1. Introduction
The loss of resources after traumatic experiences has not been studied in the U.S. Veteran population, nor has the relationship between the gain of resources after traumatic experiences and clinical outcomes. This report seeks to begin to address these gaps by introducing the conservation of resources (COR) theory—a theory that conceptualizes stress in terms of what resources a Veteran has lost and/or gained.
1.1. Review of Relevant Scholarship
Hobfoll’s conservation of resources (COR) theory states that one accumulates resources for later use to accommodate, withstand, or overcome threats [
1]. Resources are separated into four categories: personal characteristics, objects, conditions, and energy resources. Personal characteristic resources are the self and worldviews. These include a sense of optimism, a sense of purpose, and feeling independent. Object resources are possessions with functional or status value such as a car, home, or household items. Condition resources include social roles such as employment, marriage, and membership in an organization. Energy resources are valued as tools used to acquire other resources, including time, money, and information [
1]. The COR theory assumes the motivational idea that individuals strive to obtain, keep, and protect resources they value. Therefore, stress can occur in three conditions: (a) when resources are threatened, (b) when resources are lost, or (c) when there are not adequate resources following the investment of resources [
2].
Traumatic stress in terms of the COR theory entails a rapid loss of resources [
1]. Traumatic stress is more evident when the resources lost are of high value. The development of PTSD and PTSD symptomology with resource loss has been strongly supported in the literature [
3]. The more resource loss experienced, the greater PTSD symptomology—as evidenced in natural disasters, sexual assaults, terrorist attacks, foreign war-related stressors, torture survivors, political violence, medical trauma, disease epidemic, and shootings [
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14].
1.2. Hypothesis, Aims, and Objectives
This study’s hypotheses were that: (H1) greater resource loss will be associated with more PTSD symptoms, (H2) greater resource gain will be associated with less PTSD symptoms, and (H3) additional resources will be identified by Veterans.
2. Method
2.1. Inclusion/Exclusion Criteria
Inclusion criteria were (a) Veterans eligible to receive healthcare from the Tibor Rubin VA Medical Center, (b) deployment to areas associated with Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and/or Operation New Dawn (OND) wars, (c) no current diagnosis of schizophrenia or bipolar disorder, (d) received a minimum score of 21 or higher as measured using the Montreal Cognitive Assessment (MoCA) (version 7 November 2004), and (e) the ability to comprehend and satisfactorily comply with protocol requirements and sign the written informed consent prior to entering this study. Exclusion criteria included (a) a current diagnosis of schizophrenia or bipolar disorder, (b) decisional incapacity, (c) memory impairment, and (d) cognitive impairment as measured using the MoCA, with a score of 20 or lower.
2.2. Participants’ Characteristics
Participants included 19 Veterans (18 men and 1 woman) at the Tibor Rubin VA Medical Center. The mean age of participants was M = 41.42 years (SD = 9.38), and their mean years of education was M = 14.74 (SD = 2.33). Participants described themselves as Hispanic or Latino (42.1%), White or Caucasian (21.1%), Multiracial (15.8%), Asian (10.5%), African American (5.3%), and American Indian/Alaskan Native (5.3%). Four participants were foreign born, having immigrated from Colombia, Vietnam, Guatemala, and South Korea. The M number of deployments of participants was 2.84 (SD = 3.79), and the average length of military service was 156.53 months (SD = 126.67). The M time since return from participants’ deployment was 115.16 months (SD = 46.90), and the M time since the identified trauma index of participants was 148.95 months (SD = 84.18). Participants were married (57.9%), single (26.3%), divorced (10.5%), and other (5.3%). Ten participants served in the Army (n = 10), four in the Marines (n = 4), four in the Air Force (n = 4), and two in the Navy (n = 2). One Veteran served in both the Army and the Air Force. Fourteen participants served in the OIF war (n = 14), thirteen served in the OEF war (n = 13), and two served in the OND war (n = 2). Six participants served in both the OEF and OIF wars, and two participants served in the OEF, OIF, and OND wars.
