Abstract
Practitioners routinely use the single leg heel raise (SLHR) to quantify calf function in healthy and injured populations. Despite this, approaches vary and the impact of cueing on SLHR performance and results interpretation in athletesis unknown. The primary aim of this study was to quantify the level of agreement of the cued versus non-cued SLHR tests. The secondary aim was to explore test outcomes and the potential impact of intrinsic factors. Cued and non-cued SLHR tests were conducted in fifty-one Australian football players (23 women, 28 men). Metronome pacing (60 bpm) and five key cues were included in the cued condition. The level of agreement (Bland–Altman) between tests was measured for capacity (repetitions to failure) and asymmetry. Data from 100 legs were included. The non-cued and cued SLHR tests demonstrated poor agreement in both capacity and asymmetry. More repetitions to failure were performed in the non-cued SLHR [Mean (SD) = 33.9 (10.3) vs. 21.9 (5.3), p < 0.001)], and men had greater capacity (36.8 (10.4) vs. 30.3 (9.2), p < 0.001). During the cued SLHR, older players (age ≥ 30 years: −5.1 repetitions, p = 0.01) and Indigenous players (−3.4 repetitions, p = 0.002) and had reduced calf muscle function. Cueing the SLHR test significantly changes the result—outcomes are not comparable or interchangeable with the commonly used non-cued SLHR. These findings can guide practitioners quantifying calf capacity.
Keywords:
heel raise; calf; soleus; gastrocnemius; strength; endurance; injury prevention; muscle strain 1. Introduction
Calf muscle capacity is critical to lower limb function across the spectrum of locomotive and functional activities [1,2,3]. Practitioners commonly use the single leg heel raise (SLHR) test to quantify calf muscle strength–endurance as a measure of capacity in healthy [4] and clinical populations [5], as well as athletes [6,7].
Methods to perform the SLHR test vary [8,9]. The range of loading rate (beats per minute), ankle dorsiflexion (over the edge of a step vs. 10° incline vs. flat ground) and plantar flexion (partial vs. maximum height) requirements reported in research may have contributed to the inconsistency seen clinically [10]. Specific instructions and cues have been a key consideration in contemporary research and clinical settings to help standardise practice [11]. Performance and technique cues during the SLHR test may alter the number of repetitions to failure performed and potentially provide a more robust indication of an individual’s capacity when screening athletes [12,13]. Although the long-held clinical hypothesis that cueing is warranted is yet to be substantiated in Australian football players [12]. Whether cueing the SLHR test in this population significantly impacts test outcomes and the practical interpretation of theresults between conditions is unknown.
Standardising SLHR performance using cues may increase the strength of the comparisons that can be made between different people and samples [8], or after injury. Conversely, consistency and optimal performance appear unlikely clinically when these efforts are not made [14], resulting from ‘uncontrolled’ or non-cued testing. Sub-optimal use of the calf muscles, or test completion at rates that are not consistent with strength measurement [15], are potential negative consequences of the non-cued SLHR. For example, without metronome pacing, more rapid loading rates may bias elastic tissues and recoil rather than measuring the repeated force-generating capacity (i.e., strength–endurance) of the contractile elements within the calf muscles [15,16,17].
Clinicians value understanding how test procedures can impact (and potentially improve) their practice and patient outcomes [18]. This is especially apparent for practitioners aiming to use these data to help prevent or manage injuries involving the calf muscle–tendon unit, that could be associated with reduced strength-endurance, such as calf muscle strain injuries [12,19] and Achilles Tendinopathy [20,21]. Calf muscle–tendon unit injuries are problematic in athletes [22,23], and, particularly in Australian football, the consistent prevalence and susceptibility of players to recurrent calf muscle strain injuries represents a growing injury burden [24,25]. For these reasons there is high clinical value in improving practice in the implementation of SLHR testing and the interpretation of the results, based on the approach used.
Despite the potential practical value, studies investigating SLHR outcomes under non-cued versus cued conditions in athletic populations are lacking [9]. An evaluation has not been undertaken in male and female Australian football players either. The primary aim of this study was to quantify the level of agreement of the cued versus non-cued SLHR tests in terms of capacity (i.e., repetitions to failure) and asymmetry (i.e., between-leg differences). The secondary aim was to measure and describe the SLHR test outcomes, including an exploration of the potential impact of intrinsic factors, to help guide future prevention research.
