain Injury in Older Adults: Epidemiology, Outcomes, and Future Implications. J. Am. Geriatr. Soc. 2006, 54, 1590–1595. [Google Scholar] [CrossRef]
- Cusimano, M.D.; Saarela, O.; Hart, K.; Zhang, S.; McFaull, S.R. A Population-Based Study of Fall-Related Traumatic Brain Injury Identified in Older Adults in Hospital Emergency Departments. Neurosurg. Focus 2020, 49, E20. [Google Scholar] [CrossRef]
- Dams-O’Connor, K.; Cuthbert, J.P.; Whyte, J.; Corrigan, J.D.; Faul, M.; Harrison-Felix, C. Traumatic Brain Injury among Older Adults at Level I and II Trauma Centers. J. Neurotrauma 2013, 30, 2001–2013. [Google Scholar] [CrossRef]
- Peterson, A.B.; Thomas, K.E.; Zhou, H. CDC Surveillance Report of Traumatic Brain Injury-Related Deaths by Age Group, Sex, and Mechanism of Injury—United States, 2018 and 2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. Available online: https://stacks.cdc.gov/view/cdc/122988 (accessed on 12 June 2023).
- Gould, K.R.; Ponsford, J.L.; Johnston, L.; Schönberger, M. Relationship Between Psychiatric Disorders and 1-Year Psychosocial Outcome Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2011, 26, 79. [Google Scholar] [CrossRef]
- Krishnamoorthy, V.; Distelhorst, J.T.; Vavilala, M.S.; Thompson, H. Traumatic Brain Injury in the Elderly: Burden, Risk Factors, and Prevention. J. Trauma Nurs.|JTN 2015, 22, 204. [Google Scholar] [CrossRef]
- Livingston, D.H.; Lavery, R.F.; Mosenthal, A.C.; Knudson, M.M.; Lee, S.; Morabito, D.; Manley, G.T.; Nathens, A.; Jurkovich, G.; Hoyt, D.B.; et al. Recovery at One Year Following Isolated Traumatic Brain Injury: A Western Trauma Association Prospective Multicenter Trial. J. Trauma Acute Care Surg. 2005, 59, 1298. [Google Scholar] [CrossRef]
- Mushkudiani, N.A.; Engel, D.C.; Steyerberg, E.W.; Butcher, I.; Lu, J.; Marmarou, A.; Slieker, F.; McHugh, G.S.; Murray, G.D.; Maas, A.I.R. Prognostic Value of Demographic Characteristics in Traumatic Brain Injury: Results from The IMPACT Study. J. Neurotrauma 2007, 24, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, M.J.; Feinstein, A. Outcome Following Traumatic Brain Injury in the Elderly: A Critical Review. Brain Inj. 2000, 14, 749–761. [Google Scholar] [CrossRef]
- Marquez de la Plata, C.D.; Hart, T.; Hammond, F.M.; Frol, A.B.; Hudak, A.; Harper, C.R.; O’Neil-Pirozzi, T.M.; Whyte, J.; Carlile, M.; Diaz-Arrastia, R. Impact of Age on Long-Term Recovery From Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Rothweiler, B.; Temkin, N.R.; Dikmen, S.S. Aging Effect on Psychosocial Outcome in Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 1998, 79, 881–887. [Google Scholar] [CrossRef]
- Maiden, M.J.; Cameron, P.A.; Rosenfeld, J.V.; Cooper, D.J.; McLellan, S.; Gabbe, B.J. Long-Term Outcomes after Severe Traumatic Brain Injury in Older Adults. A Registry-Based Cohort Study. Am. J. Respir. Crit. Care Med. 2020, 201, 167–177. [Google Scholar] [CrossRef]
- Testa, J.A.; Malec, J.F.; Moessner, A.M.; Brown, A.W. Outcome After Traumatic Brain Injury: Effects of Aging on Recovery. Arch. Phys. Med. Rehabil. 2005, 86, 1815–1823. [Google Scholar] [CrossRef]