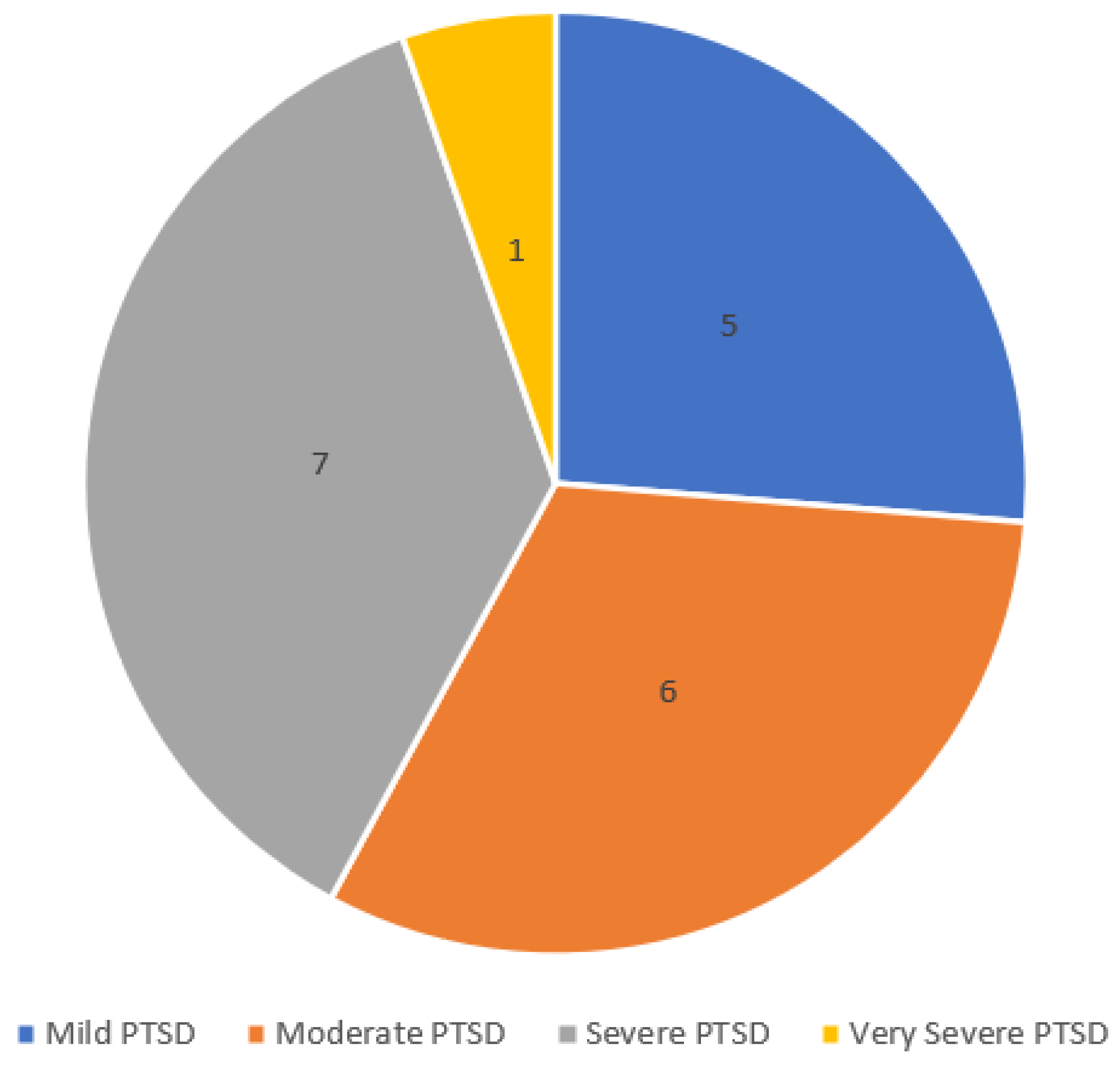
Eleven participants met DSM-5 (APA, 2013) diagnostic criteria for PTSD, and eight did not. Participants were ordinally categorized into four PTSD severity levels.