2. Materials and Methods
Human Research Ethics Committee approval was obtained for this study from The University of Notre Dame Australia (Approval: 2022-149F). Fifty-seven participants from the Western Australian Football League men’s and women’s leagues were recruited for SLHR testing during the 2023 preseason. Excluded participants (1) opted out after the first testing session due to soreness (n = 2) or (2) provided incomplete baseline data (n = 4). One leg was excluded for two participants due to an injury that precluded the leg from testing. All participants provided informed consent via an online Qualtrics survey (Qualtrics, Provo, UT, USA. https://www.qualtrics.com (accessed November 2022–March 2023).
Two commonly researched [10,26,27] and clinically utilised SLHR methods were used. Tests were conducted at two separate preseason training sessions spaced ≥ 6 days apart (i.e., to ensure the first testing session would not impact the second). One of three authors (either BG, MC or MCM) assessed the non-cued SLHR test. One author (BG) performed all cued SLHR tests. To avoid contamination of the cued SLHR, the non-cued SLHR was conducted in the first training session for almost all (92%) players. Reliable methods were used in the cued SLHR, which involved standardised performance and technique cues and associated failure criteria (Supplementary Table S1) [13,26,27].
Baseline characteristics were self-reported using Qualtrics prior to SLHR testing. The following data were recorded: chronological age (years), height (cm), weight (kg), ethnicity (as per Australian Bureau of Statistics recommendations), gender (man, woman, non-binary, prefer not to say), leg dominance (left, right, ambidextrous), competition level (league, reserves), injury history (yes/no for different injury regions), playing age (years playing Australian Football) and calf resistance training history (completing calf-focused resistance training: yes/no). International Olympic Committee (IOC) standards were used to categorise injury history data by region and type [28]. Chronological age data were handled both as continuous and categorical. Two age categories were used in separate analyses, which were based on current evidence and validated approaches [29]: (1) Age > cohort median, as older athletes are susceptible to recurrent calf muscle strain injuries [30] and (2) age ≥ 30 years, as individuals over 30 years of age have a higher incidence of calf muscle strain and Achilles tendon injuries [31,32].
In the non-cued SLHR, players performed repetitions until volitional failure was reached (i.e., volitional failure was the only reason for test cessation) [10]. During the cued SLHR, the test ended if volitional or technical failure was reached. Technical failure was based on observation and specifically occurred when cues could not be followed (Supplementary Table S1): (1) metronome pace could not be maintained (60 bpm/30 repetitions per minute), (2) knee flexion occurred, (3) a hip propulsive strategy was used, (4) vertical displacement was lost (i.e., movement forwards rather than upwards/trunk lean) and (5) there were marked deviations from plantar flexion height and alignment [7,10,26]. Testers provided generic verbal encouragement in both tests to help ensure the test was maximal. During the cued SLHR only, all players received a verbal reminder if a deviation in technique occurred, but if the error remained the test was ceased (Supplementary Table S1) and these repetitions were not counted [7,10,26]. The number of repetitions for each leg was recorded for both tests. Data were imported into and analysed in SPSS (IBM SPSS Statistics Windows, Version 29.0. Armonk, NY, USA: IBM Corp).
Frequency distributions were generated to describe categorical variables. Continuous data were evaluated for normality (raw visualisation, Shapiro–Wilk test) and were explored using descriptive statistics (mean, median, standard deviation (SD), interquartile range, range). Bland–Altman plots were generated to evaluate the level of agreement between tests for both repetitions to failure and asymmetry. Limits of agreement were calculated (mean difference ± 1.96x*standard deviation) [33,34] and simple linear regressions were used to identify the risk of proportional bias.
The SLHR test scores were non-normally distributed. Performance was measured using the Wilcoxon Signed-Rank test to compare repetitions to failure between the non-cued vs. cued SLHR tests. Parametric (independent samples t-test: cued SLHR) and non-parametric (Mann–Whitney U: non-cued SLHR) tests were used to explore the potential differences in test performance based on categorical intrinsic characteristics (e.g., age (>cohort median (yes/no); ≥30 years (yes/no)), leg dominance (dominant vs. non dominant leg), gender (women vs. men), ethnicity (Indigenous vs. non Indigenous) and exposure to calf-focused resistance training (yes/no)). Simple linear regressions were performed for continuous variables to explore potential correlations with performance (e.g., chronological age, playing age, height, weight, body mass index (BMI)). Results were considered significant if p < 0.05.
