
Risk Factors for Groin Pain in Male High School Soccer Players Undergoing an Injury Prevention Program: A Cluster Randomized Controlled Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Randomization
2.3. Blinding
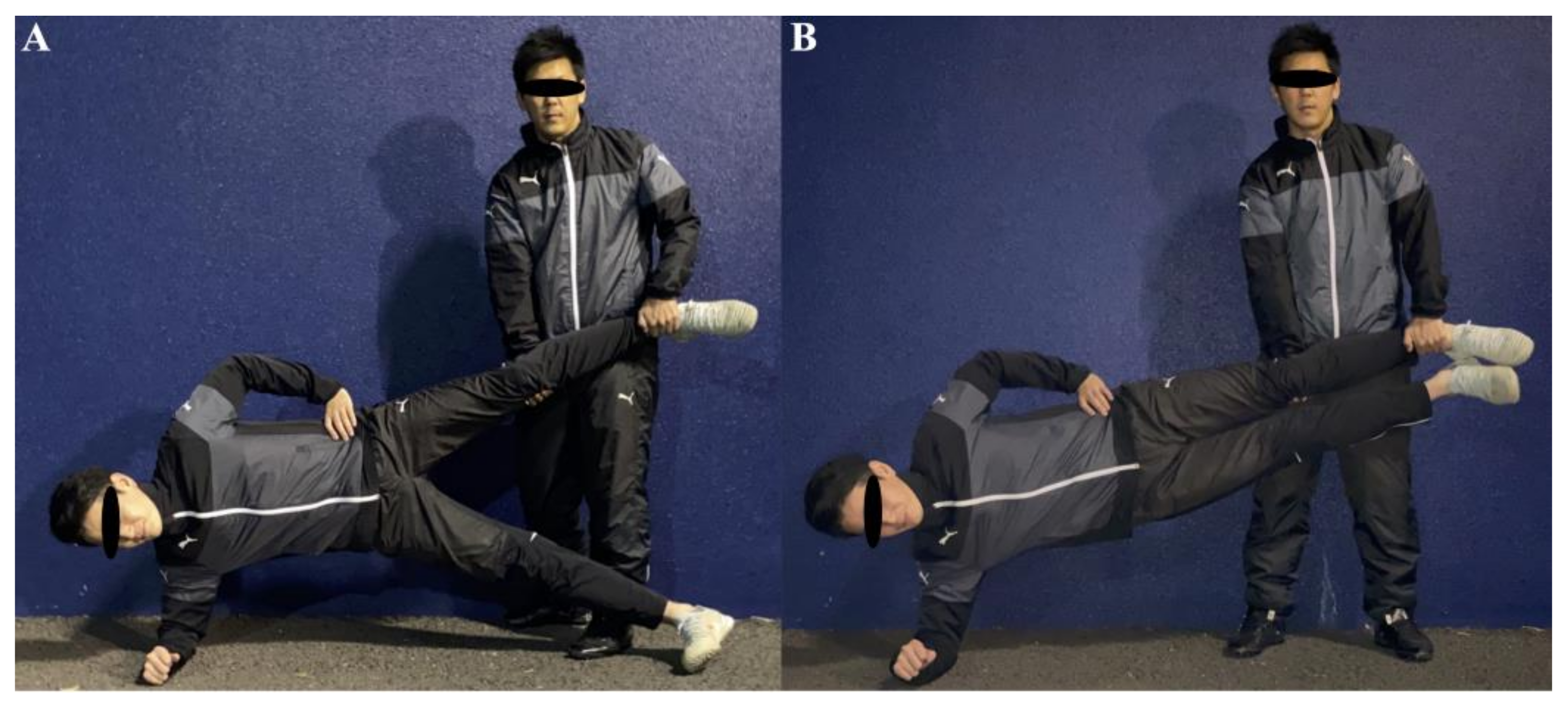
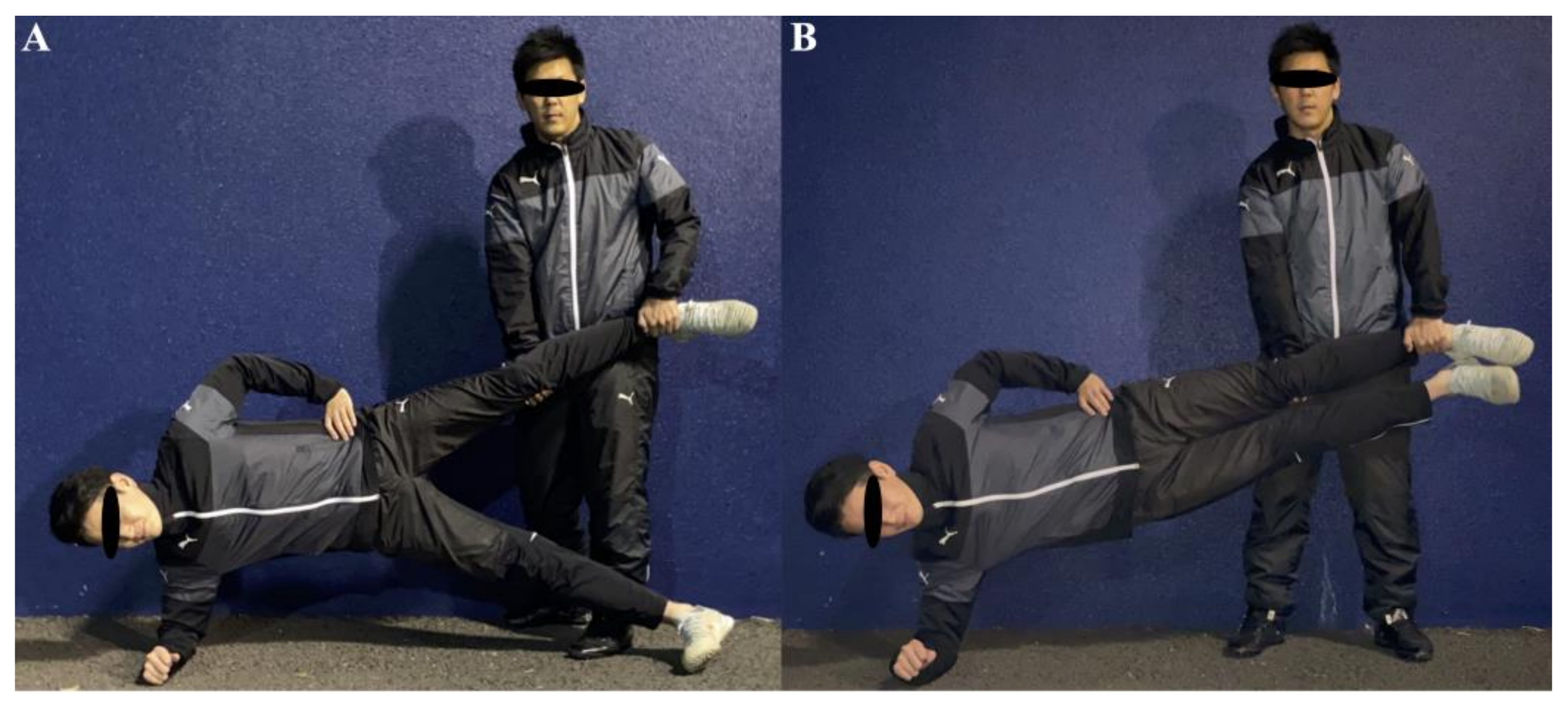
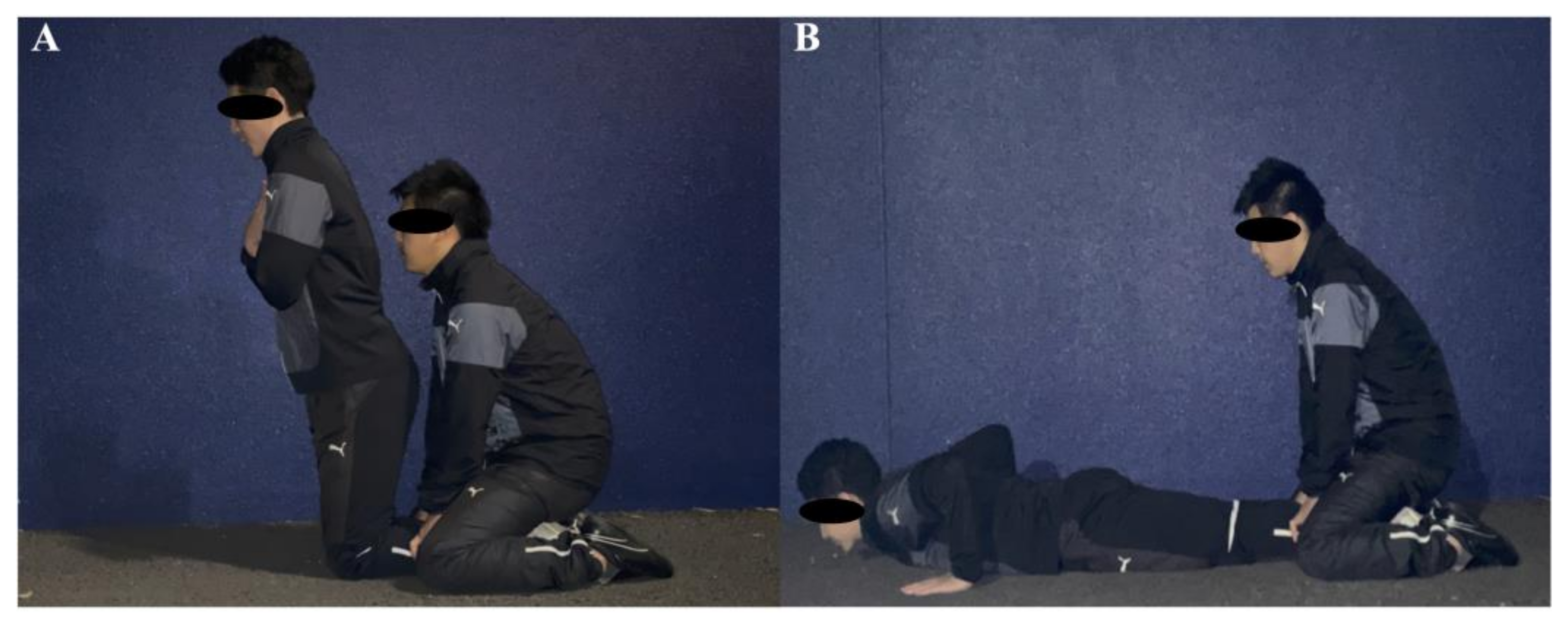
2.4. Intervention
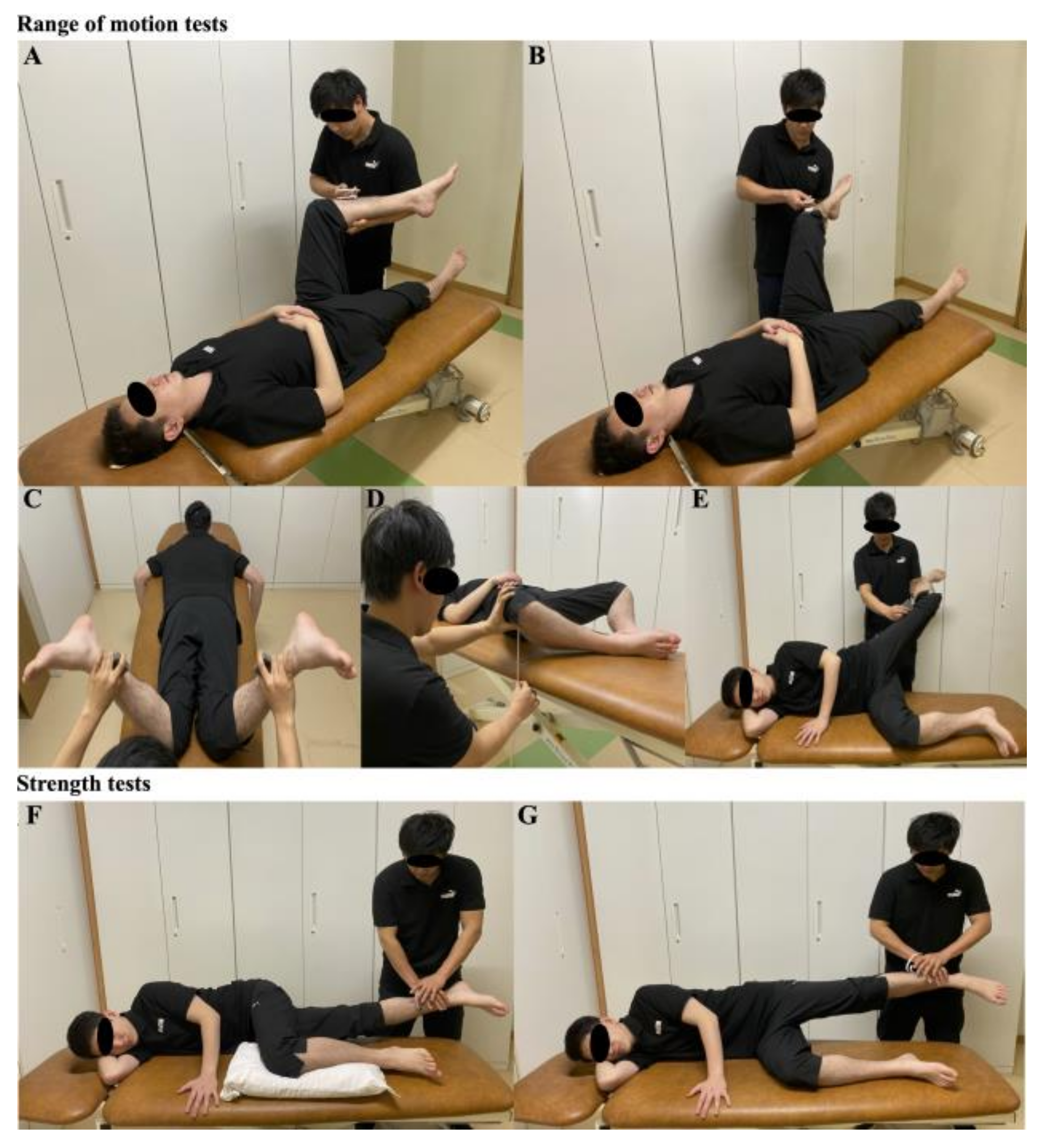
2.5. Risk Factor Screening
2.6. Injury Reporting
2.7. Sample Size
2.8. Statistical Analyses
3. Results
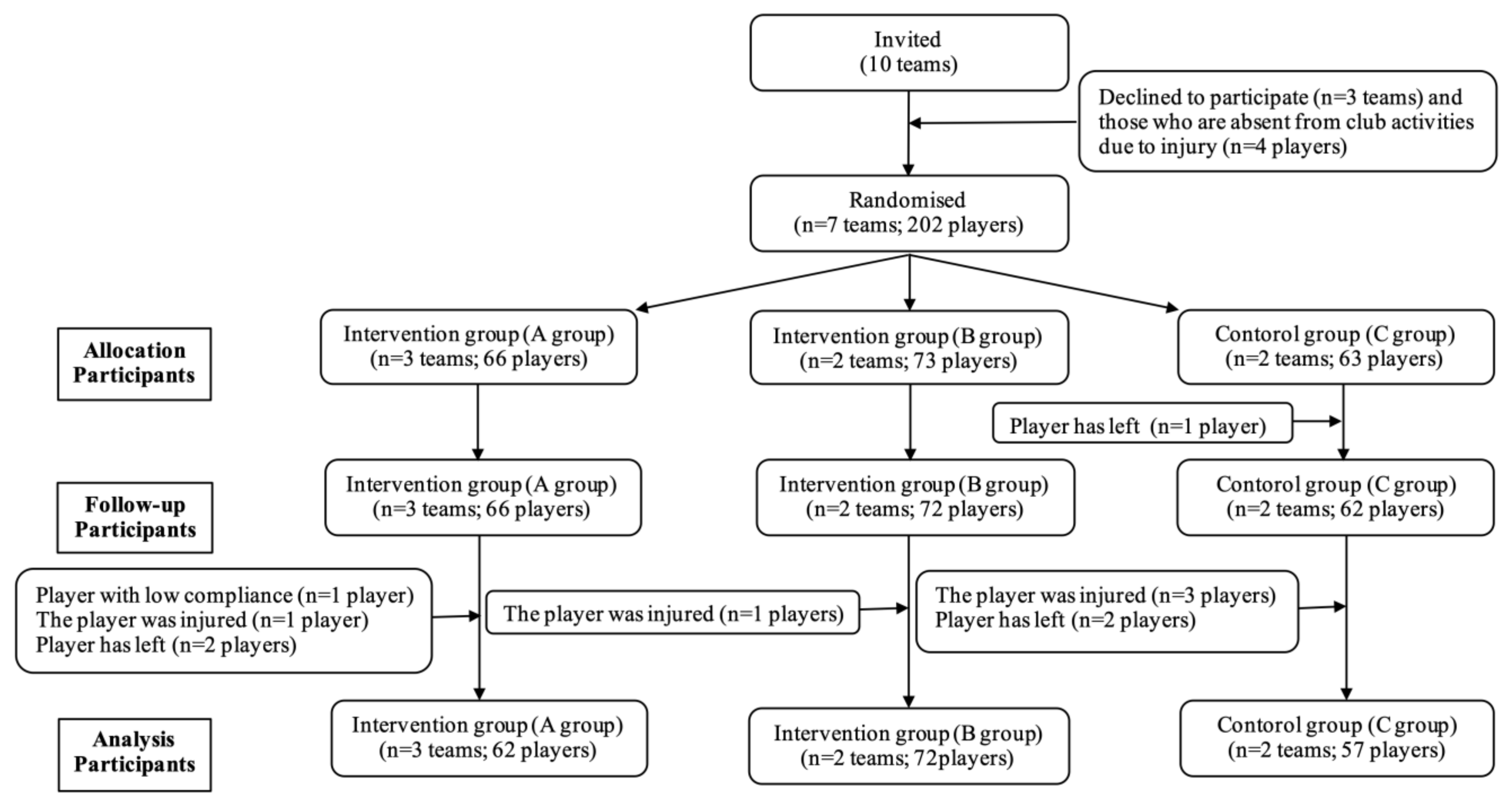
3.1. Participants
3.2. Injury Occurrence
3.3. Hip Variable Screening
3.4. Risk Factors for Groin Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brophy, R.H.; Backus, S.I.; Pansy, B.S.; Lyman, S.; Williams, R.J. Lower Extremity Muscle Activation and Alignment during the Soccer Instep and Side-foot Kicks. J. Orthop. Sports Phys. Ther. 2007, 37, 260–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judge, J.O.; Davis, B.R.; Ounpuu, S. Step length reductions in advanced age: The role of ankle and hip kinetics. J. Gerontol. A Biol. Sci. Med. Sci. 1996, 51, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Charnock, B.L.; Lewis, C.L.; Garrett, W.E., Jr.; Queen, R.M. Adductor longus mechanics during the maximal effort soccer kick. Sports Biomech. 2009, 8, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Chycki, J.; Golas, A.; Halz, M.; Maszczyk, A.; Toborek, M.; Zajac, A. Chronic Ingestion of Sodium and Potassium Bicarbonate, with Potassium, Magnesium and Calcium Citrate Improves Anaerobic Performance in Elite Soccer Players. Nutrients 2018, 10, 1610. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, R.D.; Fuller, C.W. A prospective epidemiological study of injuries in four English professional football clubs. Br. J. Sports Med. 1999, 33, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Gillquist, J. The Avoidability of Soccer Injuries. Int. J. Sports Med. 1983, 4, 124–128. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive seasons. Br. J. Sports Med. 2006, 40, 767–772. [Google Scholar] [CrossRef] [Green Version]