Figure 1 shows participants’ categories: severe (
n = 7), moderate (
n = 6), mild (
n = 5), and very severe (
n = 1). For the purpose of this data analysis, very severe and severe categories were combined. Participants were also dichotomously divided as non-PTSD and PTSD, as defined by the PSS-I (see data diagnostics).
2.3. Sampling Procedures
This research study received Institutional Review Board (IRB) approval at Azusa Pacific University (#18-010-OTH) and at the Tibor Rubin VA Medical Center (#1678). The initial goal of this study was to recruit 50 Veterans from the Tibor Rubin VA Medical Center, 25 of whom met criteria for PTSD diagnosis from the
Diagnostic and Statistical Manual of Mental Disorders and 25 of whom did not meet
DSM-5 criteria for PTSD [
15]. As this was a pilot study, a sample size of 50 was determined to be sufficient [
16]. Due to the epidemic of the novel coronavirus disease of 2019 (COVID-19), recruitment of research participants was terminated earlier than anticipated, as mandated by governing IRB bodies.
A total of 46 Veterans were approached to participate in this study, and 41.3%, or 19, consented. Of the 19 who consented, 100% completed this study. Veterans were contacted via telephone to confirm interest in this study and scheduled for a single appointment to complete the study. Veterans were recruited through flyers posted throughout the Tibor Rubin VA Medical Center in Long Beach, California. Residual funding was identified from the fourth authors’ research funds, and participants received USD 20 as compensation for completing this study. Recruitment emails were regularly sent to clinicians explaining this study and asking for referrals.
2.4. Measures and Covariates
Screening measures included a demographic questionnaire and the MoCA (version 7 November 2004) to screen for cognitive impairments [
17]. Combat exposure severity was measured using the Combat Exposure Scale (CES) [
18]. PTSD symptoms were measured using the PTSD Symptom Scale–Interview (PSS-I) [
19,
20]. Resource loss and resource gain were measured using the Conservation of Resources–Evaluation (COR-E). Two open-ended questions were added within the COR-E asking Veterans to identify additional resources that they had lost and/or gained since their traumatic experience.
2.5. Data Collection and Statistical Analyses
The data collection period was February 2018 to January 2020. This study was prematurely closed due to the outbreak of COVID-19. The first author was the only interviewer for this study. During interview appointments, the Health Insurance Portability and Accountability Act (HIPAA) and the informed consent form were explained and completed. The duration of the interview varied from 1.5 to 3 h, depending on participant factors and needs. All interviews were completed in one sitting. No adverse events were reported.
Figure 2 depicts the flow of participants. Reasons for exclude: other warzone (
n = 3), mental health condition exclusion (
n = 3), no show appointment (
n = 7), not interested (
n = 9), and lack of contact (
n = 5).
Data were entered by the first author into Microsoft Excel and migrated to SPSS Statistics (Version 26, IBM, New York, NY, USA) for analyses. Quantitative data analyses were completed using SPSS V.26 and the MOTE effect size calculator from the Missouri State DOOM lab [
21].
3. Instruments
Montreal Cognitive Assessment. The MoCA is a brief screening tool for mild cognitive impairment [
17]. Version 4 November 2004 was utilized. The MoCA has satisfactory internal consistency (
α = 0.89) and adequate general factor saturation (ω
h/ω
t = 0.74 and β = 0.78) [
22]. A cut-off score of 21 was selected for the Veteran population [
23]. The
M for the total sample was 26.21,
SD = 2.18, range = 8.
Combat Exposure Scale. The CES is a self-reporting, seven-item measure that assesses wartime stressors experienced by Veterans [
18]. Items are measured using a five-point frequency, five-point duration, and forty-five-point degree of loss scale [
18]. The CES has satisfactory internal consistency (
α = 0.85) and high test–retest reliability [
18].
PTSD Symptom Scale–Interview. The PSS-I is a seventeen-item semi-structured interview that diagnoses and assesses the severity of PTSD symptoms [
19,
20]. This tool was selected with permission for use from Dr. Edna Foa. It yields a total PTSD severity score and sub-scores for re-experiencing, avoidance, and arousal symptoms [
19]. The PSS-I has satisfactory internal consistency (
α = 0.65–0.85), high test–retest reliability, good concurrent validity, and high interrater reliability (ρ = 0.93) [
20].