3. Results
3.1. Player Characteristics
Fifty-one players [women: 23 (45%); men: 28 (55%)] were included. Players were predominantly of Australian ethnicity (88%), with 6% of participants being of ‘Aboriginal or Torres Strait Islander’ (i.e., Indigenous Australian) ethnicity. Players were predominantly league-level (e.g., ‘senior’ WAFL/W level) (65%). Almost half of the players (45%) had a previous lower limb injury, and the majority (87%) of previous lower limb injuries were muscle–tendon injuries. The complete demographics of the cohort are described in Supplementary Tables S2 and S3.
3.2. Calf Muscle Strength–Endurance
Matched non-cued and cued SLHR results from 100 legs were included. Players were tested before (18%), during (25%) and after (35%) field-based training, or during a designated lower body gym session on a separate day to field-based training (22%). Cessation of the cued SLHR was due to volitional (43%) or technical (57%) failure. The most common reasons for technical failure were reduced plantar flexion height = 49.1%; knee flexion = 24.6%; hip strategy = 10.5%; trunk rocking back and forth = 8.8%; and foot/ankle alignment during plantar flexion = 7%.
Repetitions to failure between tests were moderately correlated (r = 0.49, p < 0.001). Players recorded on average 12 fewer repetitions during the cued SLHR [mean (SD) = −12 (8.9) repetitions: Z = −8.53, p < 0.001] (Figure 1, Table 1). Only four limbs (4%) performed the same or more repetitions during the cued SLHR (equal: 1%; more: 3%). Men had a greater non-cued SLHR capacity compared to women [mean (SD) = +6.5 (18.6) repetitions: U = 755, p < 0.001] (Table 1). Indigenous players had a reduced cued SLHR capacity compared to non-Indigenous Australian players [mean (SD) = −3.4 (7.7) repetitions: t(15.5) = −3.8, p = 0.002].
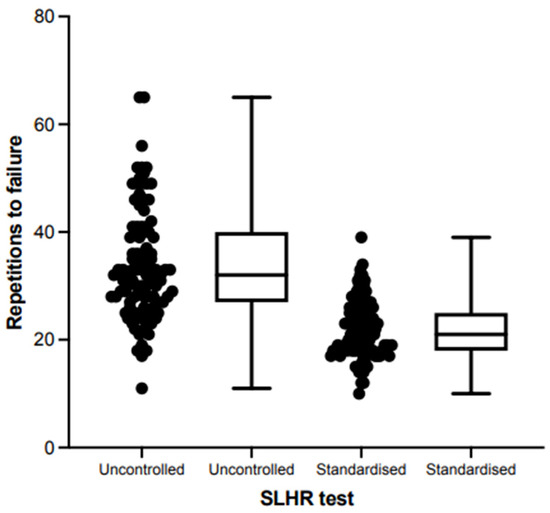
Figure 1.
Scatter, box and whisker plots for repetitions to failure during the non-cued (‘uncontrolled’) and standardised (‘cued’) single leg heel raise tests.

Table 1.
Calf strength–endurance during the non-cued and cued single leg heel raise tests.
Chronological age was not associated with SLHR performance when handled as a continuous variable (non-cued: r = −0.14, p = 0.16; cued: r = −0.12, p = 0.22). A subgroup analysis revealed that players ≥30 years old (n = 8 legs) were weaker during the cued [mean (SD) = 17 (2.2) vs. 22.1 (5.3) repetitions: t (98/4.7) = −4.2, p = 0.01] but not during the non-cued SLHR (mean (SD) = 31.5 (7.1) vs. 33.9 (10.4) repetitions: U = 169, p = 0.69). Players who reported completing calf muscle resistance training performed a greater number of SLHR repetitions to failure during both tests compared to players not undertaking this form of loading (non-cued: (SD) = +4.8 (19) repetitions, U = 873.5, p = 0.03; cued: +3.3 (10) repetitions, t (90.6) = 3.3, p = 0.001). Leg dominance and all other intrinsic player characteristics were not associated SLHR repetitions to failure under both conditions, including injury history (p > 0.05 for all).