- Werner, J.; Hagglund, M.; Walden, M.; Ekstrand, J. UEFA injury study: A prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br. J. Sports Med. 2009, 43, 1036–1040. [Google Scholar] [CrossRef] [Green Version]
- Weir, A.; Brukner, P.D.; Delahunt, E.; Ekstrand, J.; Griffin, D.R.; Khan, K.M.; Lovell, G.; Meyers, W.C.; Muschaweck, U.; Orchard, J.; et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br. J. Sports Med. 2015, 49, 768–774. [Google Scholar] [CrossRef]
- Taylor, R.; Vuckovic, Z.; Mosler, A.; Agricola, R.; Otten, R.; Jacobsen, P.; Holmich, P.; Weir, A. Multidisciplinary Assessment of 100 Athletes with Groin Pain Using the Doha Agreement: High Prevalence of Adductor-Related Groin Pain in Conjunction with Multiple Causes. Clin. J. Sport Med. 2018, 28, 364–369. [Google Scholar] [CrossRef]
- Mosler, A.B.; Weir, A.; Eirale, C.; Farooq, A.; Thorborg, K.; Whiteley, R.J.; Hölmich, P.; Crossley, K.M. Epidemiology of time loss groin injuries in a men’s professional football league: A 2-year prospective study of 17 clubs and 606 players. Br. J. Sports Med. 2018, 52, 292–297. [Google Scholar] [CrossRef]
- Arnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Risk Factors for Injuries in Football. Am. J. Sports Med. 2004, 32, 5–16. [Google Scholar] [CrossRef]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.M.K.; Engebretsen, L.; Bahr, R. Intrinsic Risk Factors for Groin Injuries among Male Soccer Players: A prospective cohort study. Am. J. Sports Med. 2010, 38, 2051–2057. [Google Scholar] [CrossRef]