- van der Vlegel, M.; Mikolić, A.; Hee, Q.L.; Kaplan, Z.R.; Helmrich, I.R.R.; van Veen, E.; Andelic, N.; Steinbuechel, N.v.; Plass, A.M.; Zeldovich, M. Health Care Utilization and Outcomes in Older Adults after Traumatic Brain Injury: A CENTER-TBI Study. Injury 2022, 53, 2774–2782. [Google Scholar] [CrossRef] [PubMed]
- Kuhne, C.A.; Ruchholtz, S.; Kaiser, G.M.; Nast-Kolb, D. Mortality in Severely Injured Elderly Trauma Patients—When Does Age Become a Risk Factor? World J. Surg. 2005, 29, 1476–1482. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Akishita, M.; Nakamura, T.; Nomura, K.; Ogawa, S.; Iijima, K.; Eto, M.; Ouchi, Y. Association of Polypharmacy with Fall Risk among Geriatric Outpatients. Geriatr. Gerontol. Int. 2011, 11, 438–444. [Google Scholar] [CrossRef]
- Dams-O’Connor, K.; Gibbons, L.E.; Landau, A.; Larson, E.B.; Crane, P.K. Health Problems Precede Traumatic Brain Injury in Older Adults. J. Am. Geriatr. Soc. 2016, 64, 844–848. [Google Scholar] [CrossRef]
- Cifu, D.X.; Kreutzer, J.S.; Marwitz, J.H.; Rosenthal, M.; Englander, J.; High, W. Functional Outcomes of Older Adults with Traumatic Brain Injury: A Prospective, Multicenter Analysis. Arch. Phys. Med. Rehabil. 1996, 77, 883–888. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.; de Guise, E.; Gosselin, N.; Feyz, M. Comparison of Functional Outcome Following Acute Care in Young, Middle-Aged and Elderly Patients with Traumatic Brain Injury. Brain Inj. 2006, 20, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Mosenthal, A.C.; Livingston, D.H.; Lavery, R.F.; Knudson, M.M.; Lee, S.; Morabito, D.; Manley, G.T.; Nathens, A.; Jurkovich, G.; Hoyt, D.B.; et al. The Effect of Age on Functional Outcome in Mild Traumatic Brain Injury: 6-Month Report of a Prospective Multicenter Trial. J. Trauma Acute Care Surg. 2004, 56, 1042. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, F.C.; Levin, H.S.; Presley, R.M.; Searcy, J.; Colohan, A.R.; Eisenberg, H.M.; Jann, B.; Bertolino-Kusnerik, L. Neurobehavioural Consequences of Closed Head Injury in Older Adults. J. Neurol. Neurosurg. Psychiatry 1994, 57, 961–966. [Google Scholar] [CrossRef]
- Goldstein, F.C.; Levin, H.S.; Goldman, W.P.; Kalechstein, A.D.; Clark, A.N.; Kenehan-Altonen, T. Cognitive and Behavioral Sequelae of Closed Head Injury in Older Adults According to Their Significant Others. J. Neuropsychiatry Clin. Neurosci. 1999, 11, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Caron, L.; Ouellet, M.-C.; Hudon, C.; Predovan, D.; Sirois, M.-J.; de Guise, É.; Lamontagne, M.-È.; Émond, M.; Le Sage, N.; Beaulieu-Bonneau, S. Cognitive Functioning Following Traumatic Brain Injury in Older Adults: Associations with Social Participation and Health-Related Quality of Life. Brain Inj. 2022, 36, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Deb, S.; Burns, J. Neuropsychiatric Consequences of Traumatic Brain Injury: A Comparison between Two Age Groups. Brain Inj. 2007, 21, 301–307. [Google Scholar] [CrossRef]
- Goldstein, F.C.; Levin, H.S.; Goldman, W.P.; Clark, A.N.; Altonen, T.K. Cognitive and Neurobehavioral Functioning after Mild versus Moderate Traumatic Brain Injury in Older Adults. J. Int. Neuropsychol. Soc. 2001, 7, 373–383. [Google Scholar] [CrossRef]
- Green, R.E.; Colella, B.; Christensen, B.; Johns, K.; Frasca, D.; Bayley, M.; Monette, G. Examining Moderators of Cognitive Recovery Trajectories After Moderate to Severe Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, S16–S24. [Google Scholar] [CrossRef]