Between-leg asymmetry during the cued [mean (SD) = 2.7 (2.1) repetitions, median: 2, range: 0–9] and non-cued [mean (SD) = 2.9 (2.9) repetitions, median: 2, range: 0–12] SLHR tests were similar (Z = −0.46, p = 0.65). Individual asymmetries during both tests were not correlated (r = 0.06, p = 0.67). Intrinsic player characteristics were not associated with asymmetry during either SLHR test (p > 0.05 for all).
3.3. Agreement between Tests
Clinically wide limits of agreement were identified when comparing the cued and non-cued SLHR repetitions to failure (mean difference ± 1.96x*SD = −5.0 to 29.5 repetitions) (Figure 2A) and asymmetry (mean difference ± 1.96x*SD = −6.9 to 7.6 repetitions) (Figure 2B). Linear regression also revealed a risk of proportional bias, with a moderate–strong correlation (r = 0.63, p < 0.001) between mean SLHR repetitions to failure and the difference in repetitions to failure performed between tests (Figure 2A). When comparing asymmetry, a proportional bias (r = 0.29, p = 0.15) or a bias towards greater asymmetry during either test (mean difference: 0.33 (3.7) repetitions, 95%CI −0.7–1.4) (Figure 2B) was not identified. Interpreted together, these findings demonstrate poor agreement between the SLHR tests and indicate that the scales of measurements within the non-cued and cued SLHRare not clinically equivalent.
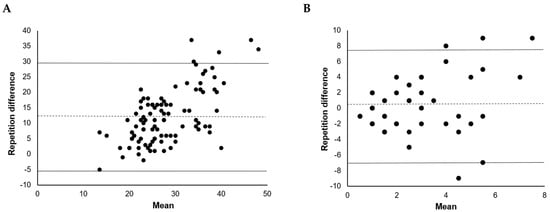
Figure 2.
Bland–Altman plots of the differences in repetitions to failure (A) and asymmetry (B) measured during the non-cued and cued single leg heel raise tests.
4. Discussion
Three key clinically relevant outcomes were demonstrated from this study: (1) the cued and non-cued SLHR tests do not measure the same construct (i.e., calf muscle strength–endurance) interchangeably—the test results are not directly comparable; (2) intrinsic factors (i.e., sex, chronological age, calf-focused resistance training exposure, ethnicity) may impact the repeated force-generating capacity of the calf muscles and warrant investigation in a larger cohort; and (3) the strength data generated from this research now exist to guide practitioners.
The repetitions to failure obtained from the cued and non-cued versions of the SLHR tests are not comparable clinically [33,34]. Our results support a long-standing hypothesis that these test conditions should not be considered interchangeable field-based or clinical measures of calf muscle function in practical settings [8]—form matters. By proxy, this may extend into SLHR interventions and explain why some SLHR interventions have a minimal effect on SLHR repetitions to failure [35] and even clinical improvement. Our results revealed that the scales of measurement within these tests are not equivalent and that Australian football players are biased towards recording a greater number of repetitions during the non-cued SLHR.
From our results and current evidence, we hypothesise that the cued SLHR test provides a more accurate representation of the repeated force-generating capacity of the contractile elements within the calf muscle–tendon unit [7,8]. Task constraints (e.g., controlling the loading rate at 60 bpm and the provision of technical cues) likely make the cued SLHR test preferential for muscular performance and increase the time under tension (i.e., cumulative load) encountered [15].
Non-cued conditions often involve the use of faster loading rates in order to utilise the stretch–shortening cycle and reduce the metabolic cost to the working muscles—incurring a greater contribution from the elastic elements of the muscle–tendon unit [16,17]. It is also possible that non-cued testing alters calf muscle work. For example, uncontrolled mechanics may result in an altered range of motion, a loss of vertical displacement (peak and cumulative), suboptimal calf muscle recruitment and the utilisation of other muscles when executing the task. From these perspectives, cueing the SLHR test may provide clinicians with a robust method to determine the repeated force-generating capacity (i.e., strength–endurance) of the calf muscles. In addition to the role of cues in standardising SLHR performance, clinicians should consider the potential impact of intrinsic factors on calf muscle strength–endurance.