- Tyler, T.F.; Nicholas, S.J.; Campbell, R.J.; McHugh, M.P. The Association of Hip Strength and Flexibility with the Incidence of Adductor Muscle Strains in Professional Ice Hockey Players. Am. J. Sports Med. 2001, 29, 124–128. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. Risk factors for groin injuries in hockey. Med. Sci. Sports Exerc. 2001, 33, 1423–1433. [Google Scholar] [CrossRef]
- Ishøi, L.; Sørensen, C.N.; Kaae, N.M.; Jørgensen, L.B.; Hölmich, P.; Serner, A. Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial. Scand. J. Med. Sci. Sports 2016, 26, 1334–1342. [Google Scholar] [CrossRef]
- Harøy, J.; Clarsen, B.; Wiger, E.G.; Oyen, M.G.; Serner, A.; Thorborg, K.; Hölmich, P.; Andersen, T.E.; Bahr, R. The Adductor Strengthening Programme prevents groin problems among male football players: A cluster-randomised controlled trial. Br. J. Sports Med. 2019, 53, 145–152. [Google Scholar] [CrossRef]
- Polglass, G.; Burrows, A.; Willett, M. Impact of a modified progressive Copenhagen adduction exercise programme on hip adduction strength and postexercise muscle soreness in professional footballers. BMJ Open Sport Exerc. Med. 2019, 5, e000570. [Google Scholar] [CrossRef] [Green Version]
- Broski, S.M.; Murthy, N.S.; Krych, A.J.; Obey, M.R.; Collins, M.S. The adductor magnus “mini-hamstring”: MRI appearance and potential pitfalls. Skelet. Radiol. 2016, 45, 213–219. [Google Scholar] [CrossRef]
- Obey, M.R.; Broski, S.M.; Spinner, R.J.; Collins, M.S.; Krych, A.J. Anatomy of the Adductor Magnus Origin. Implications for Proximal Hamstring Injuries. Orthop. J. Sports Med. 2016, 4, 2325967115625055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjølsnes, R.; Árnason, Á.; Østhagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Mosler, A.B.; Crossley, K.M.; Thorborg, K.; Whiteley, R.J.; Weir, A.; Serner, A.; Hölmich, P. Hip strength and range of