Conservation of Resources–Evaluation. The COR-E is a companion measure to the conservation of resources (COR) model and was created by Dr. Stevan Hobfoll in collaboration with Roy Lilly. This tool was selected with permission for use from Dr. Hobfoll. The COR-E is composed of two lists of 74 resources; respondents separately report their degree of resource loss or gain. The scale utilized is as follows: 0 = zero/not applicable, 1 = small degree to 4 = great degree. Example resource items include a sense of pride in myself, hope, role as leader, adequate food, extras for children, companionship, people I can learn from, affection from others, and financial stability.
Open-Ended Questions. One open-ended question was placed at the end of the loss section of the COR-E. Participants were asked to write down any additional resources they have lost since the beginning of their deployment. After writing in any such resources, they were also asked to rate the degree of “actual loss” and “threat of loss” of these resources. A second question was placed at the end of the gain section, asking participants to write down any additional resources they have gained since the beginning of their deployment and the degree of gain. Participants were not restricted by the type and quantity of resources they could list in the open-ended sections. Scales to measure the degree of resource loss and gain were alike to the scale of the original COR-E.
4. Results
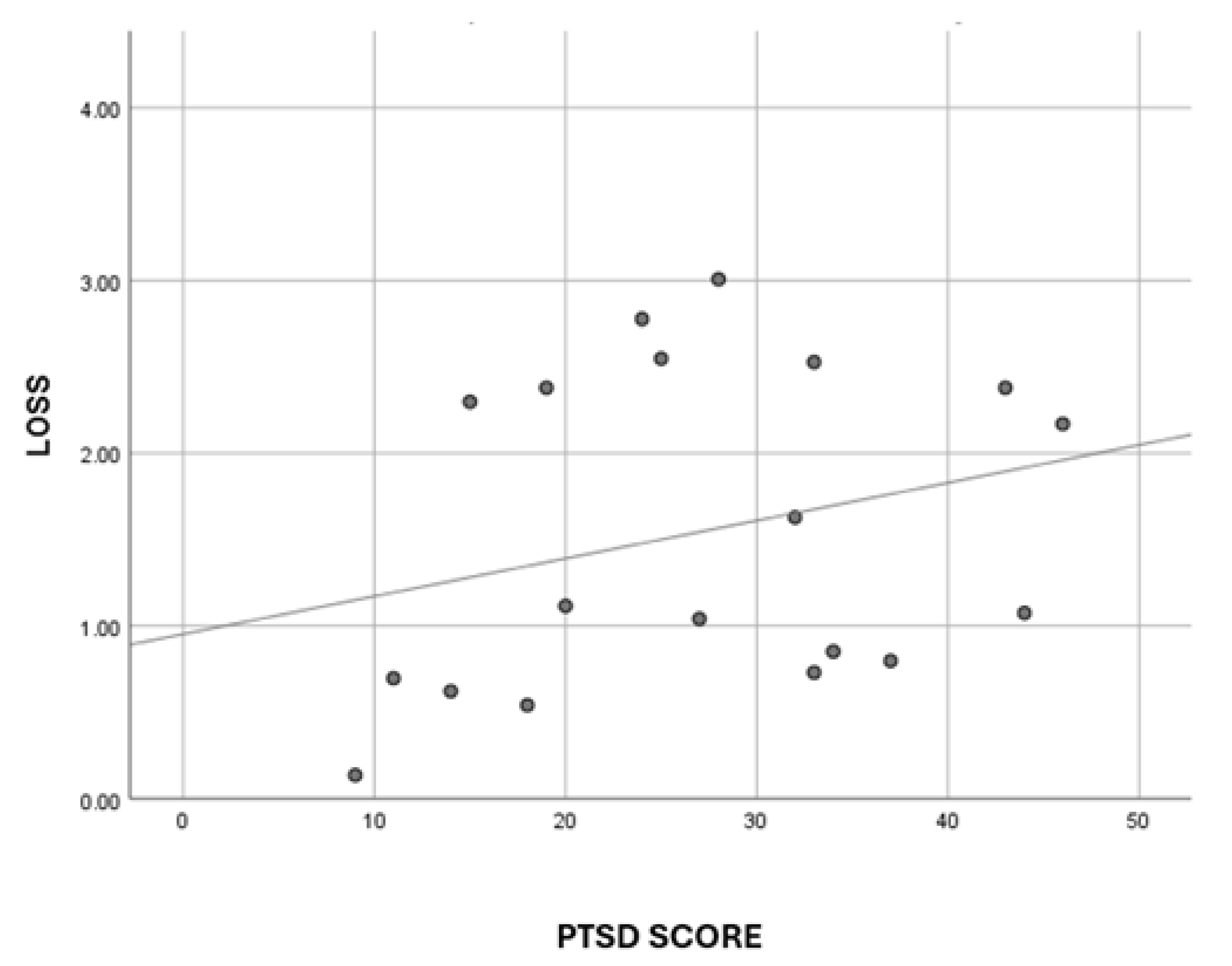
Hypothesis 1 (H1). Result: Greater resource loss will be associated with higher levels of PTSD symptoms was not fully supported. A medium effect size was found, but not at a statistically significant level.