- Hume, C.H.; Wright, B.J.; Kinsella, G.J. Systematic Review and Meta-Analysis of Outcome after Mild Traumatic Brain Injury in Older People. J. Int. Neuropsychol. Soc. 2022, 28, 736–755. [Google Scholar] [CrossRef]
- Moretti, L.; Cristofori, I.; Weaver, S.M.; Chau, A.; Portelli, J.N.; Grafman, J. Cognitive Decline in Older Adults with a History of Traumatic Brain Injury. Lancet Neurol. 2012, 11, 1103–1112. [Google Scholar] [CrossRef]
- Rapoport, M.J.; Herrmann, N.; Shammi, P.; Kiss, A.; Phillips, A.; Feinstein, A. Outcome After Traumatic Brain Injury Sustained in Older Adulthood: A One-Year Longitudinal Study. Am. J. Geriatr. Psychiatry 2006, 14, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, J.S.; Kiptanui, Z.; Tsang, Y.; Khokhar, B.; Liu, X.; Simoni-Wastila, L.; Zuckerman, I.H. Depression among Older Adults Following Traumatic Brain Injury: A National Analysis. Am. J. Geriatr. Psychiatry 2015, 23, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, J.S.; Barbour, L.; Abariga, S.A.; Rao, V.; Perfetto, E.M. Risk of Depression after Traumatic Brain Injury in a Large National Sample. J. Neurotrauma 2019, 36, 300–307. [Google Scholar] [CrossRef]
- Menzel, J.C. Depression in the Elderly after Traumatic Brain Injury: A Systematic Review. Brain Inj. 2008, 22, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Passler, J.S.; Sander, A.M.; Temkin, N.R.; Barber, J.; Gardner, R.C.; Manley, G.T. Depression in Older Adults 12 Months After Traumatic Brain Injury: A TRACK-TBI Study. Arch. Phys. Med. Rehabil. 2022, 103, 83–89. [Google Scholar] [CrossRef]
- Albrecht, J.S.; Peters, M.E.; Smith, G.S.; Rao, V. Anxiety and Post-Traumatic Stress Disorder among Medicare Beneficiaries Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2017, 32, 178–184. [Google Scholar] [CrossRef]
- Osborn, A.J.; Mathias, J.L.; Fairweather-Schmidt, A.K.; Anstey, K.J. Anxiety and Comorbid Depression Following Traumatic Brain Injury in a Community-Based Sample of Young, Middle-Aged and Older Adults. J. Affect. Disord. 2017, 213, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Whelan-Goodinson, R.; Ponsford, J.L.; Schönberger, M.; Johnston, L. Predictors of Psychiatric Disorders Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2010, 25, 320. [Google Scholar] [CrossRef]
- Kristman, V.L.; Brison, R.J.; Bédard, M.; Reguly, P.; Chisholm, S. Prognostic Markers for Poor Recovery After Mild Traumatic Brain Injury in Older Adults: A Pilot Cohort Study. J. Head Trauma Rehabil. 2016, 31, E33. [Google Scholar] [CrossRef]
- Pierce, C.A.; Hanks, R.A. Life Satisfaction After Traumatic Brain Injury and the World Health Organization Model of Disability. Am. J. Phys. Med. Rehabil. 2006, 85, 889. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Temkin, N.R.; Corrigan, J.D.; Dikmen, S.S.; Machamer, J. Social Functioning After Traumatic Brain Injury. J. Head Trauma Rehabil. 2009, 24, 460. [Google Scholar] [CrossRef] [PubMed]