motion: Normal values from a professional football league. J. Sci. Med. Sport 2017, 20, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Mosler, A.; Agricola, R.; Thorborg, K.; Weir, A.; Whiteley, R.J.; Crossley, K.M.; Hölmich, P. Is Bony Hip Morphology Associated with Range of Motion and Strength in Asymptomatic Male Soccer Players? J. Orthop. Sports Phys. Ther. 2018, 48, 250–259. [Google Scholar] [CrossRef]
- Thorborg, K.; Couppe, C.; Petersen, J.; Magnusson, S.P.; Holmich, P. Eccentric hip adduction and abduction strength in elite soccer players and matched controls: A cross-sectional study. Br. J. Sports Med. 2011, 45, 10–13. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br. J. Sports Med. 2006, 16, 96–106. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of Injury Incidences in Male Professional Adult and Elite Youth Soccer Players: A Systematic Review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [Green Version]
- Cezarino, L.G.; da Silva Grüninger, B.L.; Silva, R.S. Injury Profile in a Brazilian First-Division Youth Soccer Team: A Prospective Study. J. Athl. Train. 2020, 55, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Kerbel, Y.E.; Smith, C.M.; Prodromo, J.P.; Nzeogu, M.I.; Mulcahey, M.K. Epidemiology of Hip and Groin Injuries in Collegiate Athletes in the United States. Orthop. J. Sports Med. 2018, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Attar, W.S.A.A.; Soomro, N.; Pappas, E.; Sinclair, P.J.; Sanders, R.H. Adding a post-training FIFA 11+ exercise program to the pre-training FIFA 11+ injury prevention program reduces injury rates among male amateur soccer players: A cluster-randomised trial. J. Physiother. 2017, 63, 235–242. [Google Scholar] [CrossRef]