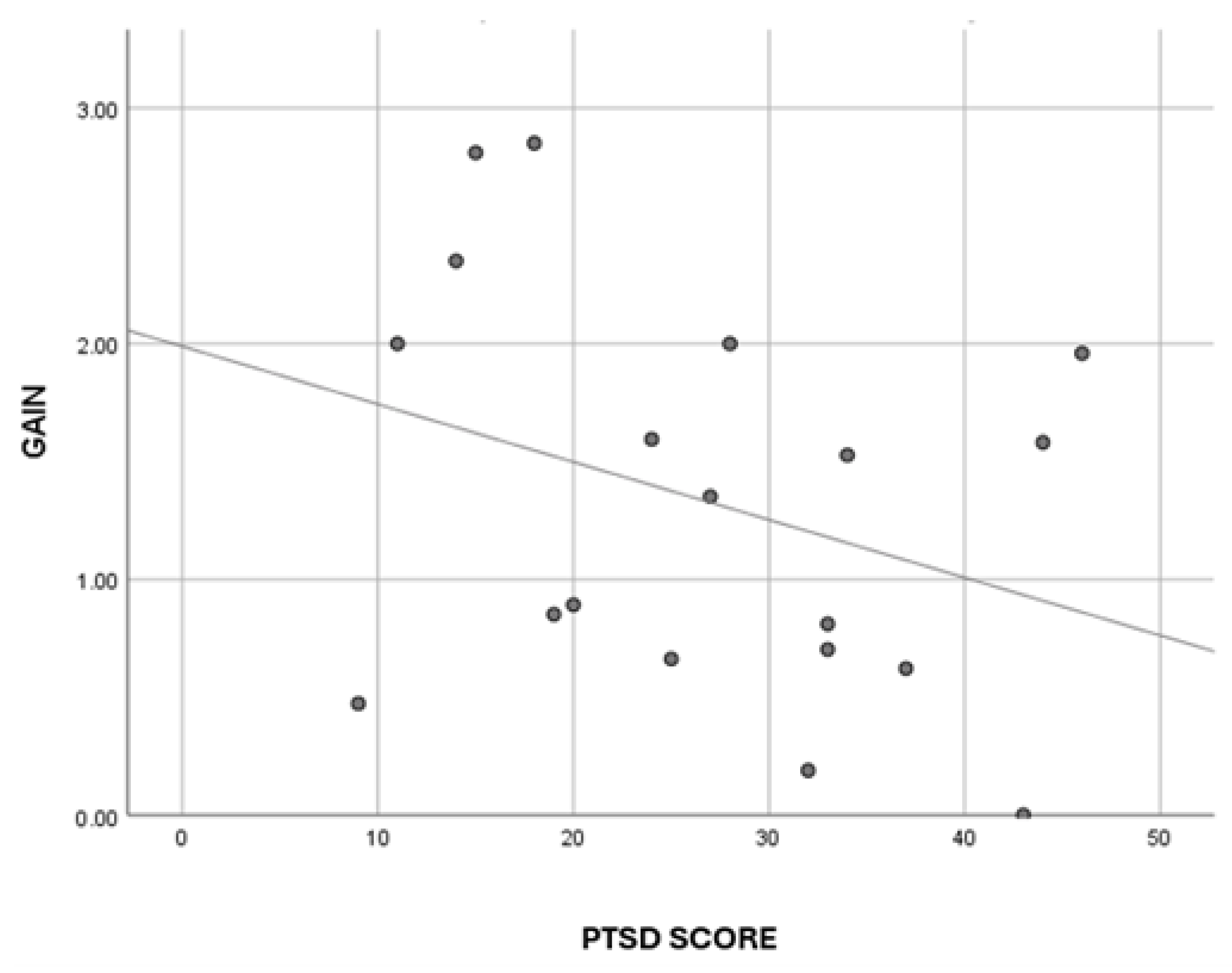
Hypothesis 2 (H2). Result: Greater resource gain will be associated with lower levels of PTSD symptoms was supported, which is a novel finding.
Hypothesis 3 (H3). Result: Additional resources will be identified by Veterans was confirmed, which is also a novel finding. There were no missing data.
Figure 3 displays the linear relationship between PTSD scores and resource loss (R
2 Linear = 0.073).
Figure 4 displays the linear relationship between PTSD scores and resource gain (R
2 Linear = 0.105).
Results of a point biserial Pearson correlation indicated there was a statistically significant medium negative correlation between PTSD diagnosis and resource gain (r(17) = −0.42, p = 0.039, one-tailed). A strong hypothesis of directionality was assumed; therefore, a one-tailed correlation analysis was utilized.
4.1. Comparing Means
Participants’ PTSD scores were divided several ways for data analysis: first, dichotomously (non-PTSD or PTSD); and second, ordinally, as defined by their respective categorical scores from the PSS-I. See
Table 1 for a summary of means by group.
4.2. Reliability
Internal consistency reliability coefficients were calculated using data from the PSS-I (α = 0.84), the COR-E gain scale (α = 0.98), and the COR-E loss scale (α = 0.99). All measures exhibited satisfactory internal consistency.
4.3. Independent t Test
An independent samples t test indicated no statistically significant differences between the M scores of resource loss and resource gain in the non-PTSD and PTSD groups. However, a large effect size in resource gain scores between PTSD and non-PTSD groups was found (t(17) = 1.880, p = 0.077, d = 0.87), with the non-PTSD group receiving higher resource gain scores than the PTSD group did.