- Huebner, R.A.; Johnson, K.; Bennett, C.M.; Schneck, C. Community Participation and Quality of Life Outcomes After Adult Traumatic Brain Injury. Am. J. Occup. Ther. 2003, 57, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Kalpinski, R.J.; Williamson, M.L.C.; Elliott, T.R.; Berry, J.W.; Underhill, A.T.; Fine, P.R. Modeling the Prospective Relationships of Impairment, Injury Severity, and Participation to Quality of Life Following Traumatic Brain Injury. BioMed Res. Int. 2013, 2013, e102570. [Google Scholar] [CrossRef] [PubMed]
- Sashika, H.; Takada, K.; Kikuchi, N. Rehabilitation Needs and Participation Restriction in Patients with Cognitive Disorder in the Chronic Phase of Traumatic Brain Injury. Medicine 2017, 96, e5968. [Google Scholar] [CrossRef] [PubMed]
- Erler, K.S.; Whiteneck, G.G.; Juengst, S.B.; Locascio, J.J.; Bogner, J.A.; Kaminski, J.; Giacino, J.T. Predicting the Trajectory of Participation After Traumatic Brain Injury: A Longitudinal Analysis. J. Head Trauma Rehabil. 2018, 33, 257. [Google Scholar] [CrossRef] [PubMed]
- Juengst, S.B.; Erler, K.S.; Neumann, D.; Kew, C.L.; Goldin, Y.; O’Neil-Pirozzi, T.M.; Rabinowitz, A.; Niemeier, J.; Bushnik, T.; Dijkers, M. Participation Importance and Satisfaction across the Lifespan: A Traumatic Brain Injury Model Systems Study. Rehabil. Psychol. 2022, 67, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Lamberty, G.J.; Nakase-Richardson, R.; Farrell-Carnahan, L.; McGarity, S.; Bidelspach, D.; Harrison-Felix, C.; Cifu, D.X. Development of a Traumatic Brain Injury Model System Within the Department of Veterans Affairs Polytrauma System of Care. J. Head Trauma Rehabil. 2014, 29, E1. [Google Scholar] [CrossRef]
- Bogner, J.; Bellon, K.; Kolakowsky-Hayner, S.A.; Whiteneck, G. Participation Assessment With Recombined Tools–Objective (PART-O). J. Head Trauma Rehabil. 2013, 28, 337. [Google Scholar] [CrossRef]
- Bogner, J.A.; Whiteneck, G.G.; Corrigan, J.D.; Lai, J.-S.; Dijkers, M.P.; Heinemann, A.W. Comparison of Scoring Methods for the Participation Assessment With Recombined Tools–Objective. Arch. Phys. Med. Rehabil. 2011, 92, 552–563. [Google Scholar] [CrossRef]
- Whiteneck, G.G.; Dijkers, M.P.; Heinemann, A.W.; Bogner, J.A.; Bushnik, T.; Cicerone, K.D.; Corrigan, J.D.; Hart, T.; Malec, J.F.; Millis, S.R. Development of the Participation Assessment With Recombined Tools–Objective for Use After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2011, 92, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, L.; Klein, K. Suppressor Variables: The Difference Between ‘Is’ Versus ‘Acting As’. J. Stat. Educ. 2014, 22, 2. [Google Scholar] [CrossRef]
- Niemeier, J.P.; Hammond, F.M.; O’Neil-Pirozzi, T.M.; Venkatesan, U.M.; Bushnik, T.; Zhang, Y.; Kennedy, R.E. Refining Understanding of Life Satisfaction in Elderly Persons with Traumatic Brain Injury Using Age-Defined Cohorts: A TBI Model Systems Study. Brain Inj. 2021, 35, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, J.P.; Harrison-Felix, C.; Corrigan, J.D.; Bell, J.M.; Haarbauer-Krupa, J.K.; Miller, A.C. Unemployment in the United States After Traumatic Brain Injury for Working-Age Individuals: Prevalence and Associated Factors 2 Years Postinjury. J. Head Trauma Rehabil. 2015, 30, 160. [Google Scholar] [CrossRef] [PubMed]
- Malone, C.; Erler, K.S.; Giacino, J.T.; Hammond, F.M.; Juengst, S.B.; Locascio, J.J.; Nakase-Richardson, R.; Verduzco-Gutierrez, M.; Whyte, J.; Zasler, N.; et al. Participation Following Inpatient Rehabilitation for Traumatic Disorders of Consciousness: A TBI Model Systems Study. Front. Neurol. 2019, 10, 1314. [Google Scholar] [CrossRef] [PubMed]