We identified intrinsic factors that may be associated with reduced calf muscle strength–endurance and warrant future evaluation. Non-modifiable (female athletes, age ≥ 30 years, Indigenous ethnicity) and modifiable (previous calf muscle resistance training exposure) factors impacted the number of repetitions to failure in the SLHR of Australian football players in the current study. While the low number of players with Indigenous ethnicity should be acknowledged, the exploratory nature of the second study aim and the need for further research is highlighted. When considering the susceptibility of women, Indigenous and older athletes to injuries involving the calf muscles (e.g., calf muscle strain [24,36,37,38] or tendon injury [32]), combined with the findings of the current study, future exploration of the potential preventative role of strengthening in these athletes may be supported as well.
Intrinsic factors can negatively impact calf muscle ‘performance fatigability’ and strength [7]. The association between older age and a previous calf muscle–tendon unit injury with reduced strength qualities, or the structural (e.g., cross-sectional area) and functional (e.g., total displacement) correlates of them, areestablished [7,26,39,40]. Our results support the potential impact of ageing on SLHR strength–endurance. The fewer cued repetitions to failure in players aged >30 years is consistent with previous data, highlighting the reduction in SLHR capacity with each decade of life [26]. These data could reflect the onset of more pronounced age-related changes affecting calf muscle structure or function.
Our findings may suggest that the SLHR test has the capacity to detect differences in the calf function of men and women athletes participating in the same sport. Previous research has not always demonstrated these differences according to sex, including maximum voluntary isometric contraction [4]. Nonetheless, while reduced calf muscle strength–endurance is hypothesised to increase the injury risk clinically, due to mechanisms such as reduced load tolerance and performance fatigability [12,41], whether different strength qualities mitigate the impact of non-modifiable intrinsic factors (e.g., age, injury history) on injury susceptibility warrants prospective evaluation in women’s and men’s league athletes.
This study provides calf muscle strength–endurance data, assessed using the SLHR test for both men’s and women’s Australian football codes. Calf strength–endurance is an important capacity to quantify clinically [8,26], as well as from a performance perspective [6]. Despite being a clinical measure of strength, it is not always closely correlated to maximum isometric calf strength [4]. Strength–endurance represents a discrete capacity [42,43] that may be especially important to athletes that require the calf muscles to possess ‘performance fatigability’ (i.e., fatigue resistance) and repeatedly generate force, such as during running [6,41]. Our cued SLHR data are also comparable to recent findings in New Zealand rugby athletes using a standardised protocol [mean (SD) = 22 (5) vs. 20 (5) [7] repetitions]. We also found that completing specific loading for the calf muscles (in the form of calf-focused resistance training) was associated with better strength–endurance. While evidence for the preventative role of strengthening in the calf muscles is lacking [44], this preliminary finding potentially highlights the practical impact of devoted loading on improving calf muscle function in sporting populations.
Strengths and Limitations
Our study is the first evaluation of the role of clinically cueing the SLHR test in any Australian football code. Our study is also the first quantification of SLHR strength–endurance in Western Australian Football League men’s and women’s players. The order of the tests were not randomised to reduce the risk of bias associated with performing the cued SLHR prior to the non-cued SLHR. The risk of confounding was also minimised by separating the testing sessions by at least 6 days, reducing the likelihood that performance would be affected by fatigue from the first testing session [4]. When conducting the cued SLHR test, all players were cued to focus on the same technical elements—contributing to standardised task completion and participant intent. In addition to controlling the loading rate, a metronome (at 60 bpm) standardised the time under tension, though it is not known what the optimal pace is, despite its common use in research [10]. As a result of our findings, clinicians are provided with data that may act as a minimum acceptable standard. It is unavoidable that some athletes may have experienced fatigue due to completing training either prior to or concurrent with the testing session, or as a result of other training activities completed in the preceding days. Due to availability, it was also unavoidable that four players performed the cued SLHR test first.
5. Conclusions
The non-cued SLHR test commonly used in clinical practice does not provide comparable capacity or asymmetry data to the cued version of the SLHR test. Strength testing methods that provide the most value for calf injury prevention is unknown and warrants further research.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/biomed4020007/s1, Table S1: clinical procedure for non-cued and cued single leg heel raise tests; Table S2: intrinsic player characteristics; Table S3: player demographic information.