4.4. One-Way ANOVA and Post Hoc
A statistically significant difference was found in resource gain scores between PTSD severity levels using a one-way ANOVA (F(2,16) = 4.062, p = 0.037). A Gabriel’s post hoc test revealed that the resource gain score in the mild PTSD group was significantly higher than that of the severe + very severe PTSD group (p = 0.034).
4.5. Open-Ended Questions Analysis
Thematic analysis of two open-ended questions was conducted. The four most common themes of additional resource loss items experienced were (a) a sense of meaning/purpose/direction, (b) safety and security, (c) trust in self and the greater good, and (d) connection/friendship. The four most common themes of additional resource gain items experienced were (a) self-empowerment, (b) fear/failure, (c) caring for self, and (d) role as an individual in a system (friendship, government). Types of resources that were additionally listed were primarily personal characteristics, and secondly condition resources.
5. Discussion
Although the sample size was small (limited by COVID-19), results are indicative of several patterns. Hypothesis 1 was only partially supported—a medium effect size was found between resource loss and PTSD, but not at the statistically significant level. Although it is a limited finding, it is similar to findings of previous studies of PTSD and resource loss [
3]. Using a larger sample, it is expected that data trends will continue, and statistical significance will emerge and re-affirm the original hypothesis that the more resources a person loses, the greater the severity of their PTSD.