- Tak, I.; Engelaar, L.; Gouttebarge, V.; Barendrecht, M.; Van Den Heuvel, S.; Kerkhoffs, G.; Langhout, R.; Stubbe, J.; Weir, A. Is lower hip range of motion a risk factor for groin pain in athletes? A systematic review with clinical applications. Br. J. Sports Med. 2017, 51, 1611–1621. [Google Scholar] [CrossRef] [Green Version]
- Rahnama, N.; Reilly, T.; Lees, A.; Graham-Smith, P. Muscle fatigue induced by exercise simulating the work rate of competitive soccer. J. Sports Sci. 2003, 21, 933–942. [Google Scholar] [CrossRef]
- Ekstrand, J.; Gillquist, J.; Möller, M.; Oberg, B.; Liljedahl, S.-O. Incidence of soccer injuries and their relation to training and team success. Am. J. Sports Med. 1983, 11, 63–67. [Google Scholar] [CrossRef]
- Price, R.J.; Hawkins, R.D.; Hulse, M.A.; Hodson, A. The Football Association medical research programme: An audit of injuries in academy youth football. Br. J. Sports Med. 2004, 38, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Hölmich, P.; Thorborg, K.; Dehlendorff, C.; Krogsgaard, K.; Gluud, C. Incidence and clinical presentation of groin injuries in sub-elite male soccer. Br. J. Sports Med. 2014, 48, 1245–1250. [Google Scholar] [CrossRef] [Green Version]
- Kearns, C.F.; Isokawa, M.; Abe, T. Architectural characteristics of dominant leg muscles in junior soccer players. Eur. J. Appl. Physiol. 2001, 85, 240–243. [Google Scholar] [CrossRef]
- Eberbach, H.; Fürst-Meroth, D.; Kloos, F.; Leible, M.; Bohsung, V.; Bode, L.; Wenning, M.; Hagen, S.; Bode, G. Long-standing pubic-related groin pain in professional academy soccer players: A prospective cohort study on possible risk factors, rehabilitation and return to play. BMC Musculoskelet. Disord. 2021, 22, 958. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Weekly Sessions | Sets (Per Side) a | Repetitions (Per Side) a | |
|---|---|---|---|---|
| CAE | 1 | 2 | 1 | 3–5 |
| 2 | 3 | 1 | 3–5 | |
| 3–4 | 3 | 1 | 7–10 | |