Author Contributions
Conceptualisation: B.G., M.C.M., E.K.R. and T.P.; Methodology: B.G., M.C.M., E.K.R. and T.P.; Formal Analysis: B.G., M.C. and M.C.M.; Investigation: B.G., M.C. and M.C.M.; Data Curation: B.G., M.C. and M.C.M.; Writing—original draft preparation: B.G. and M.C.M.; Writing—review and editing: B.G., M.C., M.C.M., E.K.R. and T.P.; Supervision: B.G., M.C.M. and T.P.; Project Administration: B.G., M.C. and M.C.M.; Funding Acquisition: B.G., E.K.R., T.P. and M.C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a The University of Notre Dame Australia Research Funding Scheme (RFS) Research Development Grant (Grant ID: IRO663/IRMA962).
Institutional Review Board Statement
Human Research Ethics Committee approval was obtained for this study (The University of Notre Dame Australia HREC approval: 2022-149F).
Informed Consent Statement
All participants provided informed consent prior to their participation in this study using an online Qualtrics survey (Qualtrics, Provo, UT, USA. https://www.qualtrics.com (accessed November 2022–March 2023).
Data Availability Statement
Study data are not available at this time due to the ongoing nature of a larger prevention project involving these data, and the ethical requirements related to this. Select data may be made available upon reasonable request after study completion.
Conflicts of Interest
Author Ebonie K Rio was employed by the company The Australian Ballet, as well as the Victorian Institute of Sport (VIS). The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Hamner, S.R.; Delp, S.L. Muscle contributions to fore-aft and vertical body mass center accelerations over a range of running speeds. J. Biomech. 2013, 46, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Maniar, N.; Schache, A.G.; Cole, M.H.; Opar, D.A. Lower-limb muscle function during sidestep cutting. J. Biomech. 2019, 82, 186–192. [Google Scholar] [CrossRef]
- Schache, A.G.; Lai, A.K.M.; Brown, N.A.T.; Crossley, K.M.; Pandy, M.G. Lower-limb joint mechanics during maximum acceleration sprinting. J. Exp. Biol. 2019, 222, jeb209460. [Google Scholar] [CrossRef] [PubMed]
- Sara, L.K.; Gutsch, S.B.; Hunter, S.K. The single-leg heel raise does not predict maximal plantar flexion strength in healthy males and females. PLoS ONE 2021, 16, e0253276. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Rio, E.; Debenham, J.; Docking, S.; Travers, M.; Gibson, W. Evaluating the progress of mid-portion achilles tendinopathy during rehabilitation: A review of outcome measures for muscle structure and function, tendon structure, and neural and pain associated mechanisms. Int. J. Sports Phys. Ther. 2018, 13, 537–551. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Ngawhika, T.M.; Balsalobre-Fernandez, C.; O’Neill, S. Calf muscle abilities are related to sprint performance in male Rugby Union players. Phys. Ther. Sport 2023, 64, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Ngawhika, T.M.; Gill, N.; Balsalobre-Fernandez, C. Validity, reliability, and normative data on calf muscle function in rugby union players from the Calf Raise application. Sports Biomech. 2022, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Hebert-Losier, K.; Schneiders, A.G.; Newsham-West, R.J.; Sullivan, S.J. Scientific bases and clinical utilisation of the calf raise test. Phys. Ther. Sport 2009, 10, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. The heel-raise test for ankle plantarflexor strength: A scoping review and meta-analysis of studies providing norms. J. Phys. Ther. Sci. 2022, 34, 528–531. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef]