Hypothesis 2 was supported—greater resource gain was associated with lower levels of PTSD symptoms. This finding is novel. Often, disease diagnosis and treatment emphasize loss, and how disease diagnosis follows loss. Using this new finding of “resource gain” and what a “patient can gain” to treat PTSD is a dramatic shift from a solely deficient perspective of disease treatment.
Hypothesis 3 was confirmed—additional resources that were lost and/or gained were identified by Veterans. This open-ended section of the COR-E was created to capture any additional resources that participants lost and/or gained that were not previously captured using the COR-E. The “openness” of the section allowed each participant to emphasize an individual loss or gain that other participants may not have necessarily experienced, but still resulted in varying levels of PTSD. This is clinically pertinent, especially from the perspective of treatment. This finding allows for a clearer understanding of which resources that are lost are associated with greater levels of PTSD and which resources that are gained are associated with lower levels of PTSD.
Implications
The COR theory states that throughout life one continuously accumulates, or gains, resources to later use to accommodate, withstand, or overcome threats [
1]. Threats are life events, stressors, and negative circumstances that consume resources. In this study, Veterans with higher PTSD severity demonstrated lower levels of gaining resources. Those with lower PTSD severity demonstrated higher levels of gaining resources. This indicated that PTSD is a threat to the accumulation of resources.
Systematically, Hobfoll defined
stability as the tendency to minimize the loss of evaluated resources in the adversity of negative circumstances and
efficiency as the tendency to quickly gain evaluated resources in the face of positive circumstances [
24]. A healthy system is paradoxically
stable and
efficient, akin to an “ebb and flow”, or two conflicting characteristics working in unison. Veterans with PTSD do not experience this in unison, but appear to struggle to minimize resource loss in the face of trauma and may not gain as many resources in positive situations.
6. Future Direction
This brief report calls for a larger study to confirm trends initially identified in this smaller sample size. Secondly, it calls for the use of a tailor-made resource list for Veterans to identify how trauma and PTSD have affected their ability to use and gain resources. With this list, Veterans can focus therapeutic efforts on minimizing resource losses (increasing stability) and gaining resources (maximizing efficiency) to promote a healthy resource system working in unison.
Author Contributions
Conceptualization and methodology: A.M., S.G., L.M. and M.H.; software: A.M.; validation: A.M., S.G., L.M. and M.H.; formal analysis: A.M.; investigation: A.M.; resources: A.M., S.G., L.M. and M.H.; data curation: A.M., S.G., L.M. and M.H.; writing—original draft preparation: A.M.; writing—review and editing: A.M., S.G., L.M. and M.H.; supervision: S.G., L.M. and M.H. All authors have read and agreed to the published version of the manuscript.
Funding
Residual funding was identified from M.H.’s research funds, and participants received USD 20 as compensation for completing this study.