- Simpson, G.K.; McRae, P.; Hallab, L.; Daher, M.; Strettles, B. Participation in Competitive Employment after Severe Traumatic Brain Injury: New Employment versus Return to Previous (Pre-Injury) Employment. Neuropsychol. Rehabil. 2020, 30, 995–1012. [Google Scholar] [CrossRef] [PubMed]
- Howe, E.I.; Andelic, N.; Perrin, P.B.; Røe, C.; Sigurdardottir, S.; Arango-Lasprilla, J.C.; Lu, J.; Løvstad, M.; Forslund, M.V. Employment Probability Trajectories Up to 10 Years after Moderate-to-Severe Traumatic Brain Injury. Front. Neurol. 2018, 9, 1051. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on the Review of the Department of Veterans Affairs Examinations for Traumatic Brain Injury. Evaluation of the Disability Determination Process for Traumatic Brain Injury in Veterans; National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- Dahan-Oliel, N.; Gelinas, I.; Mazer, B. Social Participation in the Elderly: What Does the Literature Tell Us? Medicine 2008, 20, 2. [Google Scholar] [CrossRef]
- Kearney, P.; Plax, T.G.; Lentz, P.S. Participation in Community Organizations and Socioeconomic Status as Determinants of Seniors’ Life Satisfaction. Act. Adapt. Aging 1985, 6, 31–37. [Google Scholar] [CrossRef]
- McQuistion, K.; Zens, T.; Jung, H.S.; Beems, M.; Leverson, G.; Liepert, A.; Scarborough, J.; Agarwal, S. Insurance Status and Race Affect Treatment and Outcome of Traumatic Brain Injury. J. Surg. Res. 2016, 205, 261–271. [Google Scholar] [CrossRef]
- Asemota, A.O.; George, B.P.; Cumpsty-Fowler, C.J.; Haider, A.H.; Schneider, E.B. Race and Insurance Disparities in Discharge to Rehabilitation for Patients with Traumatic Brain Injury. J. Neurotrauma 2013, 30, 2057–2065. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Kumar, R.G.; Wisniewski, S.R.; Fabio, A. Disparities in Health Care Utilization of Adults with Traumatic Brain Injuries Are Related to Insurance, Race, and Ethnicity: A Systematic Review. J. Head Trauma Rehabil. 2018, 33, E40. [Google Scholar] [CrossRef] [PubMed]
- Gorman, J.A.; Chamberlin, E.S.; Stevenson, B.J.; Calixte, R.; Crossman, D.M.; Ahern, M.E.; Mack, J.; Russo, A.; Federman, E.J. Using Veterans Socials to Build a Community: Feasibility of the VOICES Intervention. Community Ment. Health J. 2022, 58, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- McLean, A.M.; Jarus, T.; Hubley, A.M.; Jongbloed, L. Associations between Social Participation and Subjective Quality of Life for Adults with Moderate to Severe Traumatic Brain Injury. Disabil. Rehabil. 2014, 36, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Dizon, L.; Wiles, J.; Peiris-John, R. What Is Meaningful Participation for Older People? An Analysis of Aging Policies. Gerontologist 2020, 60, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Aroogh, M.D.; Shahboulaghi, F.M. Social Participation of Older Adults: A Concept Analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55. [Google Scholar]
- Sander, A.M.; Clark, A.; Pappadis, M.R. What Is Community Integration Anyway?: Defining Meaning following Traumatic Brain Injury. J. Head Trauma Rehabil. 2010, 25, 121. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).