| 5–16 | 3 | 1 | 12–15 | |
| NHE | 1 | 1 | 2 | 5 |
| 2 | 2 | 2 | 6 | |
| 3 | 2 | 3 | 6 | |
| 4 | 2 | 3 | 6, 7, 8 | |
| 5–16 | 2 | 3 | 8, 9, 10 |
| A Group (n = 66) b | B Group (n = 73) b | C Group (n = 63) b | p-Value | |
|---|---|---|---|---|
| Age (years) a | 16.4 ± 0.9 (15–18) | 16.0 ± 0.7 (15–18) | 16.1 ± 0.9 (15–18) | 0.47 |
| Height (cm) a | 170.7 ± 5.7 (156.0–186.3) | 169.2 ± 5.2 (157.2–184.0) | 170.3 ± 5.1 (160.0–180.0) | 0.24 |
| Weight (kg) a | 60.2 ± 7.1 (40–83) | 58.4 ± 7.2 (42–80) | 58.5 ± 6.5 (45–74) | 0.39 |
| Dominant foot (players) | 0.22 | |||
| Right | 55 | 67 | 52 | |
| Left | 11 | 6 | 11 | |
| Field position (players) | 0.74 | |||
| Attackers | 10 | 12 | 11 | |
| Midfielders | 24 | 27 | 23 | |
| Defenders | 26 | 23 | 24 | |
| Goalkeepers | 6 | 11 | 5 |
| A Group b (n = 66) | B Group b (n = 73) | C Group b (n = 63) | χ2 Test p-Value | A Group vs. B Group | A Group vs. C Group | B Group vs. C Group | Post-Hoc d | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| p- Value | Effect Size (φ) | p- Value | Effect Size (φ) | p-Value | Effect Size (φ) | ||||||
| Number of Injuries (%) | |||||||||||
| Groin pain | 8 (12.1) | 4 (5.5) | 18 (28.6) | 0.01 | 0.16 | 0.12 | 0.02 c | 0.20 | 0.01 | 0.31 | B<C |
| Time-lost-to-sports groin pain | 6 (9.1) | 3 (4.1) | 16 (25.4) | 0.01 | 0.24 | 0.10 | 0.01 c | 0.22 | 0.01 | 0.30 | A.B<C |
| Variable | Groin Pain (n = 25) | Non-Groin Pain (n = 177) | p-Value | Effect Size (r) |
|---|---|---|---|---|
| Hip range of motion | ||||
| External rotation (°) | ||||
| Dominant leg | 36.8 ± 7.4 | 36.2 ± 9.6 | 0.79 | 0.02 |
| Non-Dominant leg | 39.8 ± 7.5 | 38.5 ± 8.6 | 0.45 | 0.53 |
| Internal rotation (°) | ||||
| Dominant leg | 27.6 ± 6.5 | 27.4 ± 9.1 | 0.65 | 0.01 |
| Non-Dominant leg | 26.7 ± 6.1 | 27.5 ± 8.4 | 0.40 | 0.03 |
| Internal rotation in the prone position (°) | ||||