Institutional Review Board Statement
This research study received Institutional Review Board (IRB) approval at Azusa Pacific University IRB (#18-010-OTH) in February 2018 and at the Tibor Rubin VA Medical Center (#1678) in October 2018.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
Data sharing will be considered under negotiation between interested partners and authors with VA IRB participation. Requests should be made to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hobfoll, S.E. Conservation of resources. A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Traumatic stress: A theory based on rapid loss of resources. Anxiety Res. 1991, 4, 187–197. [Google Scholar] [CrossRef]
- Hollifield, M.; Gory, A.; Siedjak, J.; Nguyen, L.; Holmgreen, L.; Hobfoll, S. The benefit of conserving and gaining resources after trauma: A systematic review. J. Clin. Med. 2016, 5, 104. [Google Scholar] [CrossRef]
- Blaze, J.; Shwalb, D. Resource loss and relocation: A follow-up study of adolescents two years after Hurricane Katrina. Psychol. Trauma. 2009, 1, 312–332. [Google Scholar] [CrossRef]
- Cordova, M.J.; Walser, R.; Neff, J.; Ruzek, J.I. Predictors of emotional adjustment following traumatic injury: Personal, social, and material resources. Prehosp. Disaster Med. 2005, 20, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Dekel, R.; Hobfoll, S.E. The impact of resource loss on Holocaust survivors facing war and terrorism in Israel. Aging Ment. Health 2007, 11, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.J.; Bonanno, G.A.; Bolton, P.A.; Bass, J.K. A longitudinal investigation of changes to social resources associated with psychological distress among kurdish torture survivors living in Northern Iraq. J. Trauma. Stress 2014, 27, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Heath, N.M.; Hall, B.J.; Russ, E.U.; Canetti, D.; Hobfoll, S.E. Reciprocal relationships between resource loss and psychological distress following exposure to political violence: An empirical investigation of COR theory’s loss spirals. Anxiety Stress Coping 2012, 25, 679–695. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Canetti-Nisim, D.; Johnson, R.J. Exposure to terrorism, stress-related mental health symptoms, and defensive coping among Jews and Arabs in Israel. J. Consult. Clin. Psychol. 2006, 74, 207–218. [Google Scholar] [CrossRef]
- Littleton, H.L.; Axsom, D.; Grills-Taquechel, A.E. Adjustment following the mass shooting at Virginia Tech: The roles of resource loss and gain. Psychol. Trauma. 2009, 1, 206–219. [Google Scholar] [CrossRef]
- Littleton, H.; Kumpula, M.; Orcutt, H. Posttraumatic symptoms following a campus shooting: The role of psychosocial resource loss. Violence Vict. 2011, 26, 461–476. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.C.; Hung, F.C.; Chen, S.H. “Changes or not” is the question: The meaning of posttraumatic stress reactions one year after the Taiwan chi-chi earthquake. J. Chin. Inst. Eng. 2002, 25, 609–618. [Google Scholar] [CrossRef]
- Egozi Farkash, H.; Lahad, M.; Hobfoll, S.E.; Leykin, D.; Aharonson-Daniel, L. Conservation of resources, psychological distress, and resilience during the COVID-19 pandemic. Int. J. Public Health 2022, 67, 1604567. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.D.; Hobfoll, S.E.; Lavin, J. When it rains, it pours: The greater impact of resource loss compared to gain on psychological distress. Pers. Soc. Psychol. Bull. 1999, 25, 1172–1182. [Google Scholar] [CrossRef]
- Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013.
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Keane, T.M.; Fairbank, J.A.; Caddell, J.M.; Zimering, R.T.; Taylor, K.L.; Mora, C.A. Clinical evaluation of a measure to assess combat exposure. J. Consult. Clin. Psychol. 1989, 1, 53–55. [Google Scholar] [CrossRef]
- Foa, E.; Tolin, D. Comparison of the PTSD Symptom Scale-Interview Version and the Clinician-Administered PTSD scale. J. Trauma. Stress 2000, 13, 181–191. [Google Scholar] [CrossRef]
- Foa, E.B.; Riggs, D.S.; Dancu, C.V.; Rothbaum, B.O. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J. Trauma. Stress 1993, 6, 459–473. [Google Scholar]
- Buchanan, E. MOTE Effect Size Calculator; Missouri State DOOM Lab: Springfield, IL, USA, 2018. [Google Scholar]
- Sala, G.; Inagaki, H.; Ishioka, Y.; Masui, Y.; Nakagawa, T.; Ishizaki, T.; Arai, Y.; Ikebe, K.; Kamide, K.; Gondo, Y. The psychometric properties of the Montreal Cognitive Assessment (MoCA): A comprehensive investigation. Swiss J. Psychol. 2020, 79, 155–161. [Google Scholar] [CrossRef]
- Tolle, K.; Montgomery, V.; Gradwohl, B.; Spencer, R.; Stelmokas, J. The Montreal Cognitive Assessment in veteran postacute care: Implications of cut scores. Cogn. Behav. Neurol. 2020, 33, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. The Ecology of Stress; Hemisphere Publishing: New York, NY, USA, 1988. [Google Scholar]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}
{kind=link}
{kind=link}