- Barillas, S.R.; Oliver, J.L.; Lloyd, R.S.; Pedley, J.S. Kinetic Responses to External Cues Are Specific to Both the Type of Cue and Type of Exercise in Adolescent Athletes. J. Strength Cond. Res. 2023, 37, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; McClelland, J.A.; Semciw, A.I.; Schache, A.G.; McCall, A.; Pizzari, T. The Assessment, Management and Prevention of Calf Muscle Strain Injuries: A Qualitative Study of the Practices and Perspectives of 20 Expert Sports Clinicians. Sports Med. Open 2022, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Sman, A.D.; Hiller, C.E.; Imer, A.; Ocsing, A.; Burns, J.; Refshauge, K.M. Design and reliability of a novel heel rise test measuring device for plantarflexion endurance. BioMed Res. Int. 2014, 2014, 391646. [Google Scholar] [CrossRef] [PubMed]
- Lehecka, B.J.; Daniels, T.; Koester, B.; Kropp, W.; Reeves, M.; Waterson, R. Effects of Verbal and Tactile Cues on Gluteal Force Production and Broad Jump Distance. Int. J. Sports Phys. Ther. 2024, 19, 284–289. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M.R.; Cormack, S.J.; Gill, N.D. Strength and Power Profiling of Athletes: Selecting Tests and How to Use the Information for Program Design. Strength Cond. J. 2013, 35, 7–14. [Google Scholar] [CrossRef]
- Alcazar, J.; Csapo, R.; Ara, I.; Alegre, L.M. On the Shape of the Force-Velocity Relationship in Skeletal Muscles: The Linear, the Hyperbolic, and the Double-Hyperbolic. Front. Physiol. 2019, 10, 438208. [Google Scholar] [CrossRef]
- Cormie, P.; McGuigan, M.R.; Newton, R.U. Developing maximal neuromuscular power: Part 1--biological basis of maximal power production. Sports Med. 2011, 41, 17–38. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.C.; Debenham, J.; Bulsara, C.; Chivers, P.; Rio, E.K.; Docking, S.; Travers, M.; Gibson, W. Assessment and monitoring of Achilles tendinopathy in clinical practice: A qualitative descriptive exploration of the barriers clinicians face. BMJ Open Sport Exerc. Med. 2022, 8, e001355. [Google Scholar] [CrossRef] [PubMed]
- Meek, W.M.; Kucharik, M.P.; Eberlin, C.T.; Naessig, S.A.; Rudisill, S.S.; Martin, S.D. Calf Strain in Athletes. JBJS Rev. 2022, 10, e21.00183. [Google Scholar] [CrossRef]
- van der Vlist, A.C.; Breda, S.J.; Oei, E.H.G.; Verhaar, J.A.N.; de Vos, R.J. Clinical risk factors for Achilles tendinopathy: A systematic review. Br. J. Sports Med. 2019, 53, 1352–1361. [Google Scholar] [CrossRef]
- O’Neill, S.; Barry, S.; Watson, P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: The role of soleus. Phys. Ther. Sport 2019, 37, 69–76. [Google Scholar] [CrossRef]
- Kelly, S.; Pollock, N.; Polglass, G.; Clarsen, B. Injury and Illness in Elite Athletics: A Prospective Cohort Study Over Three Seasons. Int. J. Sports Phys. Ther. 2022, 17, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Hultman, K.; Szukics, P.F.; Grzenda, A.; Curriero, F.C.; Cohen, S.B. Gastrocnemius Injuries in Professional Baseball Players: An Epidemiological Study. Am. J. Sports Med. 2020, 48, 2489–2498. [Google Scholar] [CrossRef]
- Green, B.; Lin, M.; McClelland, J.A.; Semciw, A.I.; Schace, A.G.; Rotstein, A.; Cook, J.; Pizzari, T. Return to play and recurrence after calf muscle strain injuries in elite Australian football players. Am. J. Sports Med. 2020, 48, 363546520959327. [Google Scholar] [CrossRef]
- Orchard, J.W.; Jomaa, M.C.; Orchard, J.J.; Rae, K.; Hoffman, D.T.; Reddin, T.; Driscoll, T. Fifteen-week window for recurrent muscle strains in football: A prospective cohort of 3600 muscle strains over 23 years in professional Australian rules football. Br. J. Sports Med. 2020, 54, 1103–1107. [Google Scholar] [CrossRef]
- Hebert-Losier, K.; Wessman, C.; Alricsson, M.; Svantesson, U. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy 2017, 103, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Schneiders, A.G.; García, J.A.; Sullivan, S.J.; Simoneau, G.G. Influence of knee flexion angle and age on triceps surae muscle activity during heel raises. J. Strength Cond. Res. 2012, 26, 3124–3133. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef]