| Dominant leg | 35.7 ± 7.4 | 33.9 ± 8.3 | 1.00 | 0.07 |
| Non-Dominant leg | 35.3 ± 6.4 | 35.3 ± 7.9 | 0.59 | 0.01 |
| Abduction (°) | ||||
| Dominant leg | 46.1 ± 6.5 | 41.0 ± 5.8 | <0.001a | 0.27 |
| Non-Dominant leg | 45.5 ± 6.5 | 41.3 ± 6.2 | 0.02 a | 0.21 |
| Bent knee fall out (cm) | ||||
| Dominant leg | 13.3 ± 4.5 | 14.1 ± 4.2 | 0.37 | 0.06 |
| Non-Dominant leg | 13.8 ± 4.0 | 13.9 ± 4.0 | 0.94 | 0.01 |
| Eccentric muscle strength | ||||
| Adduction (Nm/Kg) | ||||
| Dominant leg | 2.6 ± 0.3 | 2.9 ± 0.4 | <0.001 a | 0.26 |
| Non-Dominant leg | 2.5 ± 0.3 | 2.9 ± 0.5 | <0.001 a | 0.15 |
| Abduction (Nm/Kg) | ||||
| Dominant leg | 2.0 ± 0.3 | 2.1 ± 0.3 | 0.04 a | 0.24 |
| Non-Dominant leg | 2.0 ± 0.3 | 2.2 ± 0.3 | 0.02 a | 0.17 |
| B a | SE b | p-Value | Odds | 95% CI of Odds | |||
|---|---|---|---|---|---|---|---|
| Min | Max | ||||||
| Hip range of motion | |||||||
| External rotation | |||||||
| Dominant leg | 0.006 | 0.023 | 0.79 | 1.01 | 0.96 | 1.05 | |
| Non-dominant leg | 0.019 | 0.025 | 0.45 | 1.02 | 0.97 | 1.07 | |
| Internal rotation | |||||||
| Dominant leg | 0.003 | 0.024 | 0.90 | 1.00 | 0.96 | 1.05 | |
| Non-dominant leg | −0.012 | 0.027 | 0.64 | 0.99 | 0.94 | 1.04 | |
| Internal rotation in prone | |||||||
| Dominant leg | 0.027 | 0.026 | 0.31 | 1.03 | 0.98 | 1.08 | |
| Non-dominant leg | 0.001 | 0.028 | 1.00 | 1.00 | 0.95 | 1.06 | |
| Abduction | |||||||
| Dominant leg | 0.145 | 0.039 | 0.01 d | 1.13 | 1.05 | 1.22 | |
| Non-dominant leg | 0.106 | 0.035 | 0.01 d | 1.11 | 1.04 | 1.19 | |
| BKFO c | |||||||
| Dominant leg | −0.047 | 0.052 | 0.37 | 0.96 | 0.86 | 1.06 | |
| Non-dominant leg | −0.004 | 0.054 | 0.94 | 1.00 | 0.90 | 1.11 | |
| Eccentric muscle strength | |||||||
| Adduction | |||||||
| Dominant leg | −1.991 | 0.568 | 0.01 d | 0.14 | 0.05 | 0.42 | |
| Non-dominant leg | −1.707 | 0.514 | 0.01 d | 0.18 | 0.07 | 0.50 | |
| Abduction | |||||||
| Dominant leg | −1.307 | 0.639 | 0.04 d | 0.27 | 0.08 | 0.95 | |
| Non-dominant leg | −1.476 | 0.639 | 0.02 d | 0.23 | 0.07 | 0.80 | |
| B b | SE c | p-Value | Odds | 95%CI of Odds | |||
|---|---|---|---|---|---|---|---|
| Min | Max | ||||||
| Hip Range of Motion | |||||||
| Abduction | Dominant leg | 0.152 | 0.043 | 0.01 d | 1.16 | 1.07 | 1.266 |
| Eccentric Muscle Strength | |||||||
| Adduction | Dominant leg | −2.123 | 0.601 | 0.01 d | 0.12 | 0.04 | 0.39 |
| Constant | −2.614 | 2.317 | 0.26 | 0.07 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujisaki, K.; Akasaka, K.; Otsudo, T.; Hattori, H.; Hasebe, Y.; Hall, T. Risk Factors for Groin Pain in Male High School Soccer Players Undergoing an Injury Prevention Program: A Cluster Randomized Controlled Trial. Trauma Care 2022, 2, 238-250. https://doi.org/10.3390/traumacare2020020
Fujisaki K, Akasaka K, Otsudo T, Hattori H, Hasebe Y, Hall T. Risk Factors for Groin Pain in Male High School Soccer Players Undergoing an Injury Prevention Program: A Cluster Randomized Controlled Trial. Trauma Care. 2022; 2(2):238-250. https://doi.org/10.3390/traumacare2020020
Chicago/Turabian StyleFujisaki, Kazuki, Kiyokazu Akasaka, Takahiro Otsudo, Hiroshi Hattori, Yuki Hasebe, and Toby Hall. 2022. "Risk Factors for Groin Pain in Male High School Soccer Players Undergoing an Injury Prevention Program: A Cluster Randomized Controlled Trial" Trauma Care 2, no. 2: 238-250. https://doi.org/10.3390/traumacare2020020
APA StyleFujisaki, K., Akasaka, K., Otsudo, T., Hattori, H., Hasebe, Y., & Hall, T. (2022). Risk Factors for Groin Pain in Male High School Soccer Players Undergoing an Injury Prevention Program: A Cluster Randomized Controlled Trial. Trauma Care, 2(2), 238-250. https://doi.org/10.3390/traumacare2020020