- Lee, M.; Lancaster, M.; Tulloch, L.; O’Leary, B.; Power, E.; Howes, D.; Sourbuts, B.; Berry, A.; Maher, F.; O’Neill, S. Normative isometric plantarflexion strength values for professional level, male rugby union athletes. Phys. Ther. Sport 2023, 61, 114–121. [Google Scholar] [CrossRef]
- Green, B.; Lin, M.; Schache, A.G.; McClelland, J.A.; Rotstein, A.H.; Semciw, A.I.; Cook, J.; Pizzari, T. Calf muscle strain injuries in elite Australian football players: A descriptive epidemiological evaluation. Scand. J. Med. Sci. Sports 2020, 30, 174–184. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Yasui, Y.; Tonogai, I.; Rosenbaum, A.J.; Shimozono, Y.; Kawano, H.; Kennedy, J.G. The Risk of Achilles Tendon Rupture in the Patients with Achilles Tendinopathy: Healthcare Database Analysis in the United States. BioMed. Res. Int. 2017, 2017, 7021862. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef]
- van Stralen, K.J.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Measuring agreement, more complicated than it seems. Nephron Clin. Pract. 2012, 120, c162–c167. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.C.; Travers, M.; Chivers, P.; Debenham, J.; Docking, S.I.; Rio, E.K.; Gibson, W.; Ardern, C. Can we really say getting stronger makes your tendon feel better? No current evidence of a relationship between change in Achilles tendinopathy pain or disability and changes in Triceps Surae structure or function when completing rehabilitation: A systematic review. J. Sci. Med. Sport. 2023, 26, 253–260. [Google Scholar] [CrossRef]
- Green, B.; Pizzari, T. Calf muscle strain injuries in sport: A systematic review of risk factors for injury. Br. J. Sports Med. 2017, 51, 1189–1194. [Google Scholar] [CrossRef]
- Orchard, J.W. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am. J. Sports Med. 2001, 29, 300–303. [Google Scholar] [CrossRef]
- Orchard, J.; Orchard, J.; Seward, H. A Comparison between Australian Football League (AFL) Injuries in Australian Indigenous versus Non-indigenous Players. Sports 2013, 1, 69–77. [Google Scholar] [CrossRef]
- Fujiwara, K.; Asai, H.; Toyama, H.; Kunita, K.; Yaguchi, C.; Kiyota, N.; Tomita, H.; Jacobs, J.V. Changes in muscle thickness of gastrocnemius and soleus associated with age and sex. Aging Clin. Exp. Res. 2010, 22, 24–30. [Google Scholar] [CrossRef]
- Kubo, K.; Morimoto, M.; Komuro, T.; Yata, H.; Tsunoda, N.; Kanehisa, H.; Fukunaga, T. Effects of Plyometric and Weight Training on Muscle-Tendon Complex and Jump Performance. Med. Sci. Sports Exerc. 2007, 39, 1801–1810. [Google Scholar] [CrossRef]
- Bertelson, M.L.; Hulme, A.; Peterson, J.; Brund, R.K.; Sørensen, H.; Finch, C.F.; Parner, E.T.; Nielsen, R.O. A framework for the etiology of running-related injuries. Scand. J. Med. Sci. Sports 2017, 27, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.H.; Hornsby, W.G.; Suarez, D.G.; Duca, M.; Pierce, K.C. Training Specificity for Athletes: Emphasis on Strength-Power Training: A Narrative Review. J. Funct. Morphol. Kinesiol. 2022, 7, 102. [Google Scholar] [CrossRef] [PubMed]
- Vaara, J.P.; Kyröläinen, H.; Niemi, J.; Ohrankämmen, O.; Häkkinen, A.; Kocay, S.; Häkkinen, K. Associations of maximal strength and muscular endurance test scores with cardiorespiratory fitness and body composition. J. Strength Cond. Res. 2012, 26, 2078–2086. [Google Scholar] [CrossRef] [PubMed]
- Ishøi, L.; Krommes, K.; Husted, R.S.; Juhl, C.B.; Thorborg, K. Diagnosis, prevention and treatment of common lower extremity muscle injuries in sport—Grading the evidence: A statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF). Br. J. Sports Med. 2020, 54, 528–